Heart Failure Drug Class Effects on 30-Day Readmission Rates in Patients with Heart Failure with Preserved Ejection Fraction: A Retrospective Single Center Study

 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E., Jr.; Colvin, M.M.; Drazner, M.H.; Filippatos, G.S.; Fonarow, G.C.; Givertz, M.M.; et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J. Am. Coll Cardiol. 2017, 70, 776–803. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L. Epidemiology of heart failure. Circ. Res. 2013, 113, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.T.; Jhund, P.S.; Castagno, D.; Hawkins, N.M.; Petrie, M.C.; McMurray, J.J. What have we learned about patients with heart failure and preserved ejection fraction from DIG-PEF, CHARM-preserved, and I-PRESERVE? J. Am. Coll Cardiol. 2012, 60, 2349–2356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, S.L.; Tong, X.; King, R.J.; Loustalot, F.; Hong, Y.; Ritchey, M.D. National Burden of Heart Failure Events in the United States, 2006 to 2014. Circ. Heart Fail. 2018, 11, e004873. [Google Scholar] [CrossRef] [PubMed]
- Hospital Readmissions Reduction Program (HRRP). Available online: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/HRRP/Hospital-Readmission-Reduction-Program (accessed on 18 December 2019).
- Gupta, A.; Allen, L.A.; Bhatt, D.L.; Cox, M.; DeVore, A.D.; Heidenreich, P.A.; Hernandez, A.F.; Peterson, E.D.; Matsouaka, R.A.; Yancy, C.W.; et al. Association of the Hospital Readmissions Reduction Program Implementation With Readmission and Mortality Outcomes in Heart Failure. JAMA Cardiol. 2018, 3, 44–53. [Google Scholar] [CrossRef]
- Casu, G.; Merella, P. Diuretic Therapy in Heart Failure-Current Approaches. Eur. Cardiol. 2015, 10, 42–47. [Google Scholar] [CrossRef]
- Adamson, P.B.; Abraham, W.T.; Bourge, R.C.; Costanzo, M.R.; Hasan, A.; Yadav, C.; Henderson, J.; Cowart, P.; Stevenson, L.W. Wireless pulmonary artery pressure monitoring guides management to reduce decompensation in heart failure with preserved ejection fraction. Circ. Heart Fail. 2014, 7, 935–944. [Google Scholar] [CrossRef] [Green Version]
- Bhattarai, M.; Hudali, T.; Robinson, R.; Al-Akchar, M.; Vogler, C.; Chami, Y. Impact of oral anticoagulants on 30-day readmission: A study from a single academic centre. BMJ Evid Based Med. 2019, 24, 10–14. [Google Scholar] [CrossRef]
- Robinson, R.; Hudali, T. The HOSPITAL score and LACE index as predictors of 30 day readmission in a retrospective study at a university-Affiliated community hospital. PeerJ 2017, 5, e3137. [Google Scholar] [CrossRef] [Green Version]
- Robinson, R.; Bhattarai, M.; Hudali, T. Vital Sign Abnormalities on Discharge Do Not Predict 30-Day Readmission. Clin. Med. Res. 2019, 17, 63–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, R.; Bhattarai, M.; Hudali, T.; Vogler, C. Predictors of 30-day hospital readmission: The direct comparison of number of discharge medications to the HOSPITAL score and LACE index. Future Healthc J. 2019, 6, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzuoli, A.; Testani, J.M.; Ruocco, G.; Pellegrini, M.; Ronco, C.; Nuti, R. Different diuretic dose and response in acute decompensated heart failure: Clinical characteristics and prognostic significance. Int. J. Cardiol. 2016, 224, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Okabe, T.; Yakushiji, T.; Kido, T.; Oyama, Y.; Igawa, W.; Ono, M.; Ebara, S.; Yamashita, K.; Yamamoto, M.H.; Saito, S.; et al. The association between high-Dose loop diuretic use at discharge and cardiovascular mortality in patients with heart failure. ESC Heart Fail. 2018, 5, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Mecklai, A.; Subacius, H.; Konstam, M.A.; Gheorghiade, M.; Butler, J.; Ambrosy, A.P.; Katz, S.D. In-Hospital Diuretic Agent Use and Post-Discharge Clinical Outcomes in Patients Hospitalized for Worsening Heart Failure: Insights From the EVEREST Trial. JACC Heart Fail. 2016, 4, 580–588. [Google Scholar] [CrossRef]
- Bavishi, C.; Chatterjee, S.; Ather, S.; Patel, D.; Messerli, F.H. Beta-Blockers in heart failure with preserved ejection fraction: A meta-Analysis. Heart Fail. Rev. 2015, 20, 193–201. [Google Scholar] [CrossRef]
- Feng, J.L.; Qin, X. Association between evidence-based medication at discharge and outcomes in patients with heart failure: A systematic review and meta-Analysis. Heart Fail. Rev. 2019. [Google Scholar] [CrossRef]
- van Veldhuisen, D.J.; Cohen-Solal, A.; Bohm, M.; Anker, S.D.; Babalis, D.; Roughton, M.; Coats, A.J.; Poole-Wilson, P.A.; Flather, M.D.; Investigators, S. Beta-Blockade with nebivolol in elderly heart failure patients with impaired and preserved left ventricular ejection fraction: Data From SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure). J. Am. Coll Cardiol 2009, 53, 2150–2158. [Google Scholar] [CrossRef]
- Yamamoto, K.; Origasa, H.; Hori, M.; Investigators, J.D. Effects of carvedilol on heart failure with preserved ejection fraction: The Japanese Diastolic Heart Failure Study (J-DHF). Eur. J. Heart Fail. 2013, 15, 110–118. [Google Scholar] [CrossRef]
- Khan, M.S.; Fonarow, G.C.; Khan, H.; Greene, S.J.; Anker, S.D.; Gheorghiade, M.; Butler, J. Renin-Angiotensin blockade in heart failure with preserved ejection fraction: A systematic review and meta-Analysis. ESC Heart Fail. 2017, 4, 402–408. [Google Scholar] [CrossRef]
- Cleland, J.G.; Tendera, M.; Adamus, J.; Freemantle, N.; Polonski, L.; Taylor, J.; Investigators, P.-C. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur. Heart J. 2006, 27, 2338–2345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac remodeling--Concepts and clinical implications: A consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J. Am. Coll Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [Green Version]
- Paulus, W.J.; Tschope, C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J. Am. Coll Cardiol. 2013, 62, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanam, K.; Bhatia, V.; Bajaj, N.S.; Gaba, S.; Morgan, C.J.; Fonarow, G.C.; Butler, J.; Deedwania, P.; Prabhu, S.D.; Wu, W.C.; et al. Renin-Angiotensin System Inhibition and Lower 30-Day All-Cause Readmission in Medicare Beneficiaries with Heart Failure. Am. J. Med. 2016, 129, 1067–1073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, J.N.; Tognoni, G.; Valsartan Heart Failure Trial, I. A randomized trial of the angiotensin-Receptor blocker valsartan in chronic heart failure. New Engl. J. Med. 2001, 345, 1667–1675. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Pfeffer, M.A.; Swedberg, K.; Granger, C.B.; Held, P.; McMurray, J.J.; Michelson, E.L.; Olofsson, B.; Ostergren, J.; Investigators, C.; et al. Effects of candesartan in patients with chronic heart failure and preserved left-Ventricular ejection fraction: The CHARM-Preserved Trial. Lancet 2003, 362, 777–781. [Google Scholar] [CrossRef]
- Massie, B.M.; Carson, P.E.; McMurray, J.J.; Komajda, M.; McKelvie, R.; Zile, M.R.; Anderson, S.; Donovan, M.; Iverson, E.; Staiger, C.; et al. Irbesartan in patients with heart failure and preserved ejection fraction. New Engl. J. Med. 2008, 359, 2456–2467. [Google Scholar] [CrossRef] [Green Version]
- Metra, M.; Cleland, J.G.; Weatherley, B.D.; Dittrich, H.C.; Givertz, M.M.; Massie, B.M.; O′Connor, C.M.; Ponikowski, P.; Teerlink, J.R.; Voors, A.A.; et al. Dyspnoea in patients with acute heart failure: An analysis of its clinical course, determinants, and relationship to 60-day outcomes in the PROTECT pilot study. Eur. J. Heart Fail. 2010, 12, 499–507. [Google Scholar] [CrossRef]
- Metra, M.; Teerlink, J.R.; Felker, G.M.; Greenberg, B.H.; Filippatos, G.; Ponikowski, P.; Teichman, S.L.; Unemori, E.; Voors, A.A.; Weatherley, B.D.; et al. Dyspnoea and worsening heart failure in patients with acute heart failure: Results from the Pre-RELAX-AHF study. Eur. J. Heart Fail. 2010, 12, 1130–1139. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Not Readmitted within 30-Days (n = 317) | Readmitted within 30-Days (n = 128) | p-Value |
|---|---|---|---|
| Mean age | 69 ± 12 | 67 ± 12 | 0.250 |
| Female (%) | 184 | 86 | 0.393 |
| Echocardiographic data | |||
| Left ventricular ejection fraction (LVEF) | 57 ± 9.7% | 58 ± 9.9 % | 0.185 |
| Pulmonary artery pressure | 44 ± 17.7 mmHg | 42 ± 15.2 mmHg | 0.399 |
| E/e’ ratio | 16.33 ± 8.2 | 15.14 ± 7.7 | 0.223 |
| Body Mass Index | 37.42 (15.48) | 35.72 (12.56) | 0.260 |
| Medical comorbidities (%) | |||
| Myocardial infarction | 71 | 23 | 0.165 |
| Hypertension | 141 | 60 | 0.843 |
| Hyperlipidemia | 130 | 62 | 0.437 |
| Obstructive sleep apnea | 118 | 45 | 0.345 |
| Atrial Fibrillation | 109 | 41 | 0.330 |
| Diabetes without complication | 130 | 51 | 0.417 |
| Diabetes with complication | 129 | 54 | 0.755 |
| Chronic Renal disease | 148 | 66 | 0.823 |
| Chronic lung disease | 193 | 92 | 0.241 |
| Peripheral artery disease | 30 | 8 | 0.194 |
| Tobacco use | 62 | 21 | 0.270 |
| Medication Class | Not Readmitted within 30-Days (n = 317) | Readmitted within 30-Days (n = 128) | p-Value |
|---|---|---|---|
| Angiotensin-converting enzyme inhibitors (ACEI) | 87 (27%) | 28 (20%) | 0.106 |
| Angiotensin receptor blocker (ARB) | 21 (7%) | 8 (6%) | 0.740 |
| Beta blockers (BB) | 214 (68%) | 85 (62%) | 0.22 |
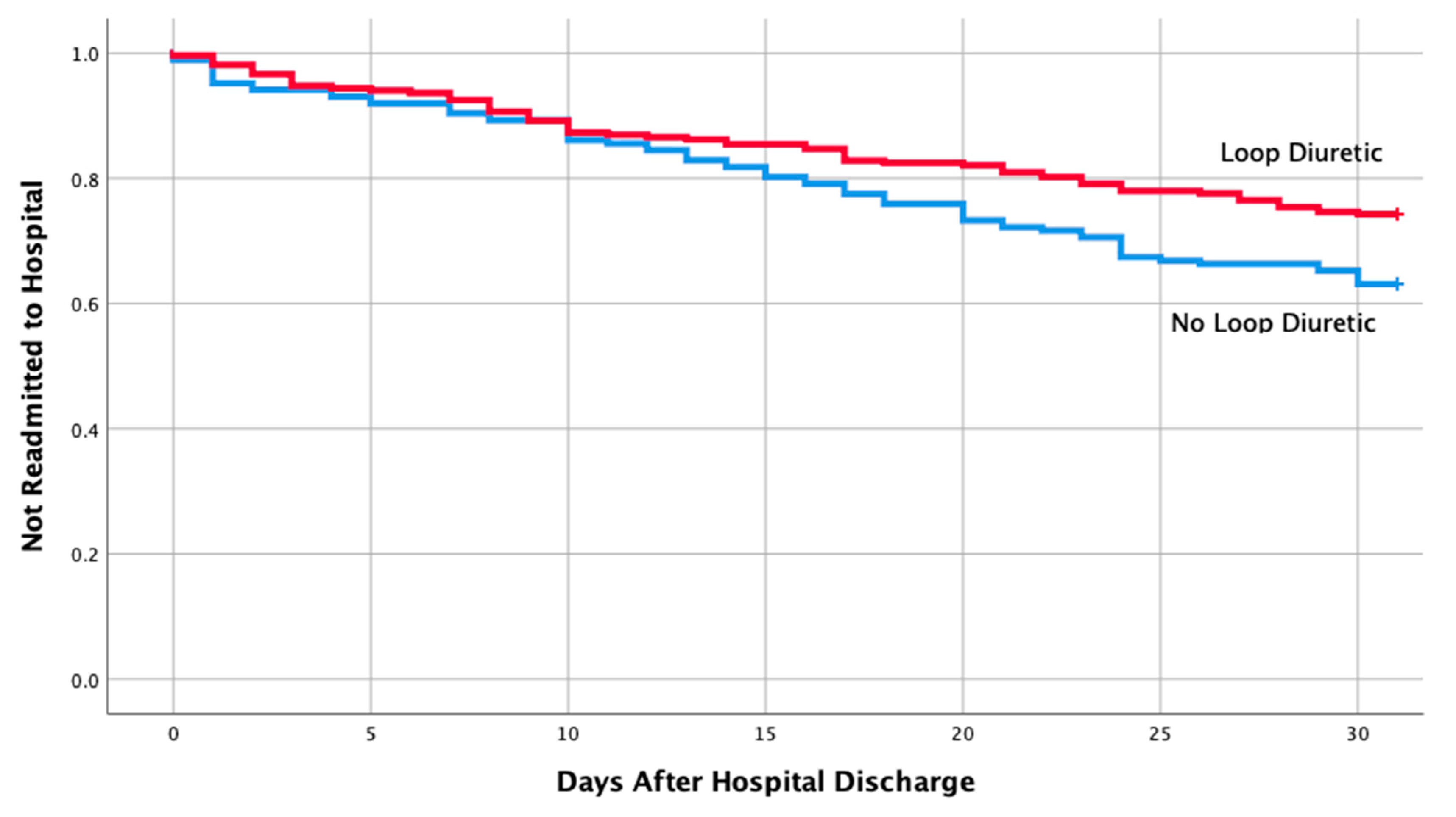
| Loop diuretics (Loop) | 199 (63%) | 69 (50%) | 0.011 |
| Aldosterone receptor antagonists (Spironolactone) | 19 (6%) | 9 (7%) | 0.829 |
| Loop + ACEI | 61 (19%) | 20 (15%) | 0.223 |
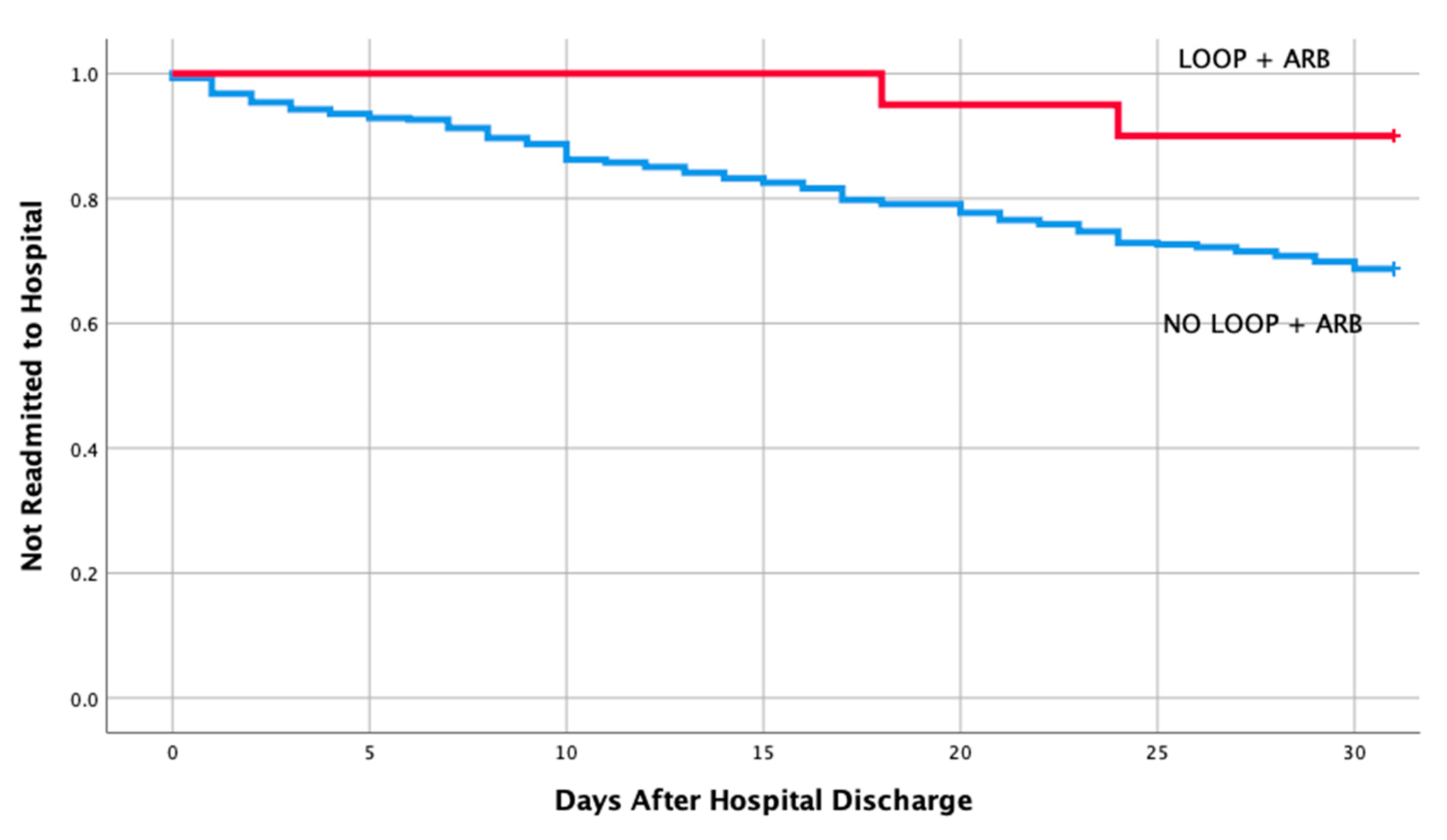
| Loop + ARB | 18 (6%) | 2 (1%) | 0.043 |
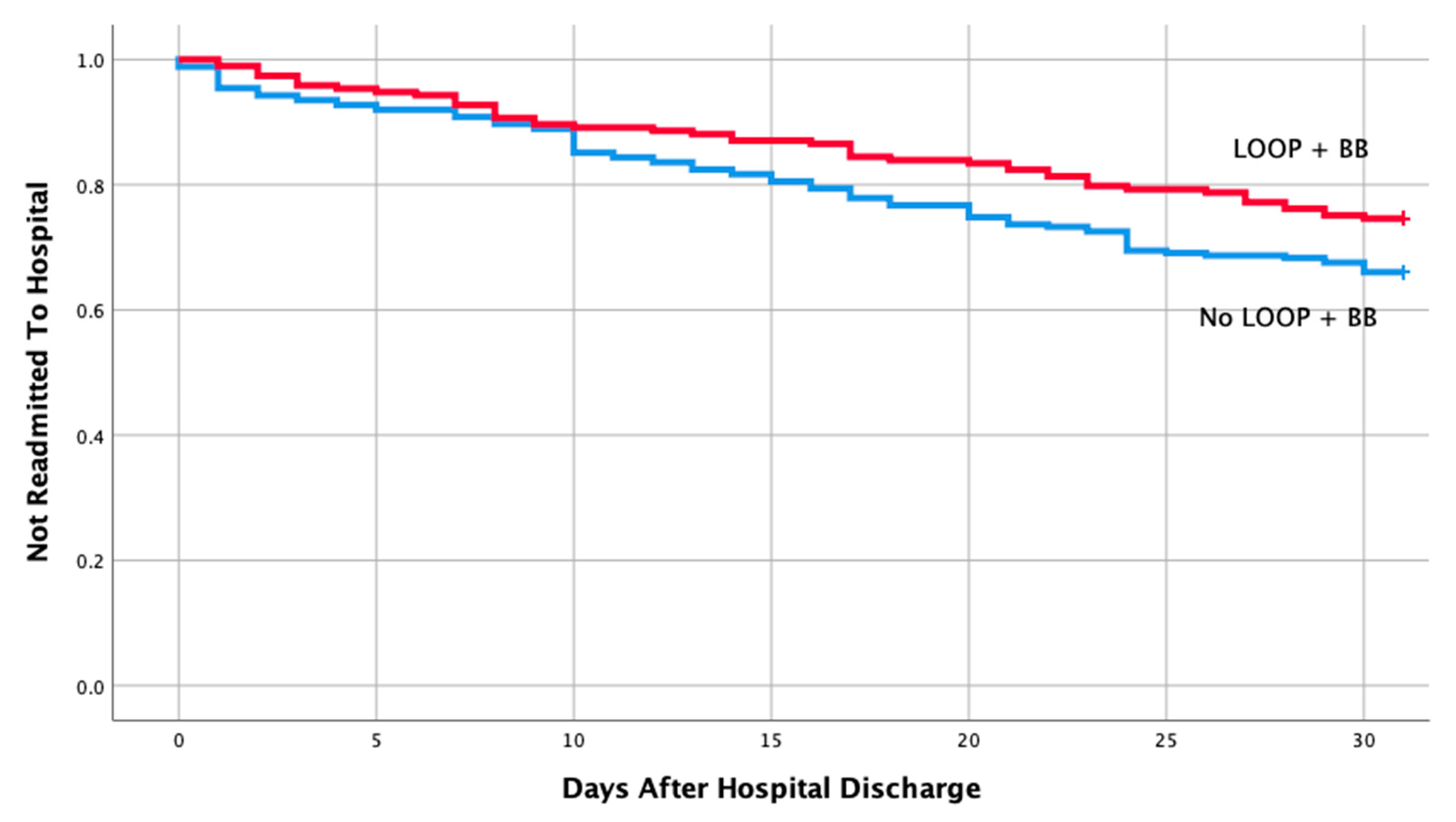
| Loop + BB | 144 (45%) | 49 (36%) | 0.049 |
| Loop + Spironolactone | 17 (5%) | 8 (6%) | 0.852 |
| Loop + BB + ACEI | 49 (16%) | 19 (14%) | 0.642 |
| Loop + BB + ARB | 15 (5%) | 2 (1 %) | 0.90 |
| Loop + ACEI + Spironolactone | 7 (2%) | 0 (0) | 0.79 |
| Loop + ARB + Spironolactone | 1 (1%) | 0 (0) | 0.59 |
| Loop + BB + Spironolactone | 13 (4%) | 4 (3%) | 0.534 |
| Loop + BB + ACEI + Spironolactone | 6 (2%) | 0 (0) | 0.104 |
| Loop + BB + ARB + Spironolactone | 1 (1%) | 0 (0) | 0.509 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parajuli, P.; Lara-Garcia, O.E.; Regmi, M.R.; Skoza, W.; Bhattarai, M.; Kulkarni, A.; Robinson, R.L. Heart Failure Drug Class Effects on 30-Day Readmission Rates in Patients with Heart Failure with Preserved Ejection Fraction: A Retrospective Single Center Study. Medicines 2020, 7, 30. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7050030
Parajuli P, Lara-Garcia OE, Regmi MR, Skoza W, Bhattarai M, Kulkarni A, Robinson RL. Heart Failure Drug Class Effects on 30-Day Readmission Rates in Patients with Heart Failure with Preserved Ejection Fraction: A Retrospective Single Center Study. Medicines. 2020; 7(5):30. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7050030
Chicago/Turabian StyleParajuli, Priyanka, Odalys Estefania Lara-Garcia, Manjari Rani Regmi, Warren Skoza, Mukul Bhattarai, Abhishek Kulkarni, and Robert Leonard Robinson. 2020. "Heart Failure Drug Class Effects on 30-Day Readmission Rates in Patients with Heart Failure with Preserved Ejection Fraction: A Retrospective Single Center Study" Medicines 7, no. 5: 30. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7050030