
Beverages Containing Plant-Derived Polyphenols Inhibit Growth and Biofilm Formation of Streptococcus mutans and Children’s Supragingival Plaque Bacteria

Abstract
:1. Introduction
2. Materials and Methods
2.1. Children’s Supragingival Plaque Samples
2.2. Ready-to-Drink (RTD) Beverages Used for S. mutans Testing
- AriZona® Diet Green Tea with Ginseng (AriZona Beverage Co., Cincinnati, OH, USA).
- AriZona® Green Tea with Ginseng and Honey (AriZona Beverage Co., Cincinnati, OH, USA).
- Gold Peak® Green Tea (The Coca Cola Co., Atlanta, GA, USA).
- Gold Peak® Diet Iced Tea (The Coca Cola Co., Atlanta, GA, USA).
- Lipton® 100% Natural Green Tea with Citrus (Unilever, Englewood Cliffs, NJ, USA).
- Lipton® 100% Natural Iced Tea with Lemon (Unilever, Englewood Cliffs, NJ, USA).
- Lipton® 100% Natural Iced Tea with Pomegranate Blueberry (Unilever, Englewood Cliffs, NJ, USA).
- Lipton® Diet Green Tea with Citrus (Unilever, Englewood Cliffs, NJ, USA).
- PureLeaf™ Iced Tea Unsweetened (Unilever, Englewood Cliffs, NJ, USA).
- PureLeaf™ Iced Tea Sweetened (Unilever, Englewood Cliffs, NJ, USA).
- PureLeaf™ Iced Tea Raspberry (Unilever, Englewood Cliffs, NJ, USA).
- Snapple® All Natural Raspberry Iced Tea (Snapple Beverage Corp., Rye Brook, NY, USA).
- Diet Snapple® Cranberry Raspberry (Snapple Beverage Corp., Rye Brook, NY, USA).
- Diet Snapple® Half Lemonade ‘n Half Iced Tea (Snapple Beverage Corp., Rye Brook, NY, USA).
- Diet Snapple® Raspberry Iced Tea (Snapple Beverage Corp., Rye Brook, NY, USA).
- Diet Snapple® Raspberry Tea (Snapple Beverage Corp., Rye Brook, NY, USA).
- SoBe™ Honey Green Tea-Lean (PepsiCo., Purchase, NY, USA).
- Ocean Spray® Diet Cranberry (Ocean Spray Cranberries Inc., Lakeville, MA, USA).
- Ocean Spray® Cranberry Juice Cocktail (Ocean Spray Cranberries Inc., Lakeville, MA, USA).
- Simply™ Cranberry Cocktail (Simply Orange Juice Co., Apopka, FL, USA).
2.3. Beverages Used for Children’s Supragingival Plaque Testing
- Prepackaged tea bags.
- -
- Lipton® Green Tea (GT; Unilever, Englewood Cliffs, NJ, USA).
- -
- Bigelow® Black Tea English Teatime (BT-ET; Bigelow Tea, Fairfield, CT, USA).
- -
- Bigelow® Black Tea Cinnamon Stick (BT-CS; Bigelow Tea, Fairfield, CT, USA).
- -
- Bigelow® Black Tea Raspberry Royale (BT-RR; Bigelow Tea, Fairfield, CT, USA).
- Ready-to-drink (RTD) bottled beverages.
- -
- PureLeaf™ Iced Tea Unsweetened (UT; black tea, Unilever, Fairfield, CT, USA).
- -
- Snapple® All Natural Green Tea (ANGT, Snapple Beverage Corp., Rye Brook, NY, USA).
- -
- Snapple® All Natural Raspberry iced Tea (ANRT; Black and Green Tea, Snapple Beverage Corp., Rye Brook, NY, USA).
- Cranberry juice cocktails.
- -
- Ocean Spray® Cranberry Juice Cocktail (CJ-OS, Ocean Spray Cranberries Inc., Lakeville, MA, USA).
- -
- Simply™ Cranberry Cocktail (CJ-S; Simply Orange Juice Co., Apopka, FL, USA).
2.4. Preparation of Test Teas/Beverages
2.5. Effects of Selected Teas and RTD Bottled Beverages on In Vitro Growth of Children’s Supragingival Plaque Bacteria
2.6. Effects of Selected Teas and RTD Bottled Beverages on In Vitro Biofilm Formation of Children’s Supragingival Plaque Bacteria
2.7. Effects of Selected RTD Bottled Beverages on In Vitro Growth and Biofilm Formation of S. mutans
2.8. Total Polyphenol Content of Test RTD Bottled Beverages and Teas
2.9. Statistical Analysis
3. Results
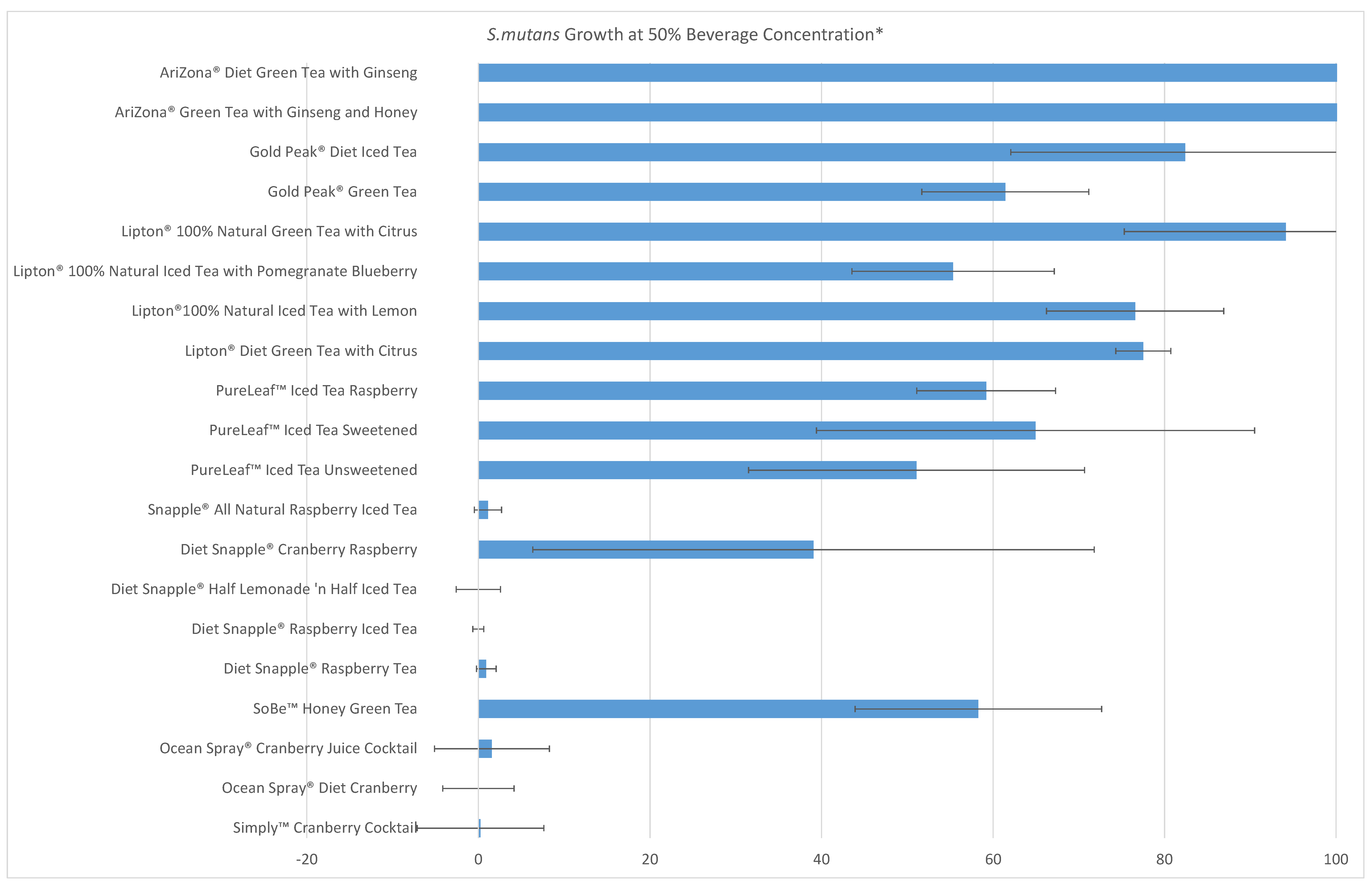
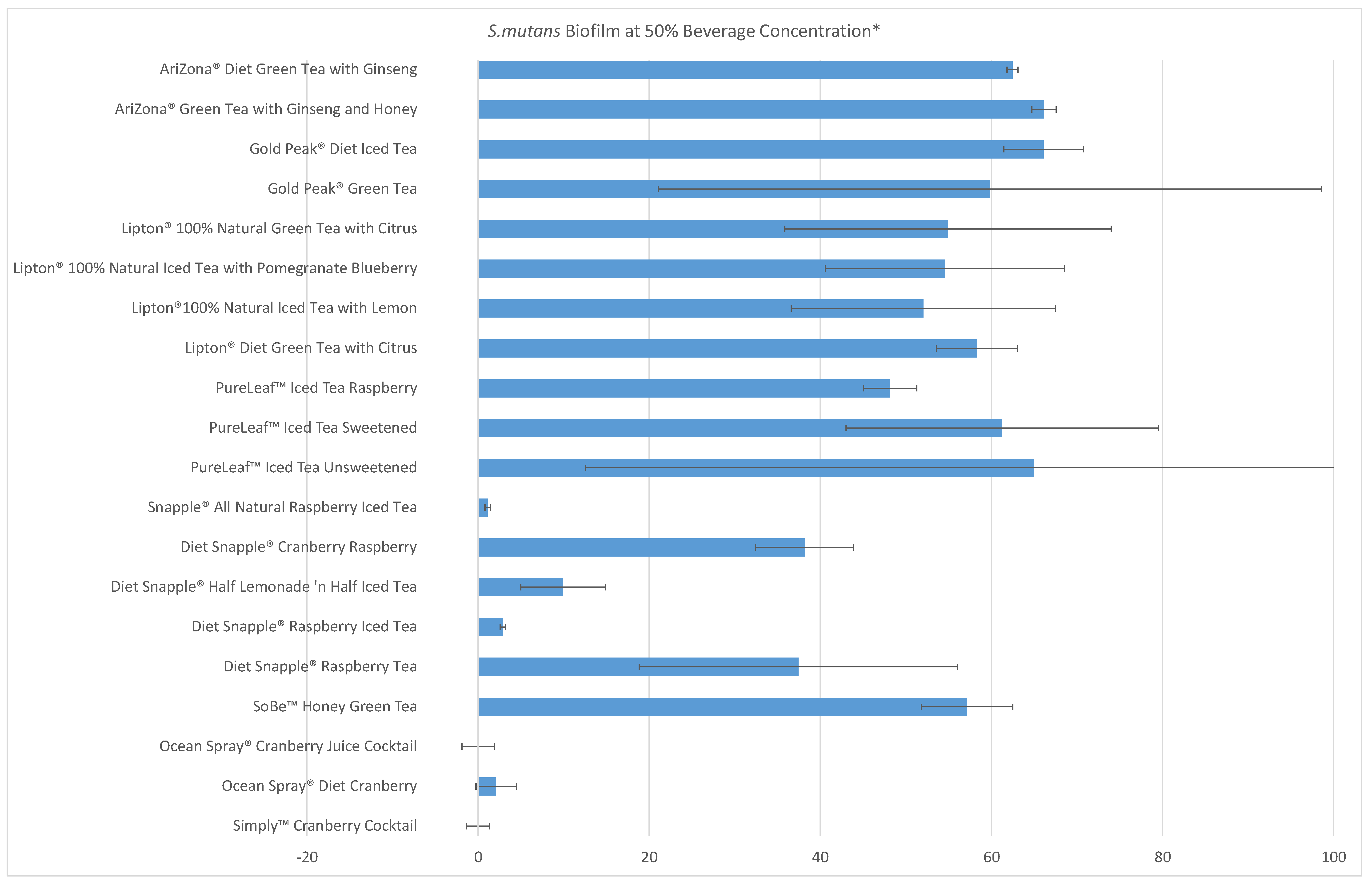
3.1. Effects of RTD Bottled Beverages on S. mutans Growth and Biofilm Formation
3.2. Effects of Teas on Growth and Biofilm Formation of Children’s Plaque Bacteria
3.3. Effects of Ready-to-Drink (RTD) Bottled Teas and Beverages on Growth and Biofilm Formation of Children’s Plaque Bacteria
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef] [PubMed]
- Bowen, W.H. Do we need to be concerned about dental caries in the coming millennium? Crit. Rev. Oral Biol. Med. 2002, 13, 126–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skinner, J.; Byun, R.; Blinkhorn, A.; Johnson, G. Sugary drink consumption and dental caries in New South Wales teenagers. Aust. Dent. J. 2015, 60, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Tahmassebi, J.F.; Duggal, M.S.; Malik-Kotru, G.; Curzon, M.E.J. Soft drinks and dental health: A review of the current literature. J. Dent. 2006, 34, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.; Suneja, B.; Walsh, L.J. Ecological approaches to dental caries prevention: Paradigm shift or shibboleth? Caries Res. 2018, 52, 153–165. [Google Scholar] [CrossRef]
- Heyman, M.B.; Abrams, S.A. Fruit juice in infants, children, and adolescents: Current recommendations. Pediatrics 2017, 139, e20170967. [Google Scholar] [CrossRef] [Green Version]
- Signoretto, C.; Canepari, P.; Stauder, M.; Vezzulli, L.; Pruzzo, C. Functional foods and strategies contrasting bacterial adhesion. Curr. Opin. Biotechnol. 2012, 23, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.D. The impact of food components and dietary factors on oral health. J. Food Drug Anal. 2012, 20, 270–274. [Google Scholar] [CrossRef]
- Basu, A.; Masek, E.; Ebersole, J.L. Dietary polyphenols and periodontitis—A mini-review of literature. Molecules 2018, 23, 1786. [Google Scholar] [CrossRef] [Green Version]
- Giacaman, R.A. Sugars and beyond. The role of sugars and the other nutrients and their potential impact on caries. Oral Dis. 2018, 24, 1185–1197. [Google Scholar] [CrossRef]
- Philip, N.; Bandara, H.; Leishman, S.J.; Walsh, L.J. Inhibitory effects of fruit berry extracts on Streptococcus mutans biofilms. Eur. J. Oral Sci. 2019, 127, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Fidler Mis, N.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellof, M.; Embleton, N.D.; Hojsak, I.; Hulst, J.; Indrio, F.; Lapillonne, A.; et al. Sugar in infants, children and adolescents: A position paper of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 65, 681–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paglia, L.; Scaglioni, S.; Torchia, V.; De Cosmi, V.; Moretti, M.; Marzo, G.; Giuca, M.R. Familial and dietary risk factors in Early Childhood Caries. Eur. J. Paediatr. Dent. 2016, 17, 93–99. [Google Scholar] [PubMed]
- Perez-Morales, E.; Bacardi-Gascon, M.; Jimenez-Cruz, A. Sugar-sweetened beverage intake before 6 years of age and weight or BMI status among older children; systematic review of prospective studies. Nutr. Hosp. 2013, 28, 47–51. [Google Scholar] [PubMed]
- Chi, D.L.; Scott, J.M. Added sugar and dental caries in children: A scientific update and future steps. Dent. Clin. N. Am. 2019, 63, 17–33. [Google Scholar] [CrossRef]
- Sánchez-Pimienta, T.G.; Rivera, J.A.; Batis, C.; Lutter, C.K. Sugar-sweetened beverages are the main sources of added sugar intake in the Mexican population. J. Nutr. 2016, 146, 1888S–1896S. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatric Dentistry. Policy on Dietary Recommendations for Infants, Children, and Adolescents. Pediatr. Dent. 2017, 40, 3. [Google Scholar]
- Gupta, A.; Dwivedi, M.; Mahdi, A.A.; Nagana Gowda, G.A.; Khetrapal, C.L.; Bhandari, M. Inhibition of adherence of multi-drug resistant E. coli by proanthocyanidin. Urol. Res. 2012, 40, 143–150. [Google Scholar] [CrossRef]
- Pandey, K.B.; Rizvi, S.I. Plant polyphenols as dietary antioxidants in human health and disease. Oxidative Med. Cell. Longev. 2009, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Hamilton-Miller, J.M.T. Anti-cariogenic properties of tea (Camellia sinensis). J. Med. Microbiol. 2001, 50, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.W.; Hamilton-Miller, J.M.; Stapleton, P.D. Antimicrobial properties of green tea catechins. Food Sci. Technol. Bull. 2005, 2, 71–81. [Google Scholar] [CrossRef] [Green Version]
- Ferrazzano, G.F.; Amato, I.; Ingenito, A.; De Natale, A.; Pollio, A. Anti-cariogenic effects of polyphenols from plant stimulant beverages (cocoa, coffee, tea). Fitoterapia 2009, 80, 255–262. [Google Scholar] [CrossRef]
- Wu, C.D.; Wei, G. 19—Tea as a functional food for oral health. In Food Constituents and Oral Health; Wilson, M., Ed.; Woodhead Publishing: Cambridge, UK, 2009; pp. 396–417. [Google Scholar]
- Koo, H.; Duarte, S.; Murata, R.M.; Scott-Anne, K.; Gregoire, S.; Watson, G.E.; Singh, A.P.; Vorsa, N. Influence of cranberry proanthocyanidins on formation of biofilms by Streptococcus mutans on saliva-coated apatitic surface and on dental caries development in vivo. Caries Res. 2010, 44, 116–126. [Google Scholar] [CrossRef] [Green Version]
- Rivero-Cruz, J.F.; Zhu, M.; Kinghorn, A.D.; Wu, C.D. Antimicrobial constituents of Thompson seedless raisins (Vitis vinifera) against selected oral pathogens. Phytochem. Lett. 2008, 1, 151–154. [Google Scholar] [CrossRef]
- Woźniewicz, M.; Nowaczyk, P.M.; Kurhańska-Flisykowska, A.; Wyganowska-Świątkowska, M.; Lasik-Kurdyś, M.; Walkowiak, J.; Bajerska, J. Consumption of cranberry functional beverage reduces gingival index and plaque index in patients with gingivitis. Nutr. Res. 2018, 58, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Utreja, A.; Lingström, P.; Evans, C.A.; Salzmann, L.B.; Wu, C.D. The effect of raisin-containing cereals on the pH of dental plaque in young children. Pediatr. Dent. 2009, 31, 498–503. [Google Scholar]
- Gaur, S.; Agnihotri, R. Green tea: A novel functional food for the oral health of older adults. Geriatr. Gerontol. Int. 2014, 14, 238–250. [Google Scholar] [CrossRef]
- Li, Y.; Jiang, X.; Hao, J.; Zhang, Y.; Huang, R. Tea polyphenols: Application in the control of oral microorganism infectious diseases. Arch. Oral Biol. 2019, 102, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhou, X.D.; Wu, C.D. Tea catechin epigallocatechin gallate inhibits Streptococcus mutans biofilm formation by suppressing GTF genes. Arch. Oral Biol. 2012, 57, 678–683. [Google Scholar] [CrossRef]
- Blumberg, J.B.; Camesano, T.A.; Cassidy, A.; Kris-Etherton, P.; Howell, A.; Manach, C.; Ostertag, L.M.; Sies, H.; Skulas-Ray, A.; Vita, J.A. Cranberries and their bioactive constituents in human health. Adv. Nutr. 2013, 4, 618–632. [Google Scholar] [CrossRef] [Green Version]
- Feghali, K.; Feldman, M.; La, V.D.; Santos, J.; Grenier, D. Cranberry proanthocyanidins: Natural weapons against periodontal diseases. J. Agric. Food Chem. 2012, 60, 5728–5735. [Google Scholar] [CrossRef]
- Kim, D.; Hwang, G.; Liu, Y.; Wang, Y.; Singh, A.P.; Vorsa, N.; Koo, H. Cranberry flavonoids modulate cariogenic properties of mixed-species biofilm through exopolysaccharides-matrix disruption. PLoS ONE 2015, 10, e0145844. [Google Scholar] [CrossRef]
- Philip, N.; Walsh, L.J. Cranberry polyphenols: Natural weapons against dental caries. Dent. J. 2019, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Ben Lagha, A.; Dudonné, S.; Desjardins, Y.; Grenier, D. Wild blueberry (Vaccinium angustifolium Ait.) polyphenols target Fusobacterium nucleatum and the host inflammatory response: Potential innovative molecules for treating periodontal diseases. J. Agric. Food Chem. 2015, 63, 6999–7008. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.D.; Zhu, M.; Turner, A.; Pauli, G.F.; Farnsworth, N.R. Cranberry extracts inhibit growth/viability of oral pathogens and biofilms. Presented at the Meeting of the International Association for Dental Research, Honolulu, HI, USA, 13 March 2004. [Google Scholar]
- Cai, L.; Wu, C.D. Compounds from Syzygium aromaticum possessing growth inhibitory activity against oral pathogens. J. Nat. Prod. 1996, 59, 987–990. [Google Scholar] [CrossRef] [PubMed]
- Riihinen, K.R.; Ou, Z.M.; Gödecke, T.; Lankin, D.C.; Pauli, G.F.; Wu, C.D. The antibiofilm activity of lingonberry flavonoids against oral pathogens is a case connected to residual complexity. Fitoterapia 2014, 97, 78–86. [Google Scholar] [CrossRef]
- Bradshaw, D.J.; Lynch, R.J. Diet and the microbial aetiology of dental caries: New paradigms. Int. Dent. J. 2013, 63, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Herod, E.L. The effect of cheese on dental caries: A review of the literature. Aust. Dent. J. 1991, 36, 120–125. [Google Scholar] [CrossRef]
- Rugg-Gunn, A.J.; Edgar, W.M.; Jenkins, G.N. The effect of altering the position of a sugary food in a meal upon plaque pH in human subjects. J. Dent. Res. 1981, 60, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.D. Grape products and oral health. J. Nutr. 2009, 139, 1818S–1823S. [Google Scholar] [CrossRef] [Green Version]
- Naval, S.; Koerber, A.; Salzmann, L.; Punwani, I.; Johnson, B.R.; Wu, C.D. The effects of beverages on plaque acidogenicity after a sugary challenge. J. Am. Dent. Assoc. 2013, 144, 815–822. [Google Scholar] [CrossRef]
- Wu, C.D.; Bo, H.; Jin, S.; Li, W.; Utreja, A. Consuming milk after sugary challenge reduces children dental plaque acidogenicity. Presented at the Meeting of the International Association for Dental Research, London, UK, 4 April 2018. [Google Scholar]
- Cleverdon, R.; Elhalaby, Y.; McAlpine, M.D.; Gittings, W.; Ward, W.E. Total polyphenol content and antioxidant capacity of tea bags: Comparison of black, green, red rooibos, chamomile and peppermint over different steep times. Beverages 2018, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- McAlpine, M.D.; Ward, W.E. Influence of steep time on polyphenol content and antioxidant capacity of black, green, rooibos, and herbal teas. Beverages 2016, 2, 17. [Google Scholar] [CrossRef]
- Xu, X.; Ou, Z.M.; Wu, C.D. Growth media affect assessment of antimicrobial activity of plant-derived polyphenols. BioMed Res. Int. 2018, 2018, 8308640. [Google Scholar] [CrossRef] [PubMed]
- Pelczar, M.J.; Chan, E.C.S.; Krieg, N.R. Control of microorganisms, the control of microorganisms by physical agents. In Microbiology; Chan, E.C.S., Krieg, N.R., Eds.; Mc Graw-Hill International: New York, NY, USA, 1988; pp. 469–509. [Google Scholar]
- Gupta, A.; Bansal, K.; Marwaha, M. Effect of high-molecular-weight component of Cranberry on plaque and salivary Streptococcus mutans counts in children: An in vivo study. J. Indian Soc. Pedod. Prev. Dent. 2015, 33, 128–133. [Google Scholar] [PubMed]
- Zhu, M.; Carvalho, R.; Scher, A.; Wu, C.D. Short-term germ-killing effect of sugar-sweetened cinnamon chewing gum on salivary anaerobes associated with halitosis. J. Clin. Dent. 2011, 22, 23–26. [Google Scholar]
- Johnson-White, B.; Buquo, L.; Zeinali, M.; Ligler, F.S. Prevention of nonspecific bacterial cell adhesion in immunoassays by use of cranberry juice. Anal. Chem. 2006, 78, 853–857. [Google Scholar] [CrossRef]
- Duarte, S.; Gregoire, S.; Singh, A.P.; Vorsa, N.; Schaich, K.; Bowen, W.H.; Koo, H. Inhibitory effects of cranberry polyphenols on formation and acidogenicity of Streptococcus mutans biofilms. FEMS Microbiol. Lett. 2006, 257, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Luu, M.; Li, W.; Kratunova, E.; Xie, Q.; Wu, C.D. Cranberry juice consumption inhibits children’s supragingival plaque regrowth and acid production. Presented at the American Academy of Pediatric Dentistry (AAPD) Annual Session, Nashvirtual, TN, USA, 21–24 May 2020. [Google Scholar]
- Wu, C.D.; Li, W.; Huang, E.; Jing, S.; Kratunova, E.; Carubio, L. Does cranberry benefit human oral health? Presented at the Meeting of the American Society for Nutrition Annual Meeting, Boston, MA, USA, 9–12 June 2018. [Google Scholar]
- Dutreix, L.; Bernard, C.; Juin, C.; Imbert, C.; Girardot, M. Do raspberry extracts and fractions have antifungal or anti-adherent potential against Candida spp.? Int. J. Antimicrob. Agents 2018, 52, 947–953. [Google Scholar] [CrossRef]
- Velićanski, A.S.; Cvetković, D.D.; Markov, S.L.; Šaponjac, V.T.; Vulić, J.J. Antioxidant and antibacterial activity of the beverage obtained by fermentation of sweetened lemon balm (Melissa officinalis L.) tea with symbiotic consortium of bacteria and yeasts. Food Technol. Biotechnol. 2014, 52, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Reddy, A.; Norris, D.F.; Momeni, S.S.; Waldo, B.; Ruby, J.D. The pH of beverages in the United States. J. Am. Dent. Assoc. 2016, 147, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, T.A. Dietary assessment and counseling for dental erosion. J. Am. Dent. Assoc. 2018, 149, 148–152. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Test Teas | Growth (MIC, mg/mL) * | Biofilm (MBIC, mg/mL) * |
|---|---|---|
| Median (Range) | Median (Range) | |
| Green Tea (GT) | 0.78 (0.39–3.13) | 1.56 (0.39–25) |
| Black Tea-English Teatime (BT-ET) | 3.13 (0.39–6.25) | 0.78 (0.39–6.25) |
| Black Tea-Cinnamon Stick (BT-CS) | 2.35 (0.39–6.25) | 1.56 (0.78–3.13) |
| Black Tea-Raspberry Royale (BT-RR) | 6.25 (0.78–25) | 1.56 (0.39–25) |
| Test Beverages | Growth (MIC *, % Beverage) | Biofilm (MBIC *, % Beverage) |
|---|---|---|
| Median (Range) | Median (Range) | |
| All Natural Raspberry Iced Tea (ANRT) | >50 | 9.38 (1.56–25) |
| All Natural Green Tea (ANGT) | >50 (50–>50) | >50 |
| Unsweetened Tea (UT) | >50 | 4.68 (1.56–12.5) |
| Cranberry Juice Cocktail (CJ-OS) | 50 (3.13–50) | >50 (1.56–>50) |
| Cranberry Cocktail (CJ-S) | 50 (3.13–50) | 50 (1.56–>50) |
| Beverages | Growth | Biofilm Formation | ||
|---|---|---|---|---|
| % Control * | % Inhibition † | % Control * | % Inhibition † | |
| All Natural Raspberry Iced Tea (ANRT) | 29.79 ± 20.23 | 70.21 | 1.16 ± 2.49 | 98.84 |
| All Natural Green Tea (ANGT) | 37.61 ± 34.32 | 62.39 | 118.94 ± 50.58 | NI ‡ |
| Unsweetened Tea (UT) | 47.63 ± 37.30 | 52.37 | 2.16 ± 1.49 | 97.84 |
| Cranberry Juice Cocktail (CJ-OS) | 4.41 ± 6.99 | 95.59 | 42.52 ± 51.99 | 57.48 |
| Cranberry Cocktail (CJ-S) | 5.42 ± 14.77 | 94.58 | 28.24 ± 63.65 | 71.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.D.; Huang, E.; Li, W.; White, M.; Jung, S.; Xie, Q. Beverages Containing Plant-Derived Polyphenols Inhibit Growth and Biofilm Formation of Streptococcus mutans and Children’s Supragingival Plaque Bacteria. Beverages 2021, 7, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/beverages7030043
Wu CD, Huang E, Li W, White M, Jung S, Xie Q. Beverages Containing Plant-Derived Polyphenols Inhibit Growth and Biofilm Formation of Streptococcus mutans and Children’s Supragingival Plaque Bacteria. Beverages. 2021; 7(3):43. https://0-doi-org.brum.beds.ac.uk/10.3390/beverages7030043
Chicago/Turabian StyleWu, Christine D., Ellen Huang, Wei Li, Mark White, Shawn Jung, and Qian Xie. 2021. "Beverages Containing Plant-Derived Polyphenols Inhibit Growth and Biofilm Formation of Streptococcus mutans and Children’s Supragingival Plaque Bacteria" Beverages 7, no. 3: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/beverages7030043