1. Introduction
Mild cognitive impairment (MCI) is often conceptualized as being a continuum, between typical age-related cognitive changes and the more moderate to severe deficits characteristic of Alzheimer’s disease (AD) and related dementia. The cognitive presentation and progression of patients with MCI is highly heterogeneous. Although some individuals with MCI ultimately progress to AD or related dementia, many maintain their clinical status or improve and revert to normal healthy aging. The original diagnostic criteria outlined by Petersen et al. [
1] emphasized that individuals with MCI demonstrate “normal” performance on activities of daily living (ADLs) and instrumental activities of daily living (IADLs). However, more research has suggested that individuals with MCI may exhibit modest difficulties or impairments when performing more complex daily activities, such as managing finances and driving [
2,
3,
4,
5].
Driving is one of the most cognitively complex daily activities, requiring the integration of multiple cognitive functions (including attention, executive function, visual spatial ability, and memory) and the engagement of a spatially extensive brain network (including frontal, parietal, motor, and cerebellar regions) [
6,
7,
8,
9,
10]. Previous on-road [
11] and simulator-based studies [
12,
13,
14,
15] have reported that patients with MCI exhibit minor difficulties when driving, rather than definitive impairment, particularly with lane maintenance [
11,
15] and car following [
13].
Given the mild nature of cognitive and functional difficulties associated with MCI, it is particularly important to understand brain changes associated with MCI during complex daily activities, including driving. Identifying early functional and structural markers in the disease process continues to provide a greater understanding of the etiology and disease progression of AD [
16]. Given that changes in brain function may precede structural changes [
16], functional magnetic resonance imaging (fMRI), which measures brain activity based on fluctuations in blood oxygen levels, may provide important insights into the pathophysiology of MCI. For example, functional connectivity analyses measure temporal synchronization of fMRI signals between different brain regions, as a measure of information sharing [
17,
18,
19], with greater functional connectivity potentially indicating greater functional integration between regions.
Multiple studies have supported the utility of task-based functional connectivity in multiple neurological populations, including MCI [
19,
20,
21,
22]. Bajo et al. [
19] reported increased interhemispheric connections as well as reduced anterior-posterior functional connectivity during a memory task using magnetoencephalography. Bokde et al. [
20] observed both reduced and increased functional connectivity between the middle frontal gyrus and multiple brain regions during a face-matching task using fMRI. However, the tasks utilized in these studies were relatively simplistic and assessed single cognitive domains. Given the subtle nature of MCI, it is important to progress from this work towards research that involves more complex and multi-faceted daily tasks, such as driving, to provide more sensitive characterization of the cognitive deficits of individuals with MCI in relation to healthy individuals. The present study addresses this need by using fMRI and driving simulation to identify patterns of functional connectivity associated with MCI and MCI-related driving difficulty. The specific aims of this study were to identify: (1) aspects of driving difficulty among patients with MCI during a cognitively complex simulated car following task; (2) alterations in functional connectivity in MCI relative to cognitively healthy adults during the simulated car following task; and (3) alterations in functional connectivity associated with increased difficulty with lane maintenance among individuals with MCI.
4. Discussion
Despite the subtle nature of MCI, individuals with this neurological condition may experience modest functional difficulties or impairments when performing more complex daily activities, including driving [
2,
3,
4,
5,
11]. To our knowledge, the present work is the first to use fMRI to characterize the relationship between MCI, brain functional connectivity, and simulated driving performance. Consistent with previous research, patients with MCI had minor difficulty with lane maintenance, exhibiting increased steering variability compared to healthy controls. Neuroimaging results suggest that patients with MCI exhibited reduced functional connectivity between regions within the frontal cortex and posterior cortical areas during a cognitively complex car following task, compared to cognitively healthy drivers. Furthermore, among individuals with MCI, increased difficulty with lane maintenance (including lane deviations and steering variability) was associated with increased connectivity between the PCC and frontal brain regions, as well as reduced connectivity within the cerebellum.
The relative subtlety of differences in driving performance associated with MCI is an important finding that agrees with existing driving literature [
11,
12,
13,
14,
15]. Furthermore, previous work supports that individuals with MCI may be at risk of driving difficulty during car following tasks [
13] and across measures of lane maintenance [
11,
15].
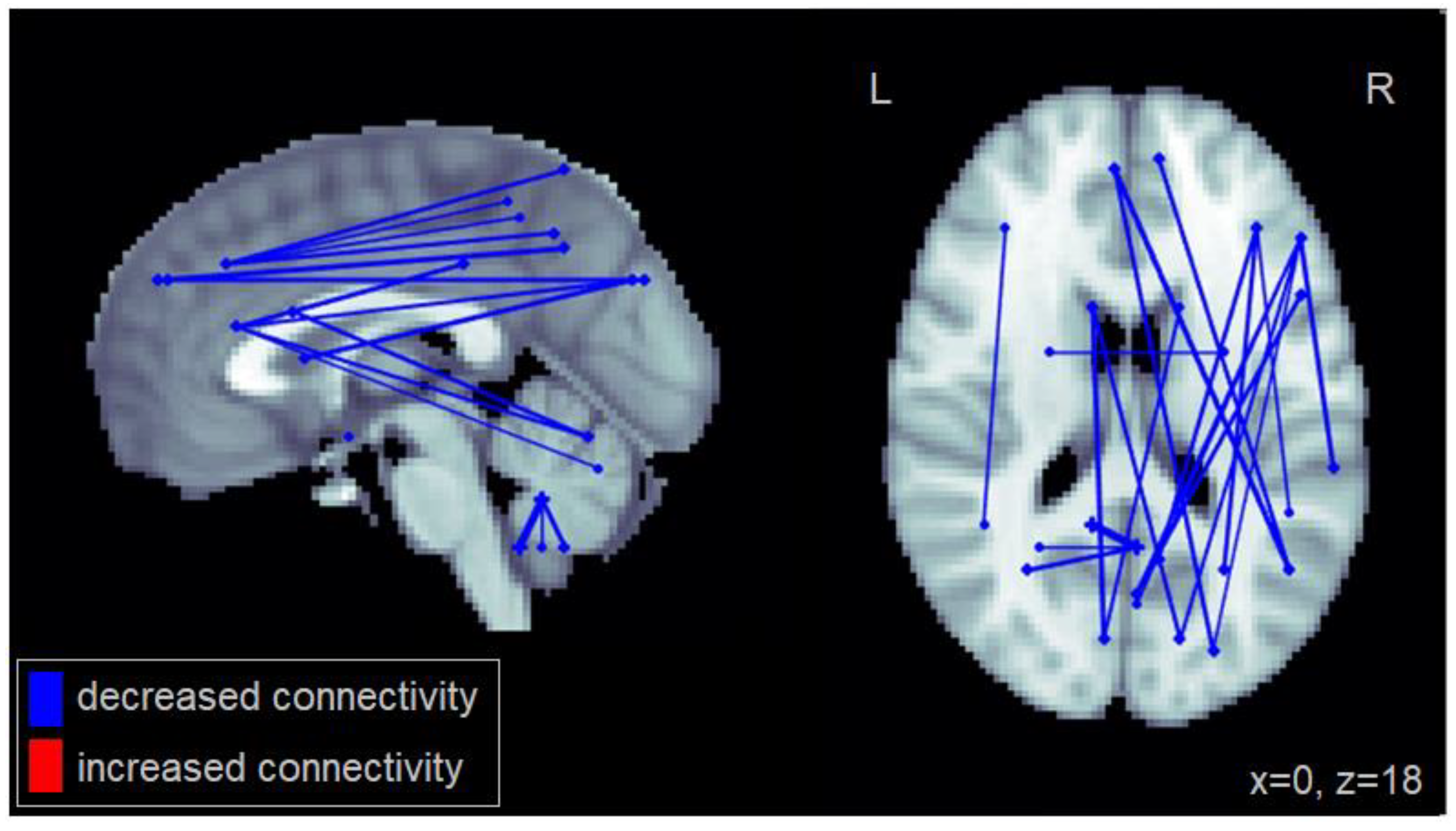
Differences in functional connectivity were also observed between individuals with MCI and cognitively healthy drivers. Patients with MCI showed reduced functional connectivity between multiple brain areas, particularly between regions within the frontal cortex and posterior regions involved in visuospatial processing. Specifically, individuals with MCI showed reduced fronto-parietal connectivity. These connections play an important role in visuospatial attention [
32] and are recruited during cognitively demanding aspects of driving [
9]. Furthermore, individuals with MCI showed reduced connectivity between regions involved in visual processing (R cuneus, R angular gyrus, R superior occipital cortex, L and R inferior and superior parietal cortex) and the medial frontal cortex as well as the right inferior frontal gyrus. The latter two areas are involved in cognitive control and performance monitoring [
33]. Reduced connectivity was also observed between the caudate, which is important for response switching and goal-directed action [
34] and the cuneus. These reductions in functional connectivity suggest that patients with MCI have reduced information sharing between regions involved in visual attention, visual processing, cognitive control, and performance monitoring. Previous fMRI and car following studies have reported the engagement of parietal, occipital, and prefrontal brain regions during successful task performance [
10,
35]. Combined with present results, this suggests that task-critical brain regions are the most affected among patients with MCI. Reduced connectivity between these regions may reflect greater task difficulty, potentially leading to minor decrement in task performance.
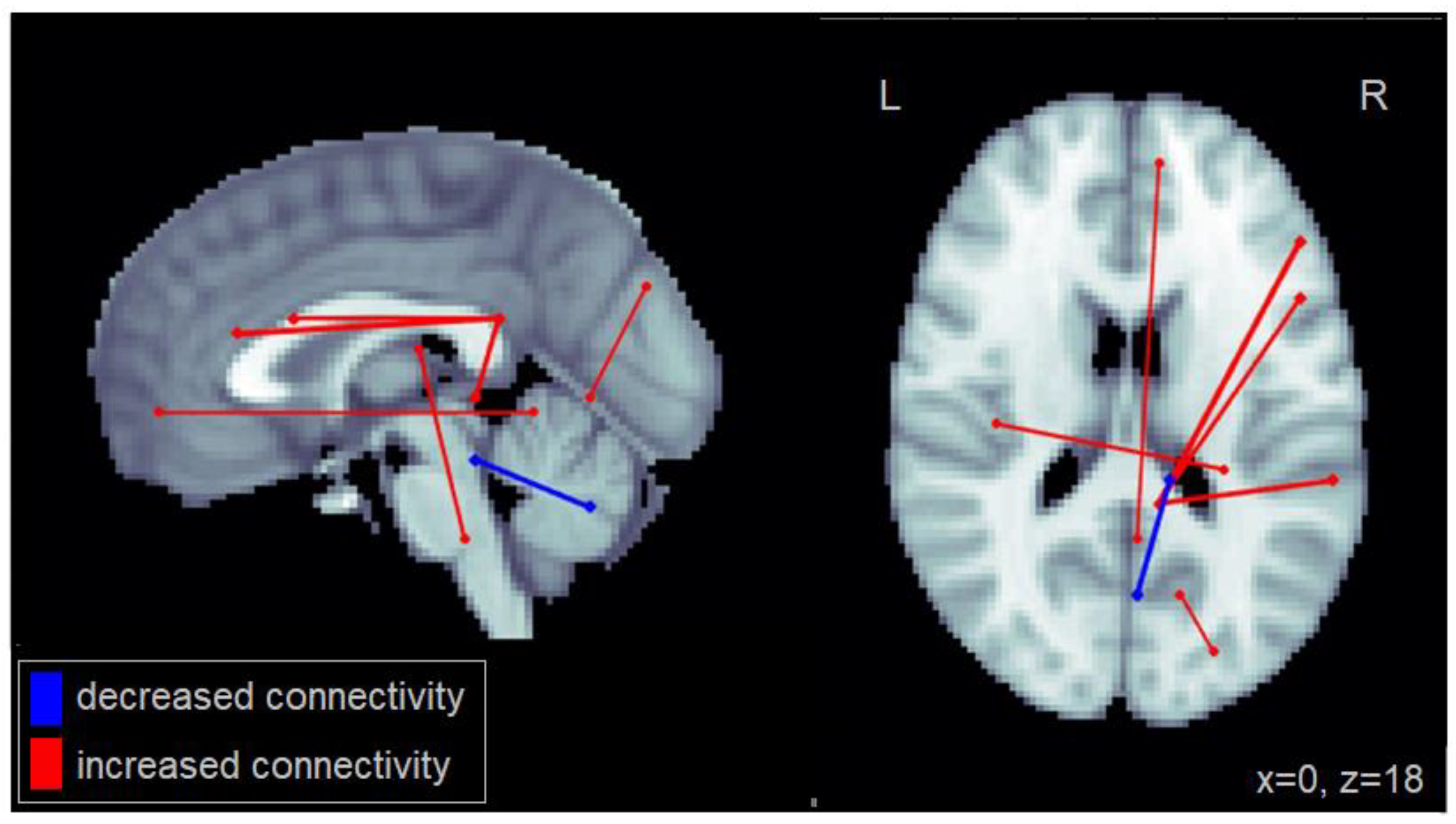
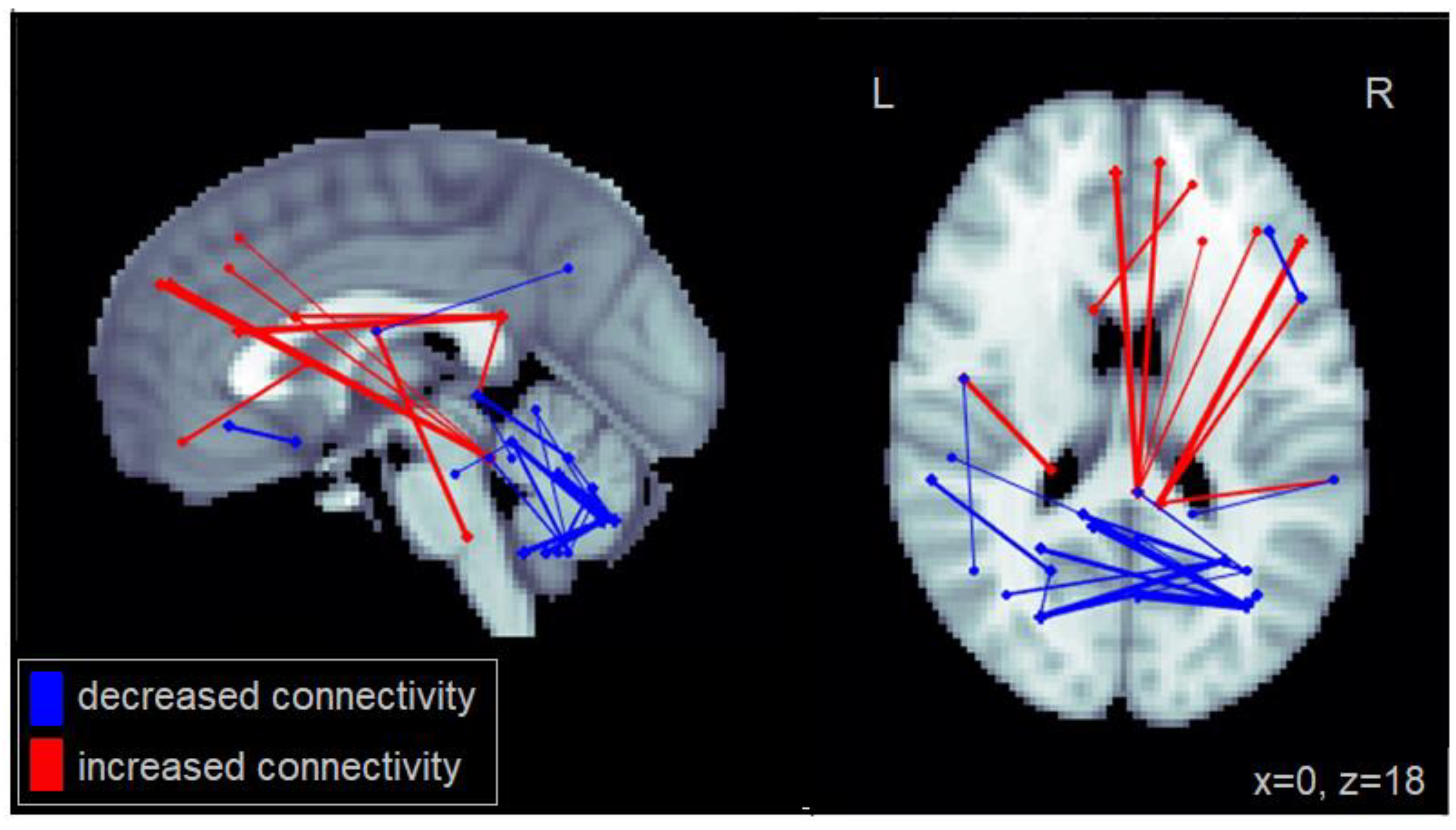
To investigate inter-individual variability in performance within the MCI group [
11,
15], functional connectivity was also investigated as a function of two measures of lane maintenance—lane deviations and steering variability (SD in steering wheel input). Individuals with MCI who committed more lane deviations showed increased connectivity between the PCC, and the inferior frontal gyrus, as well as the middle temporal cortex. Furthermore, these patients showed increased intra-cerebellar connectivity. A similar pattern was observed for steering variability, with additional reduced connectivity between the cerebellum and the middle and inferior temporal cortex.
The PCC is an important component of the DMN, a functional brain network that exhibits a pattern of increased activation and greater functional connectivity when the brain is at rest. This network, which includes the PCC, medial prefrontal cortex, and the medial, lateral, and inferior parietal cortex, tends to show deactivation during task performance [
36]. Previous research suggests that attenuation of the PCC may be important for focusing attention during task execution [
36]. However, current results showed that increased connectivity between the PCC and the inferior frontal gyrus, the middle frontal cortex, and middle temporal cortex was associated with difficulty with lane maintenance among patients with MCI. This increased connectivity with the PCC, a region of the DMN, during task performance may indicate a deficit in top-down attentional control [
36,
37,
38]. Specifically, when executing a task, the low frequency activity of the DMN can persist under certain circumstances (e.g., brain pathology) and compete with task-specific neural processes [
38]. Previous research has suggested that reduced activation in the PCC is associated with better performance on a sustained attention task [
39]. This is consistent with current results, which suggest that greater difficulty in task performance was associated with increased connectivity between the PCC and frontal as well as temporal regions. Therefore, some individuals with MCI may exhibit failed or decreased attenuation of components of the DMN (e.g., the PCC), interfering with task-relevant networks and leading to attentional lapses, and consequently increased errors in lane maintenance.
In addition to altered connectivity with the PCC, individuals with MCI who had increased difficulty with lane maintenance exhibited reduced connectivity within the cerebellum as well as reduced connectivity between the cerebellum and the middle and inferior temporal cortex. The cerebellum is a region important for motor control [
40] as well as sustained attention [
39], both of which are important functions involved in car following [
10,
35]. Furthermore, previous car following studies [
10,
35] have supported the importance of the cerebellum in successful performance on this task. Thus, altered connectivity within the cerebellum among patients with MCI may reflect reduced motor control and sustained attention, ultimately leading to greater steering difficulty (SD in steering) and increased lane deviations.
Although the current results provide important findings on functional brain changes in MCI during a complex, real-world task, there are a few methodological limitations. First, driving simulation has been noted to be being less realistic than on-road assessments and real-world driving [
41,
42]. This is particularly relevant in the fMRI-portion of the current study, which required participants to lie supine while driving. Importantly, however, previous research has supported the use of driving simulation when evaluating lane control [
43] and has shown that simulators are highly related to on-road driving performance [
44]. Given that separate cohorts were used for the behavioral and fMRI portions of the study, it was not possible to determine the association between in-scanner and out-of-scanner performance. Importantly, the same car following task and similar equipment was used for both portions of the study. Nevertheless, it will be important for future work to validate in-scanner performance by confirming that it is associated with out-of-scanner performance. Another limitation of the current study involves the patient sample. MCI is a heterogeneous condition, with different subtypes. Given the small sample size in the current study, our analysis was restricted to analyzing the MCI group as a whole—including both single domain MCI and multiple domain MCI. Thus, participants had different domains of cognitive impairment. Furthermore, the etiology of MCI may be different across participants as well as the risk of progressing to AD and related dementia. It will be important for future large-scale research studies to explore the driving profile and corresponding functional brain changes associated with various subtypes of MCI, including both single and multiple-domain amnestic and non-amnestic MCI. Furthermore, future research should include a mild probable AD subgroup as well as a longitudinal follow-up component to investigate how functional connectivity changes with disease progression. Finally, the car-following task utilized was unidimensional in space (simulated driving along a straight road) and did not involve situations that provided a range of complexity levels. Given the subtle nature of the cognitive and functional impairment associated with MCI, important additional information may be revealed by investigating both driving performance and associated functional brain changes over a range of routine to cognitively demanding aspects of driving.


{kind=link}
{kind=link}
{kind=link}


