
Influence of Social and Demographic Factors on the Montreal Cognitive Assessment (MoCA) Test in Rural Population of North-Eastern Greece

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Inclusion/Exclusion Criteria
2.2.1. Healthy Adults
2.2.2. Individuals with Mild Cognitive Impairment (MCI)
2.2.3. Individuals with Dementia
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Comparison between the Three Groups of Subjects
3.2. Montreal Cognitive Assessment (MoCA)Scoresin Healthy Adults
3.3. MoCA Scoresin Individuals with MCI
3.4. MoCA Scoresin Individuals with Dementia
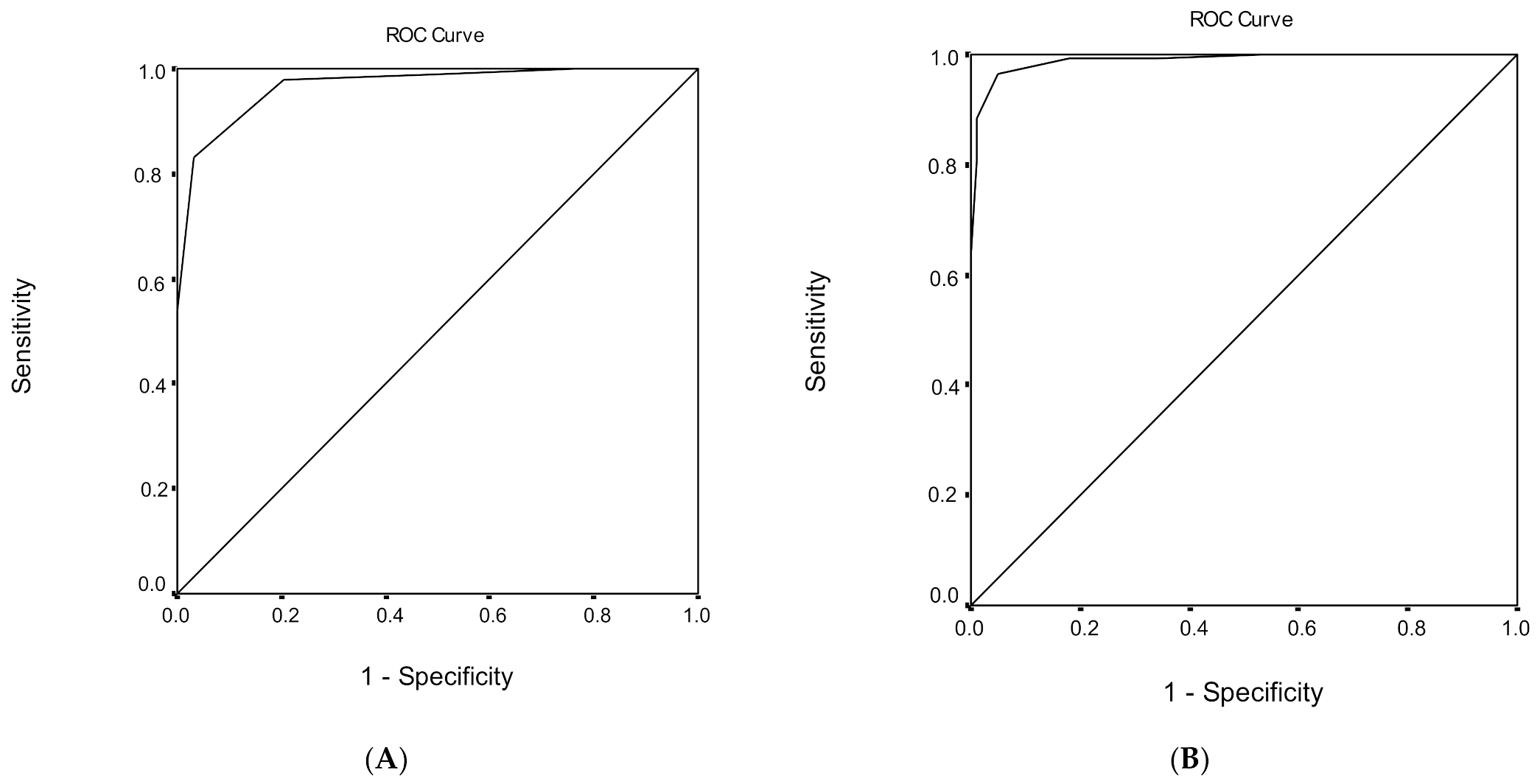
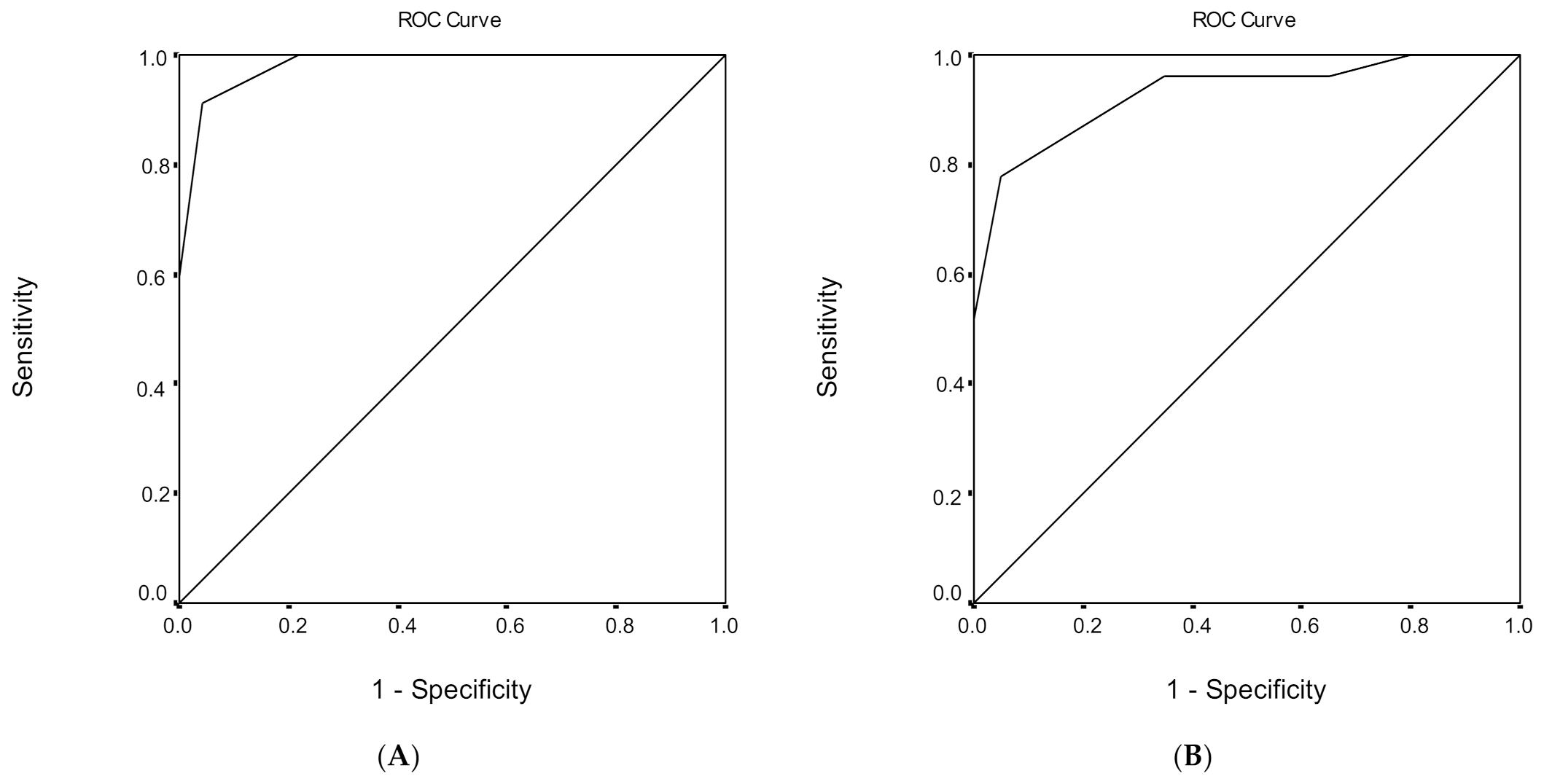
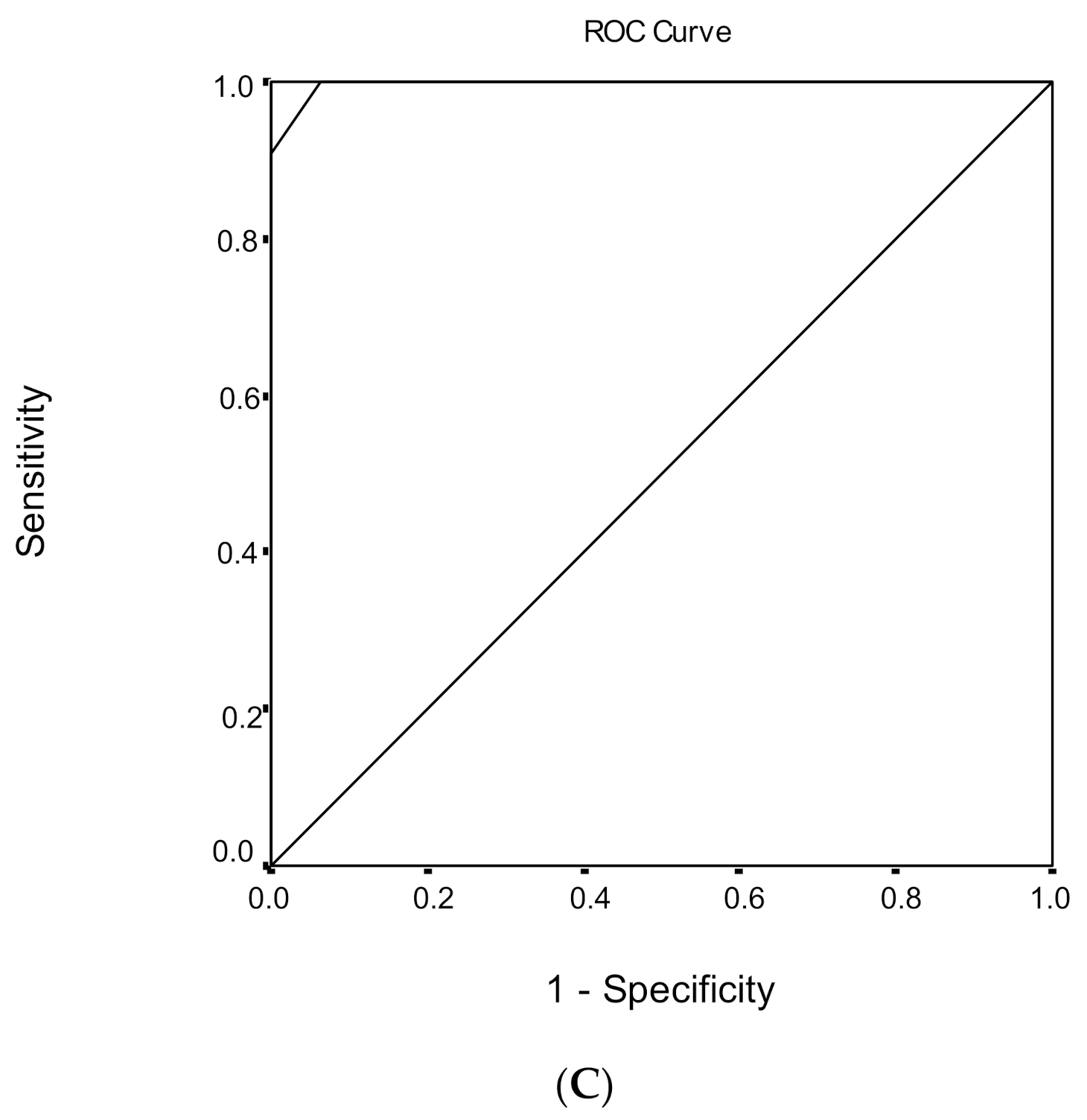
3.5. Discrimination Ability of the MoCA Score Regarding Healthy Subjects and MCI
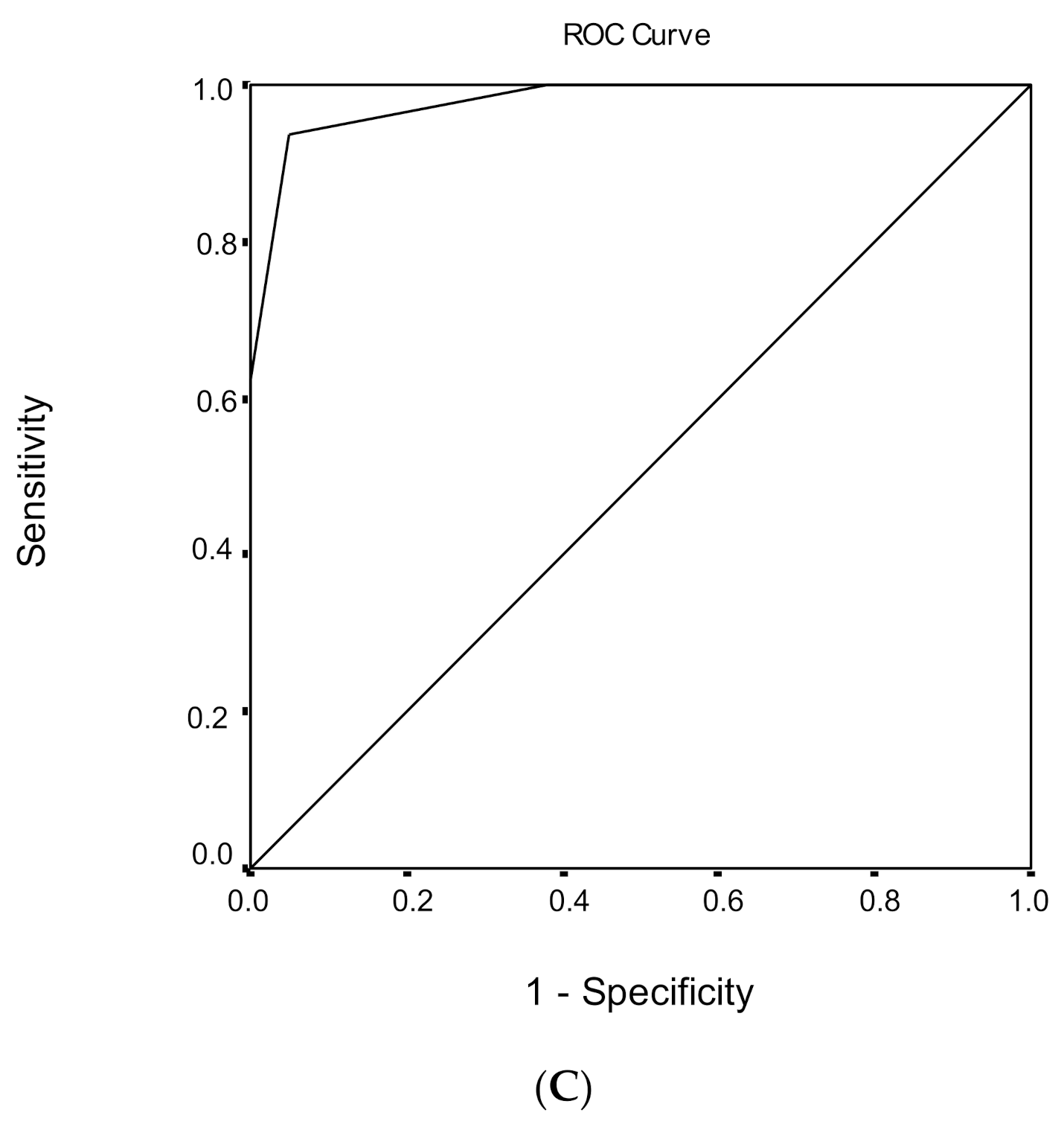
3.6. Discrimination Ability of the MoCA Score Regarding MCI and Dementia
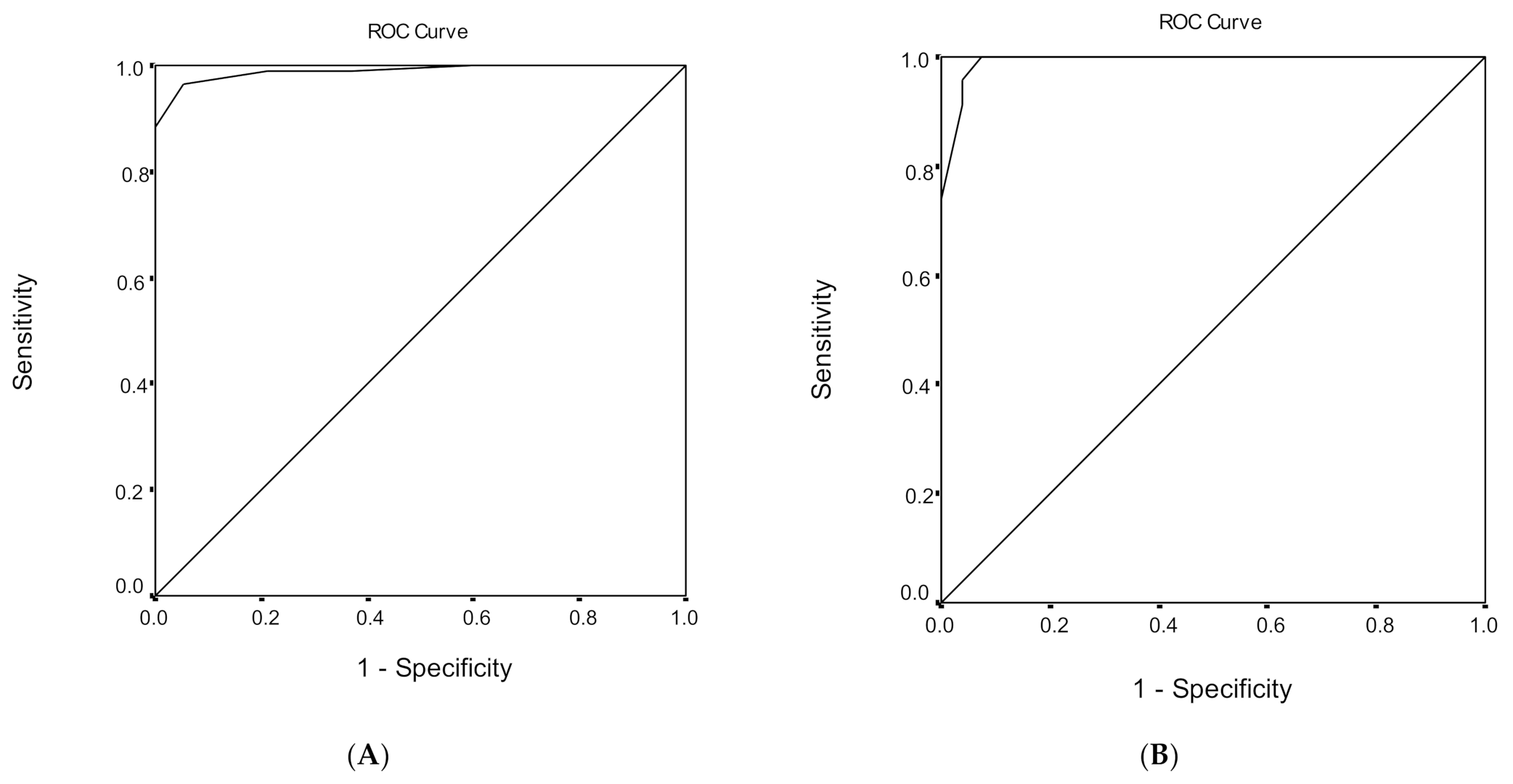
3.7. Discrimination Ability of MoCA Score Regarding Healthy Subjects and Dementia
4. Discussion
Limitations and Strengths
Author Contributions
Funding

Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prado, C.E.; Watt, S.; Treeby, M.S.; Crowe, S.F. Performance on neuropsychological assessment and progression to dementia: A meta-analysis. Psychol. Aging 2019, 34, 954–977. [Google Scholar] [CrossRef] [PubMed]
- Falk, N.; Cole, A.; Meredith, T.J. Evaluation of Suspected Dementia. Am. Fam. Physician 2018, 97, 398–405. [Google Scholar] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nilsson, F.M. Mini Mental State Examination (MMSE)—Probably one of the most cited papers in health science. Acta Psychiatr. Scand. 2007, 116, 156–157. [Google Scholar] [CrossRef]
- Trenkle, D.L.; Shankle, W.R.; Azen, S.P. Detecting Cognitive Impairment in Primary Care: Performance Assessment of Three Screening Instruments. J. Alzheimer’s Dis. 2007, 11, 323–335. [Google Scholar] [CrossRef] [Green Version]
- Xu, G.; Meyer, J.S.; Thornby, J.; Chowdhury, M.; Quach, M. Screening for mild cognitive impairment (MCI) utilizing combined mini-mental-cognitive capacity examinations for identifying dementia prodromes. Int. J. Geriatr. Psychiatry 2002, 17, 1027–1033. [Google Scholar] [CrossRef]
- Diniz, B.S.O.; Yassuda, M.S.; Nunes, P.V.; Radanovic, M.; Forlenza, O.V. Mini-mental State Examination performance in mild cognitive impairment subtypes. Int. Psychogeriatr. 2007, 19, 647–656. [Google Scholar] [CrossRef]
- Luis, C.A.; Keegan, A.P.; Mullan, M. Cross validation of the Montreal Cognitive Assessment in community dwelling older adults residing in the Southeastern US. Int. J. Geriatr. Psychiatry 2009, 24, 197–201. [Google Scholar] [CrossRef]
- Julayanont, P.; Phillips, N.; Chertkow, H.; Nasreddine, Z.S. The Montreal Cognitive Assessment (MoCA): Concept and Clinical Review. Ιn Cognitive Screening Instruments: A Practical Approach; Larner, A.J., Ed.; Springer: London, UK, 2013; pp. 111–152. [Google Scholar]
- Lee, J.-Y.; Lee, D.W.; Cho, S.-J.; Na, D.L.; Jeon, H.J.; Kim, S.-K.; Lee, Y.R.; Youn, J.-H.; Kwon, M.; Lee, J.-H.; et al. Brief Screening for Mild Cognitive Impairment in Elderly Outpatient Clinic: Validation of the Korean Version of the Montreal Cognitive Assessment. J. Geriatr. Psychiatry Neurol. 2008, 21, 104–110. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bedirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Smith, T.; Gildeh, N.; Holmes, C. The Montreal Cognitive Assessment: Validity and Utility in a Memory Clinic Setting. Can. J. Psychiatry 2007, 52, 329–332. [Google Scholar] [CrossRef]
- Konstantopoulos, K.; Vogazianos, P.; Doskas, T. Normative Data of the Montreal Cognitive Assessment in the Greek Population and Parkinsonian Dementia. Arch. Clin. Neuropsychol. 2016, 31, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Poptsi, E.; Moraitou, D.; Eleftheriou, M.; Kounti-Zafeiropoulou, F.; Papasozomenou, C.; Agogiatou, C.; Bakoglidou, E.; Batsila, G.; Liapi, D.; Markou, N.; et al. Normative Data for the Montreal Cognitive Assessment in Greek Older Adults with Subjective Cognitive Decline, Mild Cognitive Impairment and Dementia. J. Geriatr. Psychiatry Neurol. 2019, 32, 265–274. [Google Scholar] [CrossRef]
- Rahman, T.T.A.; El Gaafary, M.M. Montreal Cognitive Assessment Arabic version: Reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr. Gerontol. Int. 2009, 9, 54–61. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Suzuki, H.; Yasunaga, M.; Sugiyama, M.; Ijuin, M.; Sakuma, N.; Inagaki, H.; Iwasa, H.; Ura, C.; Yatomi, N.; et al. Brief screening tool for mild cognitive impairment in older Japanese: Validation of the Japanese version of the Montreal Cognitive Assessment. Geriatr. Gerontol. Int. 2010, 10, 225–232. [Google Scholar] [CrossRef]
- Freitas, S.; Simões, M.R.; Alves, L.; Santana, I. Montreal Cognitive Assessment (MoCA): Normative study for the Portuguese population. J. Clin. Exp. Neuropsychol. 2011, 33, 989–996. [Google Scholar] [CrossRef]
- Lu, J.; Li, D.; Li, F.; Zhou, A.; Wang, F.; Zuo, X.; Jia, X.-F.; Song, H.; Jia, J. Montreal Cognitive Assessment in Detecting Cognitive Impairment in Chinese Elderly Individuals: A Population-Based Study. J. Geriatr. Psychiatry Neurol. 2011, 24, 184–190. [Google Scholar] [CrossRef]
- Rossetti, H.C.; Lacritz, L.H.; Cullum, C.M.; Weiner, M.F. Normative data for the Montreal Cognitive Assessment (MoCA) in a population-based sample. Neurology 2011, 77, 1272–1275. [Google Scholar] [CrossRef]
- Magierska, J.; Magierski, R.; Fendler, W.; Kłoszewska, I.; Sobów, T.M. Clinical application of the Polish adaptation of the Montreal Cognitive Assessment (MoCA) test in screening for cognitive impairment. Neurol. Neurochir. Polska 2012, 46, 130–139. [Google Scholar] [CrossRef] [Green Version]
- Kenny, R.A.; Coen, R.F.; Frewen, J.; Donoghue, O.A.; Cronin, H.; Savva, G.M. Normative Values of Cognitive and Physical Function in Older Adults: Findings from The Irish Longitudinal Study on Ageing. J. Am. Geriatr. Soc. 2013, 61, S279–S290. [Google Scholar] [CrossRef]
- Narazaki, K.; Nofuji, Y.; Honda, T.; Matsuo, E.; Yonemoto, K.; Kumagai, S. Normative Data for the Montreal Cognitive Assessment in a Japanese Community-Dwelling Older Population. Neuroepidemiology 2013, 40, 23–29. [Google Scholar] [CrossRef]
- Malek-Ahmadi, M.; Powell, J.J.; Belden, C.M.; O’Connor, K.; Evans, L.; Coon, D.W.; Nieri, W. Age- and education-adjusted normative data for the Montreal Cognitive Assessment (MoCA) in older adults age 70–99. Aging Neuropsychol. Cogn. 2015, 22, 755–761. [Google Scholar] [CrossRef]
- Santangelo, G.; Siciliano, M.; Pedone, R.; Vitale, C.; Falco, F.; Bisogno, R.; Siano, P.; Barone, P.; Grossi, D.; Santangelo, F.; et al. Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol. Sci. 2014, 36, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.P.; Feng, L.; Lim, W.S.; Chong, M.S.; Lee, T.S.; Yap, K.B.; Tsoi, T.; Liew, T.M.; Gao, Q.; Collinson, S.; et al. Montreal Cognitive Assessment for Screening Mild Cognitive Impairment: Variations in Test Performance and Scores by Education in Singapore. Dement. Geriatr. Cogn. Disord. 2015, 39, 176–185. [Google Scholar] [CrossRef]
- Kopecek, M.; Stepankova, H.; Lukavsky, J.; Řípová, D.; Nikolai, T.; Bezdicek, O. Montreal cognitive assessment (MoCA): Normative data for old and very old Czech adults. Appl. Neuropsychol. Adult 2016, 24, 23–29. [Google Scholar] [CrossRef]
- Larouche, E.; Tremblay, M.-P.; Potvin, O.; Laforest, S.; Bergeron, D.; LaForce, R.; Monetta, L.; Boucher, L.; Tremblay, P.; Belleville, S.; et al. Normative Data for the Montreal Cognitive Assessment in Middle-Aged and Elderly Quebec-French People. Arch. Clin. Neuropsychol. 2016, 31, 819–826. [Google Scholar] [CrossRef] [Green Version]
- Borland, E.; Nägga, K.; Nilsson, P.M.; Minthon, L.; Nilsson, E.D.; Palmqvist, S. The Montreal Cognitive Assessment: Normative Data from a Large Swedish Population-Based Cohort. J. Alzheimer’s Dis. 2017, 59, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Thomann, A.E.; Goettel, N.; Monsch, R.J.; Berres, M.; Jahn, T.; Steiner, L.A.; Monsch, A.U. The Montreal Cognitive Assessment: Normative Data from a German-Speaking Cohort and Comparison with International Normative Samples. J. Alzheimer’s Dis. 2018, 64, 643–655. [Google Scholar] [CrossRef] [Green Version]
- Apolinario, D.; Dos Santos, M.F.; Sassaki, E.; Pegoraro, F.; Pedrini, A.V.A.; Cestari, B.; Amaral, A.H.; Mitt, M.; Müller, M.B.; Suemoto, C.K.; et al. Normative data for the Montreal Cognitive Assessment (MoCA) and the Memory Index Score (MoCA-MIS) in Brazil: Adjusting the nonlinear effects of education with fractional polynomials. Int. J. Geriatr. Psychiatry 2018, 33, 893–899. [Google Scholar] [CrossRef]
- Cesar, K.G.; Yassuda, M.S.; Porto, F.H.G.; Brucki, S.M.D.; Nitrini, R. MoCA Test: Normative and diagnostic accuracy data for seniors with heterogeneous educational levels in Brazil. Arq. Neuropsiquiatr. 2019, 77, 775–781. [Google Scholar] [CrossRef] [Green Version]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2014. [Google Scholar]
- Simpson, J.R. DSM-5 and neurocognitive disorders. J. Am. Acad. Psychiatry Law 2014, 42, 159–164. [Google Scholar] [PubMed]
- Sachdev, P.S.; Mohan, A.; Taylor, L.; Jeste, D.V. DSM-5 and Mental Disorders in Older Individuals. Harv. Rev. Psychiatry 2015, 23, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Sheikh, J.I. 9/Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Cummings, J.L.; Mega, M.; Gray, K.; Rosenberg-Thompson, S.; Carusi, D.A.; Gornbein, J. The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology 1994, 44, 2308. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Zhang, Y.X.; Feng, W. Decision tree analysis in determinants of elderly visits in poor rural areas. J. Peking Univ. Heal. Sci. 2018, 50, 450–456. [Google Scholar]
- O’Driscoll, C.; Shaikh, M. Cross-Cultural Applicability of the Montreal Cognitive Assessment (MoCA): A Systematic Review. J. Alzheimer’s Dis. 2017, 58, 789–801. [Google Scholar] [CrossRef]
- Salthouse, T.A.; Pink, J.E.; Tucker-Drob, E.M. Contextual analysis of fluid intelligence. Intelligence 2008, 36, 464–486. [Google Scholar] [CrossRef] [Green Version]
- Salthouse, T.A. Relations Between Cognitive Abilities and Measures of Executive Functioning. Neuropsychology 2005, 19, 532–545. [Google Scholar] [CrossRef]
- Salthouse, T.A. Selective review of cognitive aging. J. Int. Neuropsychol. Soc. 2010, 16, 754–760. [Google Scholar] [CrossRef]
- Nyberg, L.; Maitland, S.B.; Rönnlund, M.; Bäckman, L.; Dixon, R.A.; Wahlin, Å.; Nilsson, L.-G. Selective adult age differences in an age-invariant multifactor model of declarative memory. Psychol. Aging 2003, 18, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Bäckman, L.; Small, B.J.; Wahlin, Å.; Larsson, M. Cognitive functioning in very old age. In Handbook of Cognitive Aging; Craik, F.I.M., Salthouse, T.A., Eds.; Erlbaum: Mahwah, NJ, USA, 2000; Volume 2, pp. 499–558. [Google Scholar]
- Rönnlund, M.; Nyberg, L.; Bäckman, L.; Nilsson, L.-G. Stability, Growth, and Decline in Adult Life Span Development of Declarative Memory: Cross-Sectional and Longitudinal Data from a Population-Based Study. Psychol. Aging 2005, 20, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Hultsch, D.F.; Hertzog, C.; Small, B.J.; McDonald-Miszczak, L.; Dixon, R.A. Short-term longitudinal change in cognitive performance in later life. Psychol. Aging 1992, 7, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Bendayan, R.; Piccinin, A.M.; Hofer, S.M.; Cadar, D.; Johansson, B.; Muniz-Terrera, G. Decline in Memory, Visuospatial Ability, and Crystalized Cognitive Abilities in Older Adults: Normative Aging or Terminal Decline? J. Aging Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Burke, M.R.; Poyser, C.; Schiess, I. Age-Related Deficits in Visuospatial Memory Are due to Changes in Preparatory Set and Eye–Hand Coordinati. J. Gerontol. B 2015, 70, 682–690. [Google Scholar] [CrossRef] [Green Version]
- Mittal, S.; Verma, P.; Jain, N.; Khatter, S.; Juyal, A. Gender Based Variation in Cognitive Functions in Adolescent Subjects. Ann. Neurosci. 2012, 19, 165–168. [Google Scholar] [CrossRef] [Green Version]
- Carson, N.; Leach, L.; Murphy, K.J. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 2018, 33, 379–388. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Timmons, S.; Molloy, D.W. Screening for Mild Cognitive Impairment: Comparison of “MCI Specific” Screening Instruments. J. Alzheimer’s Dis. 2016, 51, 619–629. [Google Scholar] [CrossRef] [Green Version]
- Trzepacz, P.T.; Hochstetler, H.; Wang, S.; Walker, B.; Saykin, A.J.; for the Alzheimer’s Disease Neuroimaging Initiative. Relationship between the Montreal Cognitive Assessment and Mini-mental State Examination for assessment of mild cognitive impairment in older adults. BMC Geriatr. 2015, 15, 107. [Google Scholar] [CrossRef] [Green Version]
- Richard, E.; Schmand, B.A.; Eikelenboom, P.; Van Gool, W.A. MRI and cerebrospinal fluid biomarkers for predicting progression to Alzheimer’s disease in patients with mild cognitive impairment: A diagnostic accuracy study. BMJ Open 2013, 3, e002541. [Google Scholar] [CrossRef] [Green Version]
- Ventura, T.; De-La-Cámara, C.; Lopez-Anton, R.; Santabárbara, J.; Marcos, G.; Quintanilla, M.Á.; Campayo, A.; Lobo, E.; Roy, J.F.; Saz, P.; et al. Usefulness of 2 Questions About Age and Year of Birth in the Case-Finding of Dementia. J. Am. Med. Dir. Assoc. 2013, 14, 627.e7–627.e12. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Researchers | Language of Montreal Cognitive Assessment Test | Participant’s Range of Age (Years) | Participant Groups | Effects of Education, Age, Sex | Suggested Cut-Off Scores for the MoCA |
|---|---|---|---|---|---|
| Lee JY. et al., 2008 [10] | Korean | >65 | Normal Control (NC) Mild Cognitive Impairment (MCI) Alzheimer’s Disease (AD) | (+) education | 22/23 |
| Rahman T.T.A. and El Gaafry M. M., 2009 [15] | Arabic | 60–83 | Normal Mild Cognitive Impairment | (+) education (+) age (+) sex | They used the suggested cut-off score (26) of the original study |
| Fujiwara Y. et al., 2010 [16] | Japanese | Means 76.4, 77.3, 77.5 | Cognitive normal (NC) Mild Cognitive Impairment (MCI) Mild Alzheimer’s Disease (AD) | (−) education (−) age (−) sex | 25/26: MCI from Normal Control 25/26: AD from Normal Control |
| Freitas S. et al., 2011 [17] | Portuguese | >25 | Healthy | (+) education (+) age (−) sex | Adjusted normative values |
| Lu J. et al., 2011 [18] | Chinese | >65 | Normal Control (NC) Mild Cognitive Impairment (MCI) Dementia | (+) education (+) age (+) sex (+) urban or rural residence | 13/14: Illiterate individuals 19/20: 1–6 years of education 24/25: 7 or moreyears of education |
| Rosseti et al., 2011 [19] | English (multiethnic study) | 18–85 | Normal (general population) | (+) education (+) age | Adjusted normative values |
| Magierska J. et al., 2012 [20] | Polish | Means 76.3, 74.2, 71.4 | Cognitively Intact Controls Mild Cognitive Impairment Dementia | (+) education (+) age (−) sex | 24 (screening MCI) 19 (screening dementia) |
| Kenny R. et al., 2013 [21] | Irish | >50 | Healthy (not demented) | (+) education (+) age | Adjusted normative values |
| Narazaki K. et al.,2013 [22] | Japanese | >65 | Healthy | (+) education (+) age (−) sex | Adjusted normative values |
| Malek-Ahmadi M. et al., 2015 [23] | English | 70–99 | Healthy | (+) education (+) age | Adjusted normative values 25.03 (mean score) |
| Santangelo G. et al., 2015 [24] | Italian | 21–95 | Healthy | (+) education (+) age (−) sex | 15.5 |
| Ng TP. et al., 2015 [25] | Chinese English | Means 70.8, 69.5, 62.0 58.7 | Normal cognition Mild Cognitive Impairment | (+) education | 21/22: No education 22/23: 1–6 years of education 27/28: >6 years of education |
| Kopecek M.et al, 2016 [26] | Czech | >60 | Healthy | (+) education (+) age (−) sex | Adjusted for education and age |
| Konstantopoulos K. et al., 2016 [13] | Greek | >20 | Healthy Parkinsonian dementia | (+) education (+) age (+) sex | 21 (detecting Parkinsonian Dementia) |
| Larouche E. et al., 2016 [27] | French | 41–98 | Healthy | (+) education (+) age (+) sex | Regression-based norms |
| Borland E. et al., 2017 [28] | Swedish | 65–85 | Healthy | (+) education (+) age (+) sex | 21–25 (lower education) 24–26 (higher education) |
| Thomann A. et al., 2018 [29] | German | >65 | Healthy | (+) education (+) age (+) sex | Adjusted normative values |
| Apolinario D. et al., 2018 [30] | Brazilian | 50–90 | Healthy | (+) education (+) age (−) sex | Adjusting to education and age |
| Cesar K. et al., 2019 [31] | Brazilian | >60 | Cognitive normal Cognitive Impaired no dementia Dementia | (+) education (+) age (+) sex (except from dementia group) | 15 (distinguish cognitive normal from dementia) 19 (distinguish cognitive normal from cognitive impaired/no dementia) |
| Poptsi E. et al., 2019 [14] | Greek | >60 | Subjective Cognitive Decline (SCD) Mild Cognitive Impairment (MCI) Dementia | (+) education (−) age (−) sex | 23–26 (to distinguish adults with subjective cognitive decline from MCI) 20 (to distinguish adults with subjective cognitive decline from dementia) |
| Healthy Subjects | MCI | Dementia | p Value | |
|---|---|---|---|---|
| n | 64 | 100 | 119 | |
| Male sex | 14 (21.9) | 28 (28.0) | 49 (41.2) | 0.016 |
| Age, years | 66.73 ± 7.60 | 68.52 ± 8.62 | 72.92 ± 7.54 | <0.001 |
| Age category | <0.001 | |||
| 50–64 years | 25 (39.1) | 27 (27.0) | 16 (13.4) | |
| 65–74 years | 31 (48.4) | 51 (51.0) | 55 (46.2) | |
| ≥75 years | 8 (12.5) | 22 (22.0) | 48 (40.3) | |
| Education level | <0.001 | |||
| Low | 23 (35.9) | 57 (57.0) | 85 (71.4) | |
| Medium | 20 (31.3) | 27 (27.0) | 116 (19.3) | |
| High | 21 (32.8) | 16 (16.0) | 11 (9.2) | |
| Mini Mental State Examination score | 29.11 ± 0.69 | 27.41 ± 0.92 | 21.76 ± 3.64 | <0.001 |
| Total MOCA score | 27.58 ± 1.26 | 24.07 ± 1.57 | 16.69 ± 3.38 | <0.001 |
| Visuospatial | 4.38 ± 0.68 | 3.59 ± 0.88 | 1.77 ± 1.13 | <0.001 |
| Naming | 2.97 ± 0.18 | 2.93 ± 0.26 | 2.53 ± 0.58 | <0.001 |
| Memory | 4.97 ± 0.18 | 4.90 ± 0.33 | 3.59 ± 0.71 | <0.001 |
| Attention | 5.77 ± 0.46 | 5.20 ± 0.94 | 4.10 ± 1.55 | <0.001 |
| Language | 2.44 ± 0.61 | 1.84 ± 0.65 | 0.76 ± 0.63 | <0.001 |
| Abstraction | 1.70 ± 0.46 | 1.47 ± 0.56 | 1.11 ± 0.55 | <0.001 |
| Delayed recall | 3.89 ± 0.86 | 2.45 ± 1.42 | 0.91 ± 1.26 | <0.001 |
| Orientation | 5.97 ± 0.17 | 5.92 ± 0.27 | 4.68 ± 1.10 | <0.001 |
| Sex | Age | Education Level | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | p Value | 50–64 Years | 65–74 Years | >74 Years | p Value | Low | Medium | High | p Value | |
| MOCA (total) | 27.43 ± 1.28 | 27.62 ± 1.26 | 0.87 | 27.68 ± 1.18 | 27.48 ± 1.34 | 27.63 ± 1.30 | 0.86 | 27.65 ± 1.37 | 27.25 ± 1.41 | 27.81 ± 0.93 | 0.35 |
| Visuospatial | 4.50 ± 0.76 | 4.34 ± 0.66 | 0.06 | 4.44 ± 0.65 | 4.42 ± 0.67 | 4.00 ± 0.76 | 0.035 | 4.43 ± 0.59 | 4.35 ± 0.75 | 4.33 ± 0.73 | 0.10 |
| Naming | 3.00 ± 0.00 | 2.96 ± 0.20 | 0.77 | 3.00 ± 0.00 | 2.94 ± 0.25 | 3.00 ± 0.00 | 0.54 | 2.91 ± 0.29 | 3.00 ± 0.00 | 3.00 ± 0.00 | 0.73 |
| Memory | 5.00 ± 0.00 | 4.96 ± 0.20 | 0.52 | 5.00 ± 0.00 | 4.97 ± 0.18 | 4.88 ± 0.35 | 0.43 | 4.96 ± 0.21 | 4.95 ± 0.22 | 5.00 ± 0.00 | 0.61 |
| Attention | 5.86 ± 0.36 | 5.74 ± 0.49 | 0.23 | 5.76 ± 0.44 | 5.74 ± 0.51 | 5.88 ± 0.35 | 0.99 | 5.74 ± 0.54 | 5.75 ± 0.44 | 5.81 ± 0.40 | 0.66 |
| Language | 2.64 ± 0.50 | 2.38 ± 0.64 | 0.77 | 2.36 ± 0.57 | 2.42 ± 0.67 | 2.75 ± 0.46 | 0.13 | 2.13 ± 0.63 | 2.40 ± 0.60 | 2.81 ± 0.40 | 0.019 |
| Abstraction | 1.79 ± 0.43 | 1.68 ± 0.47 | 0.74 | 1.68 ± 0.48 | 1.74 ± 0.44 | 1.63 ± 0.52 | 0.47 | 1.48 ± 0.51 | 1.75 ± 0.44 | 1.90 ± 0.30 | 0.020 |
| Delayed recall | 3.50 ± 0.76 | 4.00 ± 0.86 | 0.016 | 4.08 ± 0.95 | 3.77 ± 0.84 | 3.75 ± 0.46 | 0.33 | 3.96 ± 0.77 | 3.65 ± 0.93 | 4.05 ± 0.86 | 0.35 |
| Orientation | 5.93 ± 0.27 | 5.98 ± 0.14 | 0.21 | 5.96 ± 0.20 | 5.97 ± 0.18 | 6.00 ± 0.00 | 0.72 | 6.00 ± 0.00 | 5.95 ± 0.22 | 5.95 ± 0.22 | 0.96 |
| Sex | Age | Education Level | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | p Value | 50–64 Years | 65–74 Years | >74 Years | p Value | Low | Medium | High | p Value | |
| MOCA (total) | 24.00 ± 1.61 | 24.10 ± 1.56 | 0.47 | 24.67 ± 1.57 | 23.98 ± 1.38 | 23.55 ± 1.79 | 0.004 | 23.86 ± 1.39 | 24.15 ± 1.88 | 24.69 ± 1.49 | 0.06 |
| Visuospatial | 3.54 ± 0.84 | 3.61 ± 0.90 | 0.43 | 4.11 ± 0.75 | 3.45 ± 0.90 | 3.27 ± 0.70 | 0.018 | 3.30 ± 0.80 | 3.78 ± 0.85 | 4.31 ± 0.70 | 0.003 |
| Naming | 2.89 ± 0.31 | 2.94 ± 0.23 | 0.95 | 2.93 ± 0.27 | 2.96 ± 0.20 | 2.86 ± 0.35 | 0.16 | 2.89 ± 0.31 | 2.96 ± 0.19 | 3.00 ± 0.00 | 0.12 |
| Memory | 4.93 ± 0.26 | 4.89 ± 0.36 | 0.26 | 4.93 ± 0.27 | 4.94 ± 0.24 | 4.77 ± 0.53 | 0.16 | 4.88 ± 0.38 | 4.93 ± 0.27 | 4.94 ± 0.25 | 0.54 |
| Attention | 5.54 ± 0.74 | 5.07 ± 0.98 | 0.026 | 5.22 ± 0.80 | 5.02 ± 1.05 | 5.59 ± 0.73 | 0.48 | 5.25 ± 0.91 | 5.04 ± 1.09 | 5.31 ± 0.79 | 0.80 |
| Language | 1.79 ± 0.79 | 1.86 ± 0.59 | 0.96 | 1.89 ± 0.70 | 1.90 ± 0.67 | 1.64 ± 0.49 | 0.18 | 1.65 ± 0.55 | 2.04 ± 0.71 | 2.19 ± 0.66 | 0.005 |
| Abstraction | 1.50 ± 0.58 | 1.46 ± 0.56 | 0.36 | 1.52 ± 0.51 | 1.55 ± 0.58 | 1.23 ± 0.53 | 0.06 | 1.32 ± 0.54 | 1.59 ± 0.57 | 1.81 ± 0.40 | 0.032 |
| Delayed recall | 2.36 ± 1.39 | 2.49 ± 1.43 | 0.72 | 2.59 ± 1.53 | 2.43 ± 1.42 | 2.32 ± 1.32 | 0.22 | 2.51 ± 1.40 | 2.48 ± 1.40 | 2.19 ± 1.56 | 0.36 |
| Orientation | 5.82 ± 0.39 | 5.96 ± 0.20 | 0.047 | 5.93 ± 0.27 | 5.94 ± 0.24 | 5.86 ± 0.35 | 0.99 | 5.93 ± 0.26 | 5.93 ± 0.27 | 5.88 ± 0.34 | 0.69 |
| Sex | Age | Education Level | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | Females | p Value | 50–64 Years | 65–74 Years | >74 Years | p Value | Low | Medium | High | p Value | |
| MOCA (total) | 16.35 ± 3.15 | 16.93 ± 3.54 | 0.44 | 16.88 ± 3.86 | 17.16 ± 3.22 | 16.08 ± 3.37 | 0.78 | 16.78 ± 3.49 | 16.48 ± 2.41 | 16.45 ± 4.41 | 0.97 |
| Visuospatial | 1.86 ± 1.27 | 1.71 ± 1.02 | 0.97 | 1.81 ± 1.38 | 1.89 ± 1.01 | 1.63 ± 1.18 | 0.49 | 1.65 ± 1.00 | 1.87 ± 1.22 | 2.55 ± 1.63 | 0.022 |
| Naming | 2.46 ± 0.54 | 2.59 ± 0.60 | 0.22 | 2.80 ± 0.41 | 2.56 ± 0.60 | 2.42 ± 0.58 | 0.038 | 2.52 ± 0.59 | 2.57 ± 0.59 | 2.55 ± 0.52 | 0.62 |
| Memory | 3.53 ± 0.71 | 3.63 ± 0.71 | 0.69 | 3.63 ± 0.89 | 3.69 ± 0.77 | 3.46 ± 0.54 | 0.61 | 3.59 ± 0.71 | 3.59 ± 0.71 | 3.55 ± 0.93 | 0.94 |
| Attention | 4.27 ± 1.47 | 3.99 ± 1.60 | 0.18 | 4.25 ± 1.34 | 4.09 ± 1.52 | 4.06 ± 1.67 | 0.64 | 4.14 ± 1.60 | 4.00 ± 1.41 | 4.00 ± 1.48 | 0.64 |
| Language | 0.84 ± 0.69 | 0.71 ± 0.59 | 0.40 | 0.75 ± 0.58 | 0.85 ± 0.65 | 0.67 ± 0.63 | 0.95 | 0.74 ± 0.62 | 0.74 ± 0.54 | 1.00 ± 0.89 | 0.35 |
| Abstraction | 1.06 ± 0.63 | 1.14 ± 0.49 | 0.23 | 1.25 ± 0.68 | 1.09 ± 0.59 | 1.08 ± 0.45 | 0.65 | 1.05 ± 0.55 | 1.26 ± 0.54 | 1.27 ± 0.47 | 0.24 |
| Delayed recall | 0.53 ± 0.98 | 1.17 ± 1.37 | 0.034 | 0.81 ± 1.22 | 0.87 ± 1.25 | 0.98 ± 1.31 | 0.80 | 1.01 ± 1.31 | 0.74 ± 1.05 | 0.45 ± 1.21 | 0.75 |
| Orientation | 4.61 ± 1.04 | 4.73 ± 1.14 | 0.10 | 5.00 ± 1.21 | 4.84 ± 1.01 | 4.40 ± 1.11 | 0.047 | 4.71 ± 1.17 | 4.65 ± 0.78 | 4.55 ± 1.13 | 0.43 |
| Education Level | AUC (95% CI) | p Value | Cut-Off | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Overall Agreement | +LR | −LR |
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy to MCI | ||||||||||
| Low | 0.982 (0.956–1.000) | <0.001 | ≤25 | 91.2 | 95.7 | 98.1 | 81.5 | 92.5 | 21.21 | 0.092 |
| Medium | 0.930 (0.858–1.000) | <0.001 | ≤25 | 77.8 | 95.0 | 95.5 | 76.0 | 85.1 | 15.56 | 0.234 |
| High | 0.979 (0.941–1.000) | <0.001 | ≤26 | 93.8 | 95.2 | 93.8 | 95.2 | 94.6 | 19.54 | 0.065 |
| Total sample | 0.968 (0.945–0.991) | <0.001 | ≤25 | 83.0 | 96.9 | 97.6 | 78.5 | 88.4 | 26.77 | 0.174 |
| MCI to Dementia | ||||||||||
| Low | 0.989 (0.976–1.000) | <0.001 | ≤21 | 96.5 | 94.7 | 96.5 | 94.7 | 95.7 | 18.21 | 0.037 |
| Medium | 0.993 (0.977–1.000) | <0.001 | ≤21 | 100.0 | 92.6 | 92.0 | 100.0 | 96.0 | 13.51 | 0 |
| High | 0.997 (0.986–1.000) | <0.001 | ≤22 | 100.0 | 93.7 | 91.7 | 100.0 | 96.3 | 15.87 | 0 |
| Total sample | 0.989 (0.979–1.000) | <0.001 | ≤21 | 96.6 | 95 | 95.8 | 96.0 | 95.9 | 19.32 | 0.036 |
| Healthy to Dementia | ||||||||||
| Low | 1.000 (1.000–1.000) | <0.001 | ≤24 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | - | 0 |
| Medium | 1.000 (1.000–1.000) | <0.001 | ≤24 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | - | 0 |
| High | 1.000 (1.000–1.000) | <0.001 | ≤24 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | - | 0 |
| Total sample | 1.000 (1.000–1.000) | <0.001 | ≤24 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | - | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsiakiri, A.; Vadikolias, K.; Tripsianis, G.; Vlotinou, P.; Serdari, A.; Terzoudi, A.; Heliopoulos, I. Influence of Social and Demographic Factors on the Montreal Cognitive Assessment (MoCA) Test in Rural Population of North-Eastern Greece. Geriatrics 2021, 6, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6020043
Tsiakiri A, Vadikolias K, Tripsianis G, Vlotinou P, Serdari A, Terzoudi A, Heliopoulos I. Influence of Social and Demographic Factors on the Montreal Cognitive Assessment (MoCA) Test in Rural Population of North-Eastern Greece. Geriatrics. 2021; 6(2):43. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6020043
Chicago/Turabian StyleTsiakiri, Anna, Konstantinos Vadikolias, Grigorios Tripsianis, Pinelopi Vlotinou, Aspasia Serdari, Aikaterini Terzoudi, and Ioannis Heliopoulos. 2021. "Influence of Social and Demographic Factors on the Montreal Cognitive Assessment (MoCA) Test in Rural Population of North-Eastern Greece" Geriatrics 6, no. 2: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6020043