
Clinical Significance of Gamma-Glutamyltranspeptidase Combined with Carbohydrate-Deficient Transferrin for the Assessment of Excessive Alcohol Consumption in Patients with Alcoholic Cirrhosis

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
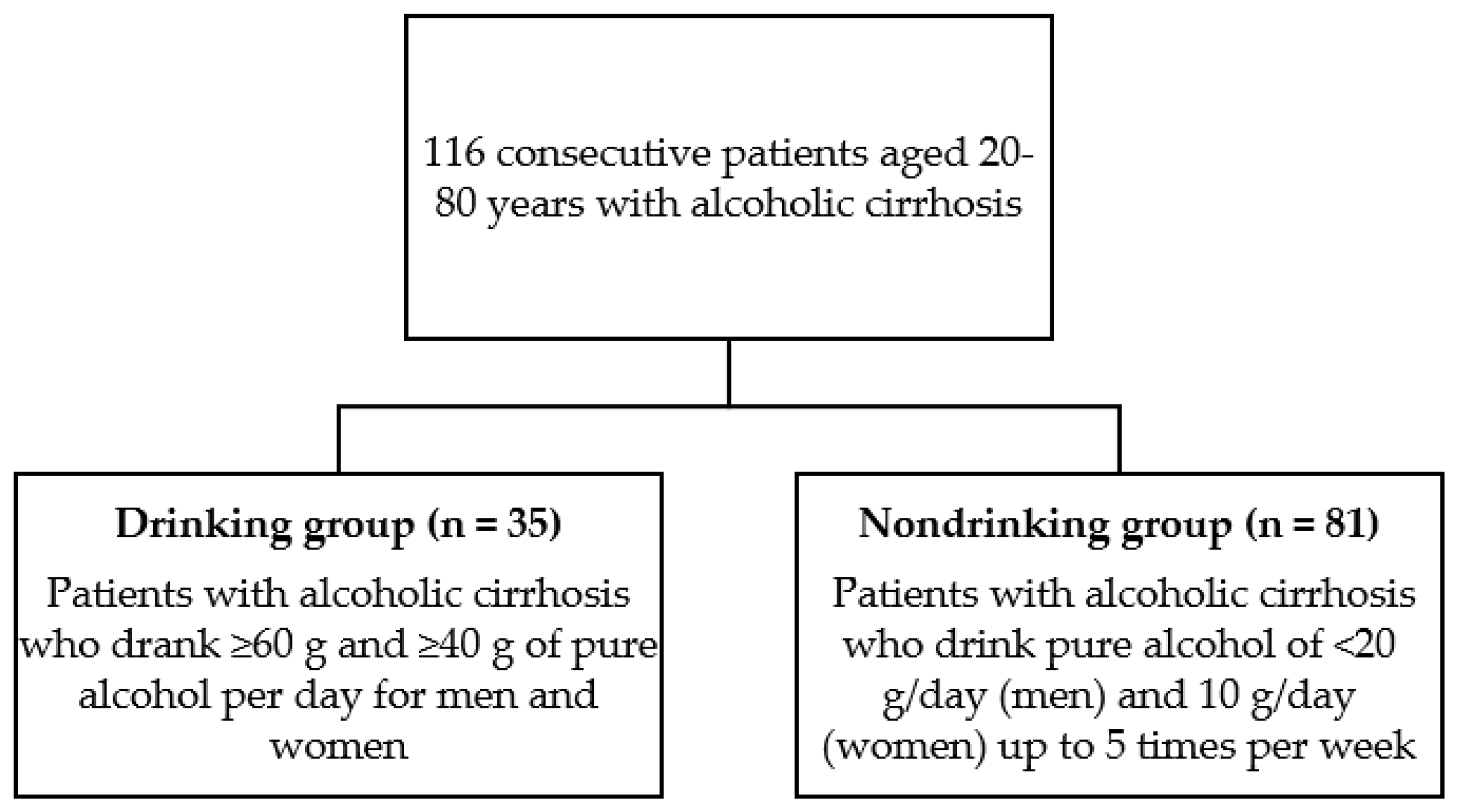
2.1. Patients
2.2. CDT and Biochemical Parameter Measurements
2.3. Statistical Analysis
3. Results
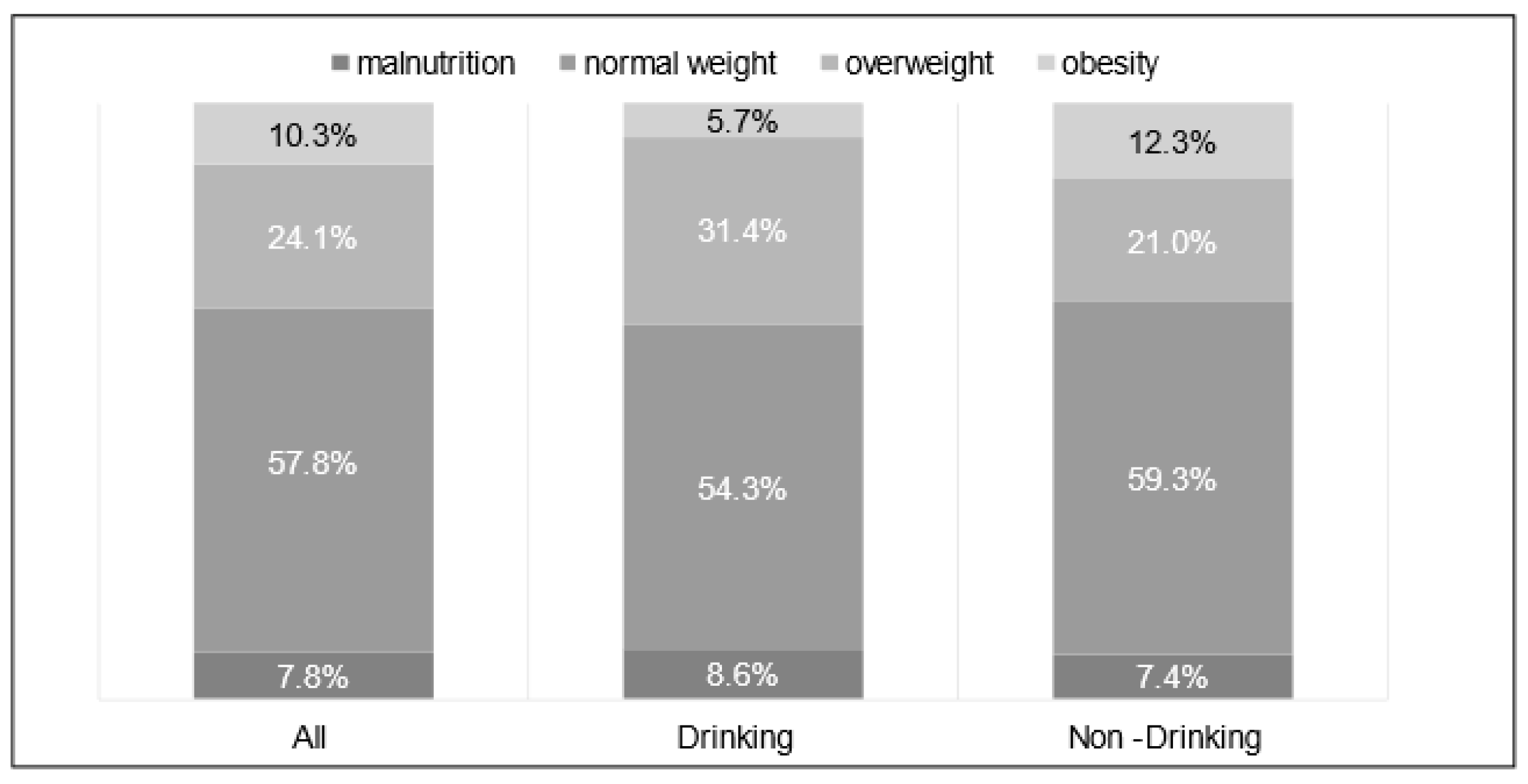
3.1. Baseline Physical and Biochemical Characteristics
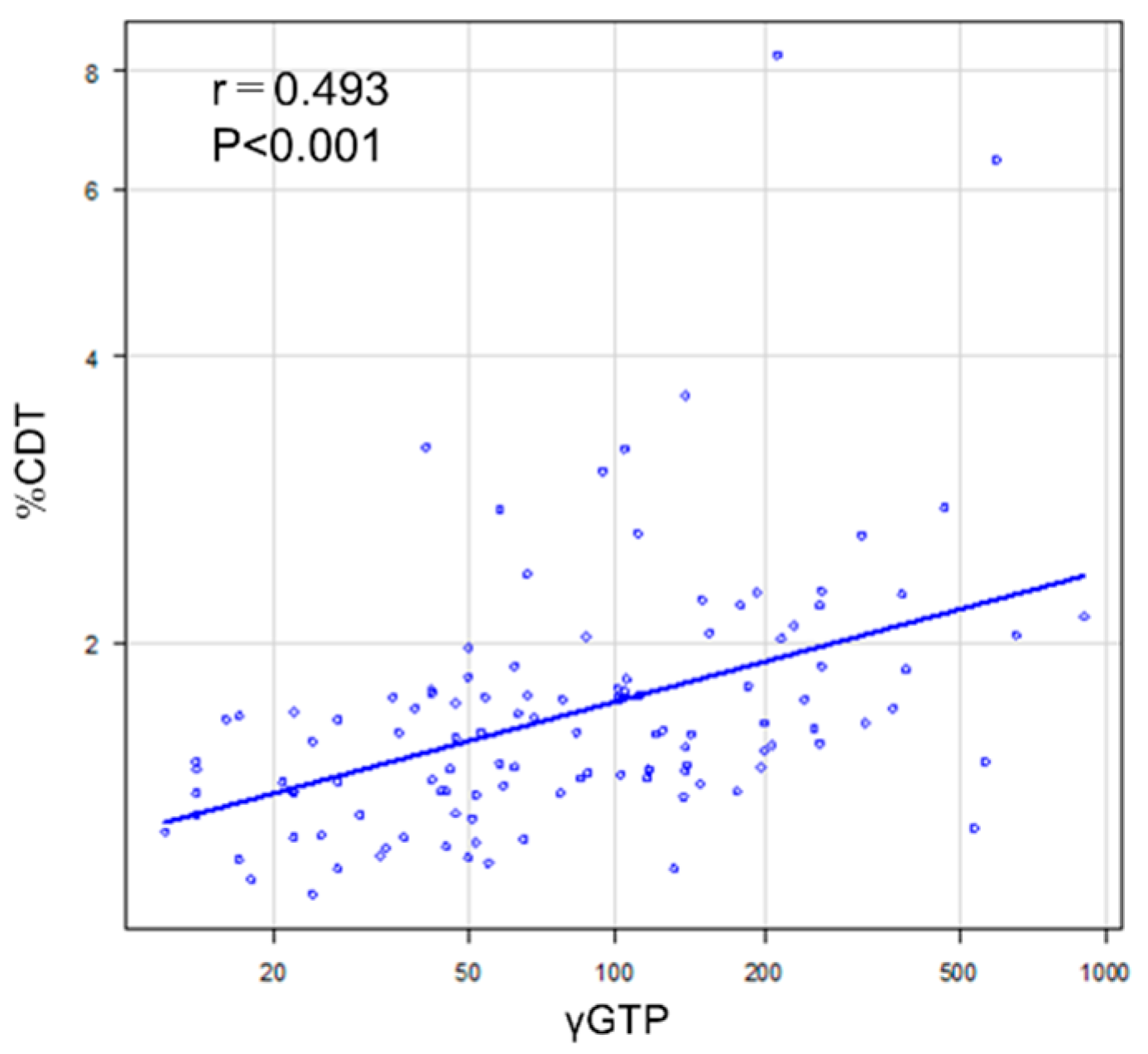
3.2. Correlation between the %CDT and γ-GTP
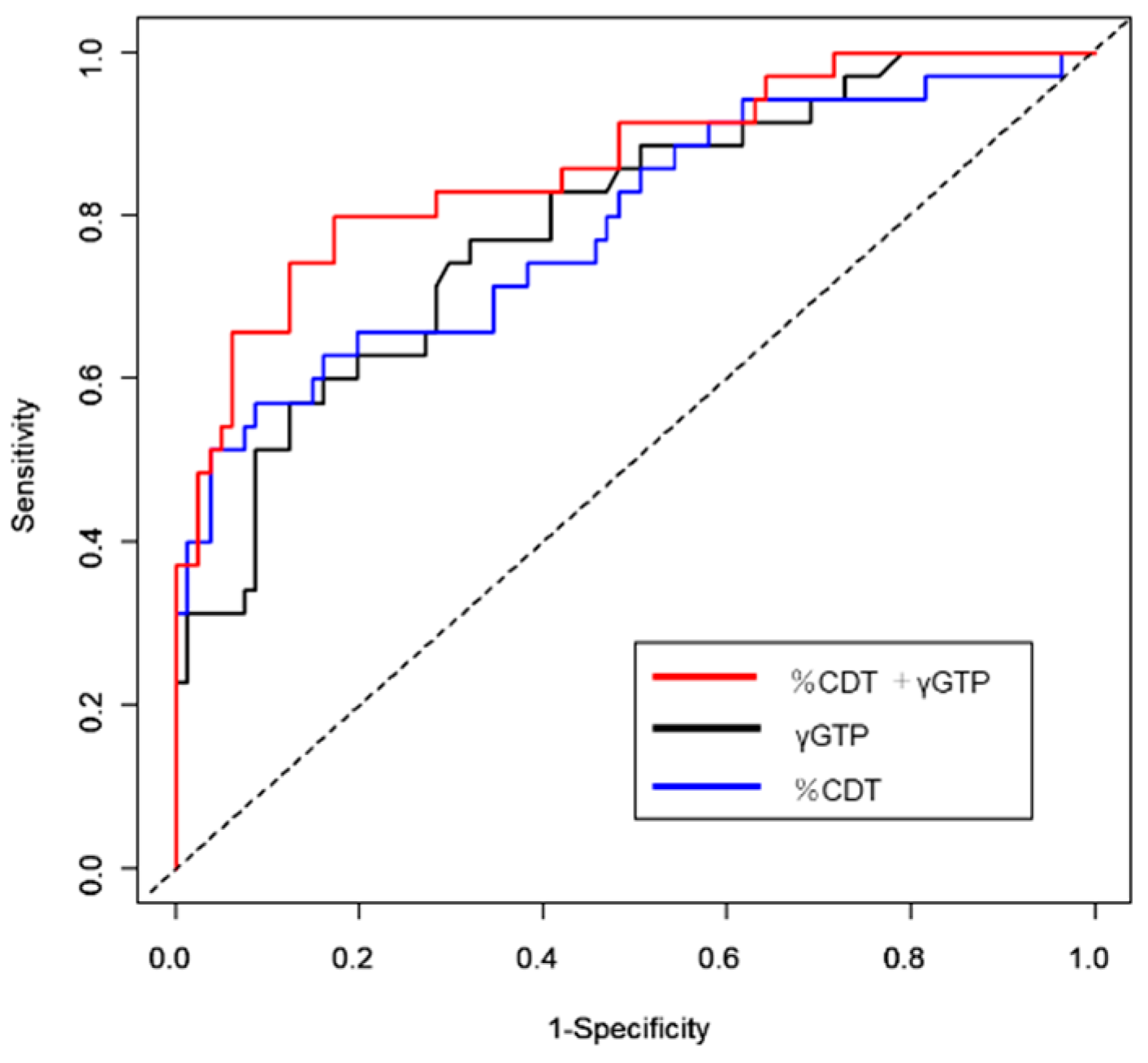
3.3. Prediction Accuracy of %CDT Alone, γ-GTP Alone, and Their Combination for Alcohol Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shima, T.; Ohtakaki, Y.; Kikuchi, H.; Uchino, H.; Isomura, M.; Aoyagi, K.; Oya, H.; Katayama, T.; Mitsumoto, Y.; Mizuno, M.; et al. A novel rapid immunoassay of serum type IV collagen 7S for the diagnosis of fibrosis stage of non-alcoholic fatty liver diseases. Hepatol. Res. 2020, 51, 263–276. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.; Eslam, M.; George, J.; Al Mahtab, M.; Akbar, S.M.F.; Jia, J.; Tian, Q.; Aggarwal, R.; Muljono, D.H.; et al. Liver diseases in the Asia-Pacific region: A Lancet Gastroenterology & Hepatology Commission. Lancet Gastroenterol. Hepatol. 2020, 5, 167–228. [Google Scholar] [CrossRef] [Green Version]
- Masaki, N.; Kawasaki, Y.; Nozaki, Y.; Yanase, M. Characteristics of patients aged over 75 years with hepatitis C virus infection treated with direct-acting antivirals in Japan: Evidence based on the nationwide, real-world database in Japan. Hepatol. Res. 2020, 51, 427. [Google Scholar] [CrossRef]
- Enomoto, H.; Ueno, Y.; Hiasa, Y.; Nishikawa, H.; Hige, S.; Takikawa, Y.; Taniai, M.; Ishikawa, T.; Yasui, K.; Takaki, A.; et al. Transition in the etiology of liver cirrhosis in Japan: A nationwide survey. J. Gastroenterol. 2020, 55, 353–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chon, H.Y.; Lee, J.S.; Lee, H.W.; Chun, H.S.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Kim, S.U. Impact of antiviral therapy on risk prediction model for hepatocellular carcinoma development in patients with chronic hepatitis B. Hepatol. Res. 2020, 51, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Crabb, D.W.; Im, G.Y.; Szabo, G.; Mellinger, J.L.; Lucey, M.R. Diagnosis and Treatment of Alcohol-Associated Liver Diseases: 2019 Practice Guidance From the American Association for the Study of Liver Diseases. Hepatology 2020, 71, 306–333. [Google Scholar] [CrossRef] [Green Version]
- Conigrave, K.M.; Davies, P.; Haber, P.; Whitfield, J.B. Traditional markers of excessive alcohol use. Addiction 2003, 98 (Suppl. S2), 31–43. [Google Scholar] [CrossRef] [PubMed]
- Fleming, M.F.; Anton, R.F.; Spies, C.D. A review of genetic, biological, pharmacological, and clinical factors that affect carbohydrate-deficient transferrin levels. Alcohol. Clin. Exp. Res. 2004, 28, 1347–1355. [Google Scholar] [CrossRef]
- Hietala, J.; Koivisto, H.; Anttila, P.; Niemela, O. Comparison of the combined marker GGT-CDT and the conventional laboratory markers of alcohol abuse in heavy drinkers, moderate drinkers and abstainers. Alcohol Alcohol. 2006, 41, 528–533. [Google Scholar] [CrossRef] [Green Version]
- Hannuksela, M.L.; Liisanantti, M.K.; Nissinen, A.E.; Savolainen, M.J. Biochemical markers of alcoholism. Clin. Chem. Lab. Med. 2007, 45, 953–961. [Google Scholar] [CrossRef]
- Allen, J.P. Use of biomarkers of heavy drinking in health care practice. Mil. Med. 2003, 168, 364–367. [Google Scholar] [CrossRef] [Green Version]
- Anton, R.F.; Moak, D.H. Carbohydrate-deficient transferrin and gamma-glutamyltransferase as markers of heavy alcohol consumption: Gender differences. Alcohol. Clin. Exp. Res. 1994, 18, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Anton, R.F.; Lieber, C.; Tabakoff, B. Carbohydrate-deficient transferrin and gamma-glutamyltransferase for the detection and monitoring of alcohol use: Results from a multisite study. Alcohol. Clin. Exp. Res. 2002, 26, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Deas, D.; Johnson, N.; Thomas, S. Carbohydrate deficient transferrin (CDT) predicts heavy drinking in adolescents with alcohol dependence. Alcohol 2019, 81, 27–30. [Google Scholar] [CrossRef]
- Bergstrom, J.P.; Helander, A. Influence of alcohol use, ethnicity, age, gender, BMI and smoking on the serum transferrin glycoform pattern: Implications for use of carbohydrate-deficient transferrin (CDT) as alcohol biomarker. Clin. Chim. Acta 2008, 388, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Golka, K.; Wiese, A. Carbohydrate-deficient transferrin (CDT)--a biomarker for long-term alcohol consumption. J. Toxicol. Environ. Health Part B 2004, 7, 319–337. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yoo, G.S.; Hee Kang, S.; Uh, Y. Is carbohydrate deficient transferrin (CDT) a useful biomarker to identify alcohol abuse in advanced liver fibrosis? Alcohol Alcohol. 2017, 52, 749–750. [Google Scholar] [CrossRef] [Green Version]
- Galan, I.; Valencia-Martin, J.L.; Guallar-Castillon, P.; Rodriguez-Artalejo, F. Alcohol drinking patterns and biomarkers of coronary risk in the Spanish population. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 189–197. [Google Scholar] [CrossRef]
- Lee, Y.J.; Cho, S.; Kim, S.R. Effect of alcohol consumption on kidney function: Population-based cohort study. Sci. Rep. 2021, 11, 2381. [Google Scholar] [CrossRef]
- Bell, S.; Daskalopoulou, M.; Rapsomaniki, E.; George, J.; Britton, A.; Bobak, M.; Casas, J.P.; Dale, C.E.; Denaxas, S.; Shah, A.D.; et al. Association between clinically recorded alcohol consumption and initial presentation of 12 cardiovascular diseases: Population based cohort study using linked health records. BMJ 2017, 356, j909. [Google Scholar] [CrossRef] [Green Version]
- De Iuliis, V.; Gelormini, R.; Flacco, M.; Moriello, G.; Caruso, M.; Barone, E.; Golato, M.; Toniato, E.; Conti, P.; Martinotti, S. Comparison of Serum Total Valproic Acid Levels and %CDT Values in Chronic Alcohol Addictive Patients in an Italian Clinic: A Retrospective Study. Drugs Real World Outcomes 2016, 3, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Fagan, K.J.; Irvine, K.M.; McWhinney, B.C.; Fletcher, L.M.; Horsfall, L.U.; Johnson, L.; O’Rourke, P.; Martin, J.; Scott, I.; Pretorius, C.J.; et al. Diagnostic sensitivity of carbohydrate deficient transferrin in heavy drinkers. BMC Gastroenterol. 2014, 14, 97. [Google Scholar] [CrossRef] [PubMed]
- Helander, A. Biological markers in alcoholism. Addict. Mech. Phenomenol. Treat. 2003, 15–32. [Google Scholar] [CrossRef]
- van Beek, J.; de Moor, M.H.M.; Geels, L.M.; Sinke, M.R.T.; de Geus, E.J.C.; Lubke, G.H.; Kluft, C.; Neuteboom, J.; Vink, J.M.; Willemsen, G.; et al. The association of alcohol intake with gamma-glutamyl transferase (GGT) levels: Evidence for correlated genetic effects. Drug Alcohol Depend. 2014, 134, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mundle, G.; Ackermann, K.; Munkes, J.; Steinle, D.; Mann, K. Influence of age, alcohol consumption and abstinence on the sensitivity of carbohydrate-deficient transferrin, gamma-glutamyltransferase and mean corpuscular volume. Alcohol Alcohol. 1999, 34, 760–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szegedi, A.; Muller, M.J.; Himmerich, H.; Anghelescu, I.; Wetzel, H. Carbohydrate-deficient transferrin (CDT) and HDL cholesterol (HDL) are highly correlated in male alcohol dependent patients. Alcohol. Clin. Exp. Res. 2000, 24, 497–500. [Google Scholar] [CrossRef]
- Hock, B.; Schwarz, M.; Domke, I.; Grunert, V.P.; Wuertemberger, M.; Schiemann, U.; Horster, S.; Limmer, C.; Stecker, G.; Soyka, M. Validity of carbohydrate-deficient transferrin (%CDT), gamma-glutamyltransferase (gamma-GT) and mean corpuscular erythrocyte volume (MCV) as biomarkers for chronic alcohol abuse: A study in patients with alcohol dependence and liver disorders of non-alcoholic and alcoholic origin. Addiction 2005, 100, 1477–1486. [Google Scholar] [CrossRef]
- Schwan, R.; Loiseaux, M.N.; Schellenberg, F.; Albuisson, E.; Favre, J.D.; Rigaud, A.; Llorca, P.M.; Gillet, C.; Reynaud, M. Multicenter validation study of the %CDT TIA kit in alcohol abuse and alcohol dependence. Alcohol. Clin. Exp. Res. 2004, 28, 1331–1337. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 116) | Drinking Group (n = 35) | Nondrinking Group (n = 81) | p-Value |
|---|---|---|---|---|
| Age (years) | 65.5 ± 11.8 | 62.4 ± 11.4 | 66.9 ± 11.7 | 0.062 |
| Male/Female | 108/8 | 32/3 | 76/5 | 0.70 |
| Height (cm) | 165.0 ± 7.2 | 165.5 ± 7.1 | 164.7 ± 7.2 | 0.60 |
| Weight (kg) | 65.6 ± 13.1 | 65.3 ± 11.5 | 65.8 ± 13.7 | 0.83 |
| Body mass index (kg/m2) | 24.0 ± 4.0 | 23.8 ± 3.5 | 24.1 ± 4.2 | 0.65 |
| Biochemical Data | All Patients (n = 116) | Drinking Group (n = 35) | Nondrinking Group (n = 81) | p-Value |
|---|---|---|---|---|
| Albumin, mean ± SD | 3.7 ± 0.7 | 3.5 ± 0.7 | 3.8 ± 0.6 | 0.019 |
| PT, % | 71.1 ± 16.8 | 68.5 ± 22.8 | 72.2 ± 13.0 | 0.28 |
| T-Bil | 1.2 (0.8–1.6) | 1.5 (0.95–3.3) | 1.1 (0.8–1.5) | 0.011 |
| Child–Pugh classification (A/B/C) | 76/29/11 | 56/21/4 | 20/8/7 | 0.053 |
| Platelet | 12.2 ± 5.9 | 12.6 ± 6.7 | 12.0 ± 5.4 | 0.67 |
| AST | 52.4 ± 42.4 | 81.6 ± 57.0 | 39.8 ± 24.9 | <0.001 |
| ALT | 25 (17–45) | 44 (23.5–59.5) | 23 (15–34) | <0.001 |
| γ-GTP | 77.5 (42–151.3) | 194 (98–319.5) | 54 (33–115) | <0.001 |
| ALP | 396.2 ± 211.3 | 469.2 ± 275.2 | 365.2 ± 166.3 | 0.015 |
| %CDT | 1.8 ± 0.9 | 2.4 ± 1.4 | 1.5 ± 0.3 | <0.001 |
| IgA | 464.1 ± 248.3 | 513.0 ± 287.1 | 443.3 ± 230.7 | 0.19 |
| Transferrin | 231.4 ± 68.6 | 220.7 ± 79.2 | 236.6 ± 63.0 | 0.35 |
| Iron | 100.4 ± 64.3 | 119.9 ± 72.3 | 91.9 ± 59.1 | 0.064 |
| Diagnostic Model | Cut Off | Se | Sp | PPV | NVP | AIC | AUC (95% CI) |
|---|---|---|---|---|---|---|---|
| γ-GTP (IU/L) | 101.5 | 0.743 | 0.704 | 0.520 | 0.864 | 116.1 | 0.792 (0.689–0.878) |
| %CDT | 1.75 | 0.657 | 0.802 | 0.590 | 0.844 | 109.7 | 0.790 (0.696–0.878) |
| γGTP + %CDT | 0.25 | 0.800 | 0.827 | 0.667 | 0.905 | 96.4 | 0.863 (0.779–0.930) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shibamoto, A.; Namisaki, T.; Suzuki, J.; Kubo, T.; Iwai, S.; Tomooka, F.; Takeda, S.; Fujimoto, Y.; Enomoto, M.; Murata, K.; et al. Clinical Significance of Gamma-Glutamyltranspeptidase Combined with Carbohydrate-Deficient Transferrin for the Assessment of Excessive Alcohol Consumption in Patients with Alcoholic Cirrhosis. Medicines 2021, 8, 39. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8070039
Shibamoto A, Namisaki T, Suzuki J, Kubo T, Iwai S, Tomooka F, Takeda S, Fujimoto Y, Enomoto M, Murata K, et al. Clinical Significance of Gamma-Glutamyltranspeptidase Combined with Carbohydrate-Deficient Transferrin for the Assessment of Excessive Alcohol Consumption in Patients with Alcoholic Cirrhosis. Medicines. 2021; 8(7):39. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8070039
Chicago/Turabian StyleShibamoto, Akihiko, Tadashi Namisaki, Junya Suzuki, Takahiro Kubo, Satoshi Iwai, Fumimasa Tomooka, Soichi Takeda, Yuki Fujimoto, Masahide Enomoto, Koji Murata, and et al. 2021. "Clinical Significance of Gamma-Glutamyltranspeptidase Combined with Carbohydrate-Deficient Transferrin for the Assessment of Excessive Alcohol Consumption in Patients with Alcoholic Cirrhosis" Medicines 8, no. 7: 39. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8070039