
3D Modeling of the Crystalline Lens Complex under Pseudoexfoliation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
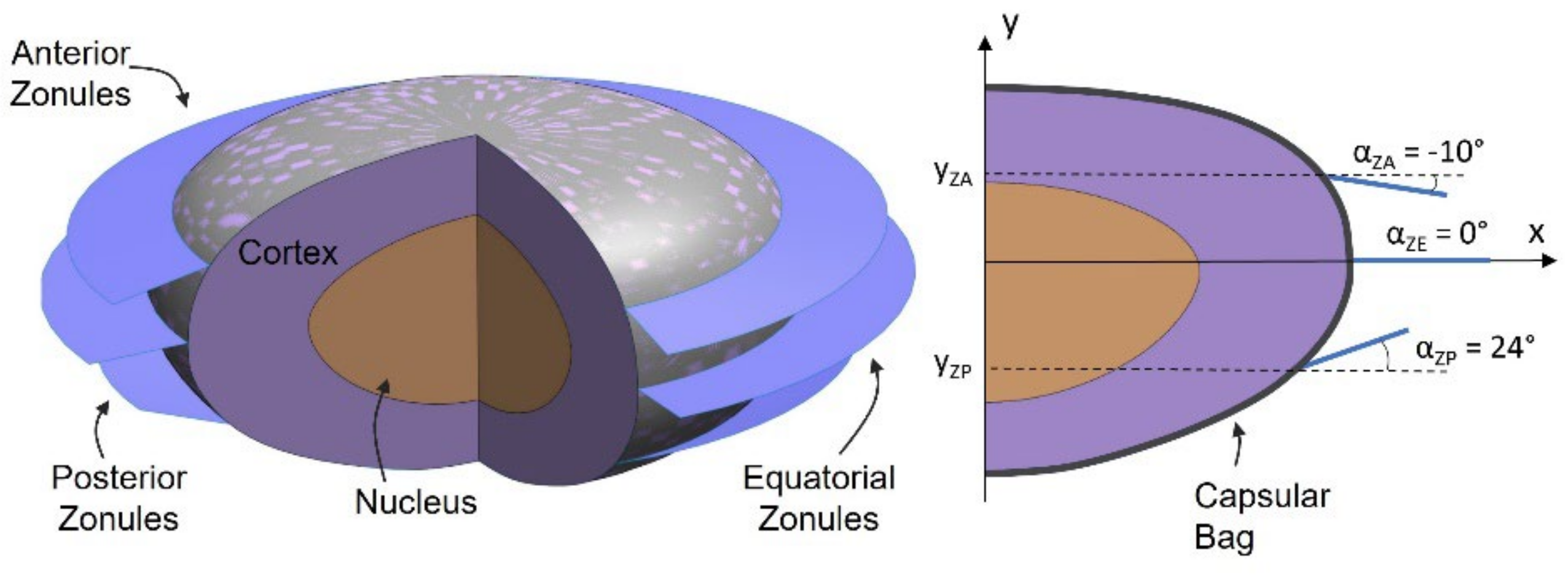
2.1. The Healthy Lens Complex
Zonular Geometry and Capsular Attachment
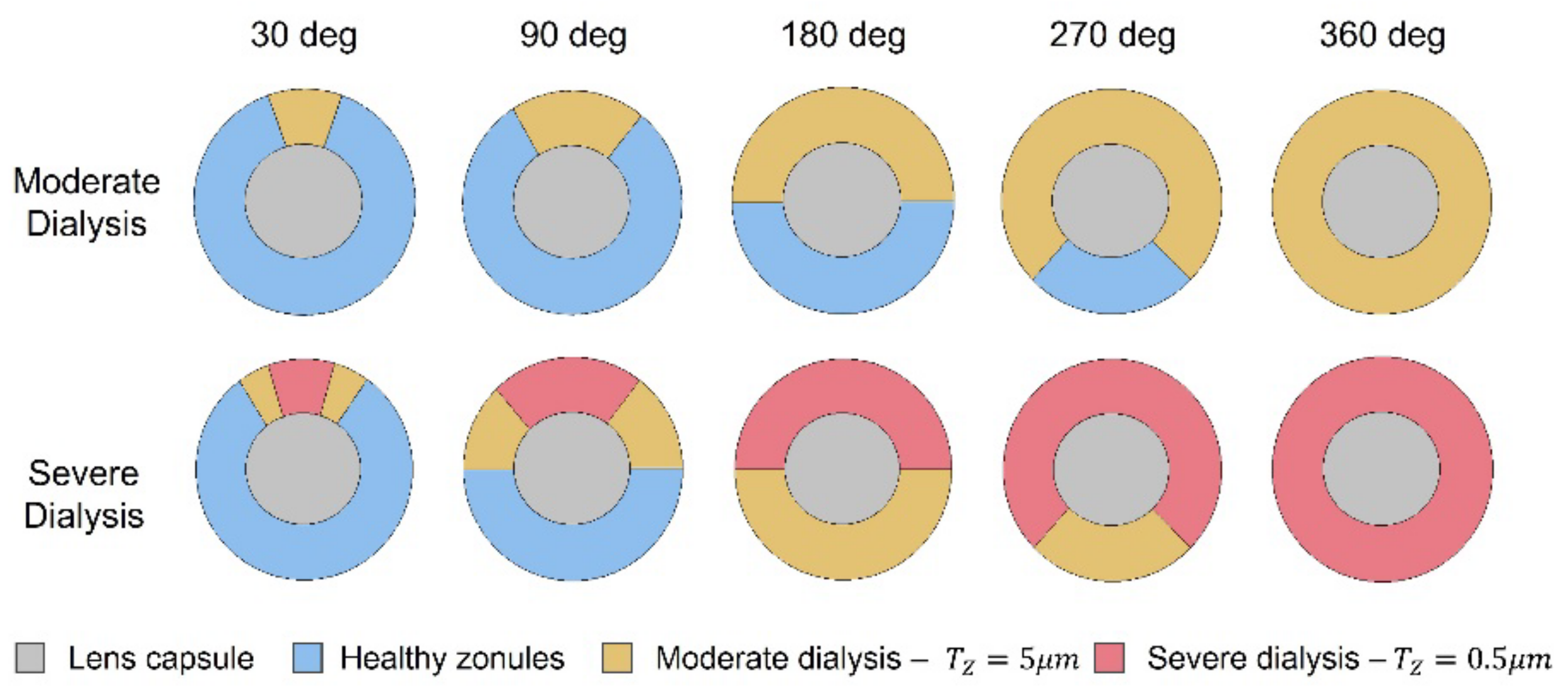
2.2. Pseudoexfoliation Syndrome
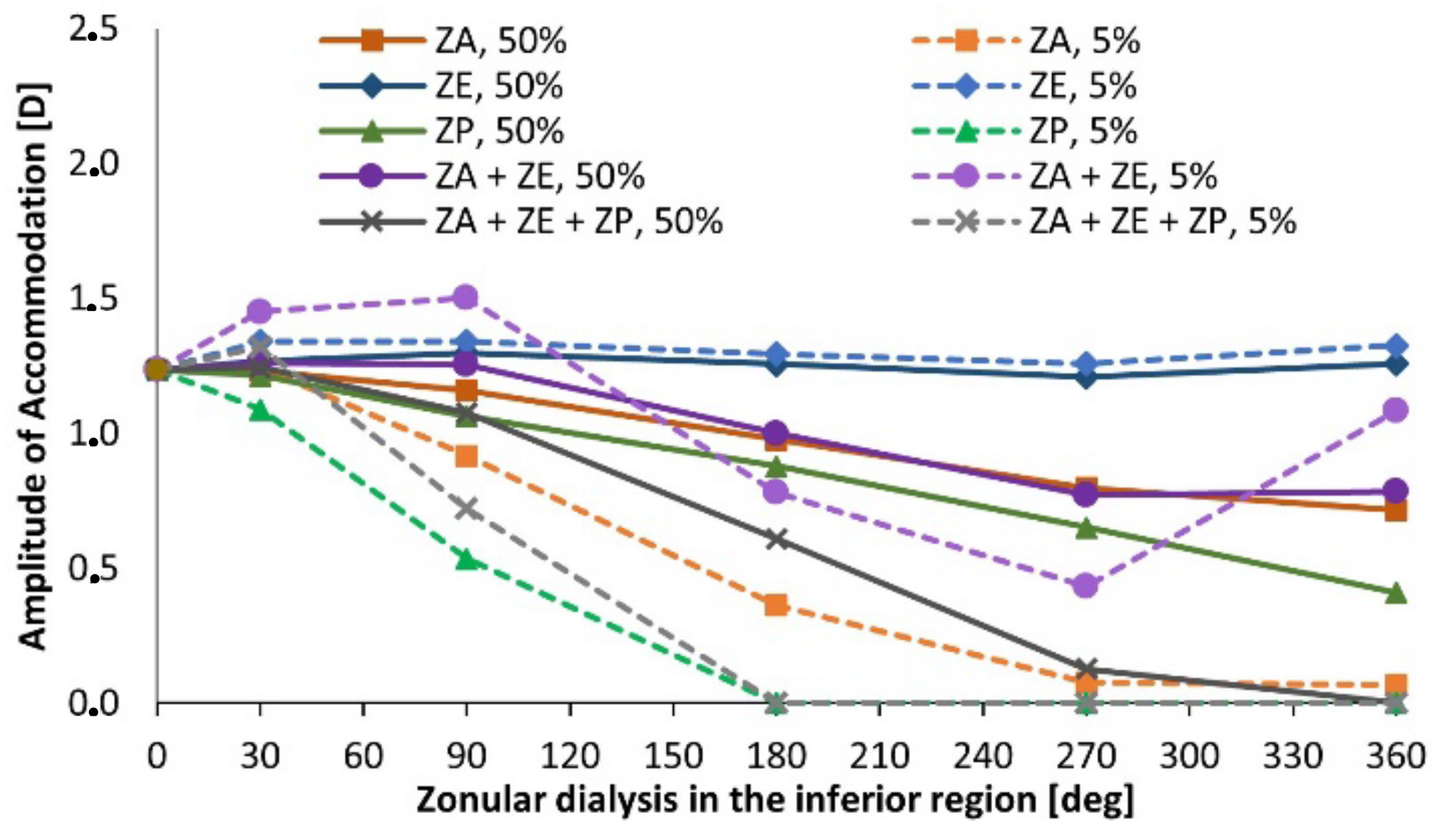
3. Results
3.1. The Healthy Lens Complex
Zonular Geometry and Capsular Attachment
3.2. Pseudoexfoliation Syndrome
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ritch, R.; Schlötzer-Schrehardt, U. Exfoliation syndrome. Surv. Ophthalmol. 2001, 45, 265–315. [Google Scholar] [CrossRef]
- Konstas, A.G.P.; Ringvold, A. Epidemiology of Exfoliation Syndrome. J. Glaucoma 2018, 27, S4–S11. [Google Scholar] [CrossRef] [PubMed]
- Yavas, G.F.; Öztürk, F.; Küsbeci, T.; Inan, Ü.; Kaplan, Ü.; Ermiş, S.S. Evaluation of the change in accommodation amplitude in subjects with pseudoexfoliation. Eye 2009, 23, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [Green Version]
- Rao, A.; Padhy, D. Pattern of pseudoexfoliation deposits on the lens and their clinical correlation- clinical study and review of literature. PLoS ONE 2014, 9, e113329. [Google Scholar] [CrossRef] [PubMed]
- Jammal, H.; Abu Ameera, M.; Al Qudah, N.; Aldalaykeh, M.; Abukahel, A.; Al Amer, A.; Al Bdour, M. Characteristics of Patients with Pseudoexfoliation Syndrome at a Tertiary Eye Care Center in Jordan: A Retrospective Chart Review. Ophthalmol. Ther. 2021, 10, 51–61. [Google Scholar] [CrossRef]
- Tekin, K.; Inanc, M.; Elgin, U. Monitoring and management of the patient with pseudoexfoliation syndrome: Current perspectives. Clin. Ophthalmol. 2019, 13, 453–464. [Google Scholar] [CrossRef] [Green Version]
- Slettedal, J.K.; Sandvik, L.; Ringvold, A. Ocular pseudoexfoliation syndrome and life span. EBioMedicine 2015, 2, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Plateroti, P.; Plateroti, A.M.; Abdolrahimzadeh, S.; Scuderi, G. Pseudoexfoliation Syndrome and Pseudoexfoliation Glaucoma: A Review of the Literature with Updates on Surgical Management. J. Ophthalmol. 2015, 2015, 370371. [Google Scholar] [CrossRef] [Green Version]
- Çınar, E.; Yüce, B.; Aslan, F. Retinal and choroidal vascular changes in eyes with pseudoexfoliation syndrome: A comparative study using optical coherence tomography angiography. Balk. Med. J. 2020, 37, 9–14. [Google Scholar] [CrossRef]
- Koretz, J.F.; Cook, C.A.; Kaufman, P.L. Aging of the human lens: Changes in lens shape upon accommodation and with accommodative loss. J. Opt. Soc. Am. A 2002, 19, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Teshigawara, T.; Meguro, A.; Sanjo, S.; Hata, S.; Mizuki, N. The advantages of femtosecond laser-assisted cataract surgery for zonulopathy. Int. Med. Case Rep. J. 2019, 12, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchison, D.A.; Thibos, L.N. Optical models of the human eye. Clin. Exp. Optom. 2016, 99, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro, R.; Palos, F.; González, L.M. Adaptive model of the gradient index of the human lens. II. Optics of the accommodating aging lens. J. Opt. Soc. Am. A 2007, 24, 2911. [Google Scholar] [CrossRef] [Green Version]
- Castanos, M.V.; Najac, T.; Dauhajre, J.; Buxton, D.F. Late intraocular Lens dislocation following scleral depression: A case report. BMC Ophthalmol. 2020, 20, 39. [Google Scholar] [CrossRef] [Green Version]
- Naumann, G.O.H.; Schlötzer-Schrehardt, U.; Küchle, M. Pseudoexfoliation syndrome for the comprehensive ophthalmologist: Intraocular and systemic manifestations. Ophthalmology 1998, 105, 951–968. [Google Scholar] [CrossRef]
- Schlötzer-Schrehardt, U.; Naumann, G.O.H. Ocular and Systemic Pseudoexfoliation Syndrome. Am. J. Ophthalmol. 2006, 141, 921–937. [Google Scholar] [CrossRef]
- Fontana, L.; Coassin, M.; Iovieno, A.; Moramarco, A.; Cimino, L. Cataract surgery in patients with pseudoexfoliation syndrome: Current updates. Clin. Ophthalmol. 2017, 11, 1377–1383. [Google Scholar] [CrossRef] [Green Version]
- Schlötzer-Schrehardt, U.; Naumann, G.O.H. A Histopathologic Study of Zonular Instability in Pseudoexfoliation Syndrome. Am. J. Ophthalmol. 1994, 118, 730–743. [Google Scholar] [CrossRef]
- Yaguchi, S.; Yaguchi, S.; Yagi-Yaguchi, Y.; Kozawa, T.; Bissen-Miyajima, H. Objective classification of zonular weakness based on lens movement at the start of capsulorhexis. PLoS ONE 2017, 12, e0176169. [Google Scholar] [CrossRef] [Green Version]
- Hoffman, R.S.; Snyder, M.E.; Devgan, U.; Allen, Q.B.; Yeoh, R.; Braga-Mele, R. Management of the subluxated crystalline lens. J. Cataract Refract. Surg. 2013, 39, 1904–1915. [Google Scholar] [CrossRef] [PubMed]
- Pierscionek, B.; Bahrami, M.; Hoshino, M.; Uesugi, K.; Regini, J.; Yagi, N. The eye lens: Age-related trends and individual variations in refractive index and shape parameters. Oncotarget 2015, 6, 30532–30544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, M.T.; Feijóo, B.; Castro, A.P.G.; Ribeiro, F.J.; Fernandes, P.R. Axisymmetric finite element modelling of the human lens complex under cataract surgery. Symmetry 2021, 13, 696. [Google Scholar] [CrossRef]
- Wang, K.; Venetsanos, D.T.; Wang, J.; Augousti, A.T.; Pierscionek, B.K. The importance of parameter choice in modelling dynamics of the eye lens article. Sci. Rep. 2017, 7, 16688. [Google Scholar]
- Rossi, T.; Ceccacci, A.; Testa, G.; Ruggiero, A.; Bonora, N.; D’Agostino, I.; Telani, S.; Ripandelli, G. Influence of anterior capsulorhexis shape, centration, size, and location on intraocular lens position: Finite element model. J. Cataract Refract. Surg. 2022, 48, 222–229. [Google Scholar] [CrossRef]
- Wang, K.; Venetsanos, D.T.; Hoshino, M.; Uesugi, K.; Yagi, N.; Pierscionek, B.K. A Modeling Approach for Investigating Opto-Mechanical Relationships in the Human Eye Lens. IEEE Trans. Biomed. Eng. 2020, 67, 999–1006. [Google Scholar] [CrossRef]
- Van Alphen, G.W.H.M.; Graebel, W.P.P. Elasticity of tissues involved in accommodation. Vis. Res. 1991, 31, 1417–1438. [Google Scholar] [CrossRef] [Green Version]
- Weeber, H.A.; Van der Heijde, R.G.L.L. Internal deformation of the human crystalline lens during accommodation. Acta Ophthalmol. 2008, 86, 642–647. [Google Scholar] [CrossRef]
- Gasser, T.C.; Ogden, R.W.; Holzapfel, G.A. Hyperelastic modelling of arterial layers with distributed collagen fibre orientations. J. R. Soc. Interface 2006, 3, 15–35. [Google Scholar] [CrossRef]
- Castro, A.P.G.; Alves, J.L. Numerical implementation of an osmo-poro-visco-hyperelastic finite element solver: Application to the intervertebral disc. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 538–550. [Google Scholar] [CrossRef]
- Godinho, M.I.; Carvalho, V.; Matos, M.T.; Fernandes, P.R.; Castro, A.P.G. Computational modeling of lumbar disc degeneration before and after spinal fusion. Clin. Biomech. 2021, 90, 105490. [Google Scholar] [CrossRef] [PubMed]
- Biermann, J.; Bredow, L.; Boehringer, D.; Reinhard, T. Evaluation of ciliary sulcus diameter using ultrasound biomicroscopy in emmetropic eyes and myopic eyes. J. Cataract Refract. Surg. 2011, 37, 1686–1693. [Google Scholar] [CrossRef] [PubMed]
- Hermans, E.A.; Dubbelman, M.; Van der Heijde, G.L.; Heethaar, R.M. Estimating the external force acting on the human eye lens during accommodation by finite element modelling. Vis. Res. 2006, 46, 3642–3650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, A.M.; Denham, D.B.; Fernandez, V.; Borja, D.; Ho, A.; Manns, F.; Parel, J.-M.; Augusteyn, R.C. In vitro dimensions and curvatures of human lenses. Vis. Res. 2006, 46, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Bocskai, Z.; Bojtár, I. Biomechanical modelling of the accommodation problem of human eye. Period. Polytech. Civ. Eng. 2013, 57, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Cabeza-Gil, I.; Grasa, J.; Calvo, B. A validated finite element model to reproduce Helmholtz’s theory of accommodation: A powerful tool to investigate presbyopia. Ophthalmic Physiol. Opt. 2021, 41, 1241–1253. [Google Scholar] [CrossRef]
- Satou, T.; Shimizu, K.; Tsunehiro, S.; Igarashi, A.; Kato, S.; Koshimizu, M.; Niida, T. Development of a new intraocular lens power calculation method based on lens position estimated with optical coherence tomography. Sci. Rep. 2020, 10, 6501. [Google Scholar] [CrossRef] [Green Version]
- Duane, A. Studies in Monocular and Binocular Accommodation, with Their Clinical Application. Trans. Am. Ophthalmol. Soc. 1922, 20, 132–157. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
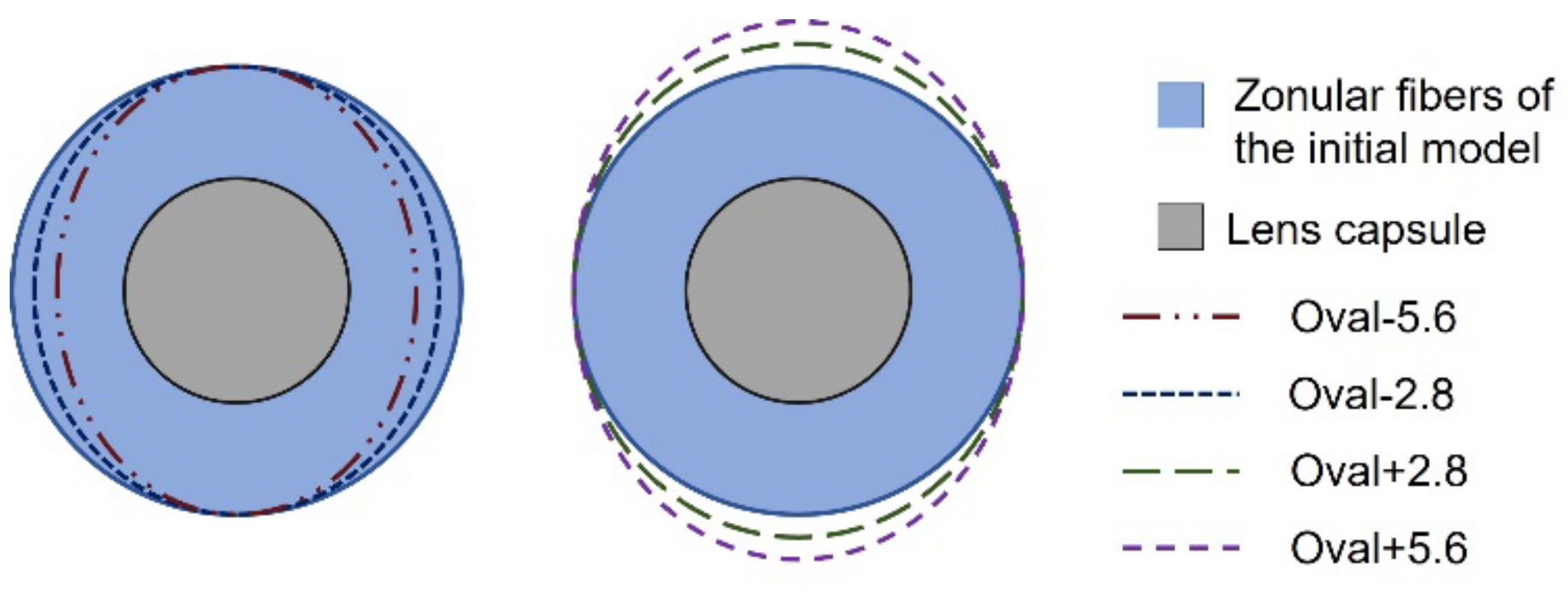
| Model | Vertical Length [mm] | Horizontal Length [mm] |
|---|---|---|
| Oval-5.6 | 1500 | 1416 |
| Oval-2.8 | 1500 | 1458 |
| Initial Model | 1500 | 1500 |
| Oval + 2.8 | 1542 | 1500 |
| Oval + 5.6 | 1584 | 1500 |
| Model | Anterior Band Width [mm] | Equatorial Band Width [mm] | Posterior Band Width [mm] |
|---|---|---|---|
| Band1 | 0.167 | 0.167 | 0.133 |
| Band2 | 0.333 | 0.333 | 0.267 |
| Band3 | 0.500 | 0.500 | 0.400 |
| Band4 | 0.590 | 0.590 | 0.548 |
| Band5 | 0.680 | 0.680 | 0.695 |
| Band6 | 0.770 | 0.770 | 0.843 |
| Band7 | 0.860 | 0.860 | 0.990 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jud, L.; Castro, A.P.G.; Ruben, R.B.; Feijóo, B.; Ribeiro, F.J.; Fernandes, P.R. 3D Modeling of the Crystalline Lens Complex under Pseudoexfoliation. Bioengineering 2022, 9, 212. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050212
Jud L, Castro APG, Ruben RB, Feijóo B, Ribeiro FJ, Fernandes PR. 3D Modeling of the Crystalline Lens Complex under Pseudoexfoliation. Bioengineering. 2022; 9(5):212. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050212
Chicago/Turabian StyleJud, Leonor, André P. G. Castro, Rui B. Ruben, Bernardo Feijóo, Filomena J. Ribeiro, and Paulo R. Fernandes. 2022. "3D Modeling of the Crystalline Lens Complex under Pseudoexfoliation" Bioengineering 9, no. 5: 212. https://0-doi-org.brum.beds.ac.uk/10.3390/bioengineering9050212