Risk Factors for Severe and Fatal Heat-Related Illness in UK Dogs—A VetCompass Study

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection and Management
2.2. Geographical Distribution of Cases
2.3. Ambient Conditions
2.4. Risk Factor Analysis
3. Results
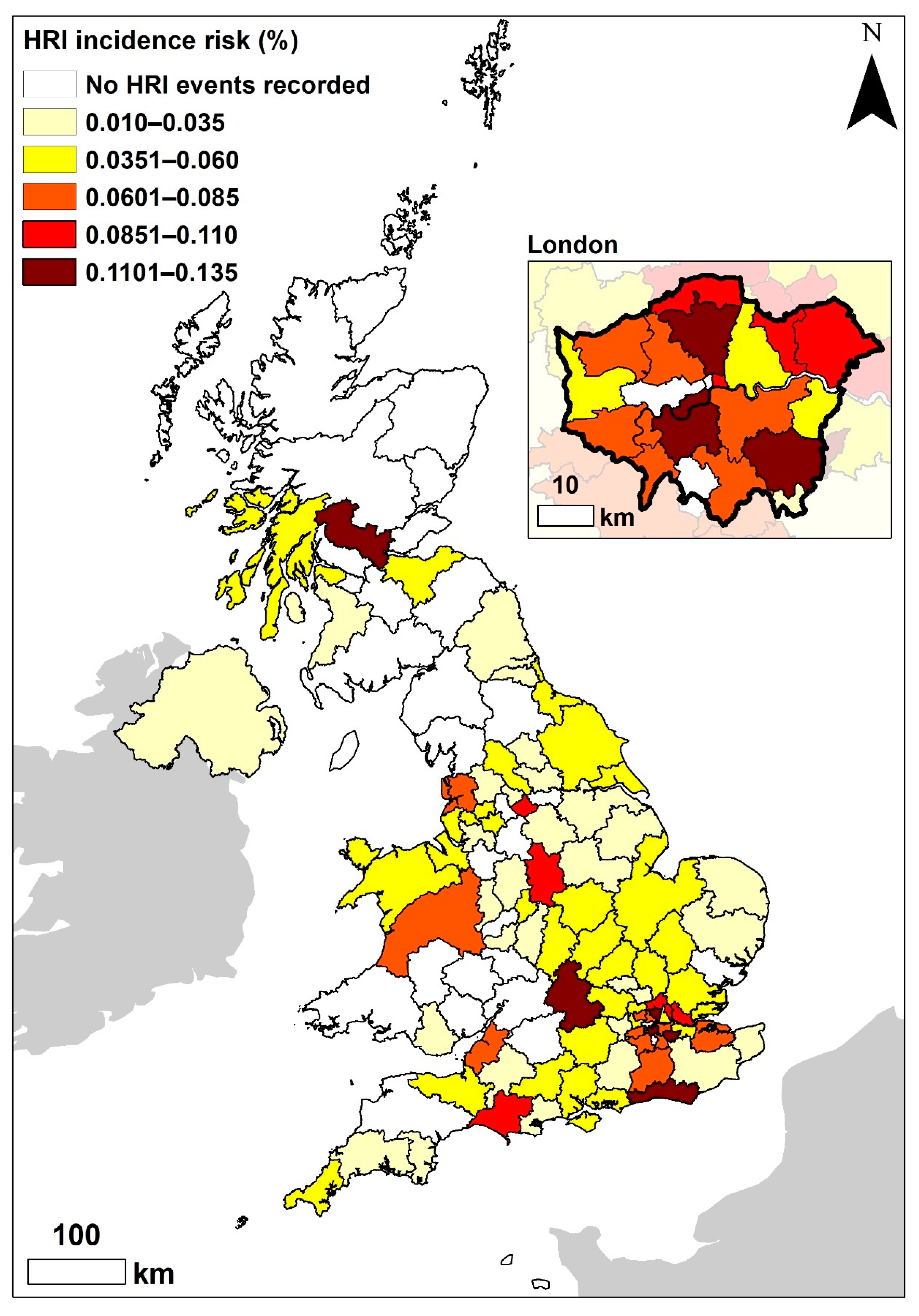
3.1. Geographical Distribution of HRI Events
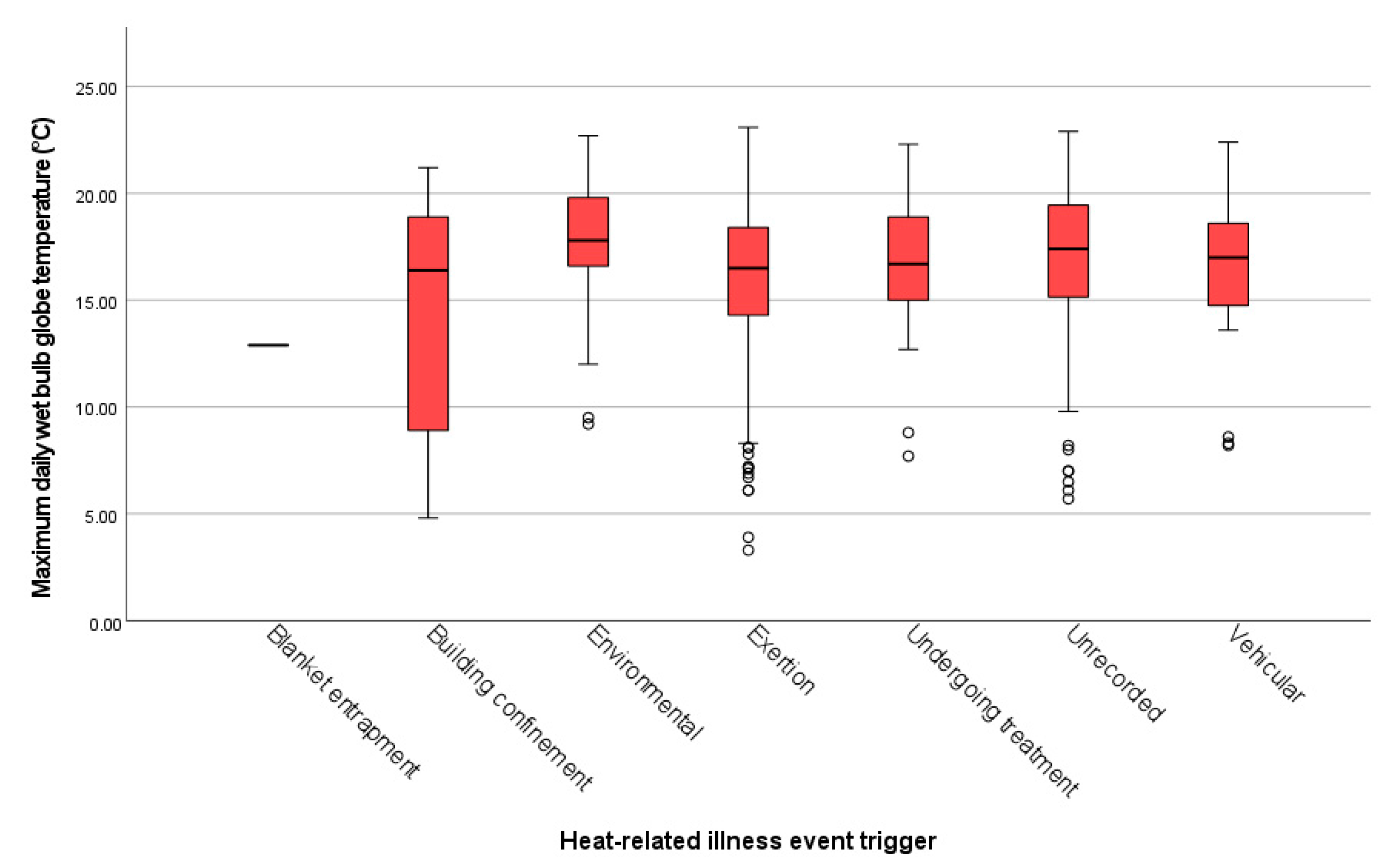
3.2. Ambient Temperature
3.3. Risk Factor Analysis for Severe HRI
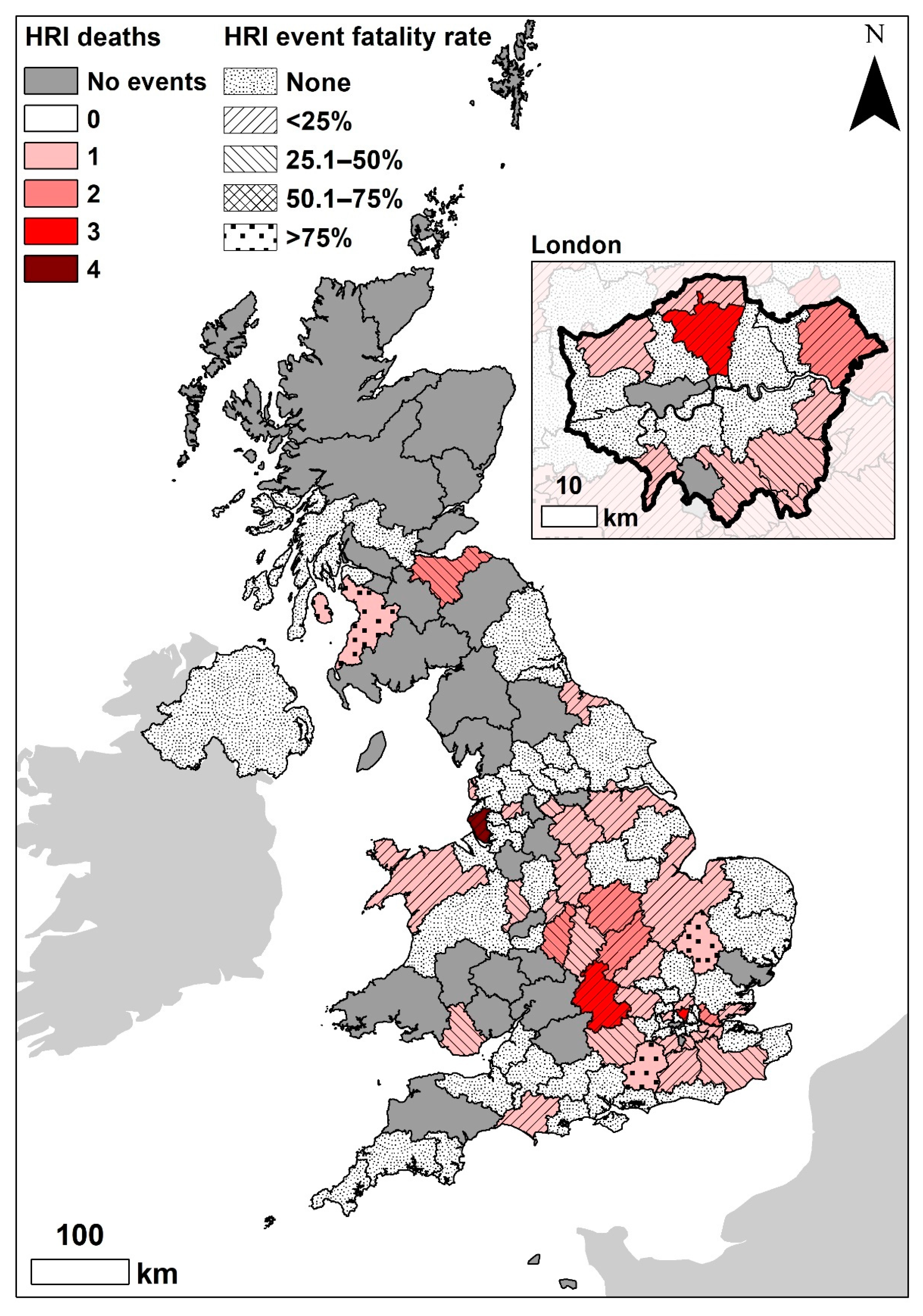
3.4. Risk Factor Analysis for Fatal HRI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fischer, E.M.; Sippel, S.; Knutti, R. Increasing probability of record-shattering climate extremes. Nat. Clim. Chang. 2021, 11, 689–695. [Google Scholar] [CrossRef]
- Ebi, K.L.; Vanos, J.; Baldwin, J.W.; Bell, J.E.; Hondula, D.M.; Errett, N.A.; Hayes, K.; Reid, C.E.; Saha, S.; Spector, J.; et al. Extreme Weather and Climate Change: Population Health and Health System Implications. Annu. Rev. Public Health 2020, 42, 293–315. [Google Scholar] [CrossRef] [PubMed]
- Protopopova, A.; Ly, L.H.; Eagan, B.H.; Brown, K.M. Climate Change and Companion Animals: Identifying Links and Opportunities for Mitigation and Adaptation Strategies. Integr. Comp. Biol. 2021, 61, 166–181. [Google Scholar] [CrossRef] [PubMed]
- Krouzecky, C.; Emmett, L.; Klaps, A.; Aden, J.; Bunina, A.; Stetina, B.U. And in the middle of my chaos there was you?—Dog companionship and its impact on the assessment of stressful situations. Int. J. Environ. Res. Public Health 2019, 16, 3664. [Google Scholar] [CrossRef] [Green Version]
- Hall, E.J.; Carter, A.J.; Farnworth, M.J. Exploring Owner Perceptions of the Impacts of Seasonal Weather Variations on Canine Activity and Potential Consequences for Human–Canine Relationships. Animals 2021, 11, 3302. [Google Scholar] [CrossRef]
- Hall, E.J.; Carter, A.J.; O’Neill, D.G. Dogs Don’t Die Just in Hot Cars—Exertional Heat-Related Illness (Heatstroke) Is a Greater Threat to UK Dogs. Animals 2020, 10, 1324. [Google Scholar] [CrossRef]
- Bouchama, A.; Knochel, J.P. Heat Stroke. N. Engl. J. Med. 2002, 346, 1978–1988. [Google Scholar] [CrossRef]
- Bruchim, Y.; Horowitz, M.; Aroch, I. Pathophysiology of heatstroke in dogs—Revisited. Temperature 2017, 4, 356–370. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Fujita, M.; Oda, Y.; Todani, M.; Hifumi, T.; Kondo, Y.; Shimazaki, J.; Shiraishi, S.; Hayashida, K.; Yokobori, S.; et al. Evaluation of a Novel Classification of Heat-Related Illnesses: A Multicentre Observational Study (Heat Stroke STUDY 2012). Int. J. Environ. Res. Public Health 2018, 15, 1962. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, T.; Todani, M.; Oda, Y.; Kaneko, T.; Kaneda, K.; Fujita, M.; Miyauchi, T.; Tsuruta, R. Predictive Factors for Hospitalization of Patients with Heat Illness in Yamaguchi, Japan. Int. J. Environ. Res. Public Health 2015, 12, 11770–11780. [Google Scholar] [CrossRef] [Green Version]
- Hall, E.J.; Carter, A.J.; Bradbury, J.; Barfield, D.; O’Neill, D.G. Proposing the VetCompass clinical grading tool for heat-related illness in dogs. Sci. Rep. 2021, 11, 6828. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, Y.; Rosenthal, T.; Sohar, E. Experimental Heatstroke a model in dogs. Arch. Intern. Med. 1973, 131, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Bynum, G.; Patton, J.; Bowers, W.; Leav, I.; Wolfe, D.; Hamlet, M.; Marsili, M. An anesthetized dog heatstroke model. J. Appl. Physiol. 1977, 43, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Hemmelgarn, C.; Gannon, K. Heatstroke: Thermoregulation, pathophysiology, and predisposing factors. Compend. Contin. Educ. Vet. 2013, 35, E4. [Google Scholar]
- Met Office UK Regional Climates. Available online: https://www.metoffice.gov.uk/research/climate/maps-and-data/regional-climates/index (accessed on 22 August 2021).
- Goldberg, M.B.; Langman, V.A.; Richard Taylor, C. Panting in dogs: Paths of air flow in response to heat and exercise. Respir. Physiol. 1981, 43, 327–338. [Google Scholar] [CrossRef]
- Budd, G.M. Wet-bulb globe temperature (WBGT)—Its history and its limitations. J. Sci. Med. Sport 2008, 11, 20–32. [Google Scholar] [CrossRef]
- Sherwood, S.C.; Huber, M. An adaptability limit to climate change due to heat stress. Proc. Natl. Acad. Sci. USA 2010, 107, 9552–9555. [Google Scholar] [CrossRef] [Green Version]
- Raymond, C.; Matthews, T.; Horton, R.M. The emergence of heat and humidity too severe for human tolerance. Sci. Adv. 2020, 6, eaaw1838. [Google Scholar] [CrossRef]
- Schroter, R.C.; Marlin, D.J. An index of the environmental thermal load imposed on exercising horses and riders by hot weather conditions. Equine Vet. J. 2010, 27, 16–22. [Google Scholar] [CrossRef]
- Marlin, D.; Misheff, M.; Whitehead, P. Optimising Performance in a Challenging Climate. In Proceedings of the FEI Sports Forum, Lausanne, Switzerland, 26–27 March 2018; Fédération Équestre Internationale: Lausanne, Switzerland, 2018. [Google Scholar]
- Gogolski, S.M.; O’Brien, C.; Lagutchik, M.S. Retrospective analysis of patient and environmental factors in heat-induced injury events in 103 military working dogs. J. Am. Vet. Med. Assoc. 2020, 256, 792–799. [Google Scholar] [CrossRef]
- Davis, M.S.; Cummings, S.L.; Payton, M.E. Effect of brachycephaly and body condition score on respiratory thermoregulation of healthy dogs. J. Am. Vet. Med. Assoc. 2017, 251, 1160–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, E.J.; Carter, A.J.; O’Neill, D.G. Incidence and risk factors for heat-related illness (heatstroke) in UK dogs under primary veterinary care in 2016. Sci. Rep. 2020, 10, 9128. [Google Scholar] [CrossRef] [PubMed]
- Bruchim, Y.; Klement, E.; Saragusty, J.; Finkeilstein, E.; Kass, P.; Aroch, I. Heat Stroke in Dogs: A Retrospective Study of 54 Cases (1999–2004) and Analysis of Risk Factors for Death. J. Vet. Intern. Med. 2006, 20, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Drobatz, K.J.; Macintire, D.K. Heat-induced illness in dogs: 42 cases (1976–1993). J. Am. Vet. Med. Assoc. 1996, 209, 1894–1899. [Google Scholar]
- Hall, E.J.; Radford, A.D.; Carter, A.J. Surveillance of heat-related illness in small animals presenting to veterinary practices in the UK between 2013–2018. Open Vet. J. 2022, 12, 5–16. [Google Scholar] [CrossRef]
- Flournoy, S.; Macintire, D.; Wohl, J. Heatstroke in Dogs: Clinical Signs, Treatment, Prognosis, and Prevention. Compend. Contin. Educ. Vet. 2003, 25, 422–431. [Google Scholar]
- Ausvet Epitools—Calculate Confidence Limits for a Sample Proportion. Available online: https://epitools.ausvet.com.au/ciproportion?page=CIProportion&SampleSize=1000&Positive=75&Conf=0.95&method=3&Digits=2 (accessed on 15 November 2019).
- Office for National Statistics. National Statistics Postcode Lookup (February 2019). Available online: https://geoportal.statistics.gov.uk/datasets/4f71f3e9806d4ff895996f832eb7aacf/about (accessed on 13 December 2021).
- MedCalc Software Ltd. Odds Ratio Calculator. Available online: https://www.medcalc.org/calc/odds_ratio.php (accessed on 10 January 2022).
- Met Office. Met Office MIDAS Open: UK Land Surface Stations Data (1853-Current). Available online: https://catalogue.ceda.ac.uk/uuid/dbd451271eb04662beade68da43546e1 (accessed on 27 July 2021).
- Dohoo, I.R.; Martin, S.W.; Stryhn, H.; Stryhn, H. Veterinary Epidemiologic Research, 2nd ed.; VER, Inc.: Québec, QC, Canada, 2009; ISBN 0919013600. [Google Scholar]
- Segev, G.; Aroch, I.; Savoray, M.; Kass, P.H.; Bruchim, Y. A novel severity scoring system for dogs with heatstroke. J. Vet. Emerg. Crit. Care 2015, 25, 240–247. [Google Scholar] [CrossRef]
- Fawcett, A.; Barrs, V.; Awad, M.; Child, G.; Brunel, L.; Mooney, E.; Martinez-Taboada, F.; McDonald, B.; McGreevy, P. Consequences and Management of Canine Brachycephaly in Veterinary Practice: Perspectives from Australian Veterinarians and Veterinary Specialists. Animals 2018, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Balmain, B.N.; Sabapathy, S.; Louis, M.; Morris, N.R. Aging and Thermoregulatory Control: The Clinical Implications of Exercising under Heat Stress in Older Individuals. Biomed Res. Int. 2018, 2018, 8306154. [Google Scholar] [CrossRef]
- O’Neill, D.G.; Church, D.B.; McGreevy, P.D.; Thomson, P.C.; Brodbelt, D.C. Longevity and mortality of owned dogs in England. Vet. J. 2013, 198, 638–643. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.J.; Chapman, L.; Thornes, J.E.; Baker, C.J. Including the urban heat island in spatial heat health risk assessment strategies: A case study for Birmingham, UK. Int. J. Health Geogr. 2011, 10, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Met Office. Southern England: Climate. Available online: https://www.metoffice.gov.uk/binaries/content/assets/metofficegovuk/pdf/weather/learn-about/uk-past-events/regional-climates/southern-england_-climate---met-office.pdf (accessed on 9 September 2019).
- Macintyre, H.L.; Heaviside, C.; Taylor, J.; Picetti, R.; Symonds, P.; Cai, X.M.; Vardoulakis, S. Assessing urban population vulnerability and environmental risks across an urban area during heatwaves—Implications for health protection. Sci. Total Environ. 2018, 610–611, 678–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shih, H.Y.; Paterson, M.B.A.; Phillips, C.J.C. Socioeconomic Influences on Reports of Canine Welfare Concerns to the Royal Society for the Prevention of Cruelty to Animals (RSPCA) in Queensland, Australia. Animals 2019, 9, 711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department for Transport Statistics. Table NTS9902: Household Car Ownership by Region and Rural Urban Classification: England. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1017101/nts9902.ods (accessed on 29 December 2021).
- Grundstein, A.; Meentemeyer, V.; Dowd, J. Maximum vehicle cabin temperatures under different meteorological conditions. Int. J. Biometeorol. 2009, 53, 255–261. [Google Scholar] [CrossRef]
- Carter, A.J.; Hall, E.J.; Connolly, S.L.; Russell, Z.F.; Mitchell, K. Drugs, dogs, and driving: The potential for year-round thermal stress in UK vehicles. Open Vet. J. 2020, 10, 216–225. [Google Scholar] [CrossRef]
- Carter, A.J.; Hall, E.J. Investigating factors affecting the body temperature of dogs competing in cross country (canicross) races in the UK. J. Therm. Biol. 2018, 72, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Nazar, K.; Greenleaf, J.E.; Pohoska, E.; Turlejska, E.; Kaciuba-Uscilko, H.; Kozlowski, S. Exercise performance, core temperature, and metabolism after prolonged restricted activity and retraining in dogs. Aviat. Space. Environ. Med. 1992, 63, 684–688. [Google Scholar] [CrossRef] [Green Version]
- Ferasin, L.; Marcora, S. Reliability of an incremental exercise test to evaluate acute blood lactate, heart rate and body temperature responses in Labrador retrievers. J. Comp. Physiol. B 2009, 179, 839–845. [Google Scholar] [CrossRef]
- Duggal, G. Add your voice to the Dogs Die in Hot Cars campaign. Vet. Rec. 2018, 182, 522–523. [Google Scholar] [CrossRef]
- BVA. Heatwave Sparks Dogs in Hot Cars Calls as Reports Hit Three Year High. Available online: https://www.bva.co.uk/news-campaigns-and-policy/newsroom/news-releases/heatwave-sparks-dogs-in-hot-cars-calls-as-reports-hit-three-year-high/ (accessed on 14 July 2019).
- Shih, H.Y.; Paterson, M.B.A.; Phillips, C.J.C. A Retrospective Analysis of Complaints to RSPCA Queensland, Australia, about Dog Welfare. Animals 2019, 9, 282. [Google Scholar] [CrossRef] [Green Version]
- Moon, K.E.; Wang, S.; Bryant, K.; Gohlke, J.M. Environmental Heat Exposure Among Pet Dogs in Rural and Urban Settings in the Southern United States. Front. Vet. Sci. 2021, 8, 742926. [Google Scholar] [CrossRef] [PubMed]
- Vanos, J.K.; Middel, A.; Mckercher, G.R.; Kuras, E.R.; Ruddell, B.L. Hot playgrounds and children’s health: A multiscale analysis of surface temperatures in Arizona, USA. Landsc. Urban Plan. 2016, 146, 29–42. [Google Scholar] [CrossRef] [Green Version]
- Jim, C.Y. Solar–terrestrial radiant-energy regimes and temperature anomalies of natural and artificial turfs. Appl. Energy 2016, 173, 520–534. [Google Scholar] [CrossRef]
- Basu, R.; Samet, J.M. Relation between Elevated Ambient Temperature and Mortality: A Review of the Epidemiologic Evidence. Epidemiol. Rev. 2002, 24, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Grundstein, A.; Duzinski, S.; Null, J. Impact of dangerous microclimate conditions within an enclosed vehicle on pediatric thermoregulation. Theor. Appl. Climatol. 2017, 127, 103–110. [Google Scholar] [CrossRef]
- Lewis, A.M. Heatstroke in Older Adults. Am. J. Nurs. 2007, 107, 52–56. [Google Scholar] [CrossRef]
- NHS. NHS’ Top Nurse Urges Public to Enjoy Sun Safely This Weekend. Available online: https://www.england.nhs.uk/2019/06/nhs-top-nurse-urges-public-to-enjoy-sun-safely-this-weekend/ (accessed on 31 October 2020).
- Hajat, S.; Vardoulakis, S.; Heaviside, C.; Eggen, B. Climate change effects on human health: Projections of temperature-related mortality for the UK during the 2020s, 2050s and 2080s. J. Epidemiol. Community Health 2014, 68, 641–648. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Potential Risk Factor for HRI | Variable Definition |
|---|---|
| Breed type | Categorical variable including all named breed types (including both Kennel Club recognised purebred and non-Kennel Club recognised purebred) and designer hybrid types with contrived names (e.g., Cockapoo, Labradoodle, Lurcher) with ≥5 HRI cases and/or ≥5000 dogs in the overall study population. All remaining dogs were assigned to grouped categories of “other purebred”, “other designer cross” or “non-designer crossbred”. |
| Skull shape | Purebred dogs were categorised by skull shape into three groups, “brachycephalic”, “mesocephalic” and “dolichocephalic”. Crossbred dogs including a brachycephalic breed were classified as “brachycephalic cross” and all other dogs listed as crossbred or unrecorded breed were classified as “skull shape unrecorded”. |
| Adult bodyweight | Adult bodyweight was defined as the mean of all bodyweight (kg) values recorded for each dog after reaching 18 months old. Bodyweight (kg) was then categorised into seven groups (<10, 10 to <20, 20 to <30, 30 to <40, 40 to <50, ≥50), dogs under 18 months or with no recorded adult bodyweight were classified as “unrecorded”. |
| Bodyweight relative to breed/sex mean | Categorical variable grouping dogs with a mean adult bodyweight “equal or above” or “below” the typical (mean) adult bodyweight for their breed and sex (calculated using the overall VetCompass study population). An “unrecorded” variable included all dogs with no adult bodyweight or labelled as crossbred. |
| Age | The age of the dog at the HRI event. Age (years) was categorised into eight groups (<2, 2 to <4, 4 to <6, 6 to <8, 8 to <10, 10 to <12, ≥12) with “unrecorded” for any dogs with no date of birth recorded in the EPR. |
| Period | HRI Cases (n) | HRI Events (n) | HRI Events with No Recorded Trigger (n) | HRI Events with a Recorded Trigger (n) |
|---|---|---|---|---|
| 2016 only | 390 | 395 | 122 | 273 |
| 2016–2018 | 839 | 856 | 264 | 592 |
| NUTS UK Region | Population (n = 905,543) | Case Number (n = 390) | 2016 HRI Incidence (%) | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| North West | 108,005 | 47 | 0.044 | Reference | ||
| London | 87,343 | 72 | 0.082 | 1.90 | 1.31–2.74 | <0.001 |
| South East | 100,034 | 54 | 0.054 | 1.24 | 0.84–1.83 | 0.279 |
| East Midlands | 75,984 | 33 | 0.043 | 1.00 | 0.64–1.56 | 0.994 |
| East of England | 99,576 | 43 | 0.043 | 0.99 | 0.66–1.50 | 0.973 |
| South West | 56,116 | 22 | 0.039 | 0.90 | 0.54–1.50 | 0.686 |
| West Midlands | 74,370 | 26 | 0.035 | 0.80 | 0.50–1.30 | 0.371 |
| Yorkshire | 101,014 | 32 | 0.032 | 0.73 | 0.46–1.14 | 0.167 |
| North East | 49,576 | 14 | 0.028 | 0.65 | 0.36–1.18 | 0.156 |
| Scotland | 36,162 | 9 | 0.025 | 0.57 | 0.28–1.17 | 0.125 |
| Wales | 32,978 | 7 | 0.021 | 0.49 | 0.22–1.08 | 0.076 |
| Northern Ireland | 8718 | 1 | 0.012 | 0.26 | 0.04–1.91 | 0.187 |
| Unrecorded | 74,082 | 30 | 0.041 | 0.93 | 0.59–1.47 | 0.758 |
| Region | HRI Events with a Recorded Trigger (n = 592) | Inciting Heat-Related Illness Event Trigger | |||
|---|---|---|---|---|---|
| Exertion No. (%) | Environmental No. (%) | Vehicular No. (%) | Building No. (%) | ||
| Whole of UK | 592 | 420 (70.95) | 84 (14.19) | 37 (6.25) | 18 (3.04) |
| London | 92 | 63 (68.48) | 13 (14.13) | 1 (1.09) * | 7 (7.61) * |
| East of England | 77 | 52 (67.53) | 14 (18.18) | 8 (10.39) | 1 (1.30) |
| South East | 75 | 62 (82.67) * | 6 (8.00) | 5 (6.67) | 2 (2.67) |
| North West | 67 | 47 (70.15) | 9 (13.43) | 5 (7.46) | 1 (1.49) |
| Yorkshire and The Humber | 65 | 47 (72.31) | 10 (15.38) | 3 (4.62) | 1 (1.54) |
| East Midlands | 50 | 34 (68.00) | 7 (14.00) | 3 (6.00) | 2 (4.00) |
| Unrecorded | 40 | 29 (72.50) | 8 (20.00) | 1 (2.50) | 0 (0.00) |
| West Midlands | 35 | 26 (74.29) | 3 (8.57) | 2 (5.71) | 1 (2.86) |
| South West | 33 | 20 (60.61) | 5 (15.15) | 4 (12.12) | 2 (6.06) |
| Scotland | 23 | 16 (69.57) | 3 (13.04) | 2 (8.70) | 1 (4.35) |
| North East | 19 | 13 (68.42) | 6 (31.58) * | 0 (0.00) | 0 (0.00) |
| Wales | 14 | 9 (64.29) | 0 (0.00) | 3 (21.43) * | 0 (0.00) |
| Northern Ireland | 2 | 2 (100) | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| Variable | Category | n (794) | Severe Cases (%) | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | 0.008 | |||||
| <2 | 129 | 11 (8.53) | Reference | |||
| 2 to <4 | 207 | 26 (12.56) | 2.04 | 0.94–4.44 | 0.072 | |
| 4 to <6 | 132 | 22 (16.67) | 3.12 | 1.37–7.08 | 0.007 | |
| 6 to <8 | 108 | 14 (12.96) | 2.53 | 1.04–6.13 | 0.041 | |
| 8 to <10 | 70 | 9 (12.86) | 2.57 | 0.95–6.96 | 0.064 | |
| 10 to <12 | 61 | 7 (11.48) | 1.77 | 0.61–5.11 | 0.291 | |
| 12+ | 83 | 22 (26.51) | 5.89 | 2.51–13.82 | <0.001 | |
| Unrecorded | 4 | 0 (0.00) | ||||
| Bodyweight (kg) | <0.001 | |||||
| <10 | 141 | 8 (5.67) | Reference | |||
| 10 to <20 | 210 | 26 (12.38) | 2.71 | 1.17–6.28 | 0.020 | |
| 20 to <30 | 141 | 19 (13.48) | 2.41 | 0.99–5.87 | 0.052 | |
| 30 to <40 | 80 | 9 (11.25) | 2.18 | 0.79–6.03 | 0.134 | |
| 40 to <50 | 24 | 4 (16.67) | 3.62 | 0.97–13.57 | 0.056 | |
| 50+ | 10 | 2 (20.00) | 4.30 | 0.76–24.4 | 0.100 | |
| Unrecorded | 188 | 43 (22.87) | 6.46 | 2.84–14.71 | <0.001 | |
| Trigger | 0.010 | |||||
| Exertion | 411 | 49 (11.92) | Reference | |||
| Blankets | 2 | 1 (50.00) | 5.64 | 0.32–99.7 | 0.238 | |
| Building | 18 | 5 (27.78) | 2.21 | 0.68–7.25 | 0.189 | |
| Environmental | 81 | 4 (4.94) | 0.37 | 0.13–1.08 | 0.069 | |
| Treatment | 27 | 3 (11.11) | 1.15 | 0.32–4.12 | 0.825 | |
| Unrecorded | 220 | 40 (18.18) | 1.69 | 1.05–2.72 | 0.031 | |
| Vehicular | 35 | 9 (25.71) | 3.03 | 1.28–7.15 | 0.011 |
| Variable | Category | n = 856 | Severe Cases (%) | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|---|
| Age (years) | <0.001 | |||||
| <2 | 139 | 7 (5.04) | Reference | |||
| 2 to <4 | 224 | 18 (8.04) | 1.47 | 0.52–4.13 | 0.469 | |
| 4 to <6 | 144 | 16 (11.11) | 1.66 | 0.56–4.90 | 0.358 | |
| 6 to <8 | 119 | 14 (11.76) | 2.98 | 0.99–8.92 | 0.051 | |
| 8 to <10 | 76 | 9 (11.84) | 3.55 | 1.03–12.22 | 0.044 | |
| 10 to <12 | 65 | 11 (16.92) | 7.29 | 2.15–24.74 | 0.001 | |
| 12+ | 84 | 23 (27.38) | 8.87 | 2.87–27.41 | <0.001 | |
| Unrecorded | 5 | 0 (0.00) | ||||
| Skull shape | 0.008 | |||||
| Mesocephalic | 377 | 37 (9.81) | Reference | |||
| Dolichocephalic | 66 | 9 (13.64) | 1.06 | 0.39–2.90 | 0.908 | |
| Brachycephalic cross | 6 | 0 (0.00) | ||||
| Brachycephalic | 287 | 42 (14.63) | 3.01 | 1.60–5.67 | <0.001 | |
| Not applicable | 120 | 10 (8.33) | 0.86 | 0.35–2.15 | 0.748 | |
| VetCompass Clinical Grade | <0.001 | |||||
| Mild | 317 | 7 (2.21) | Reference | |||
| Moderate | 366 | 20 (5.46) | 2.70 | 1.11–6.55 | 0.029 | |
| Severe | 111 | 63 (56.76) | 64.92 | 27.12–155.43 | <0.001 | |
| Unclassified | 62 | 8 (12.90) | 8.05 | 2.73–23.74 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hall, E.J.; Carter, A.J.; Chico, G.; Bradbury, J.; Gentle, L.K.; Barfield, D.; O’Neill, D.G. Risk Factors for Severe and Fatal Heat-Related Illness in UK Dogs—A VetCompass Study. Vet. Sci. 2022, 9, 231. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050231
Hall EJ, Carter AJ, Chico G, Bradbury J, Gentle LK, Barfield D, O’Neill DG. Risk Factors for Severe and Fatal Heat-Related Illness in UK Dogs—A VetCompass Study. Veterinary Sciences. 2022; 9(5):231. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050231
Chicago/Turabian StyleHall, Emily J., Anne J. Carter, Guaduneth Chico, Jude Bradbury, Louise K. Gentle, Dominic Barfield, and Dan G. O’Neill. 2022. "Risk Factors for Severe and Fatal Heat-Related Illness in UK Dogs—A VetCompass Study" Veterinary Sciences 9, no. 5: 231. https://0-doi-org.brum.beds.ac.uk/10.3390/vetsci9050231