
Successful Treatment of Mucocutaneous Lupus Erythematosus in a Dog with Prednisolone, Mycophenolate Mofetil and Tacrolimus


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
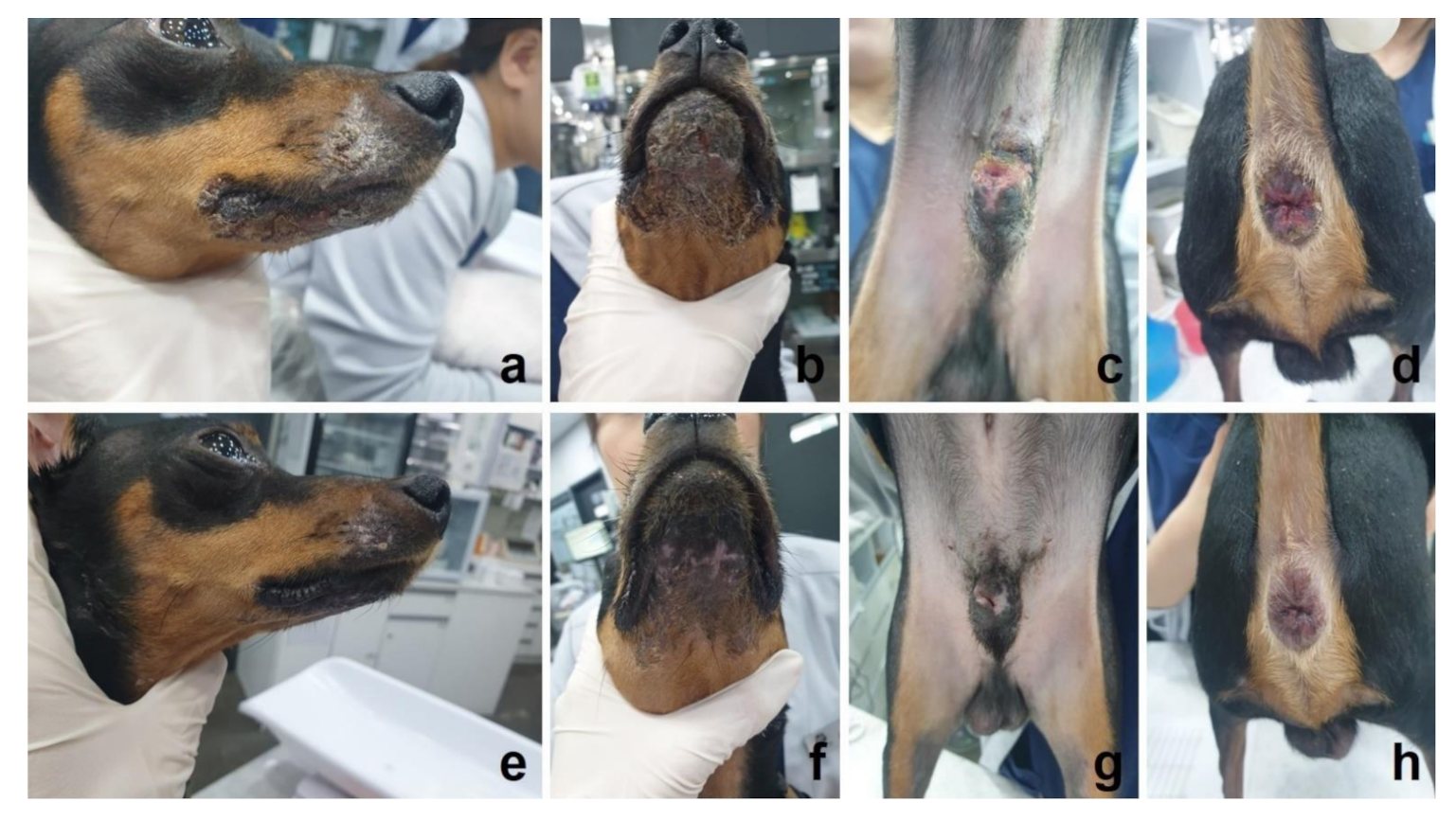
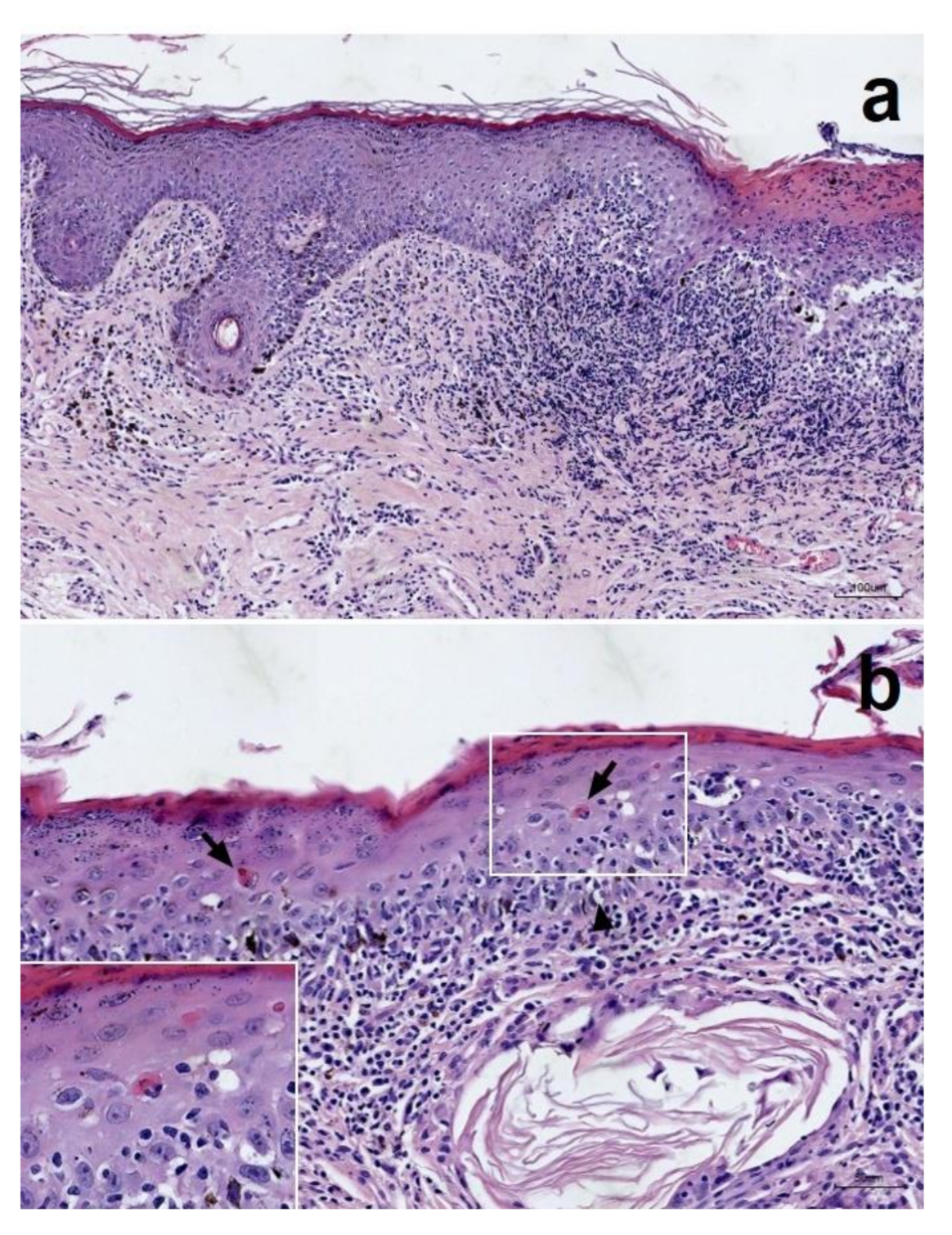
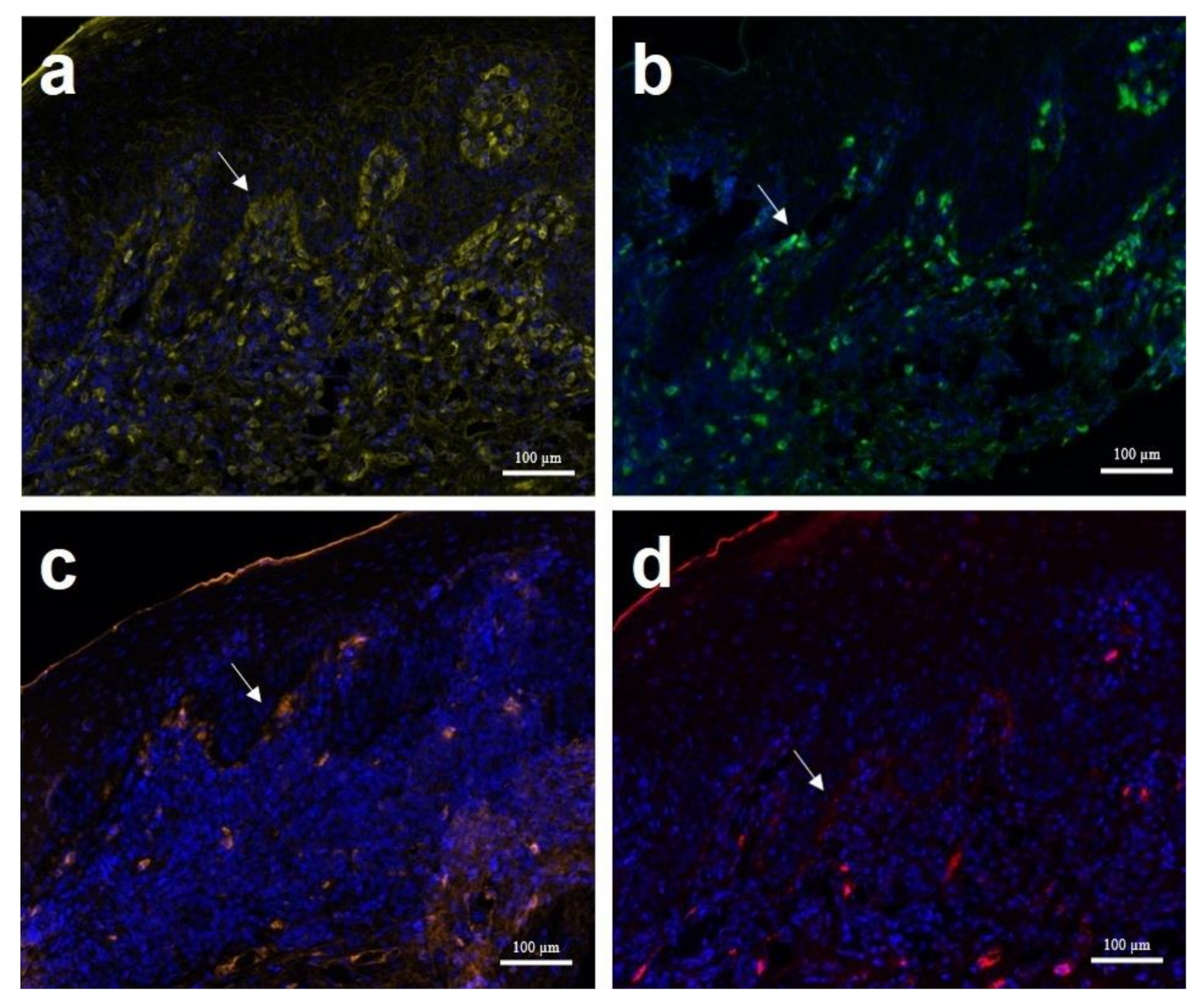
2. Case History
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burge, S.M.; Frith, P.A.; Juniper, R.P.; Wojnarowska, F. Mucosal involvement in systemic and chronic cutaneous lupus erythematosus. Br. J. Dermatol. 1989, 121, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Poirier, N. Discoid lupus erythematosus. Can. Vet. J. 1995, 36, 493. [Google Scholar] [PubMed]
- Olivry, T.; Linder, K.E.; Banovic, F. Cutaneous lupus erythematosus in dogs: A comprehensive review. BMC Vet. Res. 2018, 14, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivry, T.; Rossi, M.A.; Banovic, F.; Linder, K.E. Mucocutaneous lupus erythematosus in dogs (21 cases). Vet. Dermatol. 2015, 26, 256. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, A.L.; May, E.R.; Frank, L.A. Use of mycophenolate mofetil to treat immune-mediated skin disease in 14 dogs—A retrospective evaluation. Vet. Dermatol. 2017, 28, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrigno, A.; Hoover, K.; Blubaugh, A.; Rissi, D.; Banovic, F. Treatment of exfoliative cutaneous lupus erythematosus in a German Shorthaired Pointer dog with mycophenolate mofetil. Vet. Dermatol. 2019, 30, 350. [Google Scholar] [CrossRef] [PubMed]
- Ginel, P.J.; Blanco, B.; Lucena, R.; Jiménez, C.R.; Peinado-Guitart, C.; Mozos, E. Steroid-sparing effect of mycophenolate mofetil in the treatment of a subepidermal blistering autoimmune disease in a dog. J. S. Afr. Vet. Assoc. 2010, 81, 253–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.; Smith, J.R.; Creevy, K.E. Treatment of canine idiopathic immune-mediated haemolytic anaemia with mycophenolate mofetil and glucocorticoids: 30 cases (2007–2011). J. Small Anim. Pract. 2013, 54, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Griffies, J.D.; Mendelsohn, C.L.; Rosenkrantz, W.S.; Muse, R.; Boord, M.J.; Griffin, C.E. Topical 0.1% tacrolimus for the treatment of discoid lupus erythematosus and pemphigus erythematosus in dogs. J. Am. Anim. Hosp. Assoc. 2004, 40, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Lehner, G.M.; Linek, M. A case of vesicular cutaneous lupus erythematosus in a Border collie successfully treated with topical tacrolimus and nicotinamide–tetracycline. Vet. Dermatol. 2013, 24, 639. [Google Scholar] [CrossRef] [PubMed]
- Olivry, T.; Dunston, S.M.; Schachter, M.; Xu, L.; Nguyen, N.; Marinkovich, M.P.; Chan, L.S. A spontaneous canine model of mucous membrane (cicatricial) pemphigoid, an autoimmune blistering disease affecting mucosae and mucocutaneous junctions. J. Autoimmun. 2001, 16, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Schrauwen, E.; Junius, G.; Swinnen, C.; Maenhout, T. Dyschezia in dogs with discrete erosive anal disease and histological lesions suggestive of mucocutaneous lupus erythematosus. Vet. Rec. 2004, 154, 752–754. [Google Scholar] [CrossRef] [PubMed]
- Adolph, E.R.; Scott, D.W.; Miller, W.H.; Erb, H.N. Efficacy of tetracycline and niacinamide for the treatment of cutaneous lupus erythematosus in 17 dogs (1997–2011). Jpn. J. Vet. Dermatol. 2014, 20, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Balazs, V. Caso clínico: Lupus eritematoso mucocutáneo en un perro. Rev. Hosp. Vet. 2017, 9, 6–11. [Google Scholar]
- Mauldin, E.A.; Morris, D.O.; Brown, D.C.; Casal, M.L. Exfoliative cutaneous lupus erythematosus in German Shorthaired Pointer dogs: Disease development, progression and evaluation of three immunomodulatory drugs (ciclosporin, hydroxychloroquine, and adalimumab) in a controlled environment. Vet. Dermatol. 2010, 21, 373–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banovic, F.; Olivry, T.; Linder, K.E. Ciclosporin therapy for canine generalized discoid lupus erythematosus refractory to doxycycline and niacinamide. Vet. Dermatol. 2014, 25, 483. [Google Scholar] [CrossRef] [PubMed]
- Banovic, F.; Robson, D.; Linek, M.; Olivry, T. Therapeutic effectiveness of calcineurin inhibitors in canine vesicular cutaneous lupus erythematosus. Vet. Dermatol. 2017, 28, 493. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.C.; Wang, W.T.; Yan, L.N.; Li, B.; Wen, T.F.; Yang, J.Y.; Xu, M.Q.; Zhao, J.C.; Wei, Y.G. Effect of low-dose tacrolimus with mycophenolate mofetil on renal function following liver transplantation. World J. Gastroenterol. 2014, 20, 11356–11362. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.A.; Miller, L.W.; Russell, S.D.; Ewald, G.A.; Zucker, M.J.; Goldberg, L.R.; Eisen, H.J.; Salm, K.; Tolzman, D.; Gao, J.; et al. Tacrolimus with mycophenolate mofetil (MMF) or sirolimus vs. cyclosporine with MMF in cardiac transplant patients: 1-year report. Am. J. Transplant. 2006, 6, 1377–1386. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hyun, J.-E.; Kang, Y.-H.; Hwang, C.-Y. Successful Treatment of Mucocutaneous Lupus Erythematosus in a Dog with Prednisolone, Mycophenolate Mofetil and Tacrolimus. Vet. Sci. 2021, 8, 72. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050072
Hyun J-E, Kang Y-H, Hwang C-Y. Successful Treatment of Mucocutaneous Lupus Erythematosus in a Dog with Prednisolone, Mycophenolate Mofetil and Tacrolimus. Veterinary Sciences. 2021; 8(5):72. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050072
Chicago/Turabian StyleHyun, Jae-Eun, Yeong-Hun Kang, and Cheol-Yong Hwang. 2021. "Successful Treatment of Mucocutaneous Lupus Erythematosus in a Dog with Prednisolone, Mycophenolate Mofetil and Tacrolimus" Veterinary Sciences 8, no. 5: 72. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci8050072