Recurrent Superior Vena Cava Syndrome in a Patient with Sarcoidosis and Pancreatic Adenocarcinoma: A Case Report and Literature Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
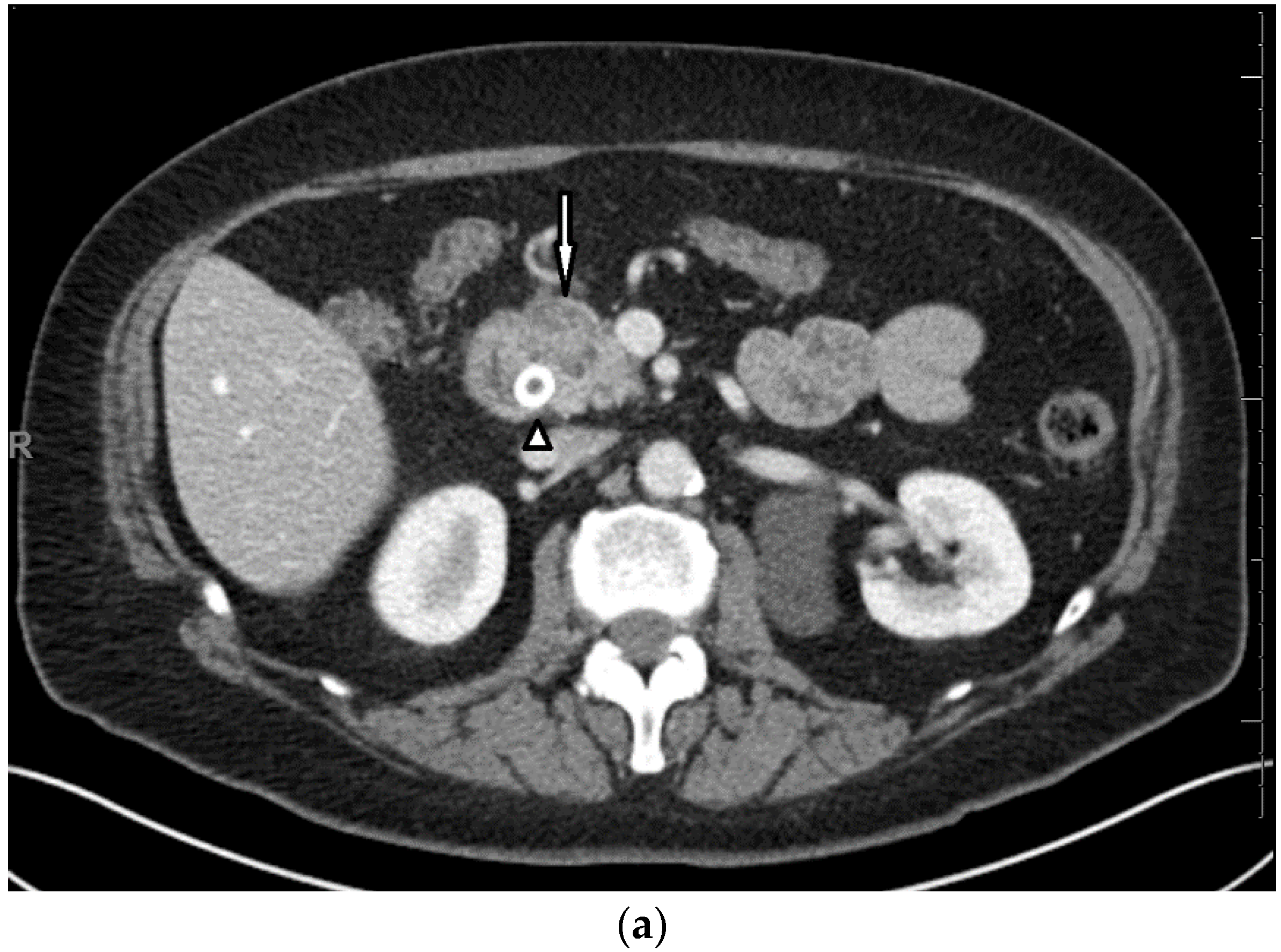
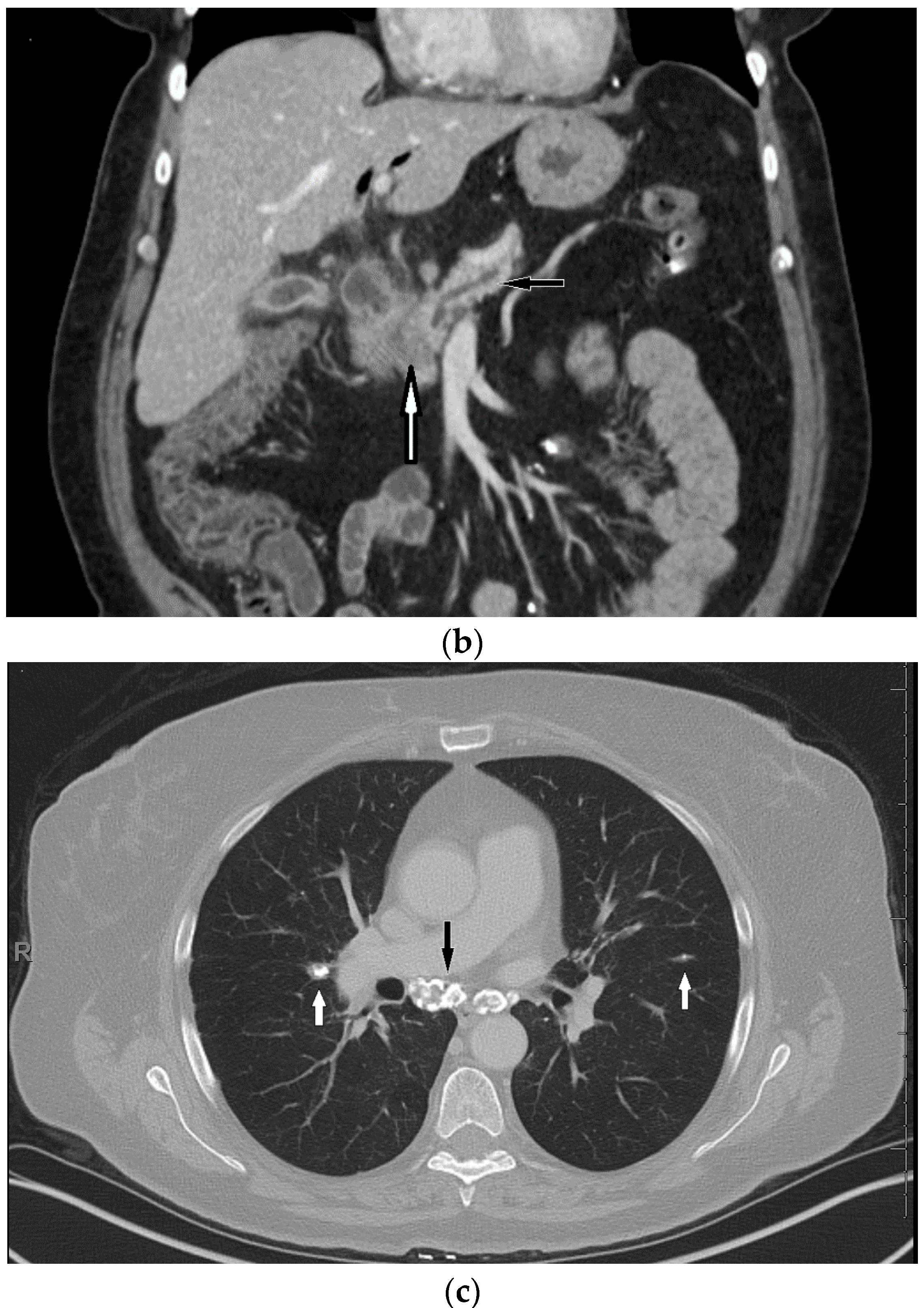
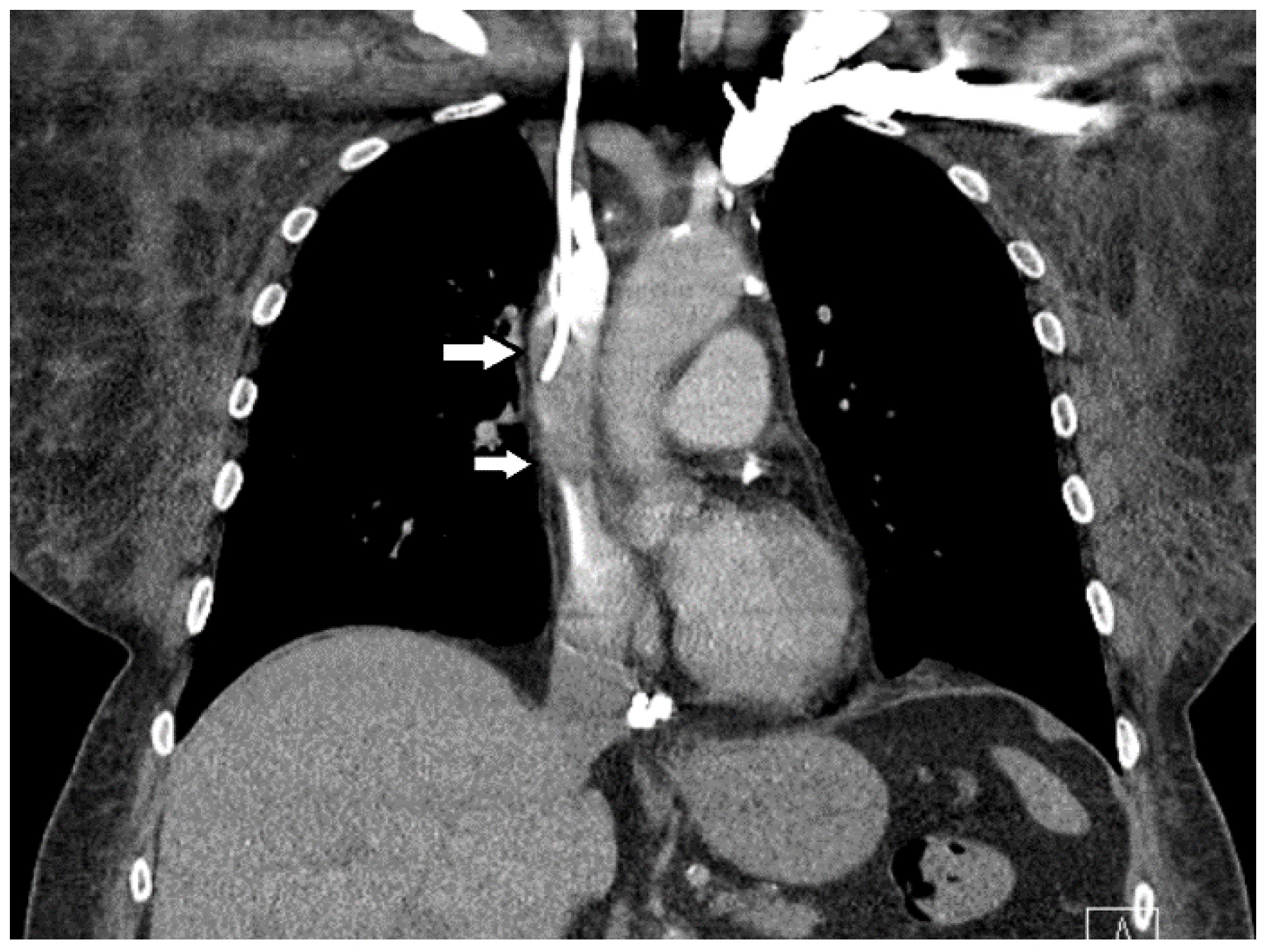
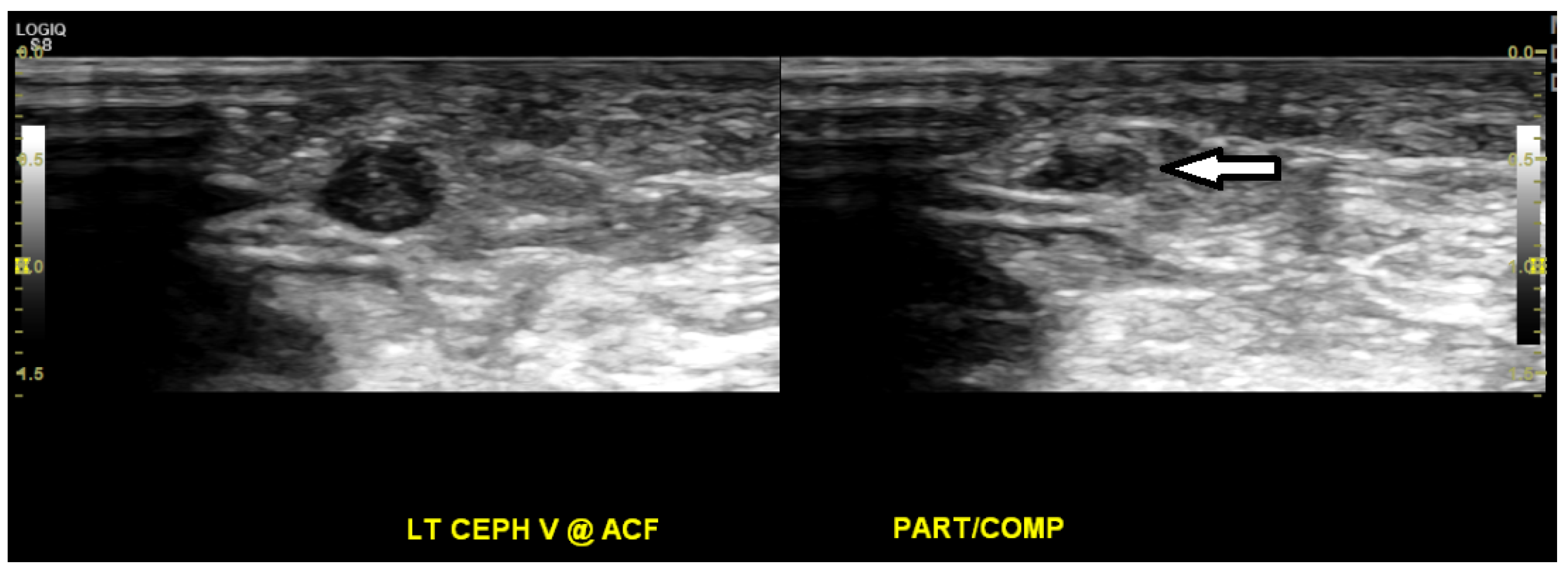
3. Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cheng, S. Superior vena cava syndrome. Cardiol. Rev. 2009, 17, 16–23. [Google Scholar] [CrossRef]
- Khan, U.A.; Shanholtz, C.B.; McCurdy, M.T. Oncologic mechanical emergencies. Hematol. Clin. 2017, 31, 927–940. [Google Scholar] [CrossRef] [PubMed]
- Morgans, W.E.; Al-Jilahawi, A.N.; Mbatha, P.B. Superior vena caval obstruction caused by sarcoidosis. Thorax 1980, 35, 397–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radke, J.R.; Kaplan, H.; Conway, W.A. The significance of superior vena cava syndrome developing in a patient with sarcoidosis. Radiology 1980, 134, 311–312. [Google Scholar] [CrossRef] [PubMed]
- Brandstetter, R.; Hansen, D.; Jarowski, C.; King, T.; Barletta, A. Superior vena cava syndrome as the initial clinical manifestation of sarcoidosis. Heart Lung J. Crit. Care 1981, 10, 101–104. [Google Scholar]
- Case Records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 11-1984. Long-standing sarcoidosis with the recent onset of the superior-vena-cava syndrome. N. Engl. J. Med. 1984, 310, 708–716. [Google Scholar] [CrossRef]
- McPherson, J.G., III; Yeoh, C.B. Rare manifestations of sarcoidosis. J. Natl. Med. Assoc. 1993, 85, 869–872. [Google Scholar]
- Ghorbani, H.; Vakili Sadeghi, M.; Hejazian, T.; Sharbatdaran, M. Superior vena cava syndrome as a paraneoplastic manifestation of soft tissue sarcoma. Hematol. Transfus. Cell Ther. 2018, 40, 75–78. [Google Scholar] [CrossRef]
- Santra, A.; Nandi, S.; Mondal, S.; Chakraborty, S. Superior vena cava syndrome due to thrombosis: A rare paraneoplastic presentation of bronchogenic carcinoma. Iran. J. Med. Sci. 2016, 41, 354–358. [Google Scholar]
- Takeda, T.; Saitoh, M.; Takeda, S. Superior Vena Cava Syndrome Caused by an Intravascular Thrombosis Due to Underlying Prostate Carcinoma. Intern. Med. 2008, 47, 2007–2010. [Google Scholar] [CrossRef] [Green Version]
- May, M.; Seehafer, M.; Helke, C.; Uberruck, T.; Gunia, S.; Hoschke, B. V.-cava-superior-syndrom mit beidseitiger jugularis- und subklaviavenenthrombose. Der Urol. A 2003, 42, 1374–1377. [Google Scholar] [CrossRef] [PubMed]
- Padovani, M.; Tillie-Leblond, I.; Vennin, P.; Demarcq, G.; Wallaert, B. Paraneoplastic superior vena cava thrombosis disclosing an ovarian tumor. Rev. Mal. Respir. 1996, 13, 598–600. [Google Scholar] [PubMed]
- Ungprasert, P.; Crowson, C.S.; Matteson, E.L. Risk of malignancy among patients with sarcoidosis: A population-based cohort study. Arthritis Care Res. 2017, 69, 46–50. [Google Scholar] [CrossRef] [Green Version]
- Maradona Hidalgo, J.A.; Alvarez Alvarez, C.; Fernández Rippe, M.L.; Suárez García, E.; Soler Sánchez, T. Sarcoidosis, pancreatic adenocarcinoma and granulomas of undetermined origin in a patient with xeroderma pigmentosum. Rev. Clin. Esp. 1983, 168, 357–360. [Google Scholar] [PubMed]
- Mao, J.T.; Fisnbein, M.C. Metastatic pancreatic cancer masquerading as pulmonary sarcoidosis. Am. J. Med. 2000, 109, 598–599. [Google Scholar] [CrossRef]
- Goto, T.; Toyama, H.; Asari, S.; Terai, S.; Mukubou, H.; Shirakawa, S.; Nanno, Y.; Mizumoto, T.; Kinoshita, H.; Tanaka, M.; et al. A case of pancreatic cancer with multiple lymph node swelling caused by sarcoidosis. Gan Kagaku Ryoho. 2017, 44, 1886–1888. [Google Scholar]
- Gupta, K.; Hassan, T.; Rizwan, S.; Hans, B.; Jawale, R.; Desilets, D. Hepatic sarcoidosis complicated with pancreatic adenocarcinoma. Case Rep. Hepatol. 2019, 2019, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, C.J.; Morinaga, L.T.K.; Alves, J.L.; Castro, M.A.; Calderaro, D.; Jardim, C.V.P.; Souza, R. Cancer-associated thrombosis: The when, how and why. Eur. Respir. Rev. 2019, 28, 180119. [Google Scholar] [CrossRef] [Green Version]
- Rømer, F.K.; Hommelgaard, P.; Schou, G. Sarcoidosis and cancer revisited: A long-term follow-up study of 555 Danish sarcoidosis patients. Eur. Respir. J. 1998, 12, 906–912. [Google Scholar] [CrossRef] [Green Version]
- Askling, J.; Grunewald, J.; Eklund, A.; Hillerdal, G.; Ekbom, A. Increased risk for cancer following sarcoidosis. Am. J. Respir. Crit. Care Med. 1999, 160, 1668–1672. [Google Scholar] [CrossRef]
- Ji, J.; Shu, X.; Li, X.; Sundquist, K.; Sundquist, J.; Hemminki, K. Cancer risk in hospitalized sarcoidosis patients: A follow-up study in Sweden. Ann. Oncol. 2009, 20, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Le Jeune, I.; Gribbin, J.; West, J.; Smith, C.; Cullinan, P.; Hubbard, R. The incidence of cancer in patients with idiopathic pulmonary fibrosis and sarcoidosis in the UK. Respir. Med. 2007, 101, 2534–2540. [Google Scholar] [CrossRef] [Green Version]
- Arkema, E.V.; Cozier, Y.C. Epidemiology of sarcoidosis: Current findings and future directions. Ther. Adv. Chronic Dis. 2018, 9, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, K.K.; Sværke, C.; Thomsen, R.W.; Nørgaard, M. Sarcoidosis and subsequent cancer risk: A Danish nationwide cohort study. Eur. Respir. J. 2015, 45, 269. [Google Scholar] [CrossRef] [Green Version]
- Gordonson, J.; Trachtenberg, S.; Sargent, E.N. Superior vena cava obstruction due to sarcoidosis. Chest 1973, 63, 292–293. [Google Scholar] [CrossRef] [PubMed]
- Bonifazi, M.; Bravi, F.; Gasparini, S.; La Vecchia, C.; Gabrielli, A.; Wells, A.U.; Renzoni, E.A. Sarcoidosis and cancer risk: Systematic review and meta-analysis of observational studies. Chest 2015, 147, 778–791. [Google Scholar] [CrossRef] [PubMed]
- Geremek, A.G.; Tomkowski, W.; Geremek, M.; Puścińska, E.; Małek, G.; Nowiński, A.; Bednarek, M.; Śliwiński, P. Sarcoidosis as a risk factor for venous thromboembolism. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 2017, 34, 170–178. [Google Scholar] [CrossRef]
- Goljan-Geremek, A.; Geremek, M.; Puscinska, E.; Sliwinski, P. Venous thromboembolism and sarcoidosis: Co-incidence or coexistence? Cent. J. Immunol. 2015, 40, 477–480. [Google Scholar] [CrossRef]
- Hathcock, J.J. Flow effects on coagulation and thrombosis. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1729–1737. [Google Scholar] [CrossRef]
- Gerke, A.K. Morbidity and mortality in sarcoidosis. Curr. Opin. Pulm. Med. 2014, 20, 472–478. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Malignant disease | Age | Sex | Clinical Presentation of SVC Syndrome | Diagnosis of SVC Syndrome | Management | Reference |
|---|---|---|---|---|---|---|
| Pancreatic Adenocarcinoma | 64 | Female | Dyspnea, facial edema, flushing of neck, fatigue | Physical exam and IV contrast enhanced CT | IV heparin followed by enoxaparin | This Report |
| Soft Tissue Sarcoma | 46 | Female | Dyspnea, right arm pain, dysphagia | Spiral chest CT with contrast | Enoxaparin | [8] |
| Bronchogenic Carcinoma | 55 | Male | Dyspnea, edema of face, neck, and chest | Physical exam and Doppler ultrasonography | Low molecular weight heparin | [9] |
| Prostate Carcinoma | 60 | Male | Facial edema | Physical exam, contrast enhanced CT and MRI | Warfarin | [10] |
| Renal Cell Carcinoma | 54 | Male | Edema of face and neck | CT and MRI | IV Heparin | [11] |
| Ovarian Papillary Carcinoma | 62 | Female | Telangiectasias on face and anterior trunk | Thoracic CT | Acenocoumarol | [12] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shenoy, G.; Kim, Y.; Newmaster, K.; McGillen, K.L.; Ruggiero, F.; Yee, N.S. Recurrent Superior Vena Cava Syndrome in a Patient with Sarcoidosis and Pancreatic Adenocarcinoma: A Case Report and Literature Review. Medicines 2020, 7, 56. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7090056
Shenoy G, Kim Y, Newmaster K, McGillen KL, Ruggiero F, Yee NS. Recurrent Superior Vena Cava Syndrome in a Patient with Sarcoidosis and Pancreatic Adenocarcinoma: A Case Report and Literature Review. Medicines. 2020; 7(9):56. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7090056
Chicago/Turabian StyleShenoy, Ganesh, Yunsung Kim, Kyra Newmaster, Kathryn L. McGillen, Francesca Ruggiero, and Nelson S. Yee. 2020. "Recurrent Superior Vena Cava Syndrome in a Patient with Sarcoidosis and Pancreatic Adenocarcinoma: A Case Report and Literature Review" Medicines 7, no. 9: 56. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7090056