
Epidemiology and Clinical Characteristics of People with Confirmed SARS-CoV-2 Infection during the Early COVID-19 Pandemic in Saudi Arabia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Data Collection
2.3. Data and Statistical Analyses
3. Results
3.1. Summary of Demographic Characteristics and Clinical Data
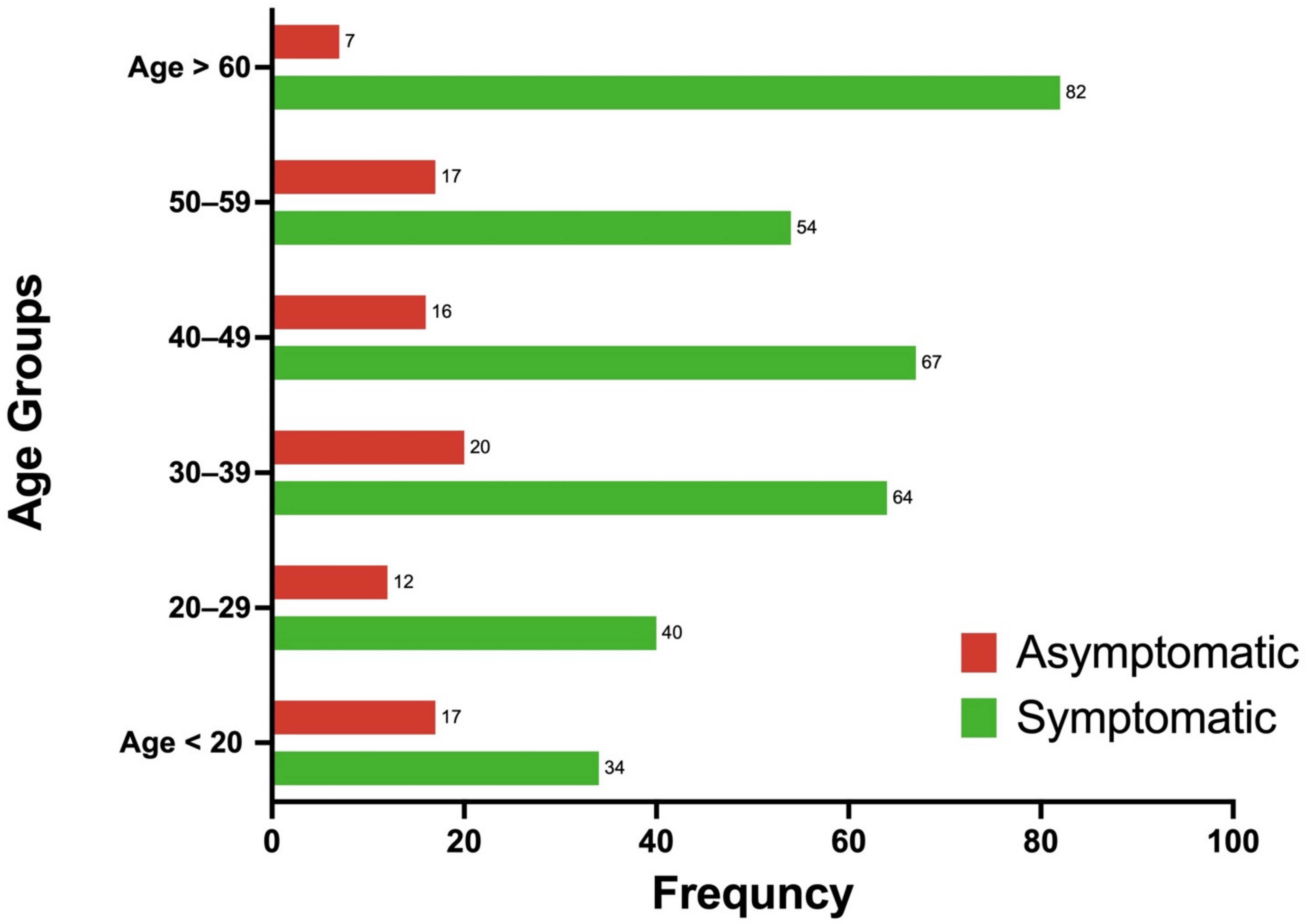
Demographic and Clinical Characteristics of Symptomatic vs. Asymptomatic Patients
3.2. Variation in Disease Incubation Times
3.3. Demographical and Clinical Characteristics Associated with Death Due to COVID-19
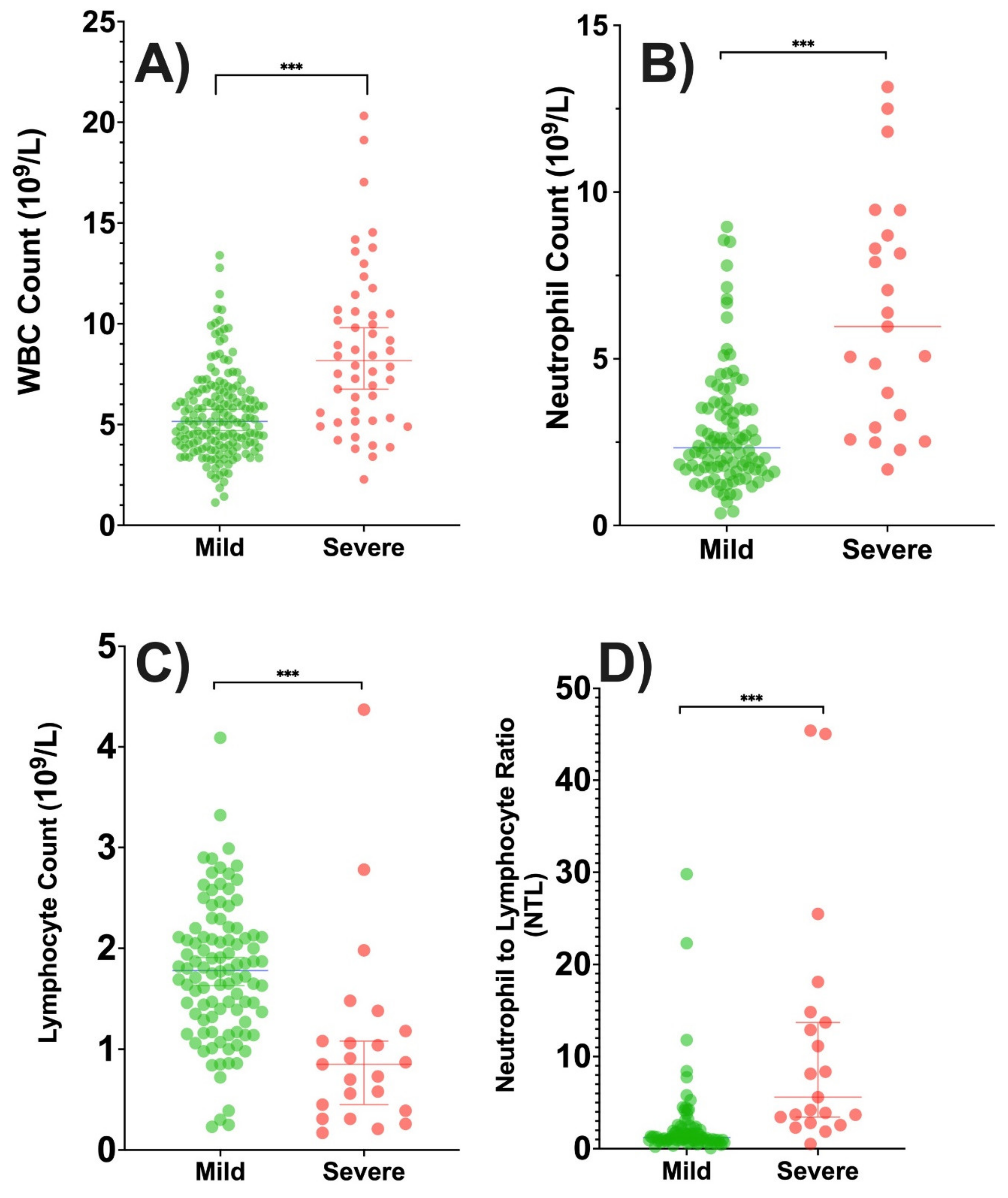
3.4. Association of Immunological Factors with Patient Outcomes, Symptoms, and Treatment Regimen
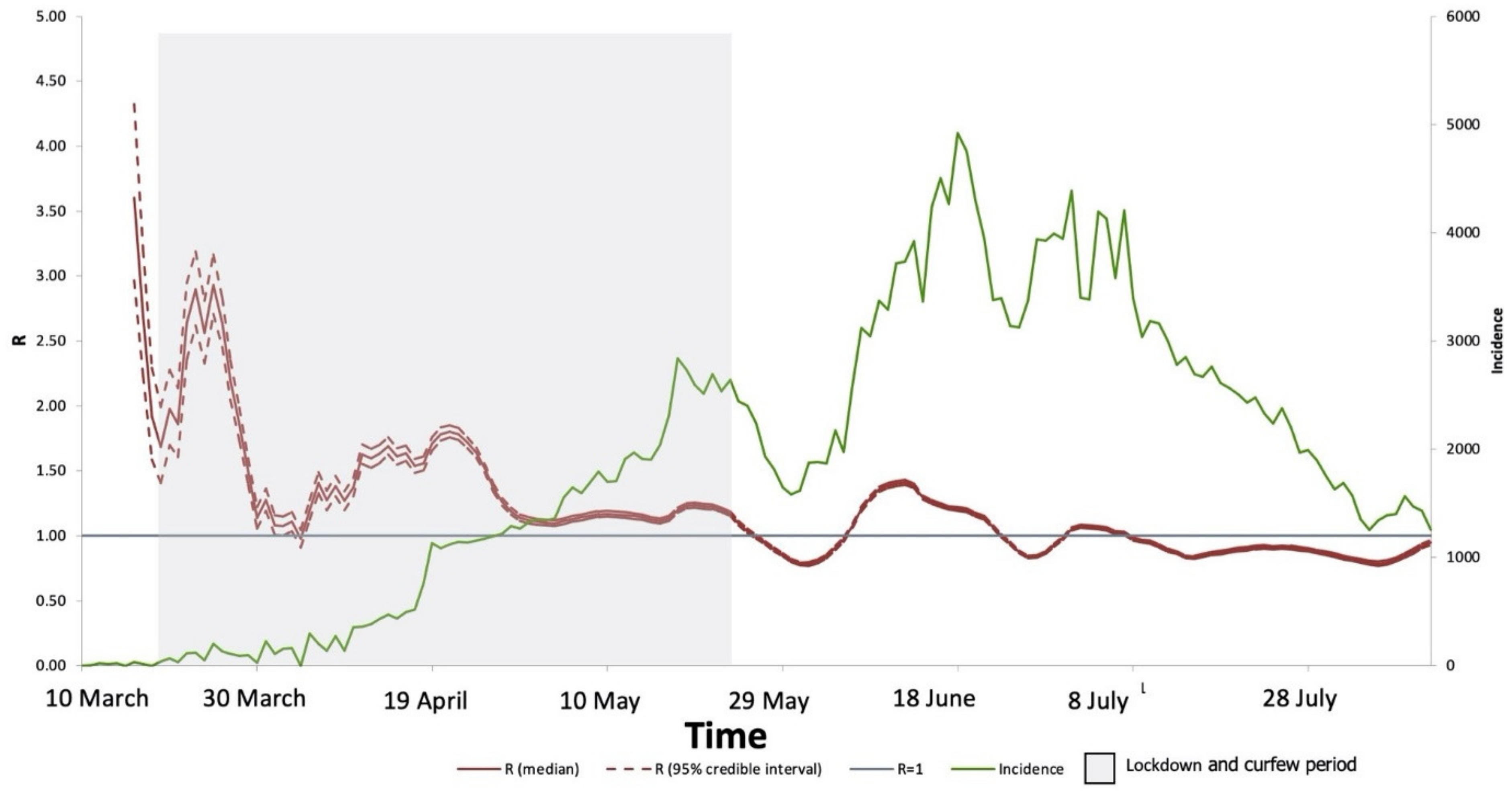
3.5. Reproduction Number Estimations and Predicting COVID-19 in Riyadh
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Obied, D.A.; Alhamlan, F.S.; Al-Qahtani, A.A.; Al-Ahdal, M.N. Containment of COVID-19: The unprecedented response of Saudi Arabia. J. Infect. Dev. Ctries. 2020, 14, 699–706. [Google Scholar] [CrossRef]
- MOH. Available online: https://covid19.moh.gov.sa/ (accessed on 7 June 2021).
- Stat, W. COVID-19 Coronavirus Pandemic Statistics. 2021. Available online: https://www.worldometers.info/coronavirus/ (accessed on 20 June 2021).
- Saudi Ministry of Health. Protocol for Patients Suspected of/Confirmed with COVID-19. 2020. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/covid19.aspx (accessed on 20 July 2021).
- Gao, J.; Tian, Z.; Yang, X. Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies. Biosci. Trends 2020, 14, 72–73. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe COVID-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Snow, E.K.; Miller, J.L.; Kester, L.; Mendham, N.A.; Heydorn, J.D.; Huang, S.C.; Leu, L.L.; Kohoutek, L.M.; Rosanelli, N.C.; Harves, K.M. Creation and maintenance of a table for assessment of evolving evidence for COVID-19–related treatments. Am. J. Heal. Pharm. 2020, 78, 154–157. [Google Scholar] [CrossRef]
- Hung, I.F.-N.; Lung, K.-C.; Tso, E.Y.-K.; Liu, R.; Chung, T.W.-H.; Chu, M.-Y.; Ng, Y.-Y.; Lo, J.; Chan, J.; Tam, A.R.; et al. Triple combination of interferon beta-1b, lopinavir–ritonavir, and ribavirin in the treatment of patients admitted to hospital with COVID-19: An open-label, randomised, phase 2 trial. Lancet 2020, 395, 1695–1704. [Google Scholar] [CrossRef]
- Cori, A.; Ferguson, N.M.; Fraser, C.; Cauchemez, S. A New Framework and Software to Estimate Time-Varying Reproduction Numbers During Epidemics. Am. J. Epidemiol. 2013, 178, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Nishiura, H.; Linton, N.M.; Akhmetzhanov, A.R. Serial interval of novel coronavirus (COVID-19) infections. Int. J. Infect. Dis. 2020, 93, 284–286. [Google Scholar] [CrossRef]
- Abbott, S.; Hellewell, J.; Munday, J.; Funk, S. The transmissibility of novel Coronavirus in the early stages of the 2019-20 outbreak in Wuhan: Exploring initial point-source exposure sizes and durations using scenario analysis. Wellcome Open Res. 2020, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.-j.; Ni, Z.-y.; Hu, Y.; Liang, W.-h.; Ou, C.-q.; He, J.-x.; Liu, L.; Shan, H.; Lei, C.-l.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.M. Coronavirus: Why Men are More Vulnerable to COVID-19 than Women? SN Compr. Clin. Med. 2020, 2, 874–876. [Google Scholar] [CrossRef]
- Hägg, S.; Jylhävä, J.; Wang, Y.; Xu, H.; Metzner, C.; Annetorp, M.; Garcia-Ptacek, S.; Khedri, M.; Boström, A.-M.; Kadir, A.; et al. Age, frailty, and comorbidity as prognostic factors for short-term outcomes in patients with Coronavirus disease 2019 in geriatric care. J. Am. Med Dir. Assoc. 2020, 21, 1555–1559.e2. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Fernandez Garcia, L.; Puentes Gutierrez, A.B.; Garcia Bascones, M. Relationship between obesity, diabetes and ICU admission in COVID-19 patients. Med. Clin. 2020, 155, 314–315. [Google Scholar] [CrossRef]
- COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Alene, M.; Yismaw, L.; Assemie, M.A.; Ketema, D.B.; Gietaneh, W.; Birhan, T.Y. Serial interval and incubation period of COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- WHO. Coronavirus. 2020. Available online: https://www.who.int/health-topics/coronavirus (accessed on 20 June 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Luzi, L.; Radaelli, M.G. Influenza and obesity: Its odd relationship and the lessons for COVID-19 pandemic. Acta Diabetol. 2020, 57, 759–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takla, M.; Jeevaratnam, K. Chloroquine, hydroxychloroquine, and COVID-19: Systematic review and narrative synthesis of efficacy and safety. Saudi Pharm. J. 2020, 28, 1760–1776. [Google Scholar] [CrossRef] [PubMed]
- Axfors, C.; Schmitt, A.M.; Janiaud, P.; van’t Hooft, J.; Abd-Elsalam, S.; Abdo, E.F.; Abella, B.S.; Akram, J.; Amaravadi, R.K.; Angus, D.C.; et al. Mortality outcomes with hydroxychloroquine and chloroquine in COVID-19 from an international collaborative meta-analysis of randomized trials. Nat. Commun. 2021, 12, 2349. [Google Scholar] [CrossRef] [PubMed]
- RECOVERY Collaborative Group. Lopinavir-ritonavir in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Effect of Hydroxychloroquine in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- WHO Solidarity Trial Consortium. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497–511. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Bruno, R.; Cauda, R.; Gialluisi, A.; Guaraldi, G.; et al. Lopinavir/Ritonavir and Darunavir/Cobicistat in Hospitalized COVID-19 Patients: Findings from the Multicenter Italian CORIST Study. Front. Med. 2021, 8, 639970. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. of Patients | Percentage of Total Patients | χ2 (p-Value) |
|---|---|---|---|
| Age | 16.23 (0.01) | ||
| <20 | 66 | 13.4 | |
| 21–30 | 61 | 12.4 | |
| 31–40 | 98 | 19.9 | |
| 41–50 | 88 | 17.9 | |
| 51–60 | 78 | 15.9 | |
| >60 | 100 | 20.4 | |
| Sex | 3.1 (0.076) | ||
| Male | 262 | 54.0 | |
| Female | 223 | 45.9 | |
| Unknown | 6 | NA* | |
| Nationality | |||
| Saudi | 372 | 77.8 | 148 (<0.0001) |
| Non-Saudi | 106 | 22.2 | |
| Unknown | 13 | NA* | |
| Other nationalities | |||
| Bangladesh | 6 | 7.1 | |
| British | 2 | 2.4 | |
| Canadian | 1 | 1.2 | |
| Egyptian | 2 | 2.4 | |
| Filipino | 25 | 29.4 | |
| Indian | 19 | 22.4 | |
| Jordanian | 7 | 8.2 | |
| Lebanese | 1 | 1.2 | |
| Nigerian | 1 | 1.2 | |
| Pakistani | 9 | 10.6 | |
| Sudanese | 7 | 8.2 | |
| Swiss | 1 | 1.2 | |
| Syrian | 1 | 1.2 | |
| Yemeni | 1 | 1.2 | |
| Saudi city or region | |||
| Riyadh | 377 | 79 | 3541 (0.0001) |
| Jeddah | 72 | 15.1 | |
| Eastern Region | 10 | 2.1 | |
| Ahsa | 2 | 0.4 | |
| Albaha | 1 | 0.2 | |
| Asir | 2 | 0.4 | |
| Hail | 1 | 0.2 | |
| Jazan | 1 | 0.2 | |
| Madinah | 1 | 0.2 | |
| Najran | 3 | 0.6 | |
| Northern Borders | 3 | 0.6 | |
| Tabouk | 2 | 0.4 | |
| Unknown | 14 | NA * | |
| Smoking status | 223 (<0.0001) | ||
| Smoker | 43 | 11.4 | |
| Nonsmoker | 333 | 88.6 | |
| Unreporte | 115 | NA * | |
| Pregnant | 177 (<0.001) | ||
| Yes | 11 | 5.02 | |
| No | 208 | 94.9 | |
| Unreported | 272 | NA * | |
| HCW | 32 (<0.0001) | ||
| Yes | 110 | 23.2 | |
| No | 169 | 35.6 | |
| Unknown | 212 | NA * | |
| BMI (kg/m2) | 168 (<0.0001) | ||
| <18.5 | 166 | 49.3 | |
| 19–30 | 7 | 1.9 | |
| 25–30 | 56 | 15.9 | |
| >30 | 122 | 34.8 | |
| Unknown | 140 | NA * | |
| Body temperature >38 °C | 261 (<0.001) | ||
| Yes | 154 | 32.9 | |
| No | 257 | 54.8 | |
| Not assessed | 58 | 12.3 | |
| Dry Cough | |||
| Yes | 152 | 32.1 | 126 (<0.001) |
| No | 244 | 51.6 | |
| Not assessed | 77 | 16.3 | |
| Runny Nose | |||
| Yes | 72 | 15.4 | 174 (<0.001) |
| No | 289 | 61.7 | |
| Not assessed | 107 | 22.9 | |
| Myalgia fatigue | |||
| Yes | 113 | 21.2 | 82 (<0.001) |
| No | 248 | 53.1 | |
| Not assessed | 106 | 22.7 | |
| Chest Radiograph | 56 (<0.001) | ||
| Normal | 231 | 49.6 | |
| Abnormal | 110 | 23.6 | |
| Not assessed | 125 | 26.8 | |
| Intensive care unit | |||
| Yes | 100 | 21.8 | 222.2 (<0.001) |
| No | 301 | 65.7 | |
| Not assessed | 33 | NA * | |
| Mechanical ventilation | |||
| Yes | 55 | 12.1 | 327.5 (<0.001) |
| No | 333 | 73.4 | |
| Unknow | 103 | NA * | |
| Comorbidities | |||
| Yes | 206 | 41.9 | 12 (<0.0001) |
| No | 285 | 58.0 | |
| Diabetes mellitus | |||
| Yes | 101 | 20.5 | 170 (<0.0001) |
| No | 390 | 79.4 | |
| Hypertension | 128 (<0.0001) | ||
| Yes | 120 | 24.4 | |
| No | 371 | 75.6 | |
| Outcome on day 14 | |||
| Recovered | 65 | 16.1 | 220 (<0.001) |
| Death | 6 | 1.5 | |
| Discharge | 34 | 8.4 | |
| Persistent disease | 134 | 33.2 | |
| Not documented | 252 | NA * | |
| Travel to countries outside Saudi Arabia | 218.9 (<0.0001) | ||
| Yes | 31 | 6.5 | |
| No | 293 | 62.1 | |
| Not reported | 133 | NA * |
| Characteristic | Mean (SD) | t-Test or Wilcoxon Test (p-Value) | |
|---|---|---|---|
| Asymptomatic (n = 89) | Symptomatic (n = 340) | ||
| Age (years) | 35.4 (18.6) | 45.1 (20.5) | 4.1 (<0.0001) * |
| BMI (kg/m2) | 26.9 (6.9) | 28.6 (7.3) | 1.79 (0.074) |
| Respiratory Rate (breaths/min) | 20.5 (4.5) | 21.7 (6.4) | 1.45 (0.075) |
| Heart rate (beats/min) | 93.9 (14.9) | 92.8 (18.6) | 0.42 (0.67) |
| Systolic blood pressure (mm Hg) | 126.9 (16.2) | 128.1 (19.5) | 0.53 (0.59) |
| Diastolic blood pressure (mm Hg) | 77.5 (10.5) | 75.8 (11) | 1.15 (0.25) |
| Mean arterial blood pressure (mm Hg) | 95.2 (11.6) | 93.5 (14.4) | 0.97 (0.33) |
| Oxygen Saturation (%) | 97.4 (1.4) | 96.2 (4.7) | 3.58 (0.0004) * |
| Hemoglobin (g/L) | 135.9 (20.6) | 129.3 (22.9) | 2.18 (0.03) * |
| Platelets (109/L) | 238.0 (113.2) | 213.6 (72.2) | 1.73 (0.088) |
| White blood cell count (109/L) | 5.6 (2.4) | 5.9 (3.1) | 0.59 (0.48) |
| Neutrophil count (109/L) | 3.1 (1.9) | 3.5 (2.1) | 2.26 (0.024) a,* |
| Lymphocyte (109/L) | 1.9 (0.95) | 1.4 (0.78) | 3.72 (0.0002) a,* |
| CD4 (mm3) | 584.6 (551.7) | 523 (349) | 0.29 (0.78) |
| Neutrophil to lymphocyte ratio | 1.8 (1.1) | 3.50 (3.2) | 3.78 (0.0002) a,* |
| CD8 (mm3) | 502.3 (285) | 323.8 (257.6) | 1.56 (0.126) |
| CD19 (mm3) | 240.6 (244) | 153.7 (231) | 0.91 (0.368) |
| NK (mm3) | 212 (132) | 140.8 (128.2) | 1.13 (0.31) |
| IgG (g/L) | 13.1 (3.5) | 11.1 (3.1) | 1.42 (0.23) |
| IgM (g/L) | 4.5 (9) | 1.1 (0.57) | 0.91 (0.40) |
| IgA (g/L) | 2.56 (1.1) | 2.56 (0.94) | 0.02 (0.98) |
| ALT (U/L) | 25.4 (24.9) | 35.9 (44.1) | 2.59 (0.01) * |
| AST (U/L) | 24.7 (13.1) | 39.9 (80.6) | 2.90 (0.0004) * |
| Characteristic | Patients, No. (%) | ||
|---|---|---|---|
| Asymptomatic (n = 89) | Symptomatic (n = 340) | χ2 (p-Value) | |
| Age group, years (n = 430) | |||
| <20, n = 51 | 17 (3.9) | 34 (7.9) | 15.1 (0.0009) * |
| 21–30, n = 52 | 12 (2.8) | 40 (9.30) | |
| 31–40, n = 84 | 20 (4.6) | 64 (14.8) | |
| 41–50, n = 83 | 16 (3.7) | 67 (15.6) | |
| 51–60, n = 71 | 17 (3.9) | 54 (12.3) | |
| >60, n = 89 | 7 (1.6) | 82 (19.1) | |
| Sex, n = 430 | |||
| Male, n = 236 | 59 (13.72) | 177 (41.2) | 5.9 (0.015) * |
| Female, n = 194 | 30 (6.98) | 164 (38.1) | |
| Nationality, n = 423 | |||
| Saudi, n = 326 | 70 (16.5) | 256 (60.5) | 1.14 (0.28) |
| Non-Saudi, n = 97 | 16 (3.8) | 81 (19.2) | |
| Smoking, n = 362 | |||
| Smoker, n = 43 | 15 (4.1) | 28 (7.7) | 5.69 (0.014) * |
| Nonsmoker, n = 319 | 60 (16.5) | 259 (71.5) | |
| Pregnancy, n = 163 | |||
| Pregnant, n = 10 | 3 (1.5) | 7 (3.6) | 1.67 (0.19) |
| Not pregnant, n = 183 | 27 (13.99) | 156 (80.8) | |
| Health Care worker, n = 269 | |||
| Yes, n = 109 | 25 (9.3) | 84 (31.2) | 0.07 (0.79) |
| No, n = 160 | 39 (14.5) | 121 (44.98) | |
| Received influenza vaccine (during the last 5 years), n = 262 | |||
| Received, n = 225 | 39 (14.9) | 186 (70.9) | 4.62 (0.032) * |
| Did not receive, n = 37 | 12 (4.6) | 25 (9.54) | |
| Comorbidities, n = 430 | 13.4 (<0.0001) * | ||
| One or more, n = 169 | 50 (11.63) | 39 (9.1) | |
| None, n = 261 | 119 (26.7) | 222 (51.6) | |
| Diabetes mellitus, n = 430 | 4.1 (0.044) * | ||
| Diagnosed with illness, n = 97 | 13 (3.02) | 84 (19.5) | |
| Not diagnosed, n = 333 | 76 (17.7) | 257 (59.8) | |
| Hypertension, n = 430 | 10.1 (0.0015) * | ||
| Diagnosed with illness, n = 115 | 12 (2.8) | 11 (17.9) | |
| Not diagnosed, n = 315 | 103 (23.9) | 238 (55.4) | |
| BMI, n = 291 | 1.17 (0.75) | ||
| <18, n = 112 | 25 (8.6) | 87 (29.9) | |
| 19–30, n = 5 | 1 (0.34) | 4 (1.4) | |
| 25–30, n = 55 | 10 (3.4) | 45 (15.6) | |
| >30, n = 119 | 20 (6.9) | 99 (34.02) | |
| Chest radiograph finding, n = 417 | 32 (<0.0001) * | ||
| Normal, n = 226 | 64 (15.4) | 162 (38.9) | |
| Abnormal, n = 108 | 2 (0.48) | 106 (25.42) | |
| Not done, n = 83 | 20 (4.8) | 63 (15.11) | |
| Pneumonia treatment, n = 328 | |||
| Yes, n = 145 | 11 (2.7) | 134 (32.6) | 22.1 (<0.0001) * |
| No, n = 266 | 72 (17.5) | 194 (47.2) | |
| Outcome on day 7, n = 392 | 9.5 (0.049) * | ||
| Recovered, n = 21 | 6 (1.53) | 15 (3.8) | |
| Death, n = 1 | 0 | 1 (0.26) | |
| Discharged, n = 18 | 6 (1.53) | 12 (3.1) | |
| Persistent disease, n = 266 | 38 (9.7) | 228 (58.2) | |
| Not documented, n = 86 | 21 (5.4) | 65 (16.6) | |
| Outcome on day 14, n = 358 | |||
| Recovered, n = 63 | 17 (4.75) | 46 (12.9) | 10.7 (0.030) * |
| Death, n = 6 | 0 | 6 (1.68) | |
| Discharged, n = 33 | 9 (2.51) | 24 (6.70) | |
| Persistent disease, n = 132 | 15 (4.2) | 117 (32.7) | |
| Not documented, n = 124 | 23 (6.42) | 101 (28.21) | |
| Blood Type, n = 250 | |||
| A, n = 71 | 12 (4.8) | 59 (23.6) | 3.04 (0.38) |
| B, n = 37 | 9 (3.6) | 28 (11.2) | |
| AB, n = 8 | 0 | 8 (3.2) | |
| O, n = 134 | 22 (8.8) | 112 (44.8) | |
| RH status, n = 250 | |||
| Rh- (n = 27) | 3 (1.20) | 40 (16.0) | 0.78 (0.37) |
| Rh+ (n = 223) | 24 (9.6) | 183 (73.2) | |
| Blood culture, n = 152 | 1.8 (0.177) | ||
| Positive, n = 15 | 0 | 15 (9.9) | |
| Negative, n = 137 | 15 (9.9) | 122 (80.3) | |
| Not tested | |||
| Recovered at data collection, n = 369 | |||
| Yes, n = 149 | 52 (14.1) | 197 (53.4) | 3.8 (0.0503) |
| No, n = 120 | 15 (4.1) | 105 (28.5) | |
| Death, n = 376 | |||
| Yes, n = 22 | 1 (0.3) | 21 (5.6) | 2.8 (0.093) |
| No, n = 354 | 66 (17.6) | 288 (76.6) | |
| Characteristic | Incubation Time, Mean (SD), Days | t-Test (p-Value) |
|---|---|---|
| Age | ||
| ≤42 | 19.9 (20.2) | 2.25 (<0.0001) * |
| >42 | 24.3 (20.2) | |
| Sex | ||
| Male | 21.1 (17.5) | 0.44 (0.66) |
| Female | 22.2 (17.2) | |
| Nationality | 1.31 (0.097) | |
| Saudi | 20.6 (16.8) | |
| Non-Saudi | 25.5 (19.2) | |
| Smoking status | ||
| Smoker | 18.5 (10.8) | 0.45 (0.657) |
| Nonsmoker | 19.8 (16.5) | |
| Symptom Status | ||
| Symptomatic | 20.9 (16.1) | |
| Asymptomatic | 20.75 (20.5) | 0.07 (0.94) |
| Treatment regimen | ||
| One or none | 22.85 (18.4) | 1.06 (0.28) |
| More than two | 20.2 (15.9) | |
| Comorbidities | ||
| One or more | 23.4 (19) | 1.1 (0.27) |
| None | 20.5 (16.15) | |
| Diabetes mellitus | ||
| Diagnosed with illness | 23.8 (15.6) | 0.80 (0.43) |
| Not diagnosed | 21.1 (17.1) | |
| Hypertension | 1.1 (0.29) | |
| Diagnosed with illness | 23.8 (25.6) | |
| Not diagnosed | 20.9 (23.7) |
| Variable | Cox Regression Univariate Model HR | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Sex | |||
| Female | 1(Ref) | ||
| Male | 1.56 | 0.67–3.66 | 0.30 |
| Age | |||
| ≤42 | 1(Ref) | ||
| >42 | 10.32 | 2.4–44.3 | 0.0017 * |
| Nationality | |||
| Saudi | 1.93 | 0.557–12.2 | 0.37 |
| Non-Saudi | 1(Ref) | ||
| BMI (kg/m2) | |||
| ≤30 | 1(Ref) | ||
| >30 | 2.28 | 0.91–5.44 | 0.065 |
| Symptom status | |||
| Asymptomatic | 1(Ref) | ||
| Symptomatic | 4.68 | 0942–85 | 0.137 |
| Comorbidities | |||
| Reported | 3.42 | 1.24–12.1 | 0.0293 * |
| Not reported | 1(Ref) | ||
| Diabetes mellitus | |||
| Reported | 3.9 | 1.68–9.4 | 0.0015 * |
| Not reported | 1(Ref) | ||
| Hypertension | |||
| Reported | 5.135 | 2.2–12.5 | 0.0002 * |
| Not reported | 1(Ref) | ||
| Comorbidities related to autoimmune disorders a | 0.0093 * | ||
| Reported | 3.1 | 1.3–7.4 | |
| Not reported | 1(Ref) | ||
| Complications (Ref = no complication) | |||
| Abdominal pain | 1.67 | 0.35–4.95 | 0.48 |
| Chest radiograph (abnormal findings) | 5.4 | 1.1–97.7 | 0.102 |
| Dry cough | 2.57 | 0.97–6.92 | 0.0532 |
| Fever (>38 °C) | 1.79 | 0.72–4.63 | 0.21 |
| Myalgia fatigue | 2.26 | 0.69–7.11 | 0.1662 |
| Nausea | 2.48 | 0.67–7.62 | 0.132 |
| Productive cough | 1.77 | 0.56–4.87 | 0.29 |
| Runny nose | 0.94 | 0.15–3.45 | 0.93 |
| Sore throat | 1.18 | 0.37–3.34 | 0.76 |
| Vomiting | 2.1 | 0.45–7.1 | 0.28 |
| Treatment Option | |||
| Not given a specific drug regimen | 0.07 | 0.011–0.25 | 0.0005 * |
| Given a specific drug regimen | 1(Ref) | ||
| Azithromycin | 3.5 | 0.819–10.4 | 0.045 * |
| Not given | 1(Ref) | ||
| HCQ | 1.52 | 0.24–5.23 | 0.575 |
| Not given | 1(Ref) | ||
| Interferon | 0 | 0–154 | 0.993 |
| Not given | 1(Ref) | ||
| lopinavir/ritonavir | 19.28 | 0.98–130.4 | 0.0008 * |
| Not given | 1(Ref) | ||
| Azithromycin + HCQ | 2.21 | 0.93–5.32 | 0.071 |
| Not given | 1(Ref) | ||
| lopinavir/ritonavir + Ribavirin | 0 | 0–50.7 | 0.997 |
| Not given | 1(Ref) | ||
| Azithromycin + HCQ + lopinavir/ritonavir | 149.6 | 5.8–3808.4 | 0.0004 * |
| Not given | 1(Ref) | ||
| Pneumonia Treatment | 9.1 | 3.28–32.3 | 0.0001 * |
| Not given | 1(Ref) | ||
| Combination Therapy (2 or more) | 2.7 | 1.1–6.6 | 0.026 * |
| Not given | 1(Ref) | ||
| Received mechanical ventilation | 90 | 18.4–1624.2 | <0.0001 * |
| Not received | 1(Ref) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhamlan, F.S.; Almaghrabi, R.S.; Devol, E.B.; Alotaibi, A.B.; Alageel, S.M.; Obeid, D.A.; Alraddadi, B.M.; Althawadi, S.I.; Mutabagani, M.S.; Al-Qahtani, A.A. Epidemiology and Clinical Characteristics of People with Confirmed SARS-CoV-2 Infection during the Early COVID-19 Pandemic in Saudi Arabia. Medicines 2022, 9, 32. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines9050032
Alhamlan FS, Almaghrabi RS, Devol EB, Alotaibi AB, Alageel SM, Obeid DA, Alraddadi BM, Althawadi SI, Mutabagani MS, Al-Qahtani AA. Epidemiology and Clinical Characteristics of People with Confirmed SARS-CoV-2 Infection during the Early COVID-19 Pandemic in Saudi Arabia. Medicines. 2022; 9(5):32. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines9050032
Chicago/Turabian StyleAlhamlan, Fatimah S., Reem S. Almaghrabi, Edward B. Devol, Anwar B. Alotaibi, Saleh M. Alageel, Dalia A. Obeid, Basem M. Alraddadi, Sahar I. Althawadi, Maysoon S. Mutabagani, and Ahmed A. Al-Qahtani. 2022. "Epidemiology and Clinical Characteristics of People with Confirmed SARS-CoV-2 Infection during the Early COVID-19 Pandemic in Saudi Arabia" Medicines 9, no. 5: 32. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines9050032