Primary Small Cell Carcinoma of the Kidney: Disease Characteristics and Treatment Outcomes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
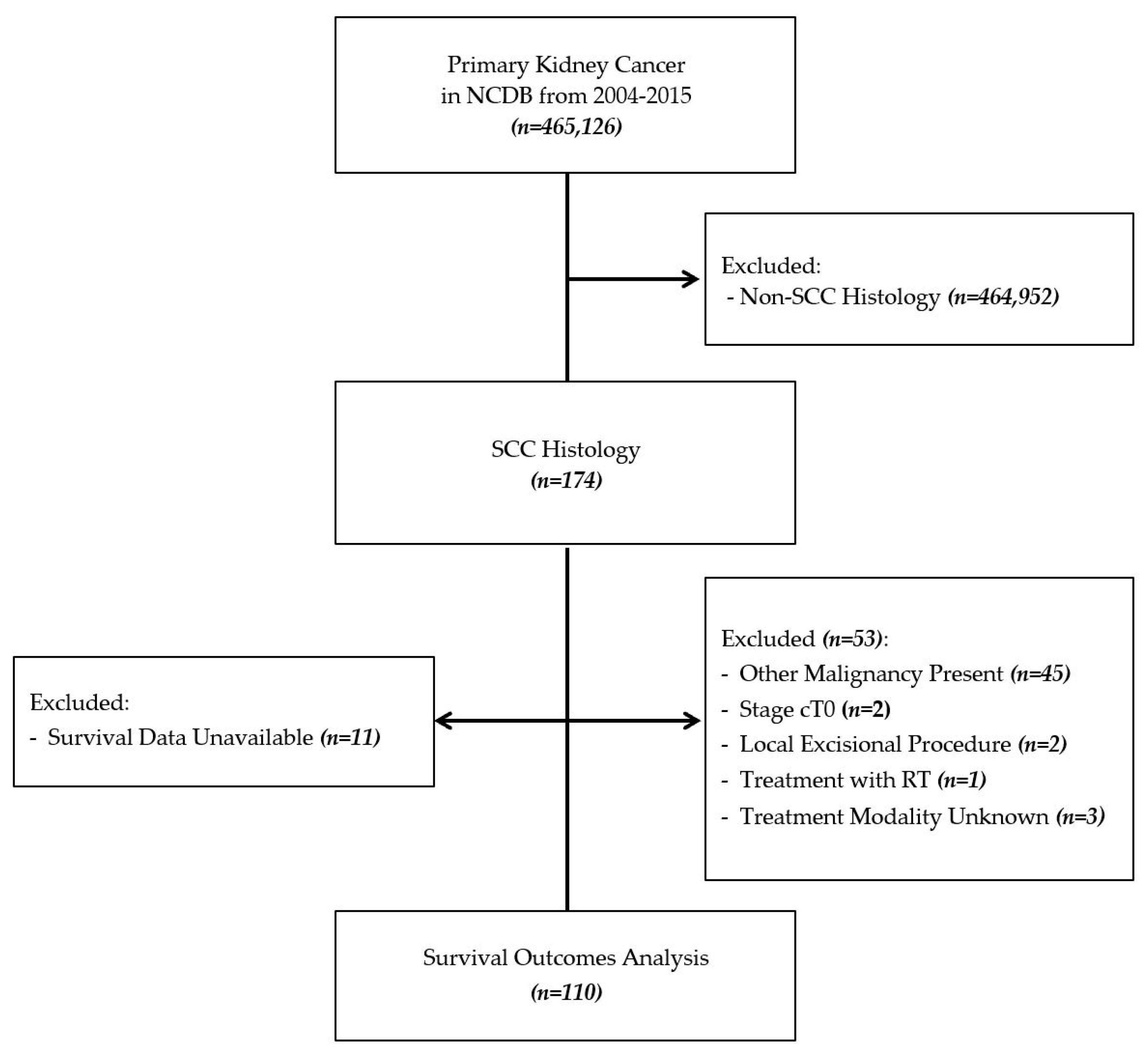
2.1. Data Source
2.2. Patient Selection
2.3. Variables
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Predictors of Mortality
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levenson, R.M.; Ihde, D.C.; Matthews, M.J.; Cohen, M.H.; Bunn, P.A.; Minna, J.D.; Gazdar, A.F. Small Cell Carcinoma Presenting as an Extrapulmonary Neoplasm: Sites of Origin and Response to Chemotherapy2. J. Natl. Cancer Inst. 1981, 67, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.F.; Aikawa, M.; Cebelin, M. Neurosecretory granules in small cell invasive carcinoma of the urinary bladder. Cancer 1981, 47, 724–730. [Google Scholar] [CrossRef]
- Ahmed, S.; Neufeld, S.; Kroczak, T.J.; Bashir, B.; Ahmed, N.; Czaykowski, P.; Aljada, I.; Koul, R.; Galloway, K.; Drachenberg, D.E. Small Cell Cancer of the Bladder and Prostate: A Retrospective Review from a Tertiary Cancer Center. Cureus 2015, 7, e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oesterling, J.E.; Brendler, C.B.; Burgers, J.K.; Marshall, F.F.; Epstein, J.I. Advanced small cell carcinoma of the bladder successful treatment with combined radical cystoprostatectomy and adjuvant methotrexate, vinblastine, doxorubicin, and cisplatin chemotherapy. Cancer 1990, 65, 1928–1936. [Google Scholar] [CrossRef]
- Nadal, R.; Schweizer, M.T.; Kryvenko, O.N.; Epstein, J.I.; Eisenberger, M.A. Small cell carcinoma of the prostate. Nat. Rev. Urol. 2014, 11, 213–219. [Google Scholar] [CrossRef]
- Cheng, L.; Jones, T.D.; McCarthy, R.P.; Eble, J.N.; Wang, M.; MacLennan, G.T.; Lopez-Beltran, A.; Yang, X.J.; Koch, M.O.; Zhang, S.; et al. Molecular Genetic Evidence for a Common Clonal Origin of Urinary Bladder Small Cell Carcinoma and Coexisting Urothelial Carcinoma. Am. J. Pathol. 2005, 166, 1533–1539. [Google Scholar] [CrossRef] [Green Version]
- Rastelli, G.; Bertolini, F.; Sartori, G.; Bigiani, N.; Cavazza, A.; Foroni, M.; Valli, R.; Rindi, G.; De Gaetani, C.; Luppi, G. Primary Mixed Adenocarcinoma and Small Cell Carcinoma of the Appendix. Am. J. Surg. Pathol. 2004, 28, 1233–1239. [Google Scholar] [CrossRef]
- Terracciano, L.; Richter, J.; Tornillo, L.; Beffa, L.; Maurer, R.; Gasser, T.C.; Moch, H.; Mihatsch, M.J.; Sauter, G. Chromosomal imbalances in small cell carcinomas of the urinary bladder. J. Pathol. 1999, 189, 230–235. [Google Scholar] [CrossRef]
- Yuan, T.-C.; Veeramani, S.; Lin, M.-F. Neuroendocrine-like prostate cancer cells: Neuroendocrine transdifferentiation of prostate adenocarcinoma cells. Endocr. Relat. Cancer 2007, 14, 531–547. [Google Scholar] [CrossRef]
- Si, Q.; Dancer, J.; Stanton, M.L.; Tamboli, P.; Ro, J.Y.; Czerniak, B.A.; Shen, S.S.; Guo, C.C. Small cell carcinoma of the kidney: A clinicopathologic study of 14 cases. Hum. Pathol. 2011, 42, 1792–1798. [Google Scholar] [CrossRef]
- Teegavarapu, P.S.; Rao, P.; Matrana, M.R.; Cauley, D.H.; Wood, C.G.; Tannir, N.M. Neuroendocrine Tumors of the Kidney: A Single Institution Experience. Clin. Genitourin. Cancer 2014, 12, 422–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.-P.; Chen, B.; Sun, X.-Z.; Guo, Y.; Yang, S.-C.; Deng, C.-H.; Huang, Y.-R. High-grade Neuroendocrine Carcinoma With Focal Squamous Metaplasia of Renal Pelvis Associated With Renal Calculus: Study of a Case. Urol. Case Rep. 2014, 2, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majhail, N.S.; Elson, P.; Bukowski, R.M. Therapy and outcome of small cell carcinoma of the kidney. Cancer 2003, 97, 1436–1441. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.; Hsu, H.-H.; Lin, H.-Y.; Chen, Y.-C.; Wong, Y.-C.; Wang, L.-J.; Ng, K.-F.; Chuang, C.-K.; Hung, C.-C.; Yang, C.-W. Factors associated with the survival of patients with primary small cell carcinoma of the kidney. Int. J. Clin. Oncol. 2011, 18, 139–147. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y. The National Cancer Data Base: A Powerful Initiative to Improve Cancer Care in the United States. Ann. Surg. Oncol. 2008, 15, 683–690. [Google Scholar] [CrossRef] [Green Version]
- US Census Bureau. About Race. Available online: http://www.census.gov/topics/population/race/about.html (accessed on 18 December 2020).
- American College of Surgeons Commission on Cancer. About Cancer Program Categories. Available online: https://www.facs.org/quality-programs/cancer/coc/accreditation/categories (accessed on 1 November 2020).
- US Census Bureau. Census Regions and Divisions of the United States. Available online: https://www2.census.gov/geo/pdfs/maps-data/maps/reference/us_regdiv.pdf (accessed on 1 November 2020).
- Xu, J.-L.; Guo, Y. Clinical characteristics and survival of extrapulmonary small cell carcinoma in 11 different primary tumor sites in the United States, 1975–2016. Curr. Med. Res. Opin. 2020, 23, 1–18. [Google Scholar] [CrossRef]
- Chu, C.; Hu, C.-Y.; Batra, R.; Lin, A.Y. Small cell carcinoma of the kidney: A case report and analysis of data from the Surveillance, Epidemiology, and End Results registry. J. Med. Case Rep. 2019, 13, 71. [Google Scholar] [CrossRef]
- Lerro, C.C.; Robbins, A.S.; Phillips, J.L.; Stewart, A.K. Comparison of Cases Captured in the National Cancer Data Base with Those in Population-based Central Cancer Registries. Ann. Surg. Oncol. 2013, 20, 1759–1765. [Google Scholar] [CrossRef]
- Cheung, M.C.; Hamilton, K.; Sherman, R.; Byrne, M.M.; Nguyen, D.M.; Franceschi, D.; Koniaris, L.G. Impact of Teaching Facility Status and High-Volume Centers on Outcomes for Lung Cancer Resection: An Examination of 13,469 Surgical Patients. Ann. Surg. Oncol. 2009, 16, 3–13. [Google Scholar] [CrossRef]
- Ayanian, J.Z.; Weissman, J.S. Teaching Hospitals and Quality of Care: A Review of the Literature. Milbank Q. 2002, 80, 569–593. [Google Scholar] [CrossRef] [Green Version]
- Shin, N.W.; Cho, J.; Yang, H.K.; Kim, S.Y.; Lee, S.H.; Suh, B.; Shin, H.-Y.; Lee, H.J.; Kim, D.G.; Park, J.-H. Oncologist Perspectives on Rare Cancer Care: A Nationwide Survey. Cancer Res. Treat. 2015, 47, 591–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galanis, E.; Frytak, S.; Lloyd, R.V. Extrapulmonary small cell carcinoma. Cancer 1997, 79, 1729–1736. [Google Scholar] [CrossRef]
- Re, G.L.; Canzonieri, V.; Veronesi, A.; Dal Bo, V.; Barzan, L.; Zancanaro, C.; Trovo, M. Extrapulmonary small cell carcinoma: A single-institution experience and review of the literature. Ann. Oncol. 1994, 5, 909–913. [Google Scholar] [CrossRef] [PubMed]
- Mackey, J.R.; Au, H.-J.; Hugh, J.; Venner, P. Genitourinary Small Cell Carcinoma: Determination of Clinical and Therapeutic Factors Associated with Survival. J. Urol. 1998, 159, 1624–1629. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Kidney Cancer. Version 2.2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf (accessed on 18 December 2020).
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Bladder Cancer. Version 5.2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf (accessed on 18 December 2020).
- Boffa, D.J.; Rosen, J.E.; Mallin, K.; Loomis, A.; Gay, G.; Palis, B.; Thoburn, K.; Gress, D.; McKellar, D.P.; Shulman, L.N.; et al. Using the National Cancer Database for Outcomes Research. JAMA Oncol. 2017, 3, 1722–1728. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Frequency (%) |
|---|---|
| Sex | |
| Male | 58 (52.7) |
| Female | 52 (47.3) |
| Age (years) | |
| 18–39 | 4 (3.6) |
| 40–49 | 8 (7.3) |
| 50–59 | 13 (11.8) |
| 60–69 | 27 (24.5) |
| 70–79 | 31 (28.2) |
| ≥80 | 27 (24.5) |
| Race | |
| Caucasian | 95 (86.4) |
| African-American | 8 (7.3) |
| Hispanic | 4 (3.6) |
| Asian/Pacific Islander | 2 (1.8) |
| Other/Unspecified | 1 (0.9) |
| Insurance Status | |
| Private/Managed Care | 32 (29.1) |
| Not Insured | 1 (0.9) |
| Medicaid | 6 (5.5) |
| Medicare | 64 (58.2) |
| Other Government Insurance | 3 (2.7) |
| Unknown | 4 (3.6) |
| Socioeconomic Status | |
| Low | 37 (33.6) |
| Middle | 32 (29.1) |
| High | 37 (33.6) |
| Unknown | 4 (3.6) |
| Facility Type | |
| Comprehensive Community Cancer Program | 48 (43.6) |
| Community Cancer Program | 11 (10.0) |
| Academic Research Program | 37 (33.6) |
| Integrated Network Cancer Program | 10 (9.1) |
| Censored * | 4 (3.6) |
| Facility Region | |
| South Atlantic | 29 (26.4) |
| New England | 5 (4.5) |
| Middle Atlantic | 9 (8.2) |
| East North Central | 21 (19.1) |
| East South Central | 5 (4.5) |
| West North Central | 9 (8.2) |
| West South Central | 8 (7.3) |
| Mountain | 7 (6.4) |
| Pacific | 13 (11.8) |
| Censored * | 4 (3.6) |
| Characteristic | Frequency (%) |
|---|---|
| Clinical T Stage | |
| cT1 | 14 (12.7) |
| cT2 | 8 (7.3) |
| cT3 | 16 (14.5) |
| cT4 | 13 (11.8) |
| cT unspecified | 59 (53.6) |
| Clinical N Stage | |
| cN0 | 27 (24.5) |
| cN1 | 30 (27.3) |
| cN2 | 4 (3.6) |
| cN unspecified | 49 (44.5) |
| Clinical M Stage | |
| cM0 | 55 (50.0) |
| cM1 | 51 (46.4) |
| cM unspecified | 4 (3.6) |
| Treatment | |
| No Treatment | 24 (21.8) |
| Chemotherapy | 19 (17.3) |
| Surgery | 29 (26.4) |
| Chemotherapy + Surgery | 22 (20.0) |
| Chemoradiotherapy | 12 (10.9) |
| Chemoradiation + Surgery | 4 (3.6) |
| Predictor | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Sex | ||
| Male | 1 (Reference) | ---- |
| Female | 2.02 (1.02–3.99) | 0.043 * |
| Age (years) | ||
| 50–59 | 1 (Reference) | ---- |
| 18–39 | 0.90 (0.14–5.69) | 0.912 |
| 40–49 | 0.58 (0.10–3.46) | 0.550 |
| 60–69 | 3.50 (1.08–11.35) | 0.037 * |
| 70–79 | 1.07 (0.27–4.16) | 0.923 |
| ≥80 | 2.62 (0.68–10.04) | 0.161 |
| Race | ||
| Caucasian | 1 (Reference) | ---- |
| African-American | 1.00 (0.27–3.70) | 0.996 |
| Hispanic | 2.75 (0.63–12.03) | 0.180 |
| Asian/Pacific Islander | 0.44 (0.02–8.29) | 0.581 |
| Other/Unspecified | 5.66 (0.14–234.76) | 0.362 |
| Insurance Status | ||
| Private/Managed Care | 1 (Reference) | ---- |
| Medicaid | 3.76 (0.85–16.52) | 0.080 |
| Medicare | 1.14 (0.46–2.82) | 0.782 |
| Other Government Insurance | 2.70 (0.25–28.85) | 0.411 |
| Unknown | 0.78 (0.12–5.02) | 0.790 |
| Socioeconomic Status | ||
| Low | 1 (Reference) | ---- |
| Middle | 0.50 (0.21–1.16) | 0.106 |
| High | 0.33 (0.12–0.99) | 0.048 * |
| Unknown | 1.88 (0.33–10.68) | 0.477 |
| Facility Type ** | ||
| Comprehensive Community Cancer Program | 1 (Reference) | ---- |
| Community Cancer Program | 0.44 (0.12–1.56) | 0.202 |
| Academic Research Program | 0.39 (0.19–0.83) | 0.015 * |
| Integrated Network Cancer Program | 2.80 (1.02–7.71) | 0.046 * |
| Facility Region ** | ||
| South Atlantic | 1 (Reference) | ---- |
| New England | 1.03 (0.22–4.73) | 0.970 |
| Middle Atlantic | 3.03 (0.65–14.17) | 0.159 |
| East North Central | 2.39 (0.92–6.22) | 0.075 |
| East South Central | 0.69 (0.12–3.98) | 0.682 |
| West North Central | 1.70 (0.34–8.45) | 0.520 |
| West South Central | 0.34 (.09–1.25) | 0.104 |
| Mountain | 1.28 (0.33–4.92) | 0.720 |
| Pacific | 1.76 (0.55–5.67) | 0.343 |
| Clinical T Stage | ||
| cT1 | 1 (Reference) | ---- |
| cT2 | 0.77 (0.13–4.46) | 0.770 |
| cT3 | 0.71 (0.21–2.37) | 0.573 |
| cT4 | 1.25 (0.35–4.49) | 0.737 |
| cT unspecified | 0.73 (0.24–2.24) | 0.577 |
| Clinical N Stage | ||
| cN0 | 1 (Reference) | ---- |
| cN1 | 2.46 (1.00–6.04) | 0.050 |
| cN2 | 0.60 (0.08–4.48) | 0.618 |
| cN unspecified | 1.42 (0.53–3.81) | 0.490 |
| Clinical M Stage | ||
| cM0 | 1 (Reference) | ---- |
| cM1 | 2.23 (1.03–4.83) | 0.043 * |
| cM unspecified | 2.33 (0.39–13.99) | 0.357 |
| Treatment | ||
| Chemotherapy | 1 (Reference) | ---- |
| No Treatment | 3.30 (1.21–9.05) | 0.020 * |
| Surgery | 1.79 (0.49–6.48) | 0.378 |
| Chemotherapy + Surgery | 0.90 (0.35–2.31) | 0.818 |
| Chemoradiotherapy | 2.07 (0.76–5.64) | 0.153 |
| Chemoradiation + Surgery | 0.29 (0.04–2.16) | 0.228 |
| Treatment | Estimate | Std. Error | 95% Confidence Interval |
|---|---|---|---|
| Chemotherapy alone | 10.020 | 1.429 | 7.219–12.821 |
| Surgery alone | 9.000 | 6.118 | 0.000–20.992 |
| Surgery + Chemotherapy | 13.500 | 2.081 | 9.421–17.579 |
| Chemoradiotherapy | 9.360 | 1.481 | 6.457–12.263 |
| Surgery + Chemoradiotherapy | 12.650 | --- | --- |
| Overall | 10.280 | 1.289 | 7.754–12.806 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monaghan, T.F.; Michelson, K.P.; Suss, N.R.; Agudelo, C.W.; Rahman, S.N.; Robins, D.J.; Flores, V.X.; McNeil, B.K.; Weiss, J.P.; Winer, A.G. Primary Small Cell Carcinoma of the Kidney: Disease Characteristics and Treatment Outcomes. Medicines 2021, 8, 6. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8010006
Monaghan TF, Michelson KP, Suss NR, Agudelo CW, Rahman SN, Robins DJ, Flores VX, McNeil BK, Weiss JP, Winer AG. Primary Small Cell Carcinoma of the Kidney: Disease Characteristics and Treatment Outcomes. Medicines. 2021; 8(1):6. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8010006
Chicago/Turabian StyleMonaghan, Thomas F., Kyle P. Michelson, Nicholas R. Suss, Christina W. Agudelo, Syed N. Rahman, Dennis J. Robins, Viktor X. Flores, Brian K. McNeil, Jeffrey P. Weiss, and Andrew G. Winer. 2021. "Primary Small Cell Carcinoma of the Kidney: Disease Characteristics and Treatment Outcomes" Medicines 8, no. 1: 6. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8010006