Emidec: A Database Usable for the Automatic Evaluation of Myocardial Infarction from Delayed-Enhancement Cardiac MRI


 , , , ,
, , , , 
Abstract
:1. Summary
2. Data Description
- -
- MR images composed of a series of DE-MRI in short axis orientation that cover the left ventricle of the heart, with the corresponding ground truths;
- -
- A text file with the clinical information.
2.1. MRI Exams
2.2. Clinical Information
3. Methods
3.1. Ethics Approval
3.2. DE-MRI Acquisition
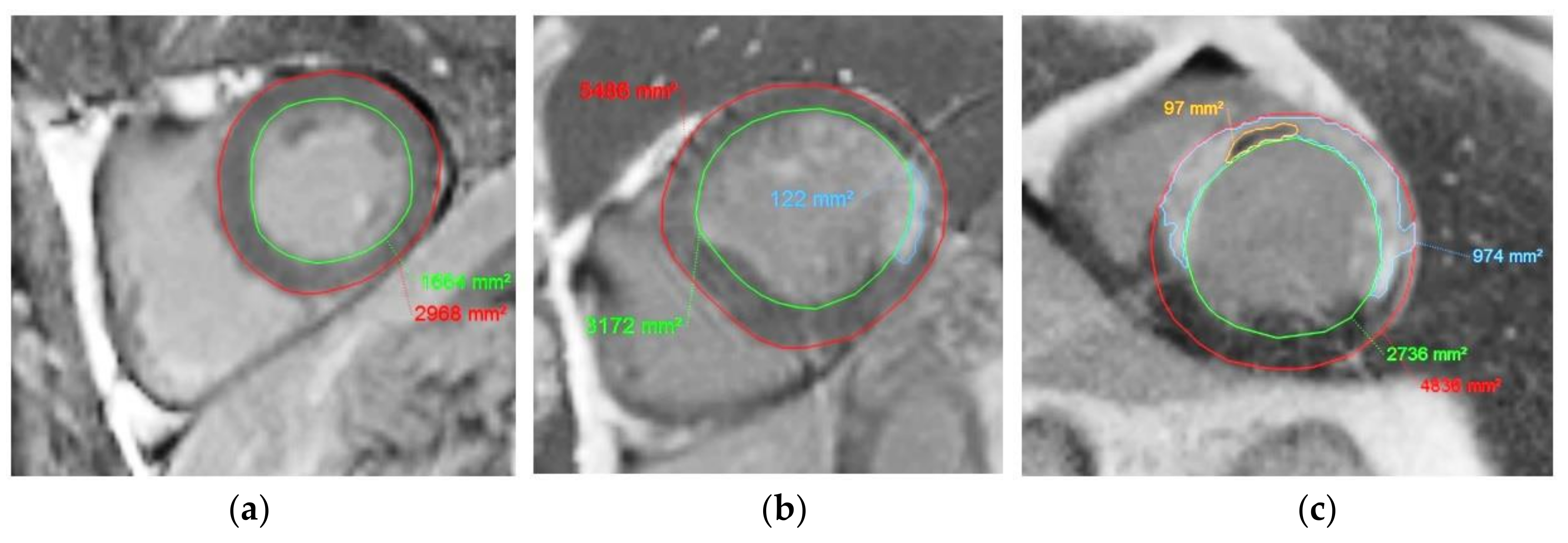
3.3. Annotation of the MR Images
3.4. Recording of the Clinical Information
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hamirani, Y.S.; Wong, A.; Kramer, C.M.; Salerno, M. Effect of microvascular obstruction and intramyocardial hemorrhage by CMR on LV remodeling and outcomes after myocardial infarction: A systematic review and meta-analysis. JACC Cardiovasc. Imag. 2014, 7, 940–952. [Google Scholar]
- Zia, M.I.; Ghugre, N.R.; Connelly, K.A.; Strauss, B.H.; Sparkes, J.D.; Dick, A.J.; Wright, G.A. Characterizing myocardial edema and hemorrhage using quantitative T2 and T2 * mapping at multiple time intervals post ST-segment elevation myocardial infarction. Circ. Cardiovasc. Imag. 2012, 5, 566–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zia, M.I.; Ramanan, V.; Roifman, I.; Connelly, K.A.; Wright, G.A.; Ghugre, N.R. Chronic persistence of hemorrhage, microvascular obstruction, and edema after myocardial infarction: Utility of cardiac magnetic resonance imaging. Can. J. Cardiol. 2020, 36, 1326.e17–1326.e19. [Google Scholar] [CrossRef] [PubMed]
- Hsu, L.Y.; Natanzon, A.; Kellman, P.; Hirsch, G.A.; Aletras, A.H.; Arai, A.E. Quantitative myocardial infarction on delayed enhancement MRI. Part I: Animal validation of an automated feature analysis and combined thresholding infarct sizing algorithm. J. Magn. Reason. Imag. 2006, 23, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.J.; Fieno, D.S.; Parrish, T.B.; Harris, K.; Chen, E.L.; Simonetti, O.; Bundy, J.; Finn, J.P.; Klocke, F.J.; Judd, R.M. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation 1999, 100, 1992–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, K.C.; Zerhouni, E.A.; Judd, R.M.; Lugo-Olivieri, C.H.; Barouch, L.A.; Schulman, S.P.; Lima, J.A. Prognostic significance of microvascular obstruction by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 1998, 97, 765–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MICCAI Registered Challenges in 2020. Available online: http://www.miccai.org/events/challenges/ (accessed on 24 September 2020).
- Emidec Challenge Registered on Zenodo Website. Available online: https://zenodo.org/record/3755234#.X2xNi9Q6_DB (accessed on 24 September 2020).
- Karim, R.; Bhagirath, P.; Claus, P.; James Housden, R.; Chen, Z.; Karimaghaloo, Z.; Sohn, H.M.; Lara Rodríguez, L.; Vera, S.; Albà, X.; et al. Evaluation of state-of-the-art segmentation algorithms for left ventricle infarct from late Gadolinium enhancement MR images. Med. Image Anal. 2016, 30, 95–107. [Google Scholar] [CrossRef] [PubMed]
- MS-CMRSeg Challenge. Available online: https://zmiclab.github.io/projects/mscmrseg19/ (accessed on 24 September 2020).
- MyoPS Challenge. Available online: https://zenodo.org/record/3715932#.X18wQxAzZaQ (accessed on 24 September 2020).
- Ibanez, B.; Aletras, A.H.; Arai, A.E.; Arheden, H.; Bax, J.; Berry, C.; Bucciarelli-Ducci, C.; Croisille, P.; Dall’Armellina, E.; Dharmakumar, R.; et al. Cardiac MRI endpoints in myocardial infarction experimental and clinical trials: JACC scientific expert panel. J. Am. Coll. Cardiol. 2019, 74, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Croisille, P.; Revel, D.; Saeed, M. Contrast agents and cardiac MR imaging of myocardial ischemia: From bench to bedside. Eur. Radiol. 2006, 16, 1951–1963. [Google Scholar] [CrossRef] [PubMed]
- Mewton, N.; Liu, C.Y.; Croisille, P.; Bluemke, D.; Lima, J.A. Assessment of Myocardial Fibrosis with Cardiac Magnetic Resonance. J. Am. Coll. Cardiol. 2011, 57, 891–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochet, A.; Lorgis, L.; Lalande, A.; Zeller, M.; Beer, J.C.; Walker, P.M.; Touzery, C.; Wolf, J.E.; Brunotte, F.; Cottin, Y. Major prognostic impact of persistent microvascular obstruction as assessed by contrast-enhanced cardiac magnetic resonance in reperfused acute myocardial infarction. Eur. Radiol. 2009, 19, 2117–2126. [Google Scholar] [CrossRef] [PubMed]
- Pineda, V.; Merino, X.; Gispert, S.; Mahía, P.; Garcia, B.; Domínguez-Oronoz, R. No-reflow phenomenon in cardiac MRI: Diagnosis and clinical implications. AJR Am. J. Roentgenol. 2008, 191, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Alpert, J.S.; Thygesen, K.; Antman, E.; Bassand, J.P. Myocardial infarction redefined—A consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J. Am. Coll. Cardiol. 2000, 36, 959–969. [Google Scholar] [PubMed] [Green Version]
- Killip, T., III; Kimball, J.T. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am. J. Cardiol. 1967, 20, 457–464. [Google Scholar] [CrossRef]
- Cochet, A.; Zeller, M.; Cottin, Y.; Robert-Valla, C.; Lalande, A.; L’Huilllier, I.; Comte, A.; Walker, P.M.; Desgres, J.; Wolf, J.E.; et al. The extent of myocardial damage assessed by contrast-enhanced MRI is a major determinant of N-BNP concentration after myocardial infarction. Eur. J. Heart Fail. 2004, 6, 555–560. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Score | Features |
|---|---|
| 1 | No sign of heart failure |
| 2 | Rales in the lungs, third heart sound (S3), and elevated jugular venous pressure, |
| 3 | Acute pulmonary edema |
| 4 | Cardiogenic shock or arterial hypotension, and evidence of peripheral vasoconstriction |
| Item Name | Comment | Type | Example |
|---|---|---|---|
| Case | Name of the exam | Characters | Case P001 1 |
| Gap between slices | Distance between two slices | Distance in mm | 10 mm |
| Sex | Sex | Character (F or M) | F |
| Age | Age in years | Number | 71 |
| Tobacco | Tobacco (yes, no, or former smoker) | Number between 1 to 3 | 1 |
| Overweight | Overweight if BMI > 25 | Character (Y/N) | Y |
| Arterial hypertension | Character (Y/N) | Y | |
| Diabetes | Character (Y/N) | Y | |
| Familial history of coronary artery disease | Previous cardiovascular events | Character (Y/N) | Y |
| ECG (ST +) | MI with STEMI | Character (Y/N) | Y |
| Troponin | Number (value in ng per mL of blood) | 11 | |
| Killip max | Number between 1 to 4 | 2 | |
| LVEF | LVEF calculated from echocardiography | Number (percentage) | 45 |
| NTProBNP | Number (value in pg per mL of blood) | 229 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lalande, A.; Chen, Z.; Decourselle, T.; Qayyum, A.; Pommier, T.; Lorgis, L.; de la Rosa, E.; Cochet, A.; Cottin, Y.; Ginhac, D.; et al. Emidec: A Database Usable for the Automatic Evaluation of Myocardial Infarction from Delayed-Enhancement Cardiac MRI. Data 2020, 5, 89. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040089
Lalande A, Chen Z, Decourselle T, Qayyum A, Pommier T, Lorgis L, de la Rosa E, Cochet A, Cottin Y, Ginhac D, et al. Emidec: A Database Usable for the Automatic Evaluation of Myocardial Infarction from Delayed-Enhancement Cardiac MRI. Data. 2020; 5(4):89. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040089
Chicago/Turabian StyleLalande, Alain, Zhihao Chen, Thomas Decourselle, Abdul Qayyum, Thibaut Pommier, Luc Lorgis, Ezequiel de la Rosa, Alexandre Cochet, Yves Cottin, Dominique Ginhac, and et al. 2020. "Emidec: A Database Usable for the Automatic Evaluation of Myocardial Infarction from Delayed-Enhancement Cardiac MRI" Data 5, no. 4: 89. https://0-doi-org.brum.beds.ac.uk/10.3390/data5040089