
A Long-Term, Real-Life Parkinson Monitoring Database Combining Unscripted Objective and Subjective Recordings

 , ,
, ,  and
and
Abstract
:1. Summary
2. Data Description
2.1. Objective Sensor Data
- The name of every edf-file contains first the sensor name, followed by the start date and time of the recording. For example, in folder “110001”, the file “13792_20180828_0752223.edf” contains the recording from participant 110001 with sensor 13792, which started recording on 28 August 2018, at 07:52:23. The read-me file “READ_ME_EMA_SENSOR_PD.txt” explains which sensor numbers represent left wrist, right wrist, or chest IMUs. The sensors actively recorded when they were not connected to a USB-charging device.
- Each edf-file contains six channels (representing the x-, y-, and z-axes for, respectively, accelerometer and gyroscope), including timestamps. Acceleration is recorded in m/s per second, and rotation is recorded in degrees per second.
- Prior to the first recording day, the clocks of all three sensors were reset and synchronized. The manufacturer assures temporal drift to be negligible over the period of two weeks with respect to merging and pairing with EMA-assessments.
- Single edf-files were created when a sensor was disconnected from the charger. A file continued storing data until the sensor was connected to a charger again and the file closed. If a recording passed midnight (00:00:00), the file closed as well, and a new file was created and continued storing data.
2.2. Subjective EMA Data
2.2.1. EMA Data Organization
- The EMA data from all patients are stored in “EMA_data.csv”.
- The fist column provides a patient number, corresponding to the sensor data folder names.
- Then, two columns provide timestamps indicating the start time and end time of beep-questionnaire completion.
- These are followed by columns providing the answers on the items from the beep-questionnaire.
- Then, columns provide the answers on the morning and evening questionnaires from the corresponding day.
- The file “EMA_data_coding.xlsx” provides a clear explanation of the coding of all questionnaire items and answers.
2.2.2. EMA Content
3. Methods
3.1. Participants
3.2. Study Design
3.3. Parkinson’s-Specific EMA Method
3.4. Devices
3.4.1. PsyMate (EMA Application)
3.4.2. MOX-5 (Wearable Sensor)
4. User Notes
4.1. Software
4.2. Interpretation of Data Quantity and Quality
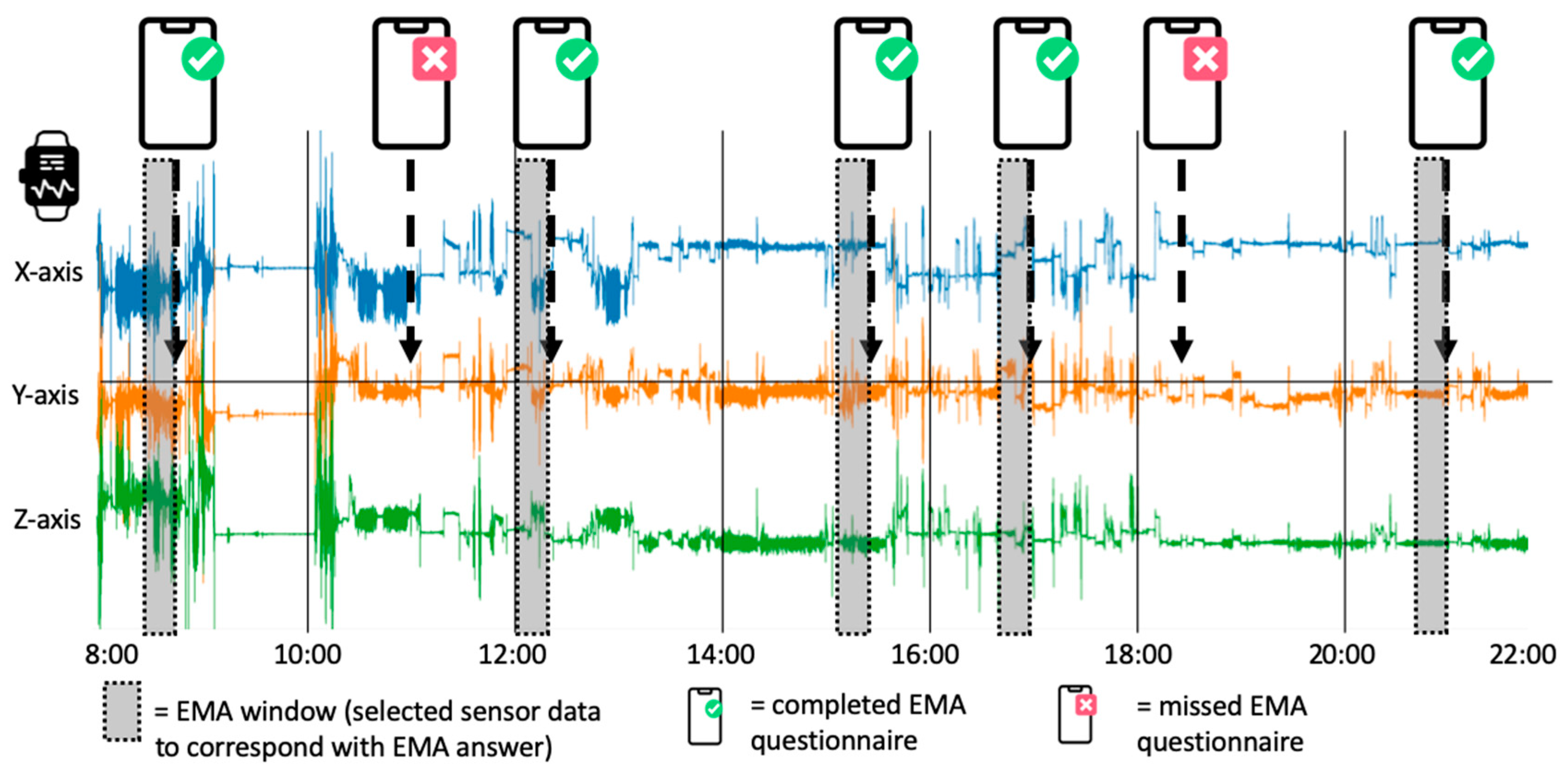
4.3. Combined Data Processing and Analyzing: Practical Example of Dopaminergic Fluctuation Detection
4.3.1. Data Merging
4.3.2. Sensor Data Pre-Processing and Feature Extraction
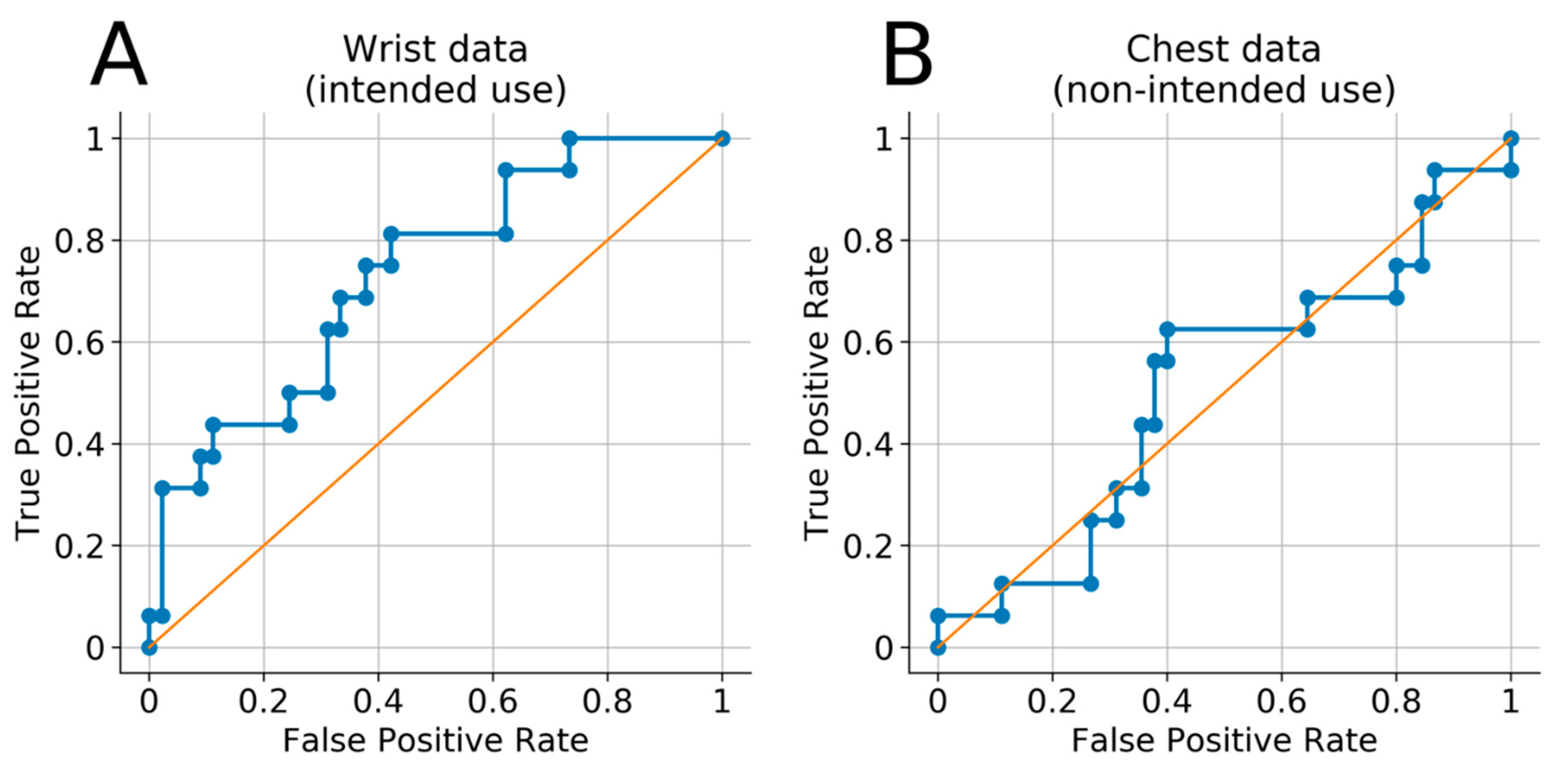
4.3.3. Classification Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Sherer, T.; Okun, M.S.; Bloem, B.R. The Emerging Evidence of the Parkinson Pandemic. J. Parkinsons Dis. 2018, 8, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Odin, P.; Ray Chaudhuri, K.; Slevin, J.T.; Volkmann, J.; Dietrichs, E.; Martinez-Martin, P.; Krauss, J.K.; Henriksen, T.; Katzenschlager, R.; Antonini, A.; et al. Collective physician perspectives on non-oral medication approaches for the management of clinically relevant unresolved issues in Parkinson’s disease: Consensus from an international survey and discussion program. Parkinsonism Relat. Disord. 2015, 21, 1133–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seppi, K.; Weintraub, D.; Coelho, M.; Perez-Lloret, S.; Fox, S.H.; Katzenschlager, R.; Hametner, E.M.; Poewe, W.; Rascol, O.; Goetz, C.G.; et al. The Movement Disorder Society Evidence-Based Medicine Review Update: Treatments for the non-motor symptoms of Parkinson’s disease. Mov. Disord. 2011, 26, 42–80. [Google Scholar] [CrossRef]
- Papapetropoulos, S.; Mitsi, G.; Espay, A.J. Digital Health Revolution: Is it Time for Affordable Remote Monitoring for Parkinson’s Disease? Front. Neurol. 2015, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, C.; Sanchez-Ferro, A.; Maetzler, W. How Mobile Health Technology and Electronic Health Records Will Change Care of Patients with Parkinson’s Disease. J. Parkinsons Dis. 2018, 8, 41–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odin, P.; Chaudhuri, K.R.; Volkmann, J.; Antonini, A.; Storch, A.; Dietrichs, E.; Pirtosek, Z.; Henriksen, T.; Horne, M.; Devos, D.; et al. Viewpoint and practical recommendations from a movement disorder specialist panel on objective measurement in the clinical management of Parkinson’s disease. Npj Parkinsons Dis. 2018, 4, 14. [Google Scholar] [CrossRef]
- Pahwa, R.; Isaacson, S.H.; Torres-Russotto, D.; Nahab, F.B.; Lynch, P.M.; Kotschet, K.E. Role of the Personal KinetiGraph in the routine clinical assessment of Parkinson’s disease: Recommendations from an expert panel. Expert Rev. Neurother. 2018, 18, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Thorp, J.E.; Adamczyk, P.G.; Ploeg, H.L.; Pickett, K.A. Monitoring Motor Symptoms During Activities of Daily Living in Individuals With Parkinson’s Disease. Front. Neurol. 2018, 9, 1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powers, R.; Etezadi-Amoli, M.; Arnold, E.M.; Kianian, S.; Mance, I.; Gibiansky, M.; Trietsch, D.; Alvarado, A.S.; Kretlow, J.D.; Herrington, T.M.; et al. Smartwatch inertial sensors continuously monitor real-world motor fluctuations in Parkinson’s disease. Sci. Transl. Med. 2021, 13, e7865. [Google Scholar] [CrossRef]
- Choi, K.W.; Chen, C.Y.; Stein, M.B.; Klimentidis, Y.C.; Wang, M.J.; Koenen, K.C.; Smoller, J.W. Assessment of Bidirectional Relationships Between Physical Activity and Depression Among Adults: A 2-Sample Mendelian Randomization Study. JAMA Psychiatry 2019, 76, 399–408. [Google Scholar] [CrossRef]
- Heijmans, M.; Habets, J.G.V.; Herff, C.; Aarts, J.; Stevens, A.; Kuijf, M.L.; Kubben, P.L. Monitoring Parkinson’s disease symptoms during daily life: A feasibility study. Npj Parkinsons Dis. 2019, 5, 21. [Google Scholar] [CrossRef]
- Vizcarra, J.A.; Sanchez-Ferro, A.; Maetzler, W.; Marsili, L.; Zavala, L.; Lang, A.E.; Martinez-Martin, P.; Mestre, T.A.; Reilmann, R.; Hausdorff, J.M.; et al. The Parkinson’s disease e-diary: Developing a clinical and research tool for the digital age. Mov. Disord. 2019, 34, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Neurotechnologies, G.L. Kinesia ProViewTM. Available online: https://www.glneurotech.com/blog/2013/05/15/press-release-kinesia-proview-launches-to-visualize-parkinsons-symptom-response-to-deep-brain-stimulation-programming/ (accessed on 20 November 2017).
- Rodriguez-Molinero, A.; Perez-Lopez, C.; Sama, A.; de Mingo, E.; Rodriguez-Martin, D.; Hernandez-Vara, J.; Bayes, A.; Moral, A.; Alvarez, R.; Perez-Martinez, D.A.; et al. A Kinematic Sensor and Algorithm to Detect Motor Fluctuations in Parkinson Disease: Validation Study under Real Conditions of Use. JMIR Rehabil. Assist. Technol. 2018, 5, e8. [Google Scholar] [CrossRef] [PubMed]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.; Keller, A. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Fasano, A.; Mancini, M. Wearable-based mobility monitoring: The long road ahead. Lancet Neurol. 2020, 19, 378–379. [Google Scholar] [CrossRef]
- Kelly, C.J.; Karthikesalingam, A.; Suleyman, M.; Corrado, G.; King, D. Key challenges for delivering clinical impact with artificial intelligence. BMC Med. 2019, 17, 195. [Google Scholar] [CrossRef] [Green Version]
- Pencina, M.J.; Goldstein, B.A.; D’Agostino, R.B. Prediction Models—Development, Evaluation, and Clinical Application. N. Engl. J. Med. 2020, 382, 1583–1586. [Google Scholar] [CrossRef]
- Kluge, F.; Del Din, S.; Cereatti, A.; Gaßner, H.; Hansen, C.; Helbostadt, J.L.; Klucken, J.; Küderle, A.; Müller, A.; Rochester, L.; et al. Consensus based framework for digital mobility monitoring. medRxiv 2020. [Google Scholar] [CrossRef]
- Galperin, I.; Hillel, I.; Del Din, S.; Bekkers, E.M.J.; Nieuwboer, A.; Abbruzzese, G.; Avanzino, L.; Nieuwhof, F.; Bloem, B.R.; Rochester, L.; et al. Associations between daily-living physical activity and laboratory-based assessments of motor severity in patients with falls and Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 62, 85–90. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hagell, P.; Nygren, C. The 39 item Parkinson’s disease questionnaire (PDQ-39) revisited: Implications for evidence based medicine. J. Neurol. Neurosurg. Psychiatry 2007, 78, 1191–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evers, L.J.W.; Krijthe, J.H.; Meinders, M.J.; Bloem, B.R.; Heskes, T.M. Measuring Parkinson’s disease over time: The real-world within-subject reliability of the MDS-UPDRS. Mov. Disord. 2019, 34, 1480–1487. [Google Scholar] [CrossRef] [Green Version]
- Heijmans, M.; Habets, J.; Kuijf, M.; Kubben, P.; Herff, C. Evaluation of Parkinson’s disease at home: Predicting tremor from wearable sensors. In Proceedings of the 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 584–587. [Google Scholar]
- Todorova, A.; Jenner, P.; Ray Chaudhuri, K. Non-motor Parkinson’s: Integral to motor Parkinson’s, yet often neglected. Pract. Neurol. 2014, 14, 310. [Google Scholar] [CrossRef]
- Seppala, J.; De Vita, I.; Jamsa, T.; Miettunen, J.; Isohanni, M.; Rubinstein, K.; Feldman, Y.; Grasa, E.; Corripio, I.; Berdun, J.; et al. Mobile Phone and Wearable Sensor-Based mHealth Approaches for Psychiatric Disorders and Symptoms: Systematic Review. JMIR Ment. Health 2019, 6, e9819. [Google Scholar] [CrossRef] [PubMed]
- Simons, C.J.; Hartmann, J.A.; Kramer, I.; Menne-Lothmann, C.; Hohn, P.; van Bemmel, A.L.; Myin-Germeys, I.; Delespaul, P.; van Os, J.; Wichers, M. Effects of momentary self-monitoring on empowerment in a randomized controlled trial in patients with depression. Eur. Psychiatry 2015, 30, 900–906. [Google Scholar] [CrossRef]
- Broen, M.P.; Marsman, V.A.; Kuijf, M.L.; Van Oostenbrugge, R.J.; van Os, J.; Leentjens, A.F. Unraveling the Relationship between Motor Symptoms, Affective States and Contextual Factors in Parkinson’s Disease: A Feasibility Study of the Experience Sampling Method. PLoS ONE 2016, 11, e0151195. [Google Scholar] [CrossRef]
- Mahadevan, N.; Demanuele, C.; Zhang, H.; Volfson, D.; Ho, B.; Erb, M.K.; Patel, S. Development of digital biomarkers for resting tremor and bradykinesia using a wrist-worn wearable device. Npj Digit. Med. 2020, 3, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Molinero, A. Monitoring of Mobility of Parkinson’s Patients for Therapeutic Purposes—Clinical Trial (MoMoPa-EC). Available online: https://clinicaltrials.gov/ct2/show/NCT04176302 (accessed on 18 November 2020).
- Michael, J. Fox Fundation. Beat-PD Dream Challenge (by Sage Bionetworks; Michael, J. Fox Foundation). Available online: https://www.michaeljfox.org/grant/beat-pd-biomarker-and-endpoint-assessment-track-parkinsons-disease-dream-challenge (accessed on 7 January 2021).
- Loring, D.W.; Block, C.; Staikova, E.; Miocinovic, S. Patient-Reported Outcomes Measurement Information System (PROMIS) Assessment of Non-Motor Features in Deep Brain Stimulation Candidates: Relationship to the Beck Depression and Anxiety Inventories. Arch. Clin. Neuropsychol. 2020. [Google Scholar] [CrossRef]
- Bloem, B.R.; Marks, W.J.J.; Silva de Lima, A.L.; Kuijf, M.L.; van Laar, T.; Jacobs, B.P.F.; Verbeek, M.M.; Helmich, R.C.; van de Warrenburg, B.P.; Evers, L.J.W.; et al. The Personalized Parkinson Project: Examining disease progression through broad biomarkers in early Parkinson’s disease. BMC Neurol. 2019, 19, 160. [Google Scholar] [CrossRef] [Green Version]
- Rochester, L.; Mazzà, C.; Mueller, A.; Caulfield, B.; McCarthy, M.; Becker, C.; Miller, R.; Piraino, P.; Viceconti, M.; Dartee, W.P.; et al. A Roadmap to Inform Development, Validation and Approval of Digital Mobility Outcomes: The Mobilise-D Approach. Digit. Biomark. 2020, 4, 13–27. [Google Scholar] [CrossRef]
- Habets, J.; Kubben, P. EMA and Wearable Sensor Monitoring in PD, V2 ed.; Maastricht University: Maastricht, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Kemp, B.; Varri, A.; Rosa, A.C.; Nielsen, K.D.; Gade, J. A simple format for exchange of digitized polygraphic recordings. Electroencephalogr. Clin Neurophysiol. 1992, 82, 391–393. [Google Scholar] [CrossRef]
- Verhagen, S.J.; Hasmi, L.; Drukker, M.; van Os, J.; Delespaul, P.A. Use of the experience sampling method in the context of clinical trials. Evid. Based Ment. Health 2016, 19, 86–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brannon, E.E.; Cushing, C.C.; Crick, C.J.; Mitchell, T.B. The promise of wearable sensors and ecological momentary assessment measures for dynamical systems modeling in adolescents: A feasibility and acceptability study. Transl. Behav. Med. 2016, 6, 558–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmier-Claus, J.E.; Myin-Germeys, I.; Barkus, E.; Bentley, L.; Udachina, A.; Delespaul, P.A.; Lewis, S.W.; Dunn, G. Experience sampling research in individuals with mental illness: Reflections and guidance. Acta Psychiatr. Scand. 2011, 123, 12–20. [Google Scholar] [CrossRef]
- Habets, J.; Heijmans, M.; Herff, C.; Simons, C.; Leentjens, A.F.; Temel, Y.; Kuijf, M.; Kubben, P. Mobile Health Daily Life Monitoring for Parkinson Disease: Development and Validation of Ecological Momentary Assessments. JMIR mHealth uHealth 2020, 8, e15628. [Google Scholar] [CrossRef]
- Papapetropoulos, S.S. Patient diaries as a clinical endpoint in Parkinson’s disease clinical trials. CNS Neurosci. Ther. 2012, 18, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Erb, M.K.; Karlin, D.R.; Ho, B.K.; Thomas, K.C.; Parisi, F.; Vergara-Diaz, G.P.; Daneault, J.F.; Wacnik, P.W.; Zhang, H.; Kangarloo, T.; et al. mHealth and wearable technology should replace motor diaries to track motor fluctuations in Parkinson’s disease. Npj Digit. Med. 2020, 3, 6. [Google Scholar] [CrossRef]
- Reback, J.; McKinney, W.; jbrockmendel; Van den Bossche, J.; Augspurger, T.; Cloud, P.; gfyoung; Sinhrks; Hawkins, S.; Klein, A.; et al. Psifr: Analysis and Visualization of Free Recall Data. Pandas-dev/pandas: Pandas 1.1.1, 2020 (Version v1.1.1) Zenodo. Available online: http://0-doi-org.brum.beds.ac.uk/10.5281/zenodo.3993412 (accessed on 20 August 2020).
- Van der Walt, S.; Colbert, S.C.; Varoquaux, G. The NumPy Array: A Structure for Efficient Numerical Computation. Comput. Sci. Eng. 2011, 13, 22–30. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]



{kind=link}
{kind=link}
| Beep Questionnaire (Repetitive, Seven Times Daily) | |
|---|---|
| Affect and cognitive items | Possible answers |
| I feel well, down, fearful, stressed, sleepy, tired, cheerful, relaxed (eight different items) | 7-point Likert scale (eight times) |
| I can concentrate well | 7-point Likert scale |
| I experience hallucinations | 7-point Likert scale |
| Contextual items | |
| I am at … | (home, work, travelling, family/friend’s place, in public) |
| I am with … | (nobody, family, partner, colleagues, friends) (multiple choice, multiple items could be selected) |
| I am doing … | (work, resting, household/odd jobs, sports, something else) (multiple choice, multiple items could be selected) |
| Physical items | |
| I can do this (my current activity) without hinder | 7-point Likert scale |
| I am comfortable walking and standing | 7-point Likert scale |
| I can sit or stand still easily | 7-point Likert scale |
| I can speak easily | 7-point Likert scale |
| I can walk easily | 7-point Likert scale |
| I experience tremor | 7-point Likert scale |
| I am moving slow | 7-point Likert scale |
| I experience stiffness | 7-point Likert scale |
| My muscles are tensioned | 7-point Likert scale |
| I am uncontrollable moving | 7-point Likert scale |
| Dopaminergic medication items | |
| I feel … (regarding medication status) | [1: OFF, 2: ON → OFF, 3: ON, 4: OFF → ON] |
| I took Parkinson’s medication since last beep | (yes, no, I do not recall) |
| Morning questionnaire | |
| I slept well | 7-point Likert scale |
| I woke up often last night | 7-point Likert scale |
| I feel rested | 7-point Likert scale |
| It was physically difficult to get up | 7-point Likert scale |
| It was mentally difficult to get up | 7-point Likert scale |
| Evening questionnaire | |
| I had long OFF periods today | 7-point Likert scale |
| I had many OFF periods today | 7-point Likert scale |
| Walking, dressing, eating/drinking, personal care, household activities went well today (five separate items) | 7-point Likert scale (five times) |
| I was tired today | 7-point Likert scale |
| Variable | Mean (Standard Deviation) or Proportion (n) |
|---|---|
| Gender (n female/n male) | 4/16 |
| Age (years) | 63 (7) |
| Levodopa Equivalent Daily Dosage (mg) | 770 (394) |
| Hoehn and Yahr Scale (n) | |
| 1 | 2 |
| 1.5 | 2 |
| 2 | 7 |
| 2.5 | 3 |
| 3 | 3 |
| 3.5 | 0 |
| 4 | 1 |
| Presence Motor Fluctuations (n yes/n no) | 12/8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habets, J.G.V.; Heijmans, M.; Leentjens, A.F.G.; Simons, C.J.P.; Temel, Y.; Kuijf, M.L.; Kubben, P.L.; Herff, C. A Long-Term, Real-Life Parkinson Monitoring Database Combining Unscripted Objective and Subjective Recordings. Data 2021, 6, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/data6020022
Habets JGV, Heijmans M, Leentjens AFG, Simons CJP, Temel Y, Kuijf ML, Kubben PL, Herff C. A Long-Term, Real-Life Parkinson Monitoring Database Combining Unscripted Objective and Subjective Recordings. Data. 2021; 6(2):22. https://0-doi-org.brum.beds.ac.uk/10.3390/data6020022
Chicago/Turabian StyleHabets, Jeroen G. V., Margot Heijmans, Albert F. G. Leentjens, Claudia J. P. Simons, Yasin Temel, Mark L. Kuijf, Pieter L. Kubben, and Christian Herff. 2021. "A Long-Term, Real-Life Parkinson Monitoring Database Combining Unscripted Objective and Subjective Recordings" Data 6, no. 2: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/data6020022