
Prospective Comparison of 24-Hour Urine Creatinine Clearance with Estimated Glomerular Filtration Rates in Chronic Renal Disease Patients of African Descent


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Ethical Approval
2.2. Demographic Data Collection
2.3. Measurements
2.4. Blood Samples and 24-Hour Urine Collections
2.5. Serum Assays Used to Determine Analytes
2.6. Creatinine Clearance and Estimated GFR
2.7. Data Analysis
3. Results
3.1. Correlation of Different Methods
3.2. Comparison of Different Methods of eGFR by Stages and Creatinine Concentration
3.3. Comparison of Methods by Normal vs. Abnormal Creatinine Levels
3.4. Comparison of Methods by Age and Gender
3.5. Comparison of Methods by Ranges of CrCl
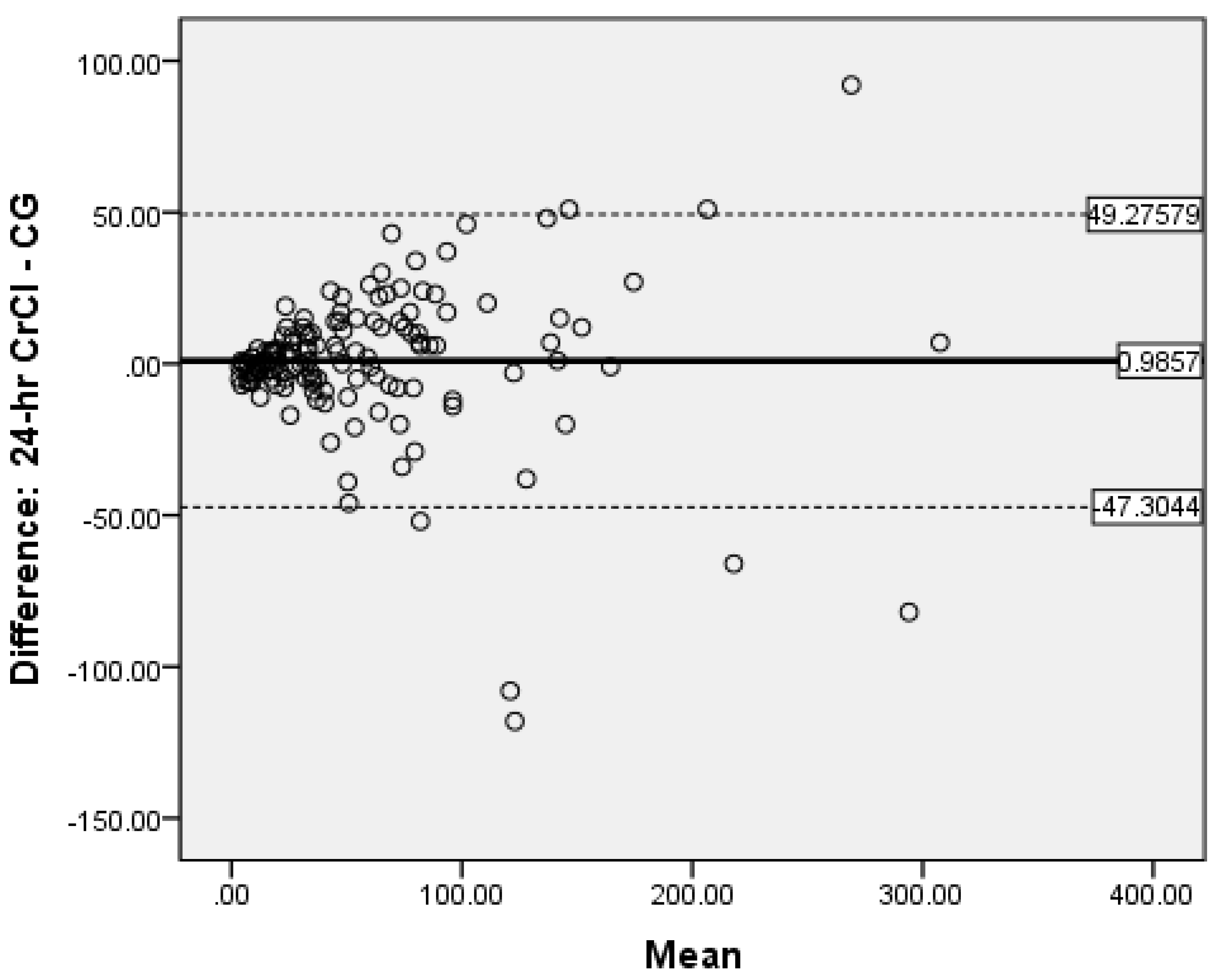
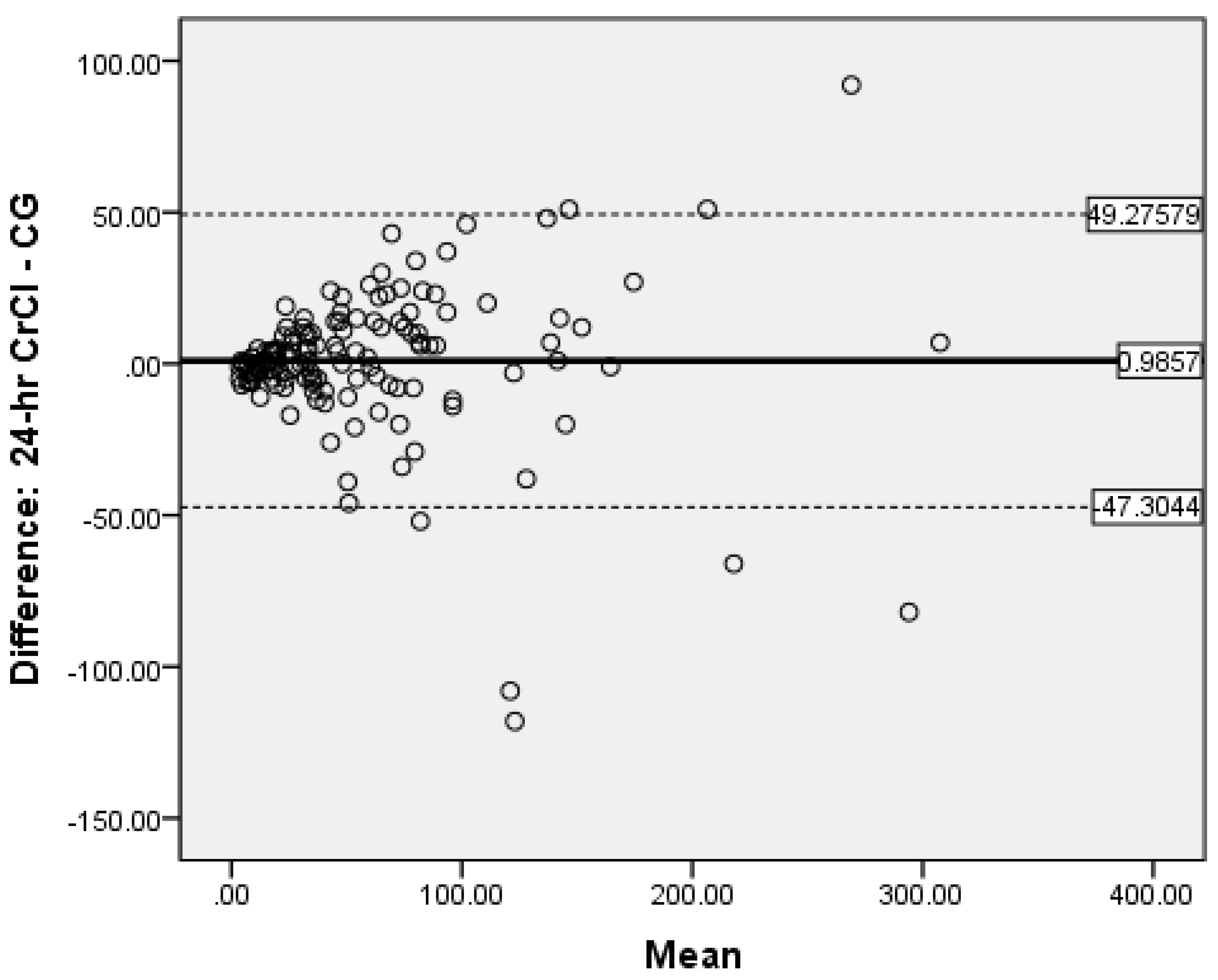
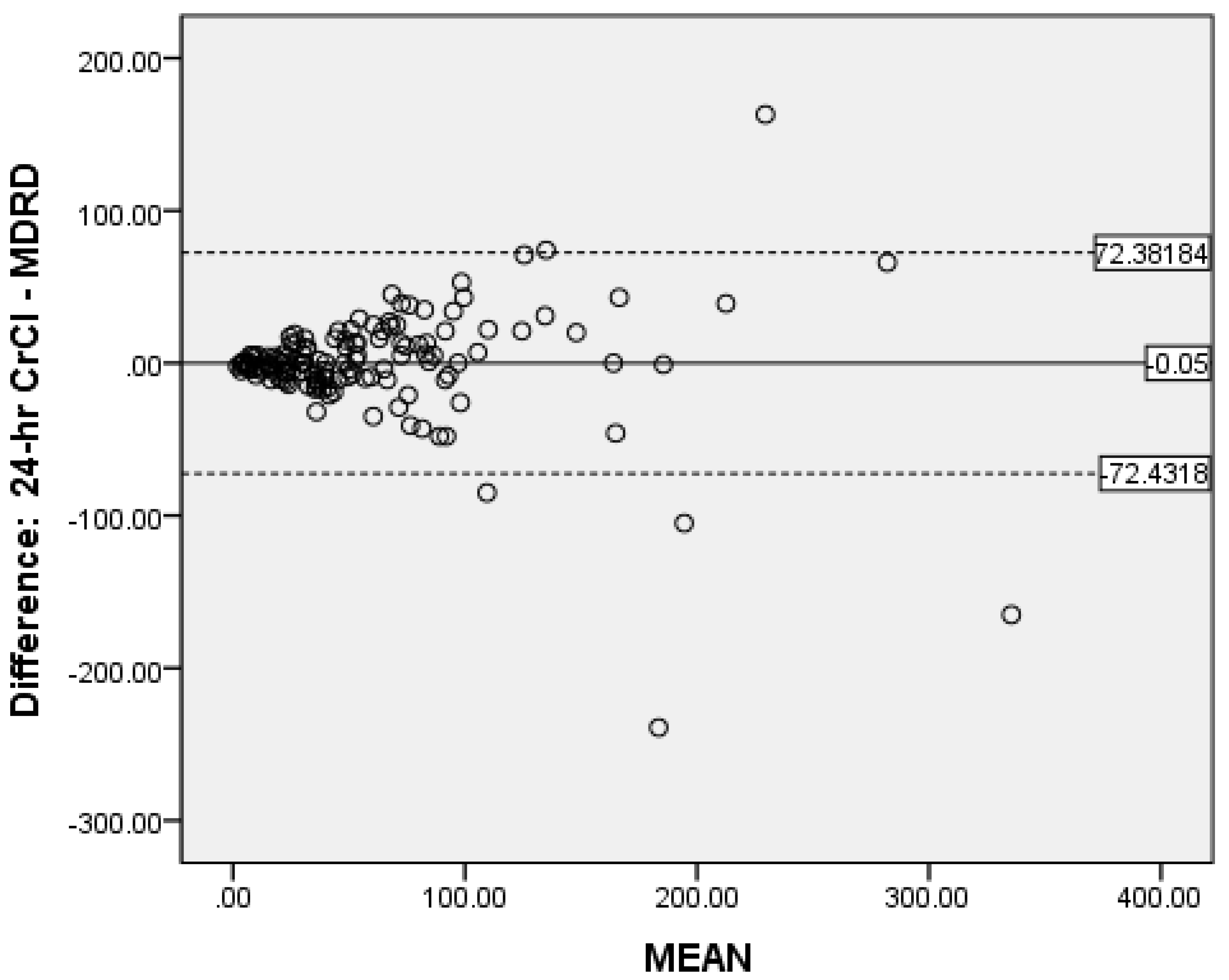
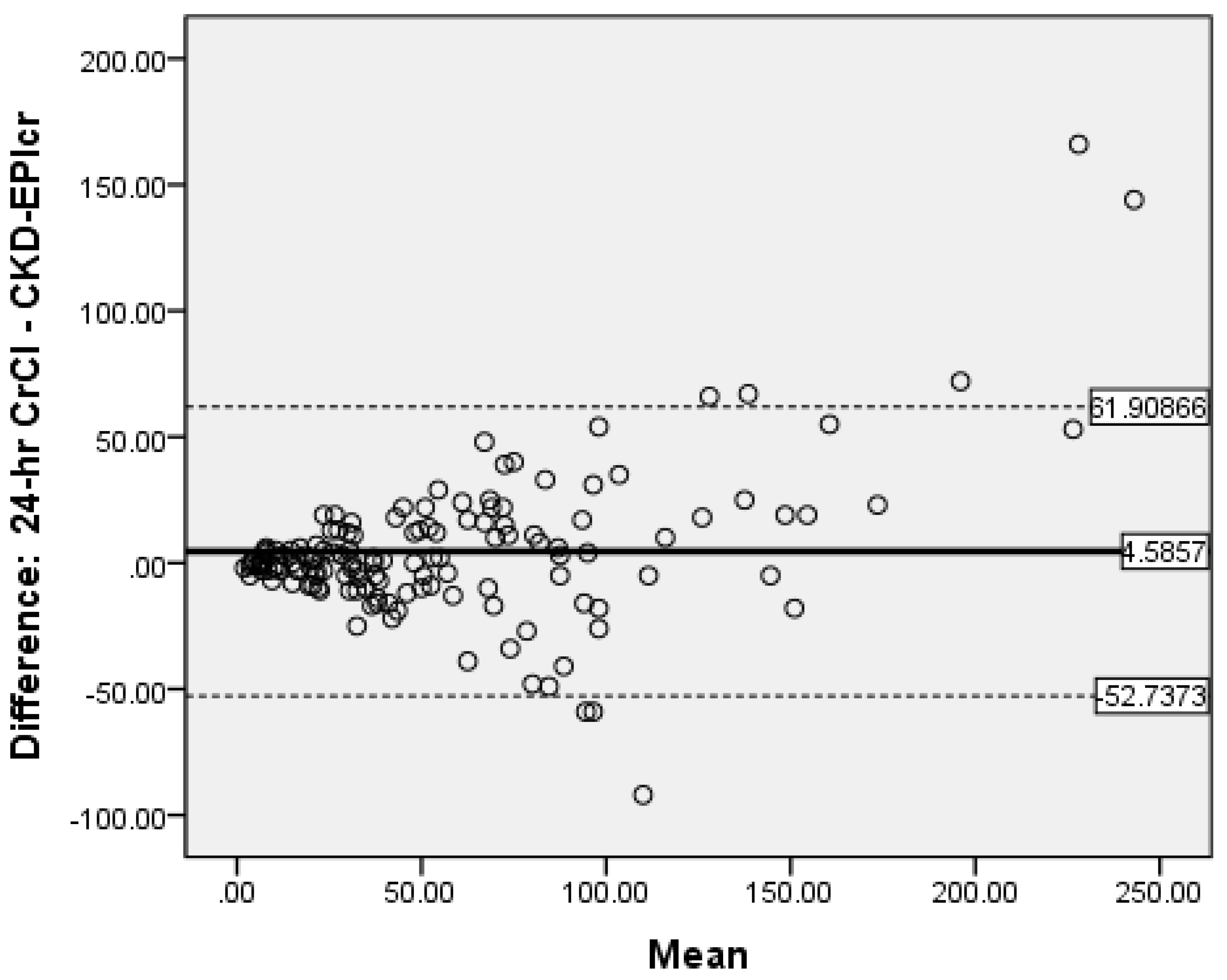
3.6. Determination of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levey, A.S.; Atkins, R.; Coresh, J.; Cohen, E.P.; Collins, A.J.; Eckardt, K.U.; Nahas, M.E.; Jaber, B.L.; Jadoul, M.; Levin, A.; et al. Chronic kidney disease as a global public health problem: Approaches and initiatives—A position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007, 72, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D. Global Prevalence of Chronic Kidney Disease—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Soyibo, A.K.; Barton, E.N. Report from the Caribbean renal registry, 2006. West Indian Med. J. 2007, 56, 355–363. [Google Scholar]
- Soyibo, A.K.; Barton, E.N. Chronic renal failure from the English-speaking Caribbean: 2007 data. West Indian Med. J. 2009, 58, 596–600. [Google Scholar]
- Witte, E.C.; Lambers Heerspink, H.J.; de Zeeuw, D.; Bakker, S.J.; de Jong, P.E.; Gansevoort, R. First morning voids are more reliable than spot urine samples to assess microalbuminuria. J. Am. Soc. Nephrol. 2009, 20, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Erman, A.; Rahamimov, R.; Mashraki, T.; Levy-Drummer, R.S.; Winkler, J.; David, I.; Hirsh, Y.; Gafter, U.; Chagnac, A. The urine albumin-to-creatinine ratio: Assessment of its performance in the renal transplant recipient population. Clin. J. Am. Soc. Nephrol. 2011, 6, 892–897. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.C.; O’Reilly, P.H. Iohexol clearance for the determination of glomerular filtration rate in clinical practice: Evidence for a new gold standard. J. Urol. 1991, 146, 675–679. [Google Scholar] [CrossRef]
- Schwartz, G.J.; Work, D.F. Measurement and estimation of GFR in children and adolescents. Clin. Am. Soc. Nephrol. 2009, 4, 1832–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LaFrance, N.D.; Drew, H.H.; Walser, M. Radioisotopic measurement of glomerular filtration rate in severe chronic renal failure. J. Nucl. Med. 1988, 29, 1927–1930. [Google Scholar]
- Perrone, R.D.; Steinman, T.I.; Beck, G.J.; Skibinski, C.I.; Royal, H.D.; Lawlor, M.; Hunsicker, L.G. Utility of radioisotopic filtration markers in chronic renal insufficiency: Simultaneous comparison of 125I-iothalamate, 169Yb-DTPA, 99mTc-DTPA, and inulin. The Modification of Diet in Renal Disease Study. Am. J. Kidney Dis. 1990, 16, 224–235. [Google Scholar] [CrossRef]
- Rowe, J.W.; Andres, R.; Tobin, J.D.; Norris, A.H.; Shock, N.W. The effect of age on creatinine clearance in men: A cross-sectional and longitudinal study. J. Gerontol. 1976, 31, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Stevens, L.A.; Coresh, J.; Greene, T.; Levey, A.S. Assessing kidney function--measured and estimated glomerular filtration rate. N. Engl. J. Med. 2006, 354, 2473–2483. [Google Scholar] [CrossRef] [Green Version]
- Banfi, G.; Del Fabbro, M. Serum creatinine values in elite athletes competing in 8 different sports: Comparison with sedentary people. Clin. Chem. 2006, 52, 330–331. [Google Scholar] [CrossRef]
- Shahbaz, H.; Gupta, M. Creatinine Clearance. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- National Kidney Foundation. K/DQI clinical practice guidelines for chronic kidney disease. Evaluation classification and stratification. Kidney Disease Outcomes quality Initiative. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Kuan, Y.; Hossain, M.; Surman, J.; El Nahas, A.M.; Haylor, J. GFR prediction using the MDRD and Cockcroft and Gault equations in patients with end-stage renal disease. Nephrol. Dial. Transplant. 2005, 20, 2394–2401. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Levey, A.S.; Greene, T.; Kusek, J.W.; Beck, G.J. A simplified equation to predict glomerular filtration rate from serum creatinine. J. Am. Soc. Nephrol. 2000, 11, 155A. [Google Scholar]
- Froissart, M.; Rossert, J.; Jacquot, C.; Paillard, M.; Houillier., P. Predictive performance of the modification of diet in renal disease and Cockcroft-Gault equations for estimating renal function. J. Am. Soc. Nephrol. 2005, 16, 763–773. [Google Scholar] [CrossRef] [Green Version]
- Poggio, E.D.; Wang, X.; Greene, T.; Van Lente, F.; Hall, P.M. Performance of the modification of diet in renal disease and Cockcroft-Gault equations in the estimation of GFR in health and in chronic kidney disease. J. Am. Soc. Nephrol. 2005, 16, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Van Deventer, H.E.; Paiker, J.E.; Katz, I.J.; George, J.A. A comparison of cystatin C- and creatinine-based prediction equations for the estimation of glomerular filtration rate in black South Africans. Nephrol. Dial. Transplant. 2011, 26, 1553–1558. [Google Scholar] [CrossRef]
- Helmersson-Karlqvist, J.; Arnlov, J.; Larsson, A. Cystatin C-based glomerular filtration rate associates more closely with mortality than creatinine-based or combined glomerular filtration rate equations in unselected patients. Eur. J. Prev. Cardiol. 2016, 23, 1649–1657. [Google Scholar] [CrossRef]
- Chi, X.H.; Li, G.P.; Wang, Q.S.; Qi, Y.S.; Huang, K.; Zhang, Q.; Xue, Y.M. CKD-EPI creatinine-cystatin C glomerular filtration rate estimation equation seems more suitable for Chinese patients with chronic kidney disease than other equations. BMC Nephrol. 2017, 18, 226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, L.X.; Sun, L.; Nicholas, S.B.; Lu, Y.; Sinha, S.; Hua, R. Comparison of bias and accuracy using cystatin C and creatinine in CKD-EPI equations for GFR estimation. Eur. J. Intern. Med. 2020, 80, 29–34. [Google Scholar] [CrossRef]
- Tapper, M.; McGrowder, D.A.; Dilworth, L.; Soyibo, A. Cystatin C, vitamin D and thyroid function test profile in chronic kidney disease patients. Diseases 2021, 9, 5. [Google Scholar] [CrossRef]
- Peake, M.; Whiting, M. Measurement of serum creatinine—Current status and future goals. Clin. Biochem. Rev. 2006, 27, 173–184. [Google Scholar]
- Delanghe, J.; Speeckaert, M. Creatinine determination according to Jaffe—What does it stand for? NDT Plus. 2011, 4, 83–86. [Google Scholar] [CrossRef]
- Haeckel, R. Assay of creatinine in serum, with use of Fuller’s Earth to remove interferents. Clin. Chem. 1981, 27, 179–183. [Google Scholar] [CrossRef]
- Hansson, L.O.; Grubb, A.; Lidén, A.; Flodin, M.; Berggren, A.; Delanghe, J.; Stove, V.; Luthe, H.; Rhode, K.H.; Beck, C.; et al. Performance evaluation of a turbidimetric cystatin C assay on different high-throughput platforms. Scand. J. Clin. Lab. Investig. 2010, 7, 347–353. [Google Scholar] [CrossRef]
- Kilbride, H.S.; Stevens, P.E.; Eaglestone, G.; Knight, S.; Carter, J.L.; Delaney, M.P.; Farmer, C.K.; Irving, J.; O’Riordan, S.; Dalton, R.N.; et al. Accuracy of the MDRD (Modification of Diet in Renal Disease) study and CKD-EPI (CKD Epidemiology Collaboration) equations for estimation of GFR in the elderly. Am. J. Kidney Dis. 2013, 61, 57–66. [Google Scholar] [CrossRef]
- Elnokeety, M.M.; Shaker, A.M.; Fayed, A.M. Creatinine, cystatin, and combined-based equations in assessment of renal functions in type 2 diabetic Egyptian patients. Egypt J. Intern. Med. 2017, 29, 105–111. [Google Scholar] [CrossRef]
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. 2013, 3, 19–62. [Google Scholar]
- Hahn, T.; Yao, S.; Dunford, L.M.; Thomas, J.; Lohr, J.; Arora, P.; Battiwalla, M.; Smiley, S.L.; McCarthy, P.L., Jr. A comparison of measured creatinine clearance versus calculated glomerular filtration rate for assessment of renal function before autologous and allogeneic BMT. Biol. Blood Marrow Transplant. 2009, 15, 574–579. [Google Scholar] [CrossRef] [Green Version]
- Adebisi, S.A. Utility of estimated glomerular filtration rate equations in Nigerians with stable chronic kidney disease. West Afr. J. Med. 2011, 30, 432–435. [Google Scholar]
- Das, S.K.; Roy, D.K.; Chowdhury, A.A.; Roy, A.S.; Ahammed, S.U.; Asadujjaman, M.; Rabbani, M.G.; Islam, M.S.; Barman, G.C.; Chanda, K.; et al. Correlation of eGFR By MDRD and CKD-EPI Formula with Creatinine Clearance Estimation in CKD Patients and Healthy Subjects. Mymensingh Med. J. 2021, 30, 35–42. [Google Scholar]
- Hu, J.; Xu, X.; Zhang, K.; Li, Y.; Zheng, J.; Chen, W.; Wang, X. Comparison of estimated glomerular filtration rates in Chinese patients with chronic kidney disease among serum creatinine-, cystatin-C- and creatinine-cystatin-C-based equations: A retrospective cross-sectional study. Clin. Chim. Acta 2020, 505, 34–42. [Google Scholar] [CrossRef]
- Verhave, J.C.; Gansevoort, R.T.; Hillege, H.L.; De Zeeuw, D.; Curhan, G.C.; De Jong, P.E. Drawbacks of the use of indirect estimates of renal function to evaluate the effect of risk factors on renal function. J. Am. Soc. Nephrol. 2004, 15, 1316–1322. [Google Scholar]
- Kumar, B.V.; Mohan, T. Retrospective comparison of estimated GFR using 2006 MDRD, 2009 CKD-EPI and Cockcroft-Gault with 24 h urine creatinine clearance. J. Clin. Diagn. Res. 2017, 11, BC09–BC12. [Google Scholar] [CrossRef]
- Krzanowski, M.; Januszek, R.; Krzanowska, K.; Kuźniewski, M.; Kopeć, J.; Chowaniec, E.; Sułowicz, W. Prevalence of the stages of chronic kidney disease (CKD) according to simplified MDRD formula in patients from ambulatory settings. Prz. Lek. 2015, 72, 277–281. [Google Scholar]
- Coresh, J.; Eknoyan, G.; Levey, A.S. Estimating the prevalence of low glomerular filtration rate requires attention to the creatinine assay calibration. J. Am. Soc. Nephrol. 2002, 13, 2811–2812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coresh, J.; Astor, B.C.; McQuillan, G.; Kusek, J.; Greene, T.; Van Lente, F.; Levey, A.S. Calibration and random variation of the serum creatinine assay as critical elements of using equations to estimate glomerular filtration rate. Am. J. Kidney Dis. 2002, 39, 920–929. [Google Scholar] [CrossRef]
- Vickery, S.; Stevens, P.E.; Dalton, R.N.; van Lente, F.; Lamb, E.J. Does the ID-MS traceable MDRD equation work and is it suitable for use with compensated Jaffe and enzymatic creatinine assays? Nephrol. Dial. Transplant. 2006, 21, 2439–2445. [Google Scholar] [CrossRef]
- Lewis, J.; Agodoa, L.; Cheek, D.; Greene, T.; Middleton, J.; O’Connor, D.; Ojo, A.; Phillips, R.; Sika, M.; Wright, J., Jr. African-American Study of Hypertension and Kidney Disease. Comparison of cross-sectional renal function measurements in African Americans with hypertensive nephrosclerosis and of primary formulas to estimate glomerular filtration rate. Am. J. Kidney Dis. 2001, 38, 744–753. [Google Scholar] [CrossRef]
- McFadden, E.C.; Hirst, J.A.; Verbakel, J.Y.; McLellan, J.H.; Hobbs, F.D.R.; Stevens, R.J.; O’Callaghan, C.A.; Lasserson, D.S. Systematic review and meta-analysis comparing the bias and accuracy of the modification of diet in renal disease and chronic kidney disease epidemiology collaboration equations in community-based populations. Clin. Chem. 2018, 64, 475–485. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, K.; Mahmoodi, B.K.; Woodward, M.; Emberson, J.R.; Jafar, T.H.; Jee, S.H.; Polkinghorne, K.R.; Shankar, A.; Smith, D.H.; Tonelli, M.; et al. Chronic Kidney Disease Prognosis Consortium. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA 2012, 307, 1941–1951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bukabau, J.B.; Yayo, E.; Gnionsahé, A.; Monnet, D.; Pottel, H.; Cavalier, E.; Nkodila, A.; Makulo, J.R.R.; Mokoli, V.M.; Lepira, F.B.; et al. Performance of creatinine- or cystatin C-based equations to estimate glomerular filtration rate in sub-Saharan African populations. Kidney Int. 2019, 95, 1181–1189. [Google Scholar] [CrossRef] [Green Version]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. CKD-EPI Investigators. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 2012, 367, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, T.; Alon, U.S.; Althahabi, R.; Garg, U. Impact of standardization of creatinine methodology on the assessment of glomerular filtration rate in children. Pediatr. Res. 2009, 65, 113–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traynor, J.; Mactier, R.; Geddes, C.C.; Fox, J.G. How to measure renal function in clinical practice. BMJ 2006, 333, 733–737. [Google Scholar] [CrossRef]
- Michels, W.M.; Grootendorst, D.C.; Verduijn, M.; Elliott, E.G.; Dekker, F.W.; Krediet, R.T. Performance of the Cockcroft-Gault, MDRD, and new CKD-EPI formulas in relation to GFR, age, and body size. Clin. J. Am. Soc. Nephrol. 2010, 5, 1003–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CrCl | CG | MDRD | CKD-EPIcr | CKD-EPIcys | CKD-EPIcr-Cys | Creatinine | Cystatin C | Urea | ||
|---|---|---|---|---|---|---|---|---|---|---|
| N | 140 | 140 | 140 | 140 | 140 | 140 | 140 | 140 | 140 | |
| CrCl | Pearson’ coefficient p (Sig. 2-tailed) | 1 | 0.906 < 0.05 | 0.799 < 0.05 | 0.863 < 0.05 | 0.895 < 0.05 | 0.901 < 0.05 | −0.511 < 0.05 | −0.623 < 0.05 | −0.600 < 0.05 |
| CG | Pearson’ coefficient p (Sig. 2-tailed) | 0.906 < 0.05 | 1 < 0.05 | 0.899 < 0.05 | 0.915 < 0.05 | 0.869 < 0.05 | 0.921 < 0.05 | −0.502 < 0.05 | −0.588 < 0.05 | −0.593 < 0.05 |
| MDRD | Pearson’s coefficient p (Sig. 2-tailed) | 0.799 < 0.05 | 0.899 < 0.05 | 1 < 0.05 | 0.929 < 0.05 | 0.840 < 0.05 | 0.921 < 0.05 | −0.514 < 0.05 | −0.591 < 0.05 | −0.585 < 0.05 |
| CKD-EPIcr | Pearson’s coefficient p (Sig. 2-tailed) | 0.863 < 0.05 | 0.915 < 0.05 | 0.929 < 0.05 | 1 < 0.05 | 0.902 < 0.05 | 0.972 < 0.05 | −0.622 < 0.05 | −0.699 < 0.05 | −0.697 < 0.05 |
| CKD-EPIcys | Pearson’ coefficient p (Sig. 2-tailed) | 0.895 < 0.05 | 0.869 < 0.05 | 0.840 < 0.05 | 0.902 < 0.05 | 1 < 0.05 | 0.975 < 0.05 | −0.565 < 0.05 | −0.753 < 0.05 | −0.691 < 0.05 |
| CKD-EPIcr-cys Pearson’s coefficient p (Sig. 2-tailed) | 0.901 < 0.05 | 0.921 < 0.05 | 0.921 < 0.05 | 0.972 < 0.05 | 0.975 < 0.05 | 1 < 0.05 | −0.599 <0.05 | −0.735 < 0.05 | −0.701 < 0.05 | |
| Creatinine | Pearson’s coefficient p (Sig. 2-tailed) | −0.511 < 0.05 | −0.502 < 0.05 | −0.514 < 0.05 | −0.622 < 0.05 | −0.565 < 0.05 | −0.599 < 0.05 | 1 < 0.05 | 0.838 < 0.05 | 0.782 < 0.05 |
| Cystatin C | Pearson’s coefficient p (Sig. 2-tailed) | −0.623 < 0.05 | −0.588 < 0.05 | −0.591 < 0.05 | −0.699 < 0.05 | −0.753 < 0.05 | −0.735 < 0.05 | 0.838 < 0.05 | 1 < 0.05 | 0.829 < 0.05 |
| Urea | Pearson’s coefficient p (Sig. 2-tailed) | −0.600 < 0.05 | −0.593 < 0.05 | −0.585 < 0.05 | −0.697 < 0.05 | −0.691 < 0.05 | −0.701 < 0.05 | 0.782 < 0.05 | 0.829 < 0.05 | 1 |
| Stages CKD | Population (n) | 24-h Creat Cl | CG | p | MDRD | p | CKD-EPI Crea | p | CKD-EPI Cys | p | CKD-EPI Crea/Cys | p |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| V | 22 | 7.32 | 9.50 | <0.05 | 8.64 | 0.14 | 7.82 | 0.53 | 11.5 | <0.05 | 8.95 | 0.07 |
| IV | 24 | 20.67 | 22.83 | 0.34 | 26.63 | <0.05 | 24.58 | <0.05 | 21.29 | 0.63 | 22.21 | 0.27 |
| III | 41 | 41.10 | 41.95 | 0.74 | 47.51 | 0.26 | 43.46 | 0.34 | 29.17 | <0.05 | 34.22 | <0.05 |
| II | 27 | 74.33 | 76.78 | 0.72 | 85.04 | 0.31 | 80.70 | 0.30 | 47.63 | <0.05 | 60.85 | <0.05 |
| I | 26 | 152.42 | 139.38 | 0.08 | 130.85 | 0.08 | 113.35 | <0.05 | 76.96 | <0.05 | 94.08 | <0.05 |
| ALL | 140 | 59.37 | 58.39 | 0.64 | 59.42 | 0.99 | 54.79 | 0.07 | 37.48 | <0.05 | 44.44 | <0.05 |
| Stage | CrCl | CG | MDRD | CKD-EPI Crea | CKD-EPI Cys | CKD-EPI Crea-Cys |
|---|---|---|---|---|---|---|
| I | 26 | 24 | 26 | 29 | 9 | 16 |
| II | 27 | 26 | 20 | 17 | 13 | 21 |
| III | 41 | 38 | 46 | 44 | 49 | 45 |
| IV | 24 | 28 | 27 | 26 | 44 | 32 |
| V | 22 | 24 | 21 | 24 | 25 | 26 |
| All | 140 | 140 | 140 | 140 | 140 | 140 |
| Serum Creatinine ≤ 124 μmol/L | |||||
|---|---|---|---|---|---|
| Method | N | Mean | SD | SE | p |
| 24-h Creat Cl | 53 | 106.26 | 64.38 | 8.84 | - |
| Cockcroft-Gault | 53 | 105.72 | 65.27 | 8.97 | 0.92 |
| MDRD | 53 | 109.79 | 69.48 | 9.54 | 0.66 |
| CKD-EPIcrea | 53 | 99.11 | 37.19 | 5.11 | 0.25 |
| CKD-EPIcys | 53 | 61.02 | 26.88 | 3.69 | <0.05 |
| CKD-EPIcre/cys | 53 | 77.47 | 32.29 | 4.44 | <0.05 |
| Serum Creatinine > 124 μmol/L | |||||
| 24-h Creat Cl | 87 | 30.80 | 22.96 | 2.46 | - |
| Cockcroft-Gault | 87 | 29.55 | 20.03 | 2.15 | 0.32 |
| MDRD | 87 | 28.74 | 16.48 | 1.77 | 0.16 |
| CKD-EPIcr | 87 | 27.78 | 16.76 | 1.80 | <0.05 |
| CKD-EPIcys | 87 | 23.14 | 11.90 | 1.28 | <0.05 |
| CKD-EPIcrea/cys | 87 | 24.32 | 13.45 | 1.44 | <0.05 |
| <60 years | |||||
| Method | N | Mean | SD | SE | p |
| 24-h CrCl | 73 | 79.96 | 62.77 | 7.35 | - |
| Cockcroft-Gault | 73 | 83.33 | 67.24 | 7.87 | 0.36 |
| MDRD | 73 | 78.52 | 73.56 | 8.61 | 0.80 |
| CKD-EPIcrea | 73 | 71.37 | 49.39 | 5.78 | 0.05 |
| CKD-EPIcys | 73 | 46.89 | 30.79 | 3.60 | <0.05 |
| CKD-EPIcrea/cys | 73 | 57.15 | 40.00 | 4.68 | <0.05 |
| 60 years and over | |||||
| 24-h CrCl | 67 | 36.94 | 25.85 | 3.40 | - |
| CG | 67 | 31.21 | 20.08 | 2.45 | <0.05 |
| MDRD | 67 | 38.61 | 26.28 | 3.21 | 0.40 |
| CKD-EPIcrea | 67 | 36.72 | 26.43 | 3.23 | 0.91 |
| CKD-EPIcys | 67 | 27.22 | 15.20 | 1.86 | <0.05 |
| CKD-EPIcrea/cys | 67 | 30.60 | 18.65 | 2.28 | <0.05 |
| Males | |||||
| Method | N | Mean | SD | SE | p |
| 24-h CrCl | 65 | 60.42 | 54.15 | 6.72 | - |
| Cockcroft-Gault | 65 | 52.57 | 47.29 | 5.74 | < 0.05 |
| MDRD | 65 | 53.92 | 41.57 | 5.16 | 0.12 |
| CKD-EPIcrea | 65 | 51.63 | 35.76 | 4.44 | <0.05 |
| CKD-EPIcys | 65 | 37.34 | 24.46 | 3.03 | <0.05 |
| CKD-EPIcrea/cys | 65 | 42.82 | 28.96 | 3.59 | <0.05 |
| Females | |||||
| 24-h CrCl | 75 | 58.47 | 59.34 | 6.85 | - |
| Cockcroft-Gault | 75 | 63.43 | 64.29 | 7.42 | 0.13 |
| MDRD | 75 | 64.19 | 71.33 | 8.24 | 0.21 |
| CKD-EPIcrea | 75 | 57.52 | 49.40 | 5.71 | 0.77 |
| CKD-EPIcys | 75 | 37.60 | 28.17 | 3.25 | <0.05 |
| CKD-EPIcr-cys | 75 | 45.85 | 38.34 | 4.43 | <0.05 |
| CrCl < 60 mL/min | |||||
| Method | N | Mean | SD | SE | p |
| 24-h CrCl | 87 | 26.92 | 16.12 | 1.73 | - |
| Cockcroft-Gault | 87 | 28.47 | 19.77 | 2.12 | 0.26 |
| MDRD | 87 | 30.13 | 19.47 | 2.09 | <0.05 |
| CKD-EPIcrea | 87 | 29.24 | 20.22 | 2.17 | 0.07 |
| CKD-EPIcys | 87 | 22.53 | 11.18 | 1.20 | <0.05 |
| CKD-EPIcr/cys | 87 | 24.52 | 14.14 | 1.52 | <0.05 |
| CrCl ≥ 60 mL/min | |||||
| 24-h CrCl | 53 | 112.64 | 59.49 | 8.17 | - |
| Cockcroft-Gault | 53 | 107.49 | 63.22 | 8.68 | 0.31 |
| MDRD | 53 | 107.51 | 70.84 | 9.73 | 0.52 |
| CKD-EPIcrea | 53 | 96.72 | 38.87 | 5.34 | <0.05 |
| CKD-EPIcys | 53 | 62.02 | 25.91 | 3.56 | <0.05 |
| CKD-EPIcr/cys | 53 | 77.15 | 32.33 | 4.44 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tapper, M.; McGrowder, D.A.; Dilworth, L.; Soyibo, A. Prospective Comparison of 24-Hour Urine Creatinine Clearance with Estimated Glomerular Filtration Rates in Chronic Renal Disease Patients of African Descent. Medicines 2021, 8, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8090048
Tapper M, McGrowder DA, Dilworth L, Soyibo A. Prospective Comparison of 24-Hour Urine Creatinine Clearance with Estimated Glomerular Filtration Rates in Chronic Renal Disease Patients of African Descent. Medicines. 2021; 8(9):48. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8090048
Chicago/Turabian StyleTapper, Marlene, Donovan A. McGrowder, Lowell Dilworth, and Adedamola Soyibo. 2021. "Prospective Comparison of 24-Hour Urine Creatinine Clearance with Estimated Glomerular Filtration Rates in Chronic Renal Disease Patients of African Descent" Medicines 8, no. 9: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines8090048