
Relationships between Long-Term Ozone Exposure and Allergic Rhinitis and Bronchitic Symptoms in Chinese Children

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
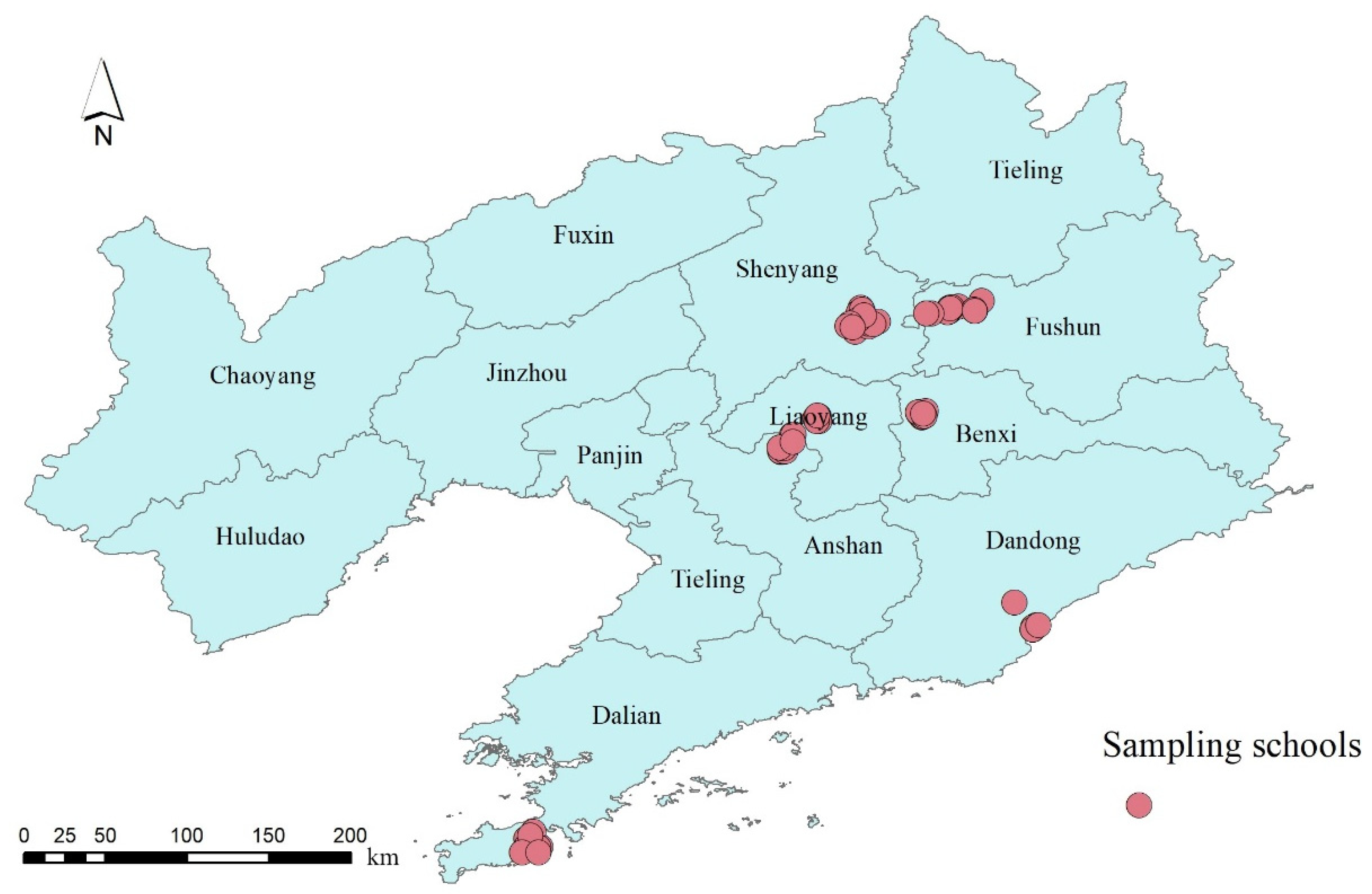
2.1. Study Population
2.2. Measurement
2.2.1. Outcomes
2.2.2. Ambient O3 Exposure Assessment
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Ambient O3 Exposure
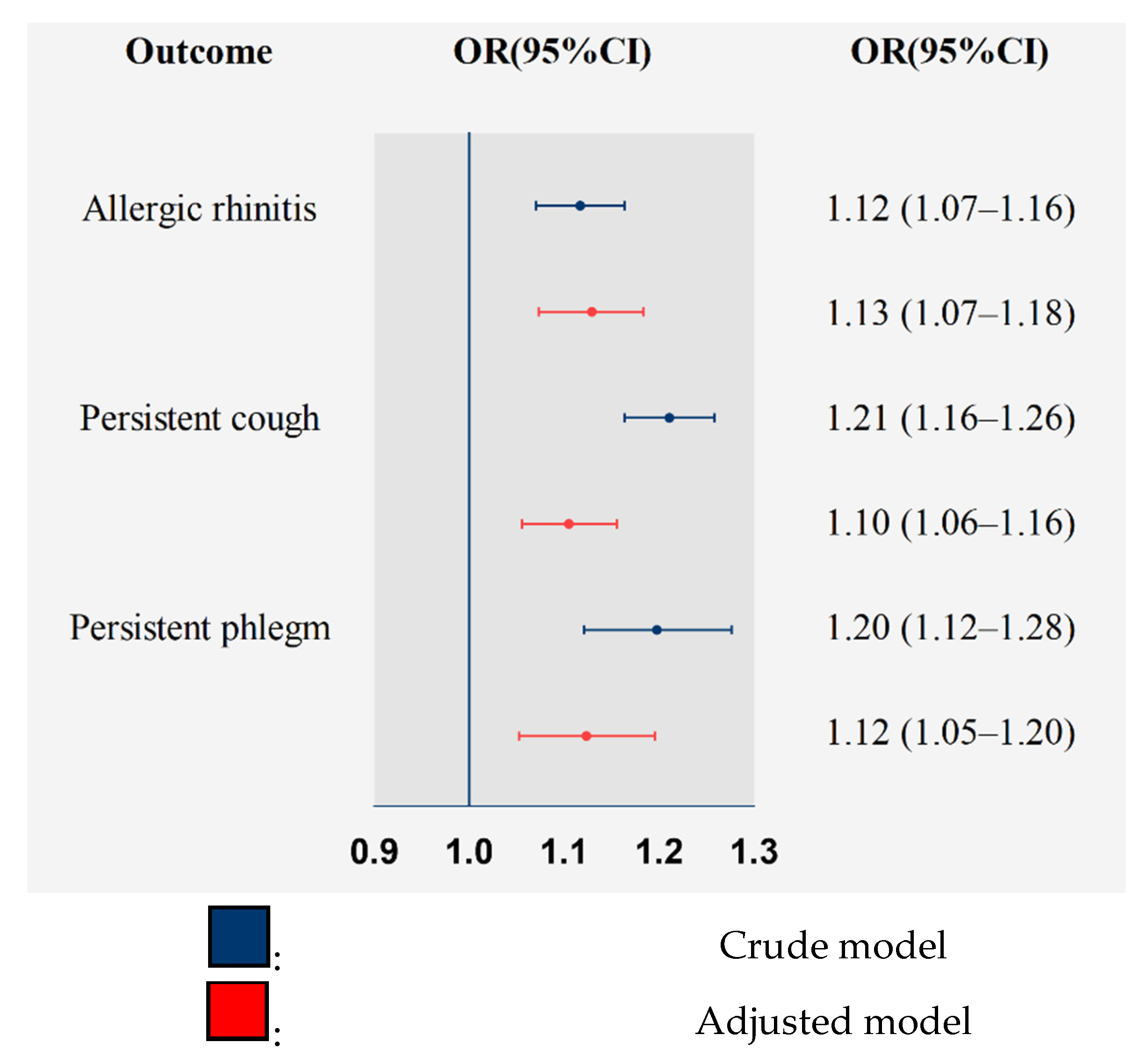
3.3. Associations between O3 and AR and Bronchitic Symptoms
4. Discussion
4.1. Associations between O3 and AR and Bronchitic Symptoms
4.2. Potential Biological Mechanisms
4.3. Significance for Public Health
4.4. Advantages and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chatkin, J.; Correa, L.; Santos, U. External Environmental Pollution as a Risk Factor for Asthma. Clin. Rev. Allergy Immu. 2021, 1–18. [Google Scholar] [CrossRef]
- Huangfu, P.; Atkinson, R. Long-term exposure to NO2 and O3 and all-cause and respiratory mortality: A systematic review and meta-analysis. Environ. Int. 2020, 144, 105998. [Google Scholar] [CrossRef]
- McConnell, R.; Berhane, K.; Gilliland, F.; London, S.J.; Islam, T.; Gauderman, W.J.; Avol, E.; Margolis, H.G.; Peters, J.M. Asthma in exercising children exposed to ozone: A cohort study. Lancet 2002, 359, 386–391. [Google Scholar] [CrossRef]
- Sahu, S.K.; Liu, S.C.; Liu, S.; Ding, D.; Xing, J. Ozone pollution in China: Background and transboundary contributions to ozone concentration & related health effects across the country. Sci. Total Environ. 2021, 761, 144131. [Google Scholar] [CrossRef] [PubMed]
- Peden, D.B. Mechanisms of pollution-induced airway disease: In vivo studies. Allergy 1997, 52, 37–44, discussion 57–38. [Google Scholar] [CrossRef] [PubMed]
- Schraufnagel, D.E.; Balmes, J.R.; Cowl, C.T.; De Matteis, S.; Jung, S.H.; Mortimer, K.; Perez-Padilla, R.; Rice, M.B.; Riojas-Rodriguez, H.; Sood, A.; et al. Air Pollution and Noncommunicable Diseases A Review by the Forum of International Respiratory Societies’ Environmental Committee, Part 1: The Damaging Effects of Air Pollution. Chest 2019, 155, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef]
- Maji, K.J.; Namdeo, A. Continuous increases of surface ozone and associated premature mortality growth in China during 2015–2019. Environ. Pollut 2021, 269, 116183. [Google Scholar] [CrossRef]
- Report on the State of the Ecology and Environment in China 2019: Ministry of Ecology and Environment, the People’s Republic of China [Updated 2020]. Available online: http://english.mee.gov.cn/Resources/Reports/soe/SOEE2019/202012/P020201215587453898053.pdf (accessed on 24 May 2021).
- Huang, C.; Liu, W.; Hu, Y.; Zou, Z.; Zhao, Z.; Shen, L.; Weschler, L.B.; Sundell, J. Updated prevalences of asthma, allergy, and airway symptoms, and a systematic review of trends over time for childhood asthma in Shanghai, China. PLoS ONE 2015, 10, e0121577. [Google Scholar] [CrossRef]
- Wong, G.W.; Leung, T.F.; Ko, F.W. Changing prevalence of allergic diseases in the Asia-pacific region. Allergy Asthma Immunol. Res. 2013, 5, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Postma, D.S.; Bush, A.; van den Berge, M. Risk factors and early origins of chronic obstructive pulmonary disease. Lancet 2015, 385, 899–909. [Google Scholar] [CrossRef]
- Stocks, J.; Hislop, A.; Sonnappa, S. Early lung development: Lifelong effect on respiratory health and disease. Lancet Resp. Med. 2013, 1, 728–742. [Google Scholar] [CrossRef]
- Kuiper, I.N.; Svanes, C.; Markevych, I.; Accordini, S.; Bertelsen, R.J.; Braback, L.; Christensen, J.H.; Forsberg, B.; Halvorsen, T.; Heinrich, J.; et al. Lifelong exposure to air pollution and greenness in relation to asthma, rhinitis and lung function in adulthood. Environ. Int. 2021, 146, 10. [Google Scholar] [CrossRef]
- Wang, I.J.; Tung, T.H.; Tang, C.S.; Zhao, Z.H. Allergens, air pollutants, and childhood allergic diseases. Int. J. Hyg. Environ. Health 2016, 219, 66–71. [Google Scholar] [CrossRef]
- To, T.; Zhu, J.Q.; Stieb, D.; Gray, N.; Fong, I.; Pinault, L.; Jerrett, M.; Robichaud, A.; Menard, R.; van Donkelaar, A.; et al. Early life exposure to air pollution and incidence of childhood asthma, allergic rhinitis and eczema. Eur. Respir. J. 2020, 55, 1900913. [Google Scholar] [CrossRef]
- Dokic, D.; Trajkovska-Dokic, E. Ozone exaggerates nasal allergic inflammation. Pril (Makedon Akad Nauk. Umet Odd Med. Nauk.) 2013, 34, 131–141. [Google Scholar]
- Fuentes, N.; Roy, A.; Mishra, V.; Cabello, N.; Silveyra, P. Sex-specific microRNA expression networks in an acute mouse model of ozone-induced lung inflammation. Biol. Sex. Differ. 2018, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, C.D.; Henneberger, P.K.; Olin, A.C.; Mehta, A.; Toren, K. Exposure to ozone gases in pulp mills and the onset of rhinitis. Scand. J. Work Environ. Health 2004, 30, 445–449. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhang, X.; Li, C.; Bai, X.; Zhao, Z.; Norback, D. Onset of respiratory symptoms among Chinese students: Associations with dampness and redecoration, PM10, NO2, SO2 and inadequate ventilation in the school. J. Asthma 2020, 57, 495–504. [Google Scholar] [CrossRef]
- Stergiopoulou, A.; Katavoutas, G.; Samoli, E.; Dimakopoulou, K.; Papageorgiou, I.; Karagianni, P.; Flocas, H.; Katsouyanni, K. Assessing the associations of daily respiratory symptoms and lung function in schoolchildren using an Air Quality Index for ozone: Results from the RESPOZE panel study in Athens, Greece. Sci. Total Environ. 2018, 633, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Berhane, K.; Chang, C.C.; McConnell, R.; Gauderman, W.J.; Avol, E.; Rapapport, E.; Urman, R.; Lurmann, F.; Gilliland, F. Association of Changes in Air Quality With Bronchitic Symptoms in Children in California, 1993–2012. JAMA 2016, 315, 1491–1501. [Google Scholar] [CrossRef] [PubMed]
- Castillejos, M.; Gold, D.R.; Dockery, D.; Tosteson, T.; Baum, T.; Speizer, F.E. Effects of ambient ozone on respiratory function and symptoms in Mexico City schoolchildren. Am. Rev. Respir. Dis. 1992, 145, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Galizia, A.; Kinney, P.L. Long-term residence in areas of high ozone: Associations with respiratory health in a nationwide sample of nonsmoking young adults [dsee comments]. Environ. Health Perspect. 1999, 107, 675–679. [Google Scholar] [CrossRef] [PubMed]
- McConnell, R.; Berhane, K.; Gilliland, F.; London, S.J.; Vora, H.; Avol, E.; Gauderman, W.J.; Margolis, H.G.; Lurmann, F.; Thomas, D.C.; et al. Air pollution and bronchitic symptoms in Southern California children with asthma. Environ. Health Perspect 1999, 107, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Zmirou, D.; Balducci, F.; Dechenaux, J.; Piras, A.; Filippi, F.; Benoit-Guyod, J.L. Meta-analysis and dose-response functions of air pollution respiratory effects. Rev. Epidemiol. Sante Publique 1997, 45, 293–304. [Google Scholar] [PubMed]
- Liu, K.K.; Li, S.S.; Qian, Z.M.; Dharmage, S.C.; Bloom, M.S.; Heinrich, J.; Jalaludin, B.; Markevych, I.; Morawska, L.; Knibbs, L.D.; et al. Benefits of influenza vaccination on the associations between ambient air pollution and allergic respiratory diseases in children and adolescents: New insights from the Seven Northeastern Cities study in China. Environ. Pollut. 2020, 256, 113434. [Google Scholar] [CrossRef] [PubMed]
- Ferris, B.G. Epidemiology Standardization Project (American Thoracic Society). Am. Rev. Respir. Dis. 1978, 118, 1–120. [Google Scholar]
- Dong, G.H.; Chen, T.; Liu, M.M.; Wang, D.; Ma, Y.N.; Ren, W.H.; Lee, Y.L.; Zhao, Y.D.; He, Q.C. Gender Differences and Effect of Air Pollution on Asthma in Children with and without Allergic Predisposition: Northeast Chinese Children Health Study. PLoS ONE 2011, 6, e22470. [Google Scholar] [CrossRef] [Green Version]
- Hwang, B.F.; Lee, Y.L. Air Pollution and Prevalence of Bronchitic Symptoms Among Children in Taiwan. Chest 2010, 138, 956–964. [Google Scholar] [CrossRef]
- Wang, J.Y.; Li, S.; Wang, S.G.; Shang, K.Z. Effects of Long-Term Dust Exposure on Human Respiratory System Health in Minqin County, China. Arch. Environ. Occup. Health 2015, 70, 225–231. [Google Scholar] [CrossRef]
- Dong, G.H.; Qian, Z.M.; Liu, M.M.; Wang, D.; Ren, W.H.; Bawa, S.; Fu, J.; Wang, J.; Lewis, R.; Zelicoff, A.; et al. Breastfeeding as a Modifier of the Respiratory Effects of Air Pollution in Children. Epidemiology 2013, 24, 387–394. [Google Scholar] [CrossRef]
- Chen, G.; Chen, J.; Dong, G.-H.; Yang, B.-Y.; Liu, Y.; Lu, T.; Yu, P.; Guo, Y.; Li, S. Improving satellite-based estimation of surface ozone across China during 2008–2019 using iterative random forest model and high-resolution grid meteorological data. Sustain. Cities Soc. 2021, 69, 102807. [Google Scholar] [CrossRef]
- Fuertes, E.; Sunyer, J.; Gehring, U.; Porta, D.; Forastiere, F.; Cesaroni, G.; Vrijheid, M.; Guxens, M.; Annesi-Maesano, I.; Slama, R.; et al. Associations between air pollution and pediatric eczema, rhinoconjunctivitis and asthma: A meta-analysis of European birth cohorts. Environ. Int. 2020, 136, 105474. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Wijga, A.H.; Hoek, G.; Bellander, T.; Berdel, D.; Bruske, I.; Fuertes, E.; Gruzieva, O.; Heinrich, J.; Hoffmann, B.; et al. Exposure to air pollution and development of asthma and rhinoconjunctivitis throughout childhood and adolescence: A population-based birth cohort study. Lancet Resp. Med. 2015, 3, 933–942. [Google Scholar] [CrossRef] [Green Version]
- National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention. BMI: Body Mass Index; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2002. Available online: http://www.cdc.gov/nccdphp/dnpa/bmi (accessed on 27 January 2012).
- Hu, Y.B.; Xu, Z.W.; Jiang, F.; Li, S.H.; Liu, S.J.; Wu, M.Q.; Yan, C.H.; Tan, J.G.; Yu, G.J.; Hu, Y.; et al. Relative impact of meteorological factors and air pollutants on childhood allergic diseases in Shanghai, China. Sci. Total Environ. 2020, 706, 135975. [Google Scholar] [CrossRef]
- Chen, J.; Li, Y.; Jiang, F. Research meteorological environmental factors in children’s allergic rhinitis. Lin Chung Er. Bi Yan Hou Tou Jing Wai Ke Za Zhi 2014, 28, 1015–1019. [Google Scholar]
- Fuertes, E.; Standl, M.; Cyrys, J.; Berdel, D.; von Berg, A.; Bauer, C.P.; Kramer, U.; Sugiri, D.; Lehmann, I.; Koletzko, S.; et al. A longitudinal analysis of associations between traffic-related air pollution with asthma, allergies and sensitization in the GINIplus and LISAplus birth cohorts. Peerj 2013, 1, e193. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Niu, Y.; Zhang, R.; Huang, Y.; Wang, J.; Qiu, W.; Zhang, X.; Han, Z.; Bao, J.; Zhu, H.; et al. Ozone inhalation induces exacerbation of eosinophilic airway inflammation and Th2-skew immune response in a rat model of AR. Biomed. Pharmacother. Biomed. Pharmacother. 2021, 137, 111261. [Google Scholar] [CrossRef]
- Sun, N.; Han, Z.J.; Wang, H.; Guo, Z.Q.; Deng, C.R.; Dong, W.Y.; Zhuang, G.S.; Zhang, R.X. Effects of Ursolic Acid on the Expression of Th1-Th2-related Cytokines in a Rat Model of Allergic Rhinitis After PM2.5 Exposure. Am. J. Rhinol. Allergy 2020, 34, 587–596. [Google Scholar] [CrossRef]
- Hodge, M.X.; Henriquez, A.R.; Kodavanti, U.P. Adrenergic and Glucocorticoid Receptors in the Pulmonary Health Effects of Air Pollution. Toxics 2021, 9, 132. [Google Scholar] [CrossRef]
- Kierstein, S.; Krytska, K.; Sharma, S.; Amrani, Y.; Salmon, M.; Panettieri, R.A.; Zangrilli, J.; Haczku, A. Ozone inhalation induces exacerbation of eosinophilic airway inflammation and hyperresponsiveness in allergen-sensitized mice. Allergy 2008, 63, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Wiegman, C.H.; Li, F.; Ryffel, B.; Togbe, D.; Chung, K.F. Oxidative Stress in Ozone-Induced Chronic Lung Inflammation and Emphysema: A Facet of Chronic Obstructive Pulmonary Disease. Front. Immunol. 2020, 11, 1957. [Google Scholar] [CrossRef] [PubMed]
- Veres, T.Z.; Rochlitzer, S.; Braun, A. The role of neuro-immune cross-talk in the regulation of inflammation and remodelling in asthma. Pharmacol. Ther. 2009, 122, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.; Kwong, K.; Lin, Y.S.; Gu, Q. Hypersensitivity of bronchopulmonary C-fibers induced by airway mucosal inflammation: Cellular mechanisms. Pulm. Pharmacol. Ther. 2002, 15, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Cabello, N.; Mishra, V.; Sinha, U.; DiAngelo, S.L.; Chroneos, Z.C.; Ekpa, N.A.; Cooper, T.K.; Caruso, C.R.; Silveyra, P. Sex differences in the expression of lung inflammatory mediators in response to ozone. Am. J. Physiol.-Lung. Cell Mol. Physiol. 2015, 309, L1150–L1163. [Google Scholar] [CrossRef] [PubMed]
- Aikin, A.C.; Herman, J.R.; Maier, E.J.; McQuillan, C.J. Atmospheric chemistry of ethane and ethylene. J. Geophys. Res. Ocean. 1982, 87, 3105–3118. [Google Scholar] [CrossRef]
- Sun, S.; Liu, W.; Guan, W.; Zhu, S.; Jia, J.; Wu, X.; Lei, R.; Jia, T.; He, Y. Effects of air pollution control devices on volatile organic compounds reduction in coal-fired power plants. Sci. Total. Environ. 2021, 782, 146828. [Google Scholar] [CrossRef]
- Gong, K.; Li, L.; Li, J.; Qin, M.; Wang, X.; Ying, Q.; Liao, H.; Guo, S.; Hu, M.; Zhang, Y.; et al. Quantifying the impacts of inter-city transport on air quality in the Yangtze River Delta urban agglomeration, China: Implications for regional cooperative controls of PM2.5 and O3. Sci. Total Environ. 2021, 779, 146619. [Google Scholar] [CrossRef]
- Air Quality Guide for Ozone: United States Environmental Protection Agency. Available online: https://www.airnow.gov/sites/default/files/2021-03/air-quality-guide_ozone_2015.pdf (accessed on 16 June 2021).



{kind=link}
{kind=link}
| Variables | Participants with at Least One of the Diseases Involved # (n = 7274) | Participants without Any of the Diseases Involved # (n = 52,480) | Total (n = 59,754) | p-Value * |
|---|---|---|---|---|
| Age (years), mean (SD) | 10.02 (3.63) | 10.35 (3.59) | 10.31 (3.60) | <0.001 |
| Gender | <0.001 | |||
| Boys | 4140 (56.92) | 26,120 (49.77) | 30,260 (50.64) | |
| Girls | 3134 (43.08) | 26,360 (50.23) | 29,494 (49.36) | |
| Height (cm), mean (SD) | 142.74 (22.29) | 144.13 (21.65) | 143.96 (21.73) | <0.001 |
| Weight (kg), mean (SD) | 39.85 (16.69) | 40.04 (16.13) | 40.02 (16.20) | 0.356 |
| Exercise time per week (hour), mean (SD) | 5.96 (7.51) | 6.65 (8.03) | 6.56 (7.97) | <0.001 |
| residence floor area per person (m2), mean (SD) | 24.52 (12.77) | 23.48 (12.39) | 23.60 (12.44) | <0.001 |
| Parental education | 0.005 | |||
| ≥high school | 5430 (74.65) | 38,356 (73.09) | 43,786 (73.28) | |
| <high school | 1844 (25.35) | 14,124 (26.91) | 15,968 (26.72) | |
| Obesity | <0.001 | |||
| No | 6646 (91.37) | 48,737 (92.87) | 55,383 (92.69) | |
| Yes | 628 (8.63) | 3743 (7.13) | 4371 (7.31) | |
| Low birth weight | 0.019 | |||
| No | 6972 (95.85) | 50,595 (96.41) | 57,567 (96.34) | |
| Yes | 302 (4.15) | 1885 (3.59) | 2187 (3.66) | |
| Premature delivery | <0.001 | |||
| No | 6756 (92.88) | 49,781 (94.86) | 56,537 (94.62) | |
| Yes | 518 (7.12) | 2699 (5.14) | 3217 (5.38) | |
| Environmental tobacco smoke exposure | <0.001 | |||
| No | 3456 (47.51) | 28,476 (54.26) | 31,932 (53.44) | |
| Yes | 3818 (52.49) | 24,004 (45.74) | 27,822 (46.56) | |
| Breastfeeding | <0.001 | |||
| No | 2726 (37.48) | 17,272 (32.91) | 19,998 (33.47) | |
| Yes | 4548 (62.52) | 35,208 (67.09) | 39,756 (66.53) | |
| Family allergic history | <0.001 | |||
| No | 4802 (66.02) | 43,410 (82.72) | 48,212 (80.68) | |
| Yes | 2472 (33.98) | 9070 (17.28) | 11,542 (19.32) | |
| Family income per year | <0.001 | |||
| ≤9999 RMB | 1655 (22.75) | 10,804 (20.59) | 12,459 (20.85) | |
| 10,000–29,999 RMB | 2445 (33.61) | 19,725 (37.59) | 22,170 (37.10) | |
| 30,000–100,000 RMB | 2560 (35.19) | 18,438 (35.13) | 20,998 (35.14) | |
| >100,000 RMB | 614 (8.44) | 3513 (6.69) | 4127 (6.91) |
| City | 2008 | 2009 | 2010 | 2011 | Average 2008–2011 |
|---|---|---|---|---|---|
| Shenyang | 91.05 (0.37) | 90.42 (0.38) | 89.55 (0.33) | 89.20 (0.25) | 90.07 (0.35) |
| Dalian | 92.92 (0.40) | 94.08 (0.08) | 92.23 (0.50) | 91.16 (0.52) | 92.62 (0.39) |
| Fushun | 87.45 (1.29) | 87.24 (1.60) | 86.44 (1.44) | 86.59 (1.41) | 86.89 (1.43) |
| Anshan | 91.30 (0.27) | 91.30 (0.24) | 89.74 (0.25) | 89.55 (0.33) | 90.45 (0.25) |
| Benxi | 85.99 (0.83) | 86.27 (0.70) | 85.72 (0.81) | 85.78 (0.68) | 85.94 (0.76) |
| Dandong | 88.57 (0.11) | 88.71 (0.11) | 87.89 (0.08) | 87.28 (0.09) | 88.11 (0.10) |
| Liaoyang | 91.13 (0.16) | 91.09 (0.05) | 89.90 (0.14) | 89.83 (0.16) | 90.48 (0.12) |
| Total | 90.91 (3.52) | 90.31 (3.30) | 89.41 (2.94) | 89.08 (2.76) | 89.92 (3.20) |
| Allergic Rhinitis | Cough | Phlegm | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p * | OR (95% CI) | p * | OR (95% CI) | p * | |
| Age | ||||||
| 2–6 | 0.96 (0.85–1.08) | 1.06 (0.97–1.15) | 1.14 (1.01–1.27) | |||
| 7–12 | 1.16 (1.07–1.24) | 0.012 | 1.23 (1.16–1.30) | 0.008 | 1.21 (1.15–1.28) | 0.423 |
| 13–17 | 1.14 (1.05–1.24) | 0.022 | 1.02 (0.93–1.12) | 0.584 | 1.03 (0.91–1.16) | 0.238 |
| Gender | ||||||
| Boys | 1.09 (0.95–1.26) | 0.96 (0.83–1.11) | 0.96 (0.80–1.15) | |||
| Girls | 1.12 (1.05–1.19) | 0.641 | 1.06 (0.99–1.13) | 0.043 | 1.07 (0.98–1.16) | 0.066 |
| Family allergic history | ||||||
| No | 1.09 (1.03–1.16) | 1.11 (1.05–1.17) | 1.12 (1.04–1.21) | |||
| Yes | 1.17 (1.09–1.26) | 0.131 | 1.09 (1.004–1.19) | 0.770 | 1.11 (0.99–1.25) | 0.890 |
| Obesity | ||||||
| No | 1.12 (1.07–1.18) | 1.11 (1.06–1.17) | 1.14 (1.06–1.22) | |||
| Yes | 1.17 (0.98–1.39) | 0.662 | 1.02 (0.89–1.17) | 0.243 | 0.99 (0.81–1.2) | 0.183 |
| Breastfeeding | ||||||
| No | 1.13 (1.04–1.22) | 1.05 (0.98–1.13) | 1.07 (0.97–1.19) | |||
| Yes | 1.13 (1.06–1.20) | 0.995 | 1.14 (1.08–1.20) | 0.081 | 1.15 (1.06–1.24) | 0.275 |
| Premature delivery | ||||||
| No | 1.12 (1.07–1.18) | 1.11 (1.06–1.16) | 1.13 (1.06–1.21) | |||
| Yes | 1.19 (1.01–1.40) | 0.510 | 1.07 (0.92–1.25) | 0.701 | 1.05 (0.85–1.28) | 0.481 |
| Low birth weight | ||||||
| No | 1.13 (1.07–1.18) | 1.10 (1.05–1.15) | 1.11 (1.04–1.19) | |||
| Yes | 1.18 (0.94–1.47) | 0.697 | 1.23 (0.99–1.53) | 0.308 | 1.30 (1.004–1.69) | 0.247 |
| Environmental tobacco smoke exposure | ||||||
| No | 1.15 (1.08–1.22) | 1.07 (1.01–1.14) | 1.09 (0.99–1.20) | |||
| Yes | 1.10 (1.03–1.18) | 0.372 | 1.13 (1.07–1.20) | 0.216 | 1.15 (1.06–1.25) | 0.382 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, P.-E.; Qian, Z.; McMillin, S.E.; Vaughn, M.G.; Xie, Z.-Y.; Xu, Y.-J.; Lin, L.-Z.; Hu, L.-W.; Yang, B.-Y.; Zeng, X.-W.; et al. Relationships between Long-Term Ozone Exposure and Allergic Rhinitis and Bronchitic Symptoms in Chinese Children. Toxics 2021, 9, 221. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090221
Zhou P-E, Qian Z, McMillin SE, Vaughn MG, Xie Z-Y, Xu Y-J, Lin L-Z, Hu L-W, Yang B-Y, Zeng X-W, et al. Relationships between Long-Term Ozone Exposure and Allergic Rhinitis and Bronchitic Symptoms in Chinese Children. Toxics. 2021; 9(9):221. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090221
Chicago/Turabian StyleZhou, Pei-En, Zhengmin (Min) Qian, Stephen Edward McMillin, Michael G. Vaughn, Zhong-Yue Xie, Yu-Jie Xu, Li-Zi Lin, Li-Wen Hu, Bo-Yi Yang, Xiao-Wen Zeng, and et al. 2021. "Relationships between Long-Term Ozone Exposure and Allergic Rhinitis and Bronchitic Symptoms in Chinese Children" Toxics 9, no. 9: 221. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090221