Second Generation of Tissue-Engineered Ligament Substitutes for Torn ACL Replacement: Adaptations for Clinical Applications



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
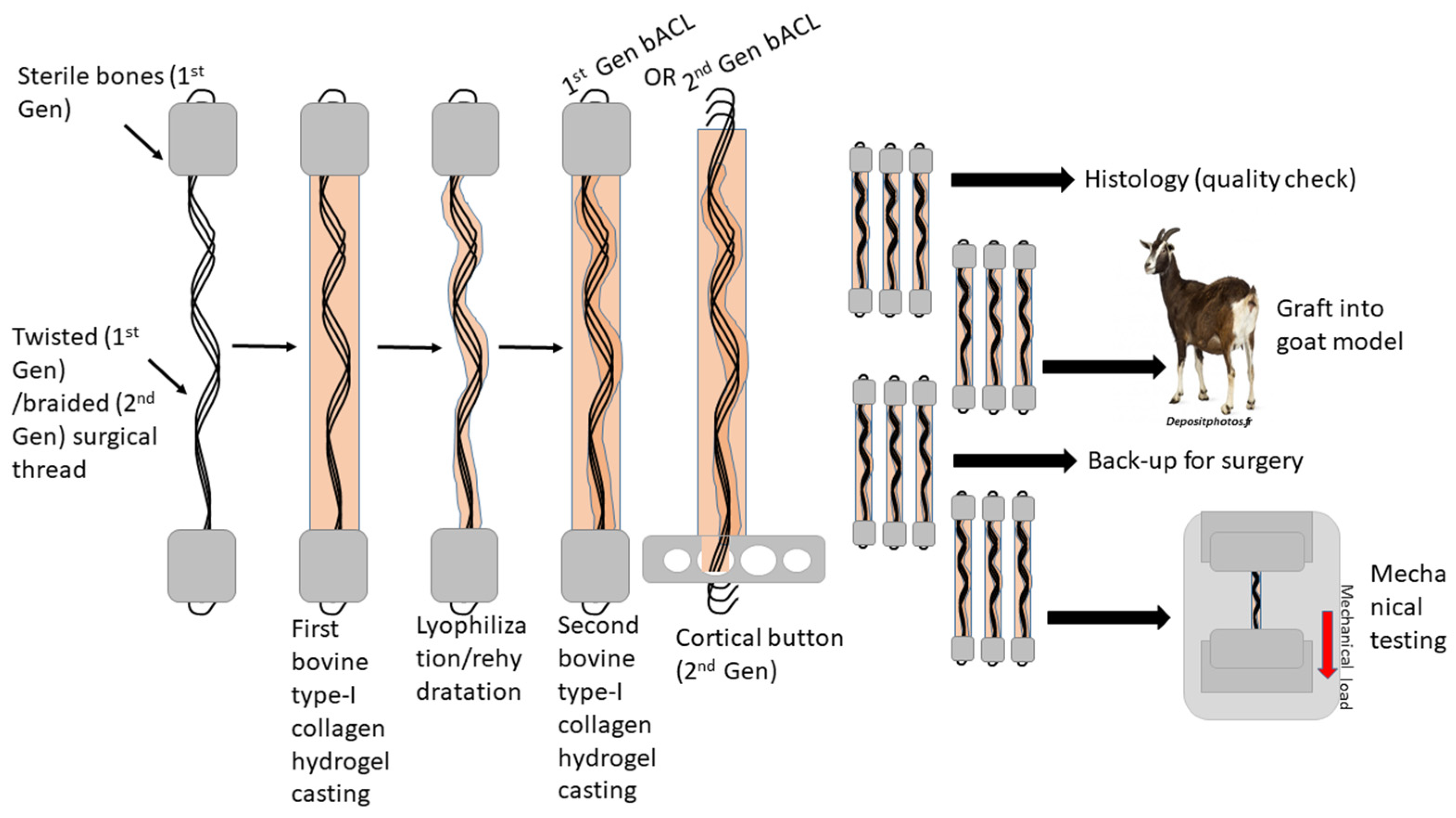
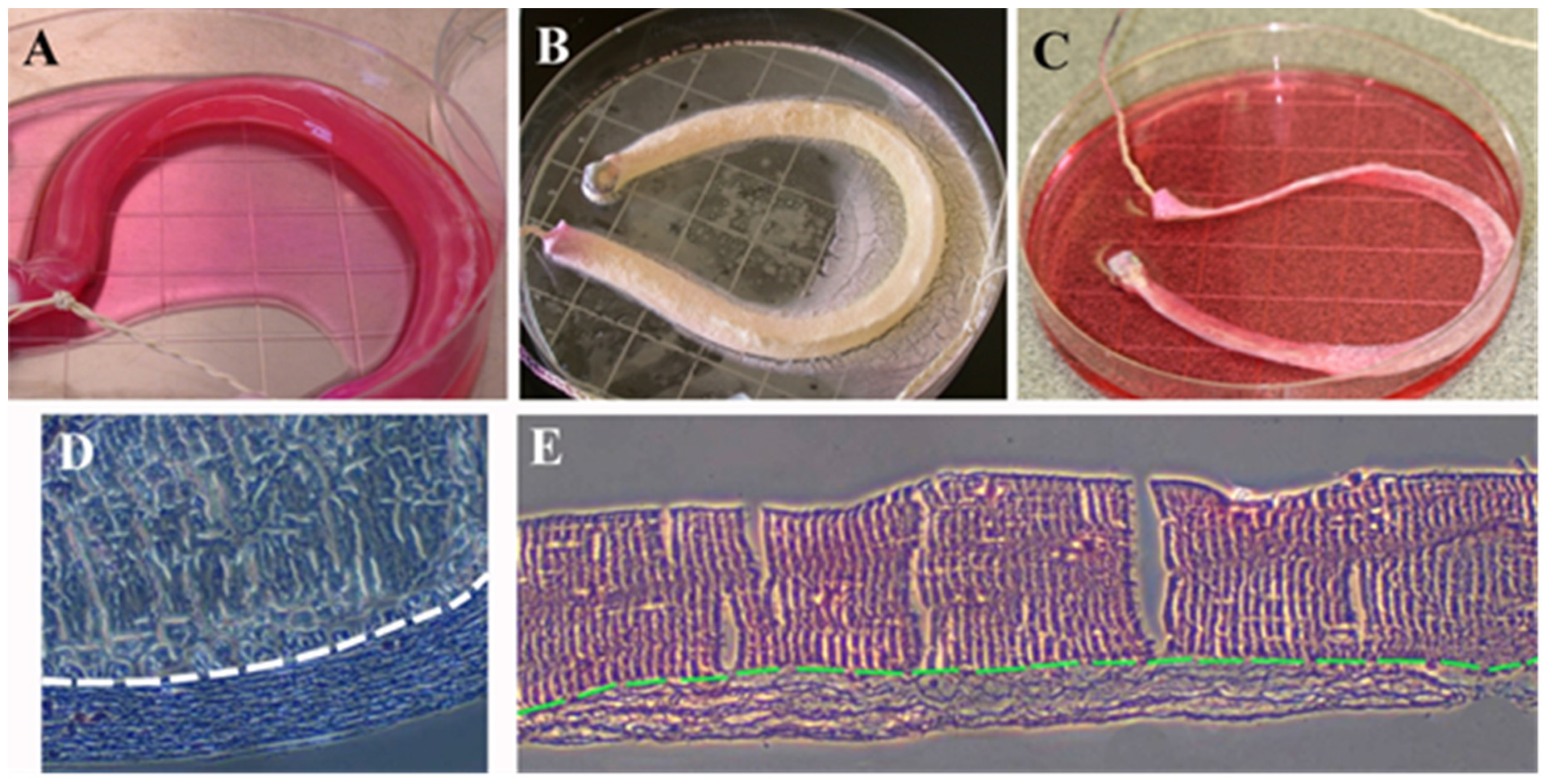
2.2. Preparation of Acellular Graftable bACLs Anchored with Bones
2.3. Surgical Procedures for Implantation of Acellular bACLs Anchored with Bones into Goats
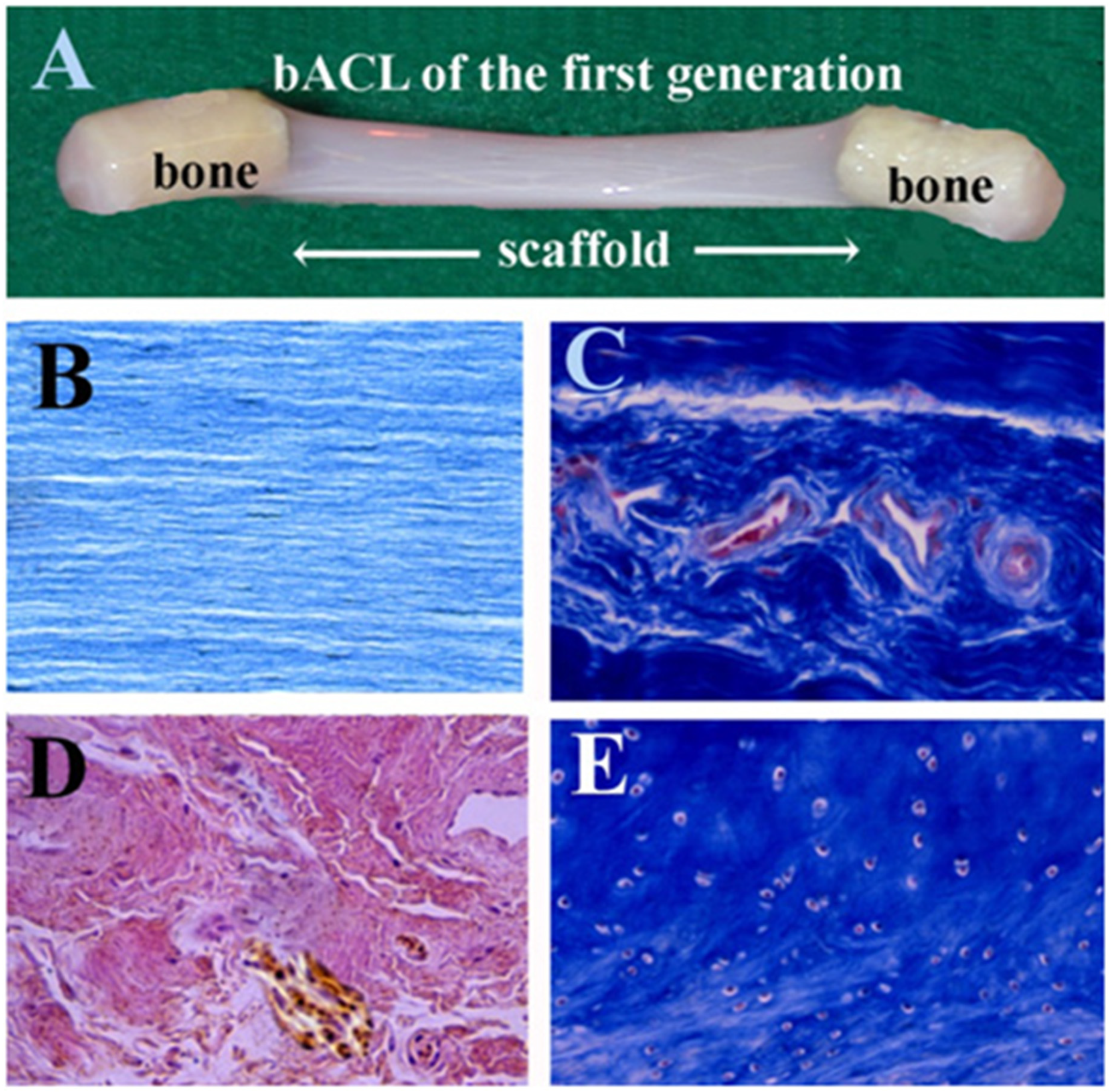
2.4. Histological Analysis of bACLs before and after Implantation, Ex Vivo
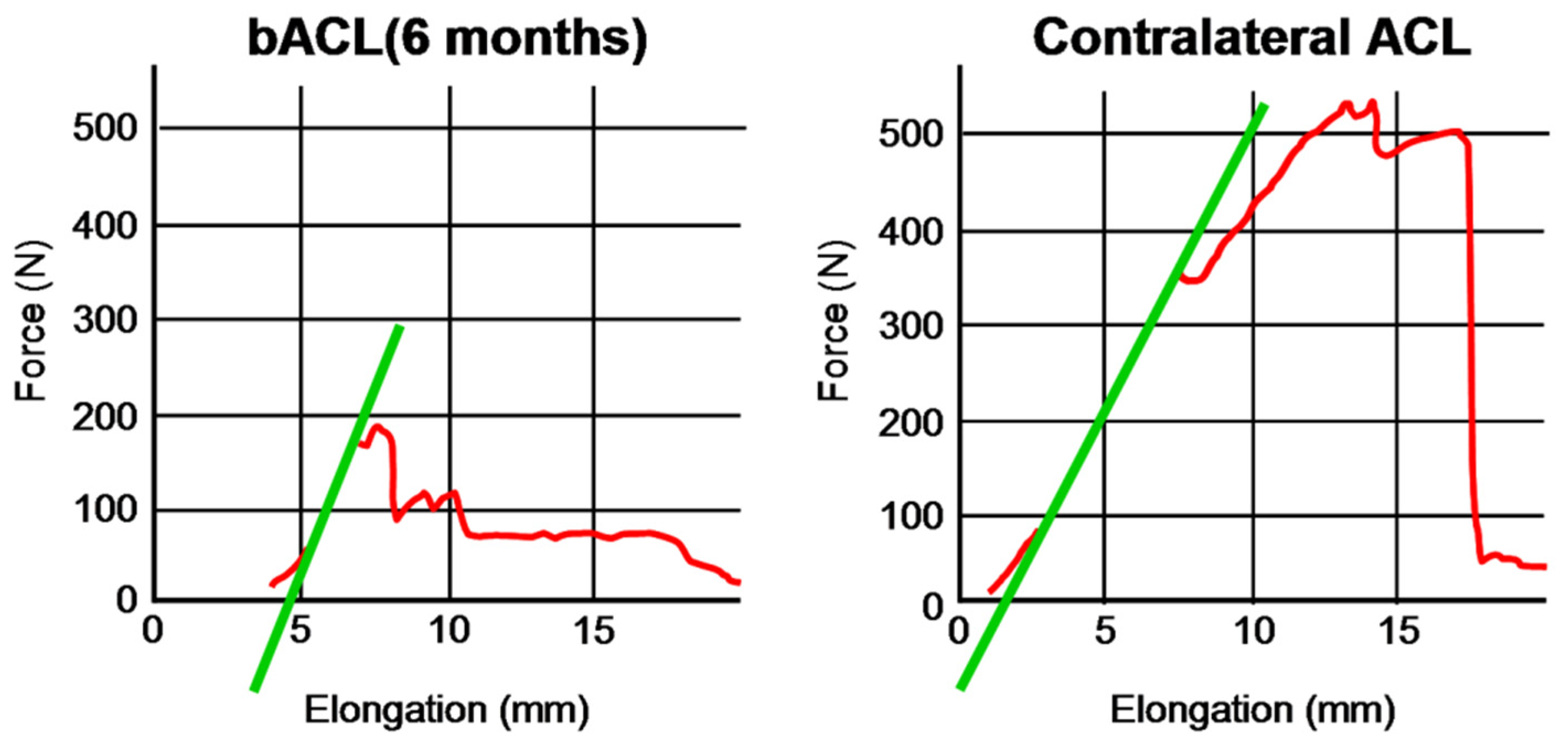
2.5. Mechanical Analyses
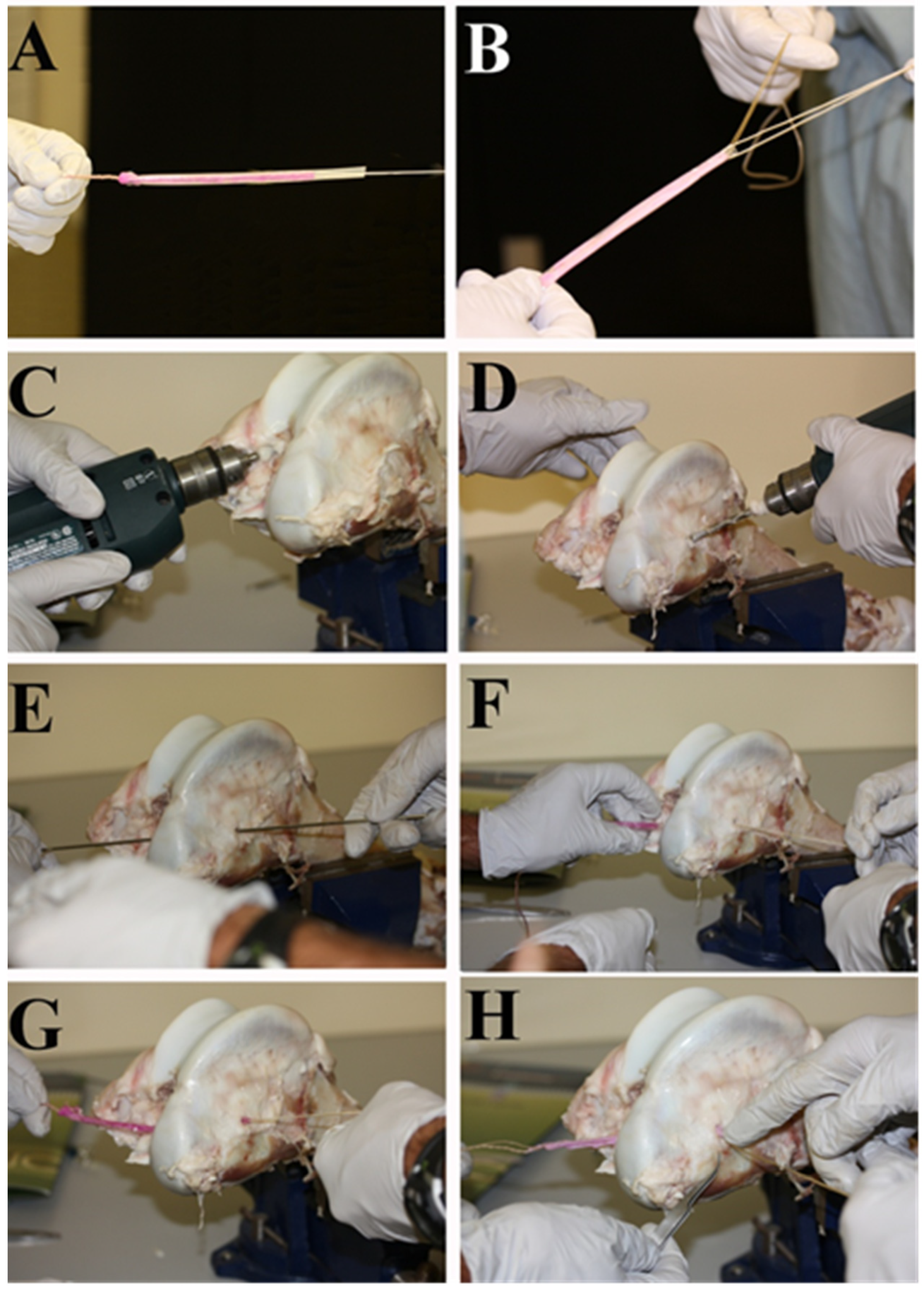
2.6. Preparation of a Second Generation of Graftable Acellular bACLs
2.7. Surgical Testing
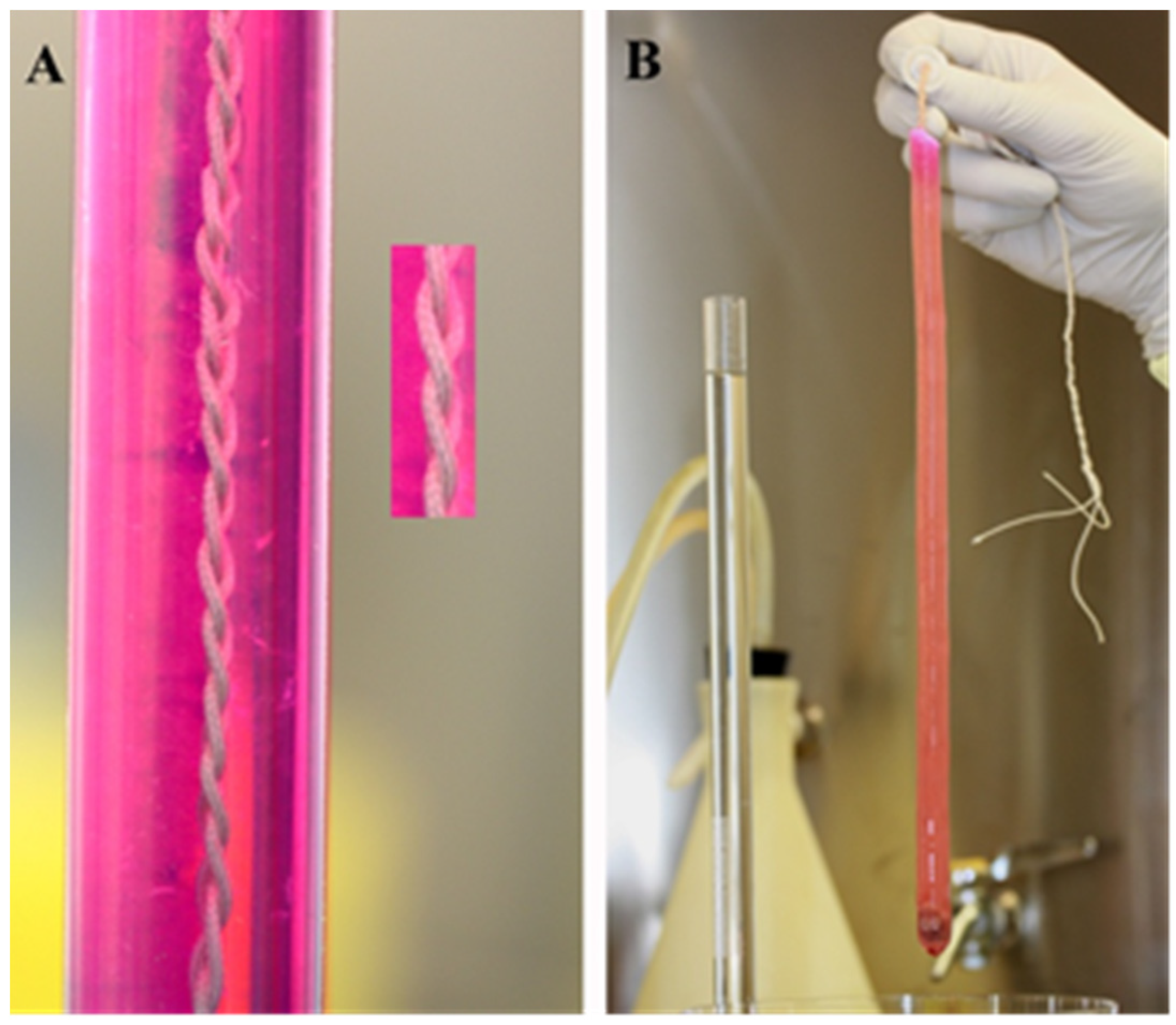
2.8. Mechanical Characterization of the Braided Thread Scaffold
2.9. Histological Analyses of the Scaffold
3. Results
3.1. Grafting of the First Generation of Acellular bACLs
3.2. Endobutton Fixations of bACLs
3.3. Strength of the Braided Thread
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J.; Larson, D.R.; Dahm, D.L.; Levy, B.A.; Stuart, M.J.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am. J. Sports Med. 2016, 44, 1502–1507. [Google Scholar] [CrossRef]
- Rayan, F.; Nanjayan, S.K.; Quah, C.; Ramoutar, D.; Konan, S.; Haddad, F.S. Review of evolution of tunnel position in anterior cruciate ligament reconstruction. World J. Orthop. 2015, 6, 252–262. [Google Scholar] [CrossRef]
- Renstrom, P.; Ljungqvist, A.; Arendt, E.; Beynnon, B.; Fukubayashi, T.; Garrett, W.; Georgoulis, T.; Hewett, T.E.; Johnson, R.; Krosshaug, T.; et al. Non-contact ACL injuries in female athletes: An International Olympic Committee current concepts statement. Br. J. Sports Med. 2008, 42, 394–412. [Google Scholar] [CrossRef] [Green Version]
- LaBella, C.R.; Hennrikus, W.; Hewett, T.E. Council on Sports Medicine and Fitness, and Section on Orthopaedics. Anterior cruciate ligament injuries: Diagnosis, treatment, and prevention. Pediatrics 2014, 133, e1437–e1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hospodar, S.J.; Miller, M.D. Controversies in ACL reconstruction: Bone-patellar tendon-bone anterior cruciate ligament reconstruction remains the gold standard. Sports Med. Arthrosc. Rev. 2009, 17, 242–246. [Google Scholar] [CrossRef]
- Koga, H.; Muneta, T.; Yagishita, K.; Watanabe, T.; Mochizuki, T.; Horie, M.; Nakamura, T.; Otabe, K.; Sekiya, I. Mid- to long-term results of single-bundle versus double-bundle anterior cruciate ligament reconstruction: Randomized controlled trial. Arthrosc. J. Arthrosc. Relat. Surg. 2015, 31, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Carey, J.L.; Spindler, K.P. Does autograft choice determine intermediate-term outcome of ACL recon-struction? Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 462–472. [Google Scholar] [CrossRef] [Green Version]
- Noyes, F.R.; Butler, D.L.; Grood, E.S.; Zernicke, R.F.; Hefzy, M.S. Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J. Bone Jt. Surg. Am. Vol. 1984, 66, 344–352. [Google Scholar] [CrossRef]
- Zhao, L.; Lu, M.; Deng, M.; Xing, J.; He, L.; Wang, C. Outcome of bone-patellar tendon-bone vs hamstring tendon autograft for anterior cruciate ligament reconstruction: A meta-analysis of randomized controlled trials with a 5-year minimum follow-up. Medicine 2020, 99, e23476. [Google Scholar] [CrossRef]
- Mather, R.C., 3rd; Hettrich, C.M.; Dunn, W.R.; Cole, B.J.; Bach, B.R., Jr.; Huston, L.J.; Reinke, E.K.; Spindler, K.P. Cost-Effectiveness Analysis of Early Reconstruction Versus Rehabili-tation and Delayed Reconstruction for Anterior Cruciate Ligament Tears. Am. J. Sports Med. 2014, 42, 1583–1591. [Google Scholar] [CrossRef]
- Mengsteab, P.Y.; Nair, L.S.; Laurencin, C.T. The past, present and future of ligament regenerative engineering. Regen. Med. 2016, 11, 871–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, F.A.; Cowden, C.H., 3rd; Sanders, E.J. Revision rates after anterior cruciate ligament reconstruction using bone-patellar tendon-bone allograft or autograft in a population 25 years old and younger. Arthrosc. J. Arthrosc. Relat. Surg. 2014, 30, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Engelman, G.H.; Carry, P.M.; Hitt, K.G.; Polousky, J.D.; Vidal, A.F. Comparison of allograft versus autograft anterior cruci-ate ligament reconstruction graft survival in an active adolescent cohort. Am. J. Sports Med. 2014, 42, 2311–2318. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A.; Leigh, W.B.; Richmond, A.K. Younger patients are at increased risk for graft rupture and contra-lateral injury after anterior cruciate ligament reconstruction. Am. J. Sports Med. 2014, 42, 641–647. [Google Scholar] [CrossRef]
- von Porat, A.; Roos, E.M.; Roos, H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: A study of radiographic and patient relevant outcomes. Ann. Rheum. Dis. 2004, 63, 269–273. [Google Scholar] [CrossRef]
- Leong, N.L.; Petrigliano, F.A.; McAllister, D.R. Current tissue engineering strategies in anterior cruciate ligament recon-struction. J. Biomed. Mater. Res. Part A 2014, 102, 1614–1624. [Google Scholar] [CrossRef] [PubMed]
- Nau, T.; Teuschl, A. Regeneration of the anterior cruciate ligament: Current strategies in tissue engineering. World J. Orthop. 2015, 6, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Goulet, F.R.D.; Cloutier, R.; Tremblay, P.; Belzil, A.M.; Lamontagne, J.; Bouchard, M.; Tremblay, J.; Stevens, L.M.; Labrosse, J.; Langelier, E.; et al. Torn ACL: A new bioengineered substitute brought from the laboratory to the knee joint. Appl. Bionics Biomech. 2004, 1, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, P.; Cloutier, R.; Lamontagne, J.; Belzil, A.-M.; Larkin, A.-M.; Chouinard, L.; Chabaud, S.; Laverty, S.; Lussier, B.; Goulet, F. Potential of skin fibroblasts for application to anterior cruciate ligament tissue engineering. Cell Transpl. 2011, 20, 535–542. [Google Scholar] [CrossRef]
- Goulet, F.C.S.; Simon, F.; Napa, I.D.; Moulin, V.; Hart, D.A. Engineering of ligaments and tendons: Potential of tis-sue-Engineered Ligament Substitutes for Ruptured ACL Replacement; InTechOpen: London, UK, 2011. [Google Scholar]
- Goulet, F.G.; Germain, L.; Cloutier, R.; Lamontagne, J.; Robitaille, H.; Boucard, L.; Auger, F.A. Tissue-engineered ACL from the laboratory to the knee joint. Can. Orthop. Assoc. Bull. 2006, 74, 35–36. [Google Scholar]
- Goulet, F.G.L.; Poole, A.R.; Auger, F.A. Tendons and Ligaments; Academic Press Ltd.: San Diego, CA, USA, 2007. [Google Scholar]
- Goulet, F.R.D.; Cloutier, R.; Germain, L.; Poole, A.R.; Auger, F.A. Tendons and Ligaments; Academic Press Ltd.: San Diego, CA, USA, 2000. [Google Scholar]
- Hart, D.A.S.N.G.; Goulet, F. Tissue engineering of ACL replacements. Sports Med. Arthrosc. Rev. 2005, 13, 170–176. [Google Scholar] [CrossRef]
- Amis, A.A.; Dawkins, G.P. Functional anatomy of the anterior cruciate ligament. Fibre bundle actions related to ligament replacements and injuries. J. Bone Jt. Surg. Br. Vol. 1991, 73, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Butler, D.L.; Kay, M.D.; Stouffer, D.C. Comparison of material properties in fascicle-bone units from human patellar tendon and knee ligaments. J. Biomech. 1986, 19, 425–432. [Google Scholar] [CrossRef]
- Cooper, J.A.; Lu, H.H.; Ko, F.K.; Freeman, J.W.; Laurencin, C.T. Fiber-based tissue-engineered scaffold for ligament replacement: Design considerations and in vitro evaluation. Biomaterials 2005, 26, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Frank, C.B. Ligament structure, physiology and function. J. Musculoskelet. Neuronal Interact. 2004, 4, 199–201. [Google Scholar]
- Gurlek, A.C.; Sevinc, B.; Bayrak, E.; Erisken, C. Synthesis and characterization of polycaprolactone for anterior cruciate ligament regeneration. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 71, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Lin, V.S.; Lee, M.C.; O’Neal, S.; McKean, J.; Sung, K.L. Ligament tissue engineering using synthetic biodegradable fiber scaffolds. Tissue Eng. 1999, 5, 443–452. [Google Scholar] [CrossRef]
- Lu, H.H.; Cooper, J.A., Jr.; Manuel, S.; Freeman, J.W.; Attawia, M.A.; Ko, F.K.; Laurencin, C.T. Anterior cruciate ligament regeneration using braided biodegradable scaffolds: In vitro optimization studies. Biomaterials 2005, 26, 4805–4816. [Google Scholar] [CrossRef]
- Laurencin, C.T.; Freeman, J.W. Ligament tissue engineering: An evolutionary materials science approach. Biomaterials 2005, 26, 7530–7536. [Google Scholar] [CrossRef]
- Teuschl, A.; Heimel, P.; Nürnberger, S.; van Griensven, M.; Redl, H.; Nau, T. A Novel Silk Fiber-Based Scaffold for Regeneration of the Anterior Cruciate Ligament: Histological Results from a Study in Sheep. Am. J. Sports Med. 2016, 44, 1547–1557. [Google Scholar] [CrossRef]
- Altman, G.H.; Horan, R.L.; Lu, H.H.; Moreau, J.; Martin, I.; Richmond, J.C.; Kaplan, D.L. Silk matrix for tissue engineered anterior cruciate ligaments. Biomaterials 2002, 23, 4131–4141. [Google Scholar] [CrossRef]
- Vaupel, P.; Schmidberger, H.; Mayer, A. The Warburg effect: Essential part of metabolic reprogramming and central contributor to cancer progression. Int. J. Radiat. Biol. 2019, 95, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.S.; Smith, S.D.; LaPrade, C.M.; Turnbull, T.L.; LaPrade, R.F.; Wijdicks, C.A. A biomechanical comparison of femoral cor-tical suspension devices for soft tissue anterior cruciate ligament reconstruction under high loads. Am. J. Sports Med. 2015, 43, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ranjan, R.; Gaba, S.; Goel, L.; Asif, N.; Kalra, M.; Kumar, R.; Kumar, A. In vivo comparison of a fixed loop (EndoButton CL) with an adjustable loop (TightRope RT) device for femoral fixation of the graft in ACL reconstruction: A prospective randomized study and a literature review. J. Orthop. Surg. 2018, 26, 2309499018799787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baj, A.; Beltramini, G.A.; Romano, M.; Lauritano, D.; Gaudio, R.M.; Palmieri, A.; Cura, F.; Giannì, A.B. Genetic effects of Vicryl® on fibroblast primary culture. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. 1), 215–220. [Google Scholar]
- Murray, M.M.; Spindler, K.P.; Devin, C.; Snyder, B.S.; Muller, J.; Takahashi, M.; Ballard, P.; Nanney, L.B.; Zurakowski, D. Use of a collagen-platelet rich plasma scaffold to stimulate healing of a central defect in the canine ACL. J. Orthop. Res. 2006, 24, 820–830. [Google Scholar] [CrossRef] [PubMed]
- Looney, A.M.; Leider, J.D.; Horn, A.R.; Bodendorfer, B.M. Bioaugmentation in the surgical treatment of anterior cruciate ligament injuries: A review of current concepts and emerging techniques. SAGE Open Med. 2020, 8, 2050312120921057. [Google Scholar] [CrossRef]
- Penkova, C.B. Stabilizing effect of glycerol on collagen type I isolated from different species. Food Chem. 1999, 66, 483–487. [Google Scholar] [CrossRef]
- Robayo, L.M.; Moulin, V.J.; Tremblay, P.; Cloutier, R.; Lamontagne, J.; Larkin, A.-M.; Chabaud, S.; Simon, F.; Islam, N.; Goulet, F. New ligament healing model based on tissue-engineered collagen scaffolds. Wound Repair Regen. Int. J. Tissue Repair Regen. 2011, 19, 38–48. [Google Scholar] [CrossRef]
- Benson, D.M.; Hopper, G.P.; Wilson, W.T.; Mackay, G.M. Anterior Cruciate Ligament Reconstruction Using Bone-Patellar Tendon-Bone Autograft With Suture Tape Augmentation. Arthrosc. Tech. 2021, 10, e249–e255. [Google Scholar] [CrossRef]
- Bédard, P.; Gauvin, S.; Ferland, K.; Caneparo, C.; Pellerin, È.; Chabaud, S.; Bolduc, S. Innovative Human Three-Dimensional Tissue-Engineered Models as an Alternative to Animal Testing. Bioengineering 2020, 7, 115. [Google Scholar] [CrossRef] [PubMed]
- Forestiero, A.; Carniel, E.L.; Natali, A.N. Biomechanical behaviour of ankle ligaments: Constitutive formulation and numerical modelling. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Orozco, G.A.; Tanska, P.; Mononen, M.E.; Halonen, K.S.; Korhonen, R.K. The effect of constitutive representations and structural constituents of ligaments on knee joint mechanics. Sci. Rep. 2018, 8, 2323. [Google Scholar] [CrossRef] [PubMed]
- Benos, L.; Stanev, D.; Spyrou, L.; Moustakas, K.; Tsaopoulos, D.E. A Review on Finite Element Modeling and Simulation of the Anterior Cruciate Ligament Reconstruction. Front. Bioeng. Biotechnol. 2020, 8, 967. [Google Scholar] [CrossRef]
- Forestiero, A.; Carniel, E.L.; Fontanella, C.G.; Natali, A.N. Numerical model for healthy and injured ankle ligaments. Australas. Phys. Eng. Sci. Med. 2017, 40, 289–295. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Specimen Tested | Ultimate Tensile Strength (N/mm2) | Stiffness (N/mm) |
|---|---|---|
| ACL (a) | 520 ± 68 | 64 ± 11 |
| bACL (a) | 94 ± 14 | 102 ± 15 |
| Vycril braided thread (b) | 340 ± 28 | 10.2 ± 0.3 |
| 1st Generation of Acellular bACLs | 2nd Generation of Acellular bACLs | |
|---|---|---|
| Matrix | Bovine Type I collagen hydrogel (can easily be replaced by commercially available recombinant human Type I hydrogels) | idem |
| Anchorage | Sterile bone plugs | Endobutton (cortical button) |
| (limited availability and potential regulatory issues) | ||
| Protection of the graft during implantation | None | Dialysis membrane (efficiency tested by orthopedic surgeons) |
| Advantages | Surgical procedure similar to standard BPTB procedure | All items used are commercially available and approved by the FDA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, F.; Moreira-Pereira, J.; Lamontagne, J.; Cloutier, R.; Goulet, F.; Chabaud, S. Second Generation of Tissue-Engineered Ligament Substitutes for Torn ACL Replacement: Adaptations for Clinical Applications. Bioengineering 2021, 8, 206. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120206
Simon F, Moreira-Pereira J, Lamontagne J, Cloutier R, Goulet F, Chabaud S. Second Generation of Tissue-Engineered Ligament Substitutes for Torn ACL Replacement: Adaptations for Clinical Applications. Bioengineering. 2021; 8(12):206. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120206
Chicago/Turabian StyleSimon, Franck, Jadson Moreira-Pereira, Jean Lamontagne, Rejean Cloutier, Francine Goulet, and Stéphane Chabaud. 2021. "Second Generation of Tissue-Engineered Ligament Substitutes for Torn ACL Replacement: Adaptations for Clinical Applications" Bioengineering 8, no. 12: 206. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering8120206