
Canadian Dental Patients with a Single-Unit Implant-Supported Restoration in the Aesthetic Region of the Mouth: Qualitative and Quantitative Patient-Reported Outcome Measures (PROMs)



Abstract
:Abstract
Dataset
Dataset License
1. Summary
2. Data Description
3. Experimental Design, Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
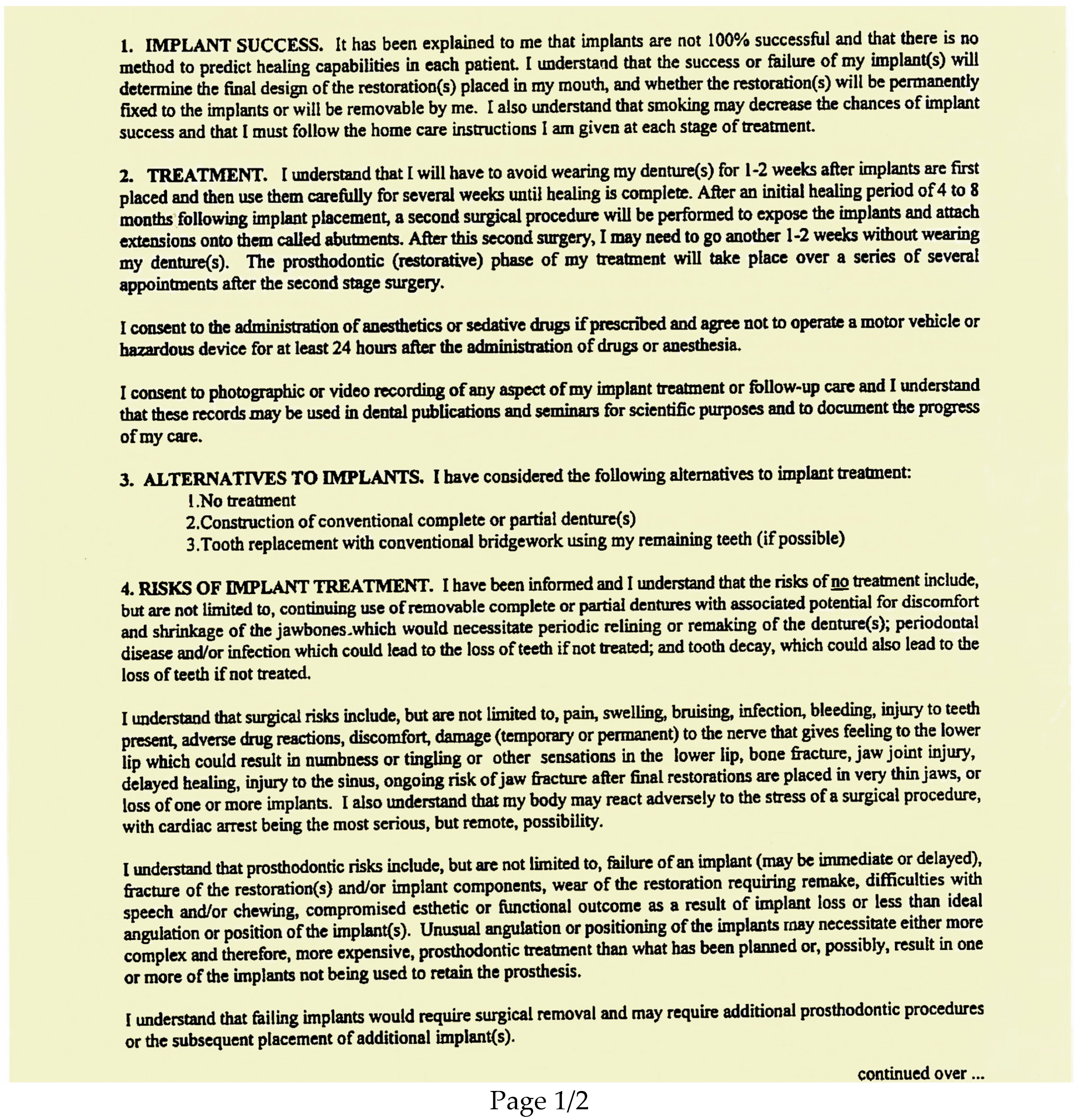
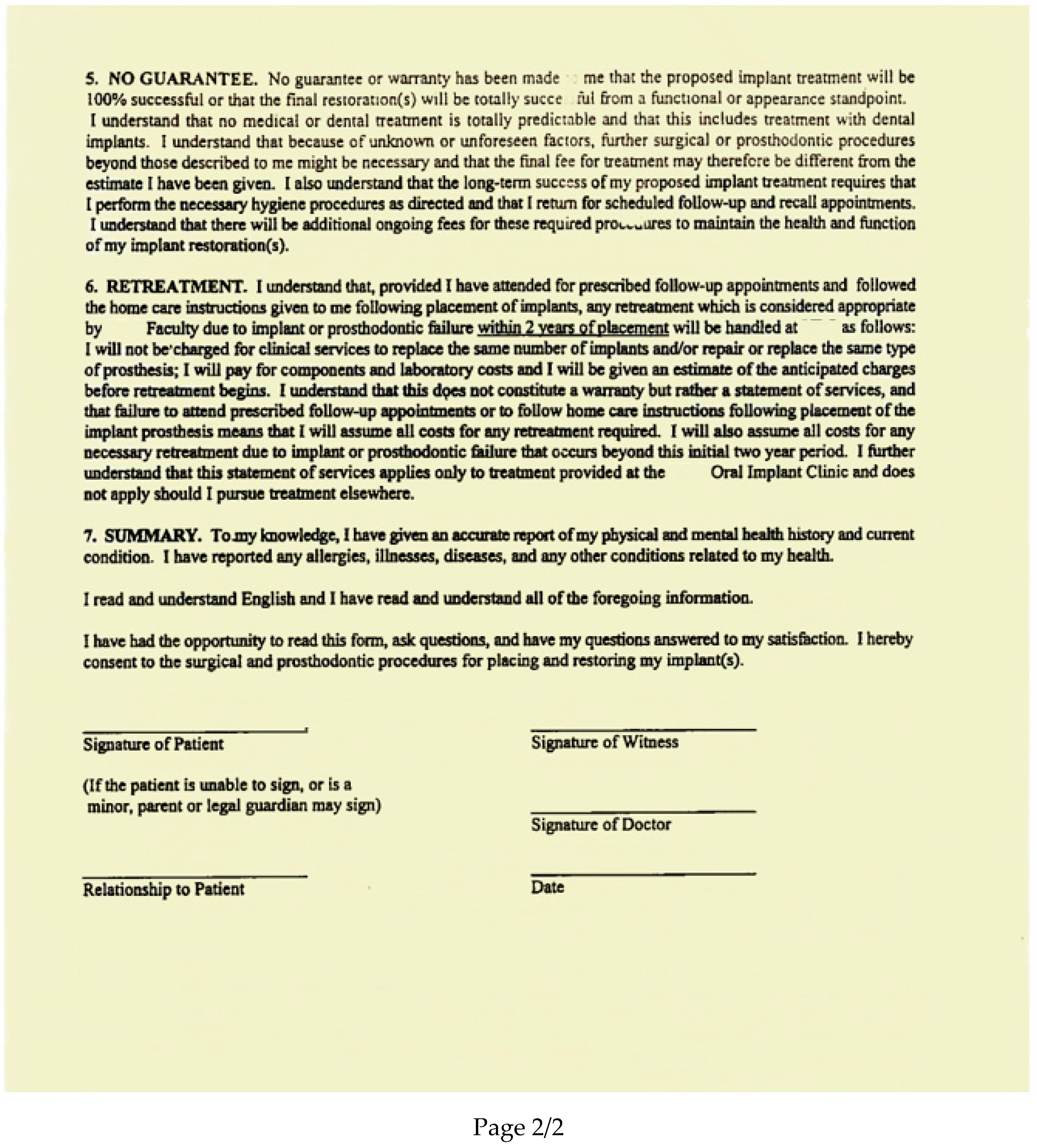
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statement
References
- Hazaveh, M.; Hovey, R. Patient experience of living with orofacial pain: An interpretive phenomenological study. JDR Clin. Trans. Res. 2018, 3, 264–271, [Included 6 participants]. [Google Scholar] [CrossRef] [PubMed]
- Polit, D.F.; Beck, C.T. Generalization in quantitative and qualitative research: Myths and strategies. Int. J. Nurs. Stud. 2010, 47, 1451–1458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesaffre, E.; Feine, J.; Leroux, B.; Declerck, D. Statistical and Methodological Aspects of Oral Health Research; Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- van Manen, M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy; Routledge: New York, NY, USA, 2016. [Google Scholar]
- van Manen, M. Phenomenology of Practice: Meaning-Giving Methods in Phenomenological Research and Writing; Routledge: New York, NY, USA, 2014. [Google Scholar]
- Afrashtehfar, K.I.; Bryant, S.R. Understanding the lived experience of North American dental patients with a single-tooth implant in the upper front region of the mouth: Protocol for a qualitative study. JMIR. Res. Protoc. 2021, 10, e25767. [Google Scholar] [CrossRef] [PubMed]
- Guest, G.; Bunce, A.; Johnson, L. How many interviews are enough? Field Methods 2016, 18, 59–82. [Google Scholar] [CrossRef]
- Kashbour, W.A.; Rousseau, N.S.; Thomason, J.M.; Ellis, J.S. Provision of information to patients on dental implant treatment: Clinicians’ perspectives on the current approaches and future strategies. J. Dent. 2018, 76, 117–124, [Included 8 participants]. [Google Scholar] [CrossRef]
- Grey, E.B.; Harcourt, D.; O’Sullivan, D.; Buchanan, H.; Kilpatrick, N.M. A qualitative study of patients’ motivations and expectations for dental implants. Br. Dent. J. 2013, 214, E1, [Included 9 participants]. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afshari, F.S.; Yuan, J.-C.-C.; Quimby, A.; Harlow, R.; Campbell, S.D.; Sukotjo, C. Advanced predoctoral implant program at UIC: Description and qualitative analysis. J. Dent. Educ. 2014, 78, 770–778, [Included 9 participants]. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; Assery, M.K.A.; Bryant, S.R. Aesthetic parameters and patient-perspective assessment tools for maxillary anterior single implants. Int. J. Dent. 2021, 2021, 6684028. [Google Scholar] [CrossRef] [PubMed]
- Belser, U.C.; Grutter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; Brägger, U.; Hicklin, S.P. Reliability of interproximal bone height measurements in bone- and tissue-level implants: A methodological study for improved calibration purposes. Int. J. Oral. Maxillofac. Implants 2020, 35, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Afrashtehfar, K.I.; Assery, M.K.A.; Bryant, S.R. Patient satisfaction in medicine and dentistry. Int. J. Dent. 2020, 2020, 6621848. [Google Scholar] [CrossRef]
- Del Monte, S.; Afrashtehfar, K.I.; Emami, E.; Abi Nader, S.; Tamimi, F. Lay preferences for dentogingival esthetic parameters: A systematic review. J. Prosthet. Dent. 2017, 118, 717–724. [Google Scholar] [CrossRef]
- Willig, C.; Stainton-Rogers, W. The SAGE Handbook of Qualitative Research in Psychology, 2nd ed.; SAGE Publications Ltd. Long: Sauzender Oaks, CA, USA, 2017. [Google Scholar] [CrossRef]
- Ghanem, H.; Afrashtehfar, K.I.; Abi-Nader, S.; Tamimi, F. Impact of a “TED-Style” presentation on potential patients’ willingness to accept dental implant therapy: A one-group, pre-test post-test study. J. Adv. Prosthodont. 2015, 7, 437–445. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Assery, M.K. Five considerations in cosmetic and esthetic dentistry. J. N. J. Dent. Assoc. 2014, 85, 14–15. [Google Scholar] [PubMed]
- [dataset]. Afrashtehfar, K.I. Coded qualitative responses into categories to allow for additional analyses, Mendeley Data, v1. 2020. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question ID | Participant ID * | Mean | SD | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |||
| A | B | C | D | E | F | H | I | J | |||
| Q1 | 100 | 99 | 81 | 78 | 89 | 73 | 78 | 91 | 100 | 87.7 | 10.6 |
| Q2 | 100 | 99 | 79 | 86 | 91 | 84 | 80 | 92 | 100 | 90.1 | 8.4 |
| Q3 | 100 | 99 | 80 | 90 | 88 | 65 | 82 | 89 | 100 | 88.1 | 11.4 |
| Q4 | 80 | 99 | 82 | 76 | 90 | 63 | 83 | 95 | 100 | 85.3 | 12.0 |
| Q5 | 100 | 98 | 66 | 88 | 90 | 68 | 82 | 98 | 100 | 87.8 | 13.3 |
| Q6 | 87 | 99 | 100 | 85 | 91 | 72 | 59 | 83 | 100 | 86.2 | 13.8 |
| Mean | 94.5 | 98.8 | 81.3 | 83.8 | 89.8 | 70.8 | 77.3 | 91.3 | 100 | – | – |
| SD | 8.8 | 0.4 | 10.9 | 5.6 | 1.2 | 7.5 | 9.2 | 5.2 | 0 | – | – |
| Participant ID * | Tooth Implant Site (FDI) | Pink Aesthetic Score | White Aesthetic Score | Total PES | Total WES | TOTAL PES/WES | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesial Papillae | Distal Papillae | Curvature of the Facial Soft Tissue Line | Level of Facial Mucosa | Root Convexity/Soft Tissue Colour and Texture | Tooth Form | Outline and Volume of the Clinical Crown | Colour | Surface Texture | Translucency and characterization | ||||||
| 1 | A | 21 | 1 | 0.5 | 0 | 1 | 1.5 | 0.5 | 0.5 | 2 | 1.5 | 0.5 | 3 | 5 | 8 |
| 2 | B | 11 | 1.5 | 1.5 | 1 | 2 | 1 | 1.5 | 1.5 | 1 | 2 | 2 | 8 | 8 | 16 |
| 3 | C | 21 | 1.5 | 1.5 | 1.5 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 6.5 | 6 | 12.5 |
| 4 | D | 22 | 0.5 | 1 | 1 | 1.5 | 0.5 | 1 | 1.5 | 1.5 | 1 | 1 | 4 | 6 | 10 |
| 5 | E | 22 | 2 | 2 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 2 | 1 | 7.5 | 4.5 | 12 |
| 6 | F | 22 | 1 | 2 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | 1 | 1 | 5 | 4.5 | 9.5 |
| 7 | H | 24 | 1 | 1.5 | 1 | 1.5 | 1.5 | 26 | 24 | 2 | 1.5 | 1.5 | 6.5 | 7.5 | 14 |
| 8 | I | 22 | 1 | 1.5 | 1 | 0 | 1 | 60 | 22 | 0.5 | 1.5 | 1 | 4.5 | 4 | 8.5 |
| 9 | J | 21 | 1.5 | 0 | 1 | 0 | 0.5 | 66 | 21 | 1 | 1 | 0.5 | 3 | 3 | 6 |
| Part 1: Introductory Background Questions (Icebreaker) How long ago did you come to lose your tooth? How did you get interested/motivated in dental implants? How did you come to make the decision? Were you provided enough information at school (dental specialty students) for deciding to have an implant? What was the most attractive idea about having an implant? How long did it take you to make the decision to have an implant? What information would you wish you had at the beginning to be better prepared before going for the implant? Did you investigate the risks of something going wrong? How comfortable would you be now if you needed a new implant in another place? |
| Part 2: Is about Your Overall Satisfaction with the Implant Tooth So, would you say the overall results were better or worse than expected? Why? |
| Part 3: Is about Your Satisfaction with the Appearance (or Look) of Your Implant Tooth Do you feel you received enough information about what to expect? What would you liked to have been explained better? Was the result better or worse than expected? |
| Part 4: Is about Satisfaction with Your Functioning and Social Experiences Relating to Your Implant Tooth Is there anything you expected to be able to do with your dental implant that you cannot? What? Why? After having the dental implant, has there been any kind of improvement in (1) confidence, (2) self-image/self-esteem, (3) social life? How? Could you give an example? |
| Part 5: Any other Important Experiences that Affect Satisfaction with Your Implant Tooth, such as Complications, Maintenance or Financial Aspects Was there any lip biting or discomfort immediately after the crown was implanted? |
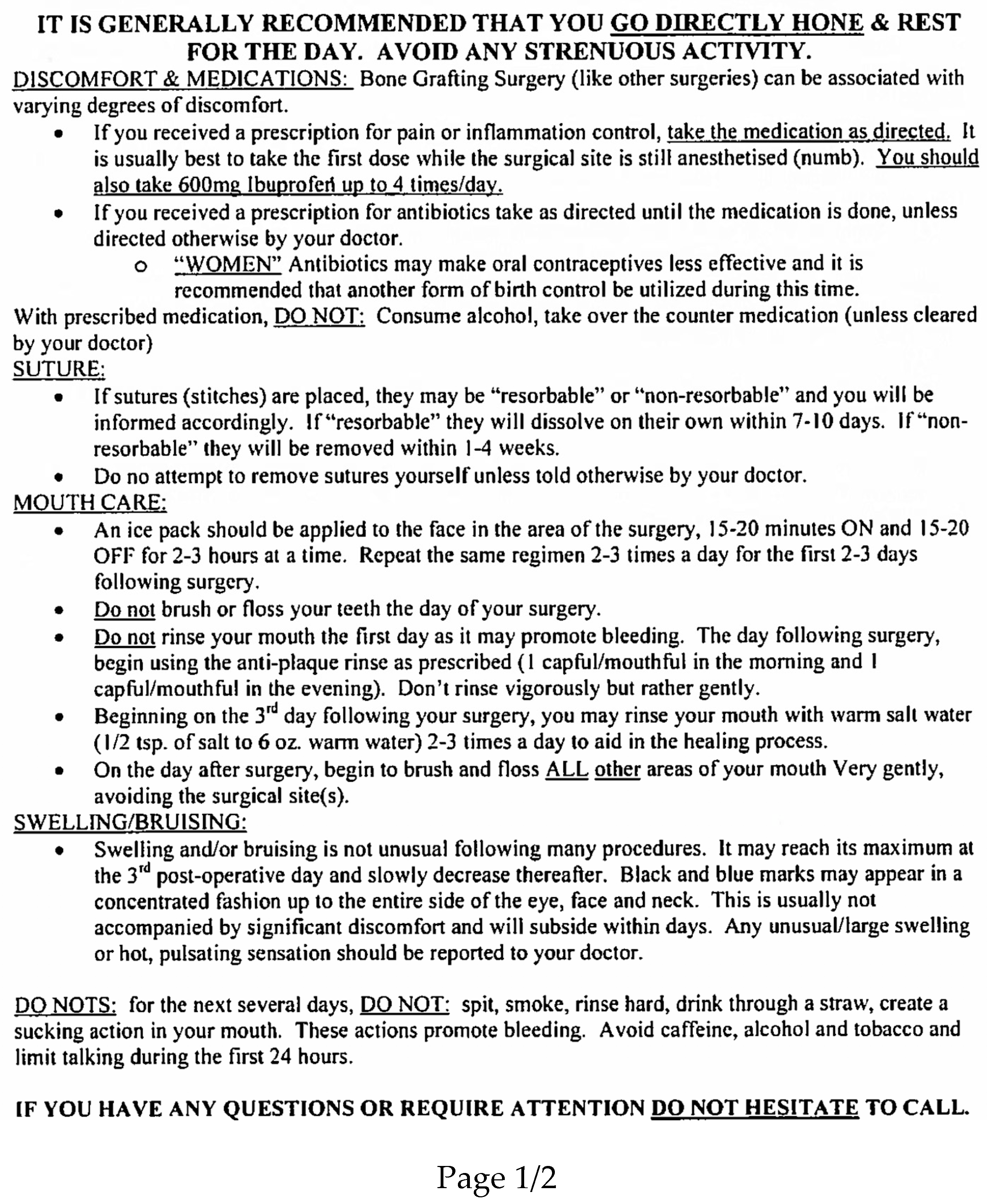
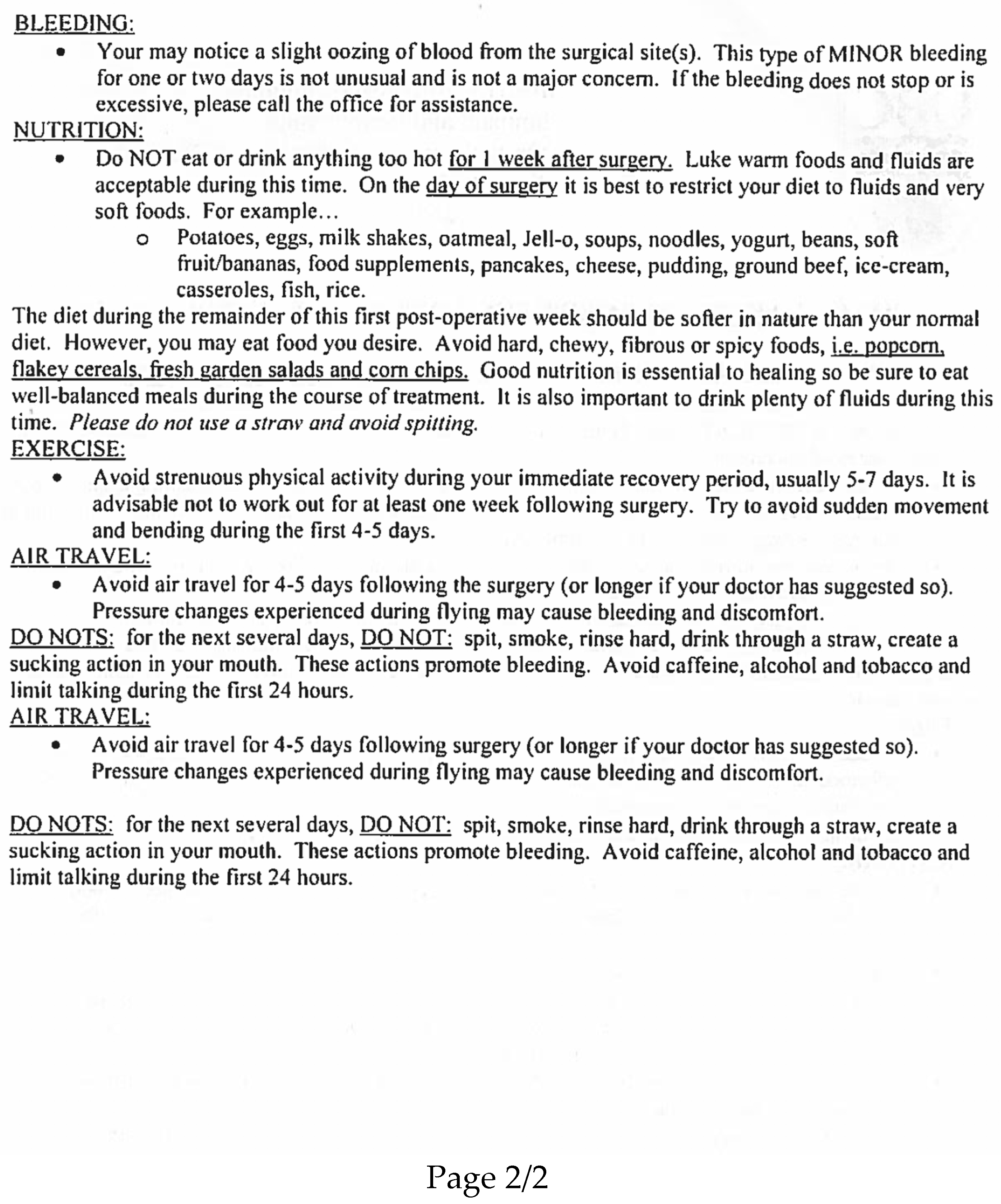
| Part 6: Surgical Aspects of the Implant Tooth Treatment What were your feelings immediately after the surgery procedure? What can be improved for the future? (e.g., if you or your friend/relative had the procedure) Please describe your recovery from the implant surgery. Do you feel you received enough information about the recovery process? Was the recovery process better or worse than expected? What was the worst part of your implant experience? Did you have any complications during the surgery or healing period? Did you have other issues such as pain or distress during the healing period? How long did the implant take? How long do you expect your implant to last? Do teeth or implants last longer? What is peri-implantitis? Can implants get infected? Are teeth or implants more resistant to infections around the bone and gums? |
| This study is part of the research project at the Faculty of Dentistry. Results of the study will be written up for publication in a scholarly journal. |
| Purpose of our study: You have been invited to participate in this study at the Faculty of Dentistry to explore your perceptions and experiences with a single dental implant in the front of the mouth. What will happen? We will take a dental impression of your upper teeth in addition to two clinical pictures of your teeth. We will also ask you questions about comfort and satisfaction with your implant tooth. If you agree, we will use audio recorders to help us document your opinions, and we will give you an opportunity to read and modify the word transcript of the interview. The visit to the clinic and interview will require up to two hours of your time. Risks and benefits to you: The interview will ask you to think about the comfort and satisfaction of your mouth and implant tooth during usual daily activities. By participating, you will have an opportunity to express your thoughts and feelings. However, we are not able to take a treatment role in this study, so if you need to, we would recommend that you return to your existing dentist for any follow-up. Confidentiality: Your participation and all information that you give us will be confidentially stored on two password-protected and encrypted laptop computers. These will be available only to the investigators. You will not be identified personally in any of the reports of the study and the statements will only be identified by a pseudonym (not your real name). All of the recordings and study data will be deleted ten years after publication of the project. Compensation: As an honorarium for your participation, we will pay you CAD xx.00 at the end of the interview. Contact information: If you have any concerns or complaints about your rights as a research participant and/or your experiences while participating in this study, contact the Research Participant Complaint Line in the Office of Research Ethics: e-mail [email protected] or call toll free x-xxx-xxx-xxxx. Consent: Your participation in this study is entirely voluntary. You can choose not to answer any question and to withdraw from the study at any time without consequences to your dental care at UBC or elsewhere. You have received all the information you requested about the study and you know who you can contact if you have questions. |
| I acknowledge my receipt of a copy of this consent form, and I consent to participate in this study. _________________________ _______________________ ________________ Print Participant’s Name Participant’s Signature Date _________________________ _______________________ ________________ Investigator’s Name Investigator’s Signature Date |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afrashtehfar, K.I.; Igarashi, K.; Bryant, S.R. Canadian Dental Patients with a Single-Unit Implant-Supported Restoration in the Aesthetic Region of the Mouth: Qualitative and Quantitative Patient-Reported Outcome Measures (PROMs). Data 2021, 6, 90. https://0-doi-org.brum.beds.ac.uk/10.3390/data6080090
Afrashtehfar KI, Igarashi K, Bryant SR. Canadian Dental Patients with a Single-Unit Implant-Supported Restoration in the Aesthetic Region of the Mouth: Qualitative and Quantitative Patient-Reported Outcome Measures (PROMs). Data. 2021; 6(8):90. https://0-doi-org.brum.beds.ac.uk/10.3390/data6080090
Chicago/Turabian StyleAfrashtehfar, Kelvin I., Kensuke Igarashi, and S. Ross Bryant. 2021. "Canadian Dental Patients with a Single-Unit Implant-Supported Restoration in the Aesthetic Region of the Mouth: Qualitative and Quantitative Patient-Reported Outcome Measures (PROMs)" Data 6, no. 8: 90. https://0-doi-org.brum.beds.ac.uk/10.3390/data6080090