
Proof of Concept of Novel Visuo-Spatial-Motor Fall Prevention Training for Old People

 ,
,
Abstract
:1. Introduction
1.1. Falling of Older People: Dual Causes
1.2. A Medical Geriaters Wake-Up Call
1.3. A Visuo-Spatial-Motor Tool for Fall Prevention
1.4. Blinks and Saccades Induce Perception Errors
1.5. Evaluation of Balance, Motor Skills, and Cordination
2. Materials and Methods
2.1. Subjects
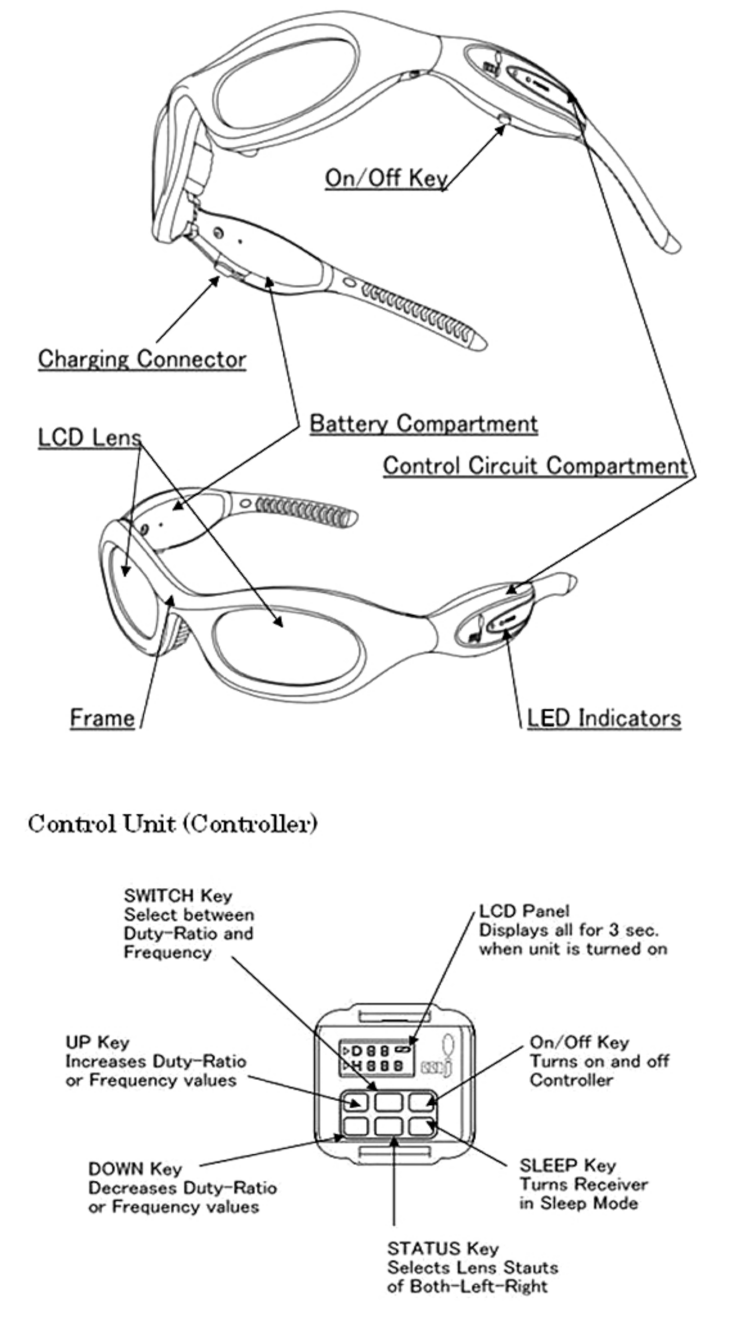
2.2. Training and Test Instruments
2.3. Data Collection
2.4. Research Development
2.4.1. The Eyes as a Tool for Maintaining Balance
2.4.2. Peripheral Sight
2.5. The Interventions
2.5.1. Physical Exercises, the Motor Program
2.5.2. Visual Plus Physical Exercises: Visuo-Spatial-Motor Intervention
2.6. Statistical Analysis
2.6.1. Testing Independence of the Three Intervention Groups
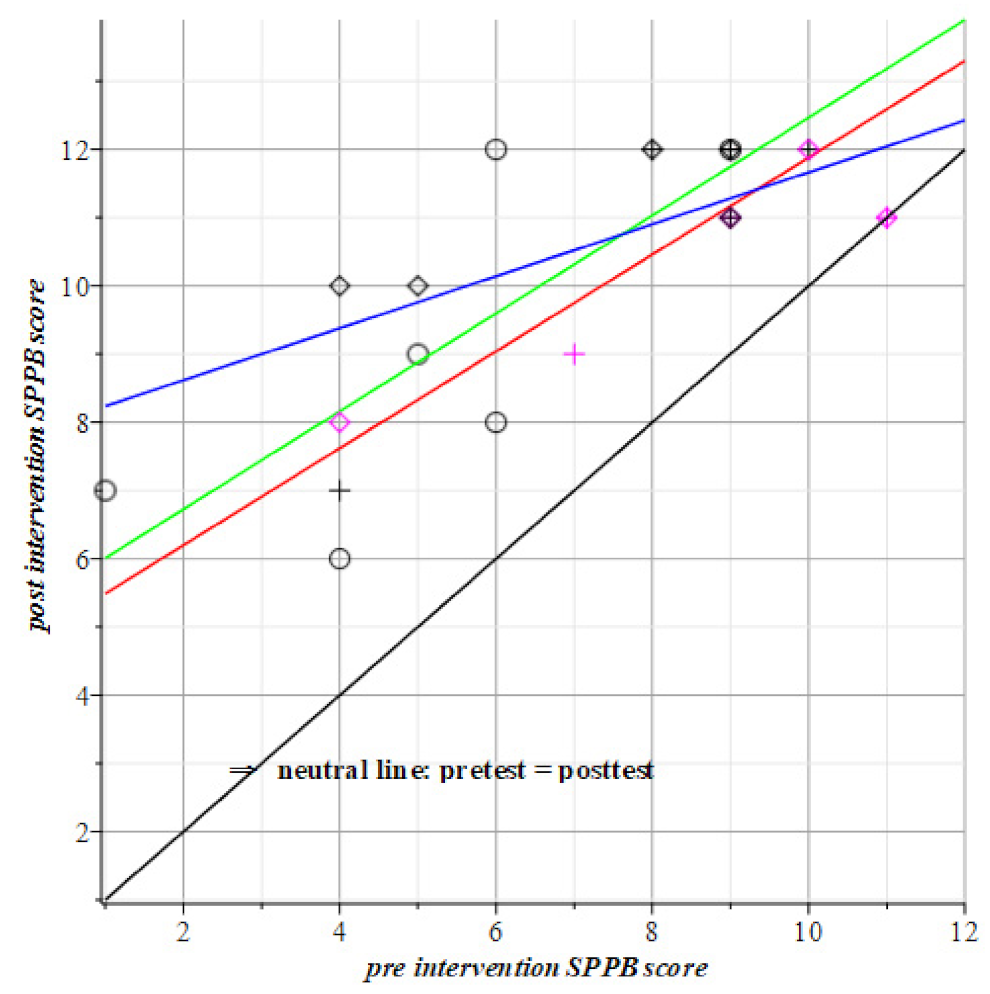
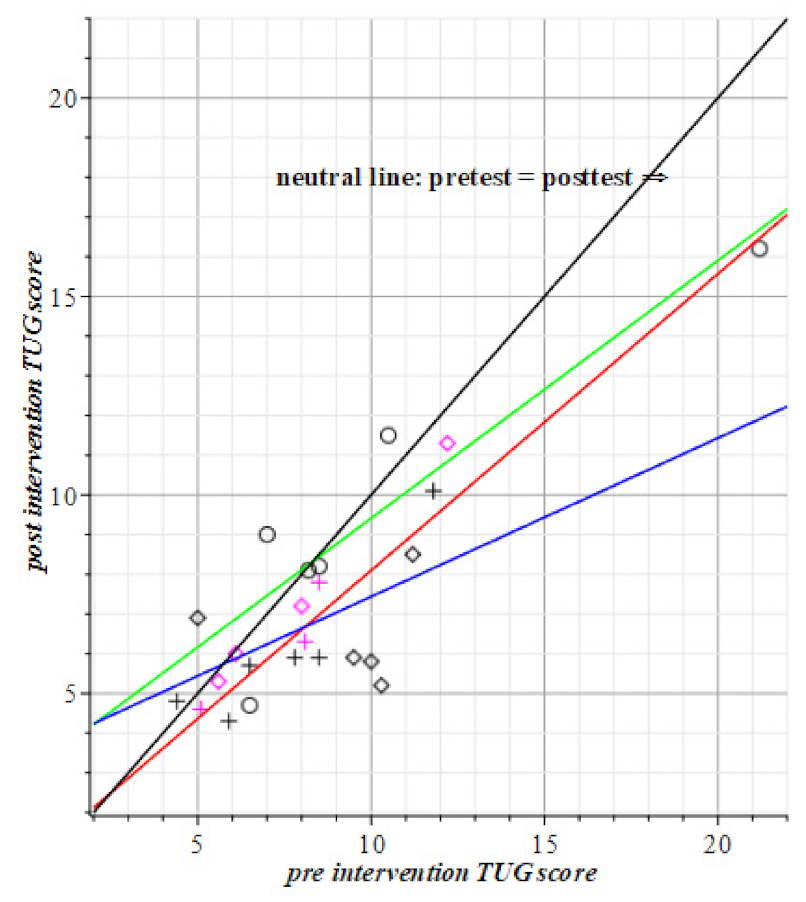
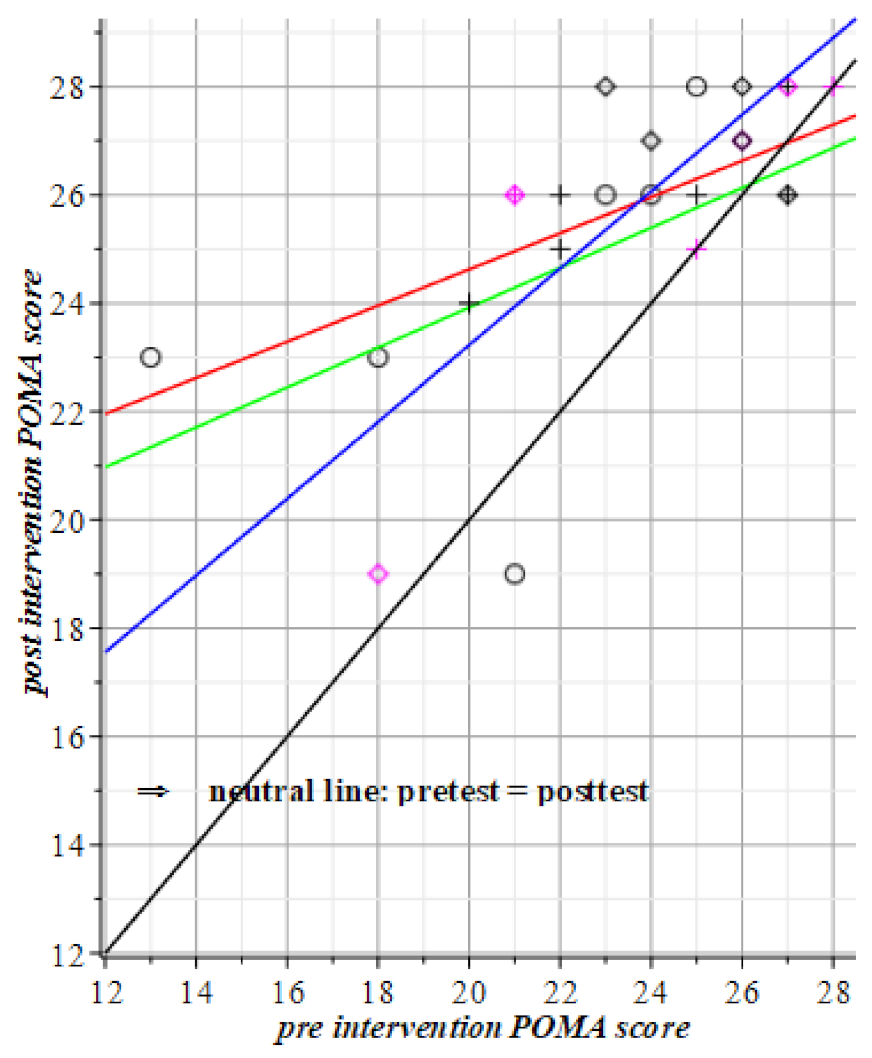
2.6.2. Comparison of Intervention Groups w.r.t. the SPPB, TUG, and POMA Motor Tests
2.6.3. Comparison of the Interventions w.r.t. the Visuo-Spatial-Motor Tests
3. Results
3.1. Independence of the Groups
3.2. Summary of Section
Comparison of the Intervention w.r.t. SPPB, TUG, and POMA
3.3. Comparison of Interventions and Subjects with Help of Testing with FitLight®s
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Experimental Set-Up for Testing Reaction Times

- −
- Runtime exercise: 60 s
- −
- Timeout: 3 s
- −
- Light delay: 0.05 s
- −
- Touch sensor mode: Distance 20 cm
- −
- Led mode: Standard
- −
- Light mode: Full light
- The lights come on “haphazardly”;
- The subject must deactivate the illuminated disc as soon as possible;
- The moment the light is extinguished, another light switches on immediately. The subject must also turn off this light, etc.
- −
- Measure the subject’s average reaction time in relation to the visual stimulation;
- −
- Measure the number of hits, the subject is able to score in 60 s.
- How quickly the subject’s eyes detect the lights;
- How quickly the brain processes provide a response to that information;
- How fast and efficient is the motor movement towards the target and how fast to be ready for the next action.
- How many lights did you take out in 60 s?
- Missed lights?
- Average reaction time?
Appendix B. Test and Set-Up for Fusion Flexibility of the Eyes

- −
- Time out: 5 s
- −
- Light Delay: 0.05 s
- −
- Impact sensitivity: 1
- −
- Lamps: 10
- −
- Color lamps: Varying: Blue, Red, Green, Yellow, Cyan, and Magenta
- −
- Led mode: Standard
- −
- Light mode: Full light
- 4 lamps on a table and 6 lamps are mounted on a tripod;
- The subject sits on a chair at that table;
- The exercise begins: First a lamp on the table lights up;
- The subject must deactivate the illuminated disc as soon as possible and at that moment a lamp on one of the stands switches on;
- The subject names the number associated with that lamp and the color of the lamp that came on, in that order;
- An assistant turns out the lamp that came on, after which the subject names the number and color;
- When that lamp is turned off, another lamp lights up on the table and the subject at the table repeats the exercise.
- −
- Measure the subject’s average reaction time in relation to the visual stimulation;
- −
- Measure how long it takes the subject to turn off the 16 lights.
- Quickly the subject’s eyes detect the lights?
- Quickly the brain processes provide a response to that information?
- Fast and efficient is the motor movement towards the target and how fast to be ready for the next action?
- How much time do you need to turn off 16 lights?
- Missed lights?
- Average reaction time?
Appendix C. Test and Set-Up of Leg Movements

- −
- Runtime exercise: 24 lights
- −
- Timeout: 4 s
- −
- Light delay: Dynamic from 0.05 to 2.10 s
- −
- Impact sensitivity: 1
- −
- Lamps: 6
- −
- Color lamps: Varying: Blue, Red, Green, Yellow, Cyan, and Magenta
- −
- Led mode: Standard
- −
- Light mode: Full light
- The lights come on “haphazardly”;
- The subject must deactivate the illuminated disc as soon as possible;
- The moment the light is extinguished, another light will turn on. The lights are not switched on after an equal interval, but this interval varies;
- The subject must also turn off this light, etc.
- −
- Measure the subject’s average reaction time in relation to the visual stimulation;
- −
- Measure how long it takes the subject to turn off the 24 lights.
- Quickly the subject’s eyes detect the lights?
- Quickly the brain processes provide a response to that information?
- Fast and efficient is the motor movement towards the target and how fast to be ready for the next action?
- How much time do you need to turn off 24 lights?
- Missed lights?
- Average reaction time?
References
- Tang, P.F.; Woollacott, M.H. Inefficient postural responses to unexpected slips during walking in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1998, 53A, M471–M480. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.F.; Woollacott, M.H. Phase-dependent modulation of proximal and distal postural responses to slips in young and older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1999, 54A, M89–M102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okubo, Y.; Sturnieks, D.L.; Brodie, M.A.; Duran, L.; Lord, S.R. Effect of Reactive Balance Training Involving Repeated Slips and Trips on Balance Recovery Among Older Adults: A Blinded Randomized Controlled Trial. J. Gerontol. Ser. A 2019, 74, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.L.; Scarpace, D.; Alexander, N.B. Tests of stepping as indicators of mobility, balance, and fall risk in balance-impaired older adults. J. Am. Geriatr. Soc. 2004, 52, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Hartholt, K.A.; van Beeck, E.F.; Polinder, S.; van der Velde, N.; van Lieshout, E.M.M.; Panneman, M.J.M.; van der Cammen, T.J.M.; Patka, P. Societal consequences of falls in the older population: Injuries, healthcare costs and long term reduced quality of life. J. Trauma 2011, 71, 748–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Does, H.; Baan, A.; Panneman, M. Privé-Valongevallen Bij Ouderen; Report 812; Report 870; Veiligheid: Amsterdam, The Netherlands, 2020; pp. 1–22. Available online: www.Veiligheid.nl (accessed on 25 June 2021).
- Scuffham, P.; Chaplin, S.; Legood, R. Incidence and costs of unintentional falls in older people in the United Kingdom. J. Epidemiol. Community Health 2003, 57, 740–744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurmi, I.; Lüthje, P. Incidence and costs of falls and fall injuries among elderly in institutional care. Scand. J. Prim. Health Care 2002, 20, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Haddad, Y.K.; Bergen, G.; Florence, C.S. Estimating the Economic Burden Related to Older Adult Falls by State. J. Public Health Manag. Pract. 2019, 25, E17–E24. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnadottir, S.A.; Bruce, J.; Lall, R.; Withers, E.J.; Underwood, M.; Shaw, F.; Sheridan, R.; Hossain, A.; Lamb, S.E.; Martin, F.; et al. The importance of different frailty domains in a population based sample in England. BMC Geriatr. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Luukinen, H.; Koski, K.; Laippala, P.; Kivelä, S.-L. Factors Predicting Fractures During Falling Impacts Among Home-Dwelling Older Adults. J. Am. Geriatr. Soc. 1997, 45, 1302–1309. [Google Scholar] [CrossRef]
- Maki, B.E. Gait Changes in Older Adults: Predictors of Falls or Indicators of Fear? J. Am. Geriatr. Soc. 1997, 45, 313–320. [Google Scholar] [CrossRef]
- Hill, K.D.; Schwarz, J.A.; Kalogeropoulos, A.J.; Gibson, S.J. Fear of falling revisited. Arch. Phys. Med. Rehabil. 1996, 77, 1025–1029. [Google Scholar] [CrossRef]
- Roaldsen, K.S.; Halvarsson, A.; Sahlström, T.; Ståhle, A. Task-specific balance training improves self-assessed function in community-dwelling older adults with balance deficits and fear of falling: A randomized controlled trial. Clin. Rehabil. 2014, 28, 1189–1197. [Google Scholar] [CrossRef] [Green Version]
- Lavedán, A.; Viladrosa, M.; Jürschik, P.; Botigué, T.; Nuín, C.; Masot, O.; Lavedán, R. Fear of falling in community-dwelling older adults: A cause of falls, a consequence, or both? PLoS ONE 2018, 13, e0194967. [Google Scholar] [CrossRef]
- Wollesen, B.; Wanstrath, M.; Van Schooten, K.S.; Delbaere, K. A taxonomy of cognitive tasks to evaluate cognitive-motor interference on spatiotemoporal gait parameters in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2019, 16, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Buchner, D.M.; Hornbrook, M.C.; Kutner, N.G.; Tinetti, M.E.; Ory, M.G.; Mulrow, C.D.; Schechtman, K.B.; Gerety, M.B.; Fiatarone, M.A.; Wolf, S.L.; et al. Development of the Common Data Base for the FICSIT trials. J. Am. Geriatr. Soc. 1993, 41, 297–308. [Google Scholar] [CrossRef]
- Yamada, M.; Ichihashi, N. Predicting the probability of falls in community-dwelling elderly individuals using the trail-walking test. Environ. Health Prev. Med. 2010, 15, 386–391. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Close, J.C.T.; Heim, J.; Sachdev, P.S.; Brodaty, H.; Slavin, M.J.; Kochan, N.A.; Lord, S.R. A multifactorial approach to understanding fall risk in older people. J. Am. Geriatr. Soc. 2010, 58, 1679–1685. [Google Scholar] [CrossRef]
- Rossat, A.; Fantino, B.; Nitenberg, C.; Annweiler, C.; Poujol, L.; Herrmann, F.R.; Beauchet, O. Risk factors for falling in community-dwelling older adults: Which of them are associated with the recurrence of falls? J. Nutr. Health Aging 2010, 14, 787–791. [Google Scholar] [CrossRef]
- Lecuyer Giguère, F.; Frasnelli, A.; De Guise, É.; Frasnelli, J. Olfactory, cognitive and affective dysfunction assessed 24 h and one year after a mild Traumatic Brain Injury (mTBI). Brain Inj. 2019, 33, 1184–1193. [Google Scholar] [CrossRef] [PubMed]
- Physiopedia. Available online: https://www.physio-pedia.com/ (accessed on 4 September 2020).
- Special Issue on Elderly Falls. J. Saf. 2011, 42, 415–542. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/journal/journal-of-safety-research/vol/42/issue/6 (accessed on 25 June 2021).
- Fixsen, D.; Scott, V.; Blase, K.; Naoom, S.; Wagar, L. When evidence is not enough: The challenge of implementing fall prevention strategies. J. Saf. Res. 2011, 42, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, V.; Jones-Hughes, T.; Thompson-Coon, J.; Boddy, K.; Stein, K. Implementing the evidence for preventing falls among community-dwelling older people: A systematic review. J. Saf. Res. 2011, 42, 443–451. [Google Scholar] [CrossRef]
- Haines, T.P.; Waldron, N.G. Translation of falls prevention knowledge into action in hospitals: What should be translated and how should it be done? J. Saf. Res. 2011, 42, 431–442. [Google Scholar] [CrossRef]
- Noonan, R.K.; Sleet, D.A.; Stevens, J.A. Closing the gap: A research agenda to accelerate the adoption and effective use of proven older adult fall prevention strategies. J. Saf. Res. 2011, 42, 427–430. [Google Scholar] [CrossRef]
- Beauchet, O.; Allali, G.; Berrut, G.; Dubost, V. Is low lower-limb kinematic variability always an index of stability? Gait Posture 2007, 26, 327–328. [Google Scholar] [CrossRef]
- Muir, S.W.; Beauchet, O.; Montero-Odasso, M.; Annweiler, C.; Fantino, B.; Speechley, M. Association of executive function impairment, history of falls and physical performance in older adults: A cross-sectional population-based study in Eastern France. J. Nutr. Health Aging 2013, 17, 661–665. [Google Scholar] [CrossRef] [Green Version]
- Muir, J.W.; Kiel, D.P.; Hannan, M.; Magaziner, J.; Rubin, C.T. Dynamic Parameters of Balance Which Correlate to Elderly Persons with a History of Falls. PLoS ONE 2013, 8, e70566. [Google Scholar] [CrossRef]
- Cuevas-Trisan, R. Balance Problems and Fall Risks in the Elderly. Clin. Geriatr. Med. 2019, 35, 173–183. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gstes, S.; Clemson, L.M.; Lamb, S.E.; Gates, S.; Clemson, L.M.; Lamb, S.E. Environmental interventions for preventing falls in older people living in the community (Review). Cochrane Database Syst. Rev. 2012, 2012, 1–416. [Google Scholar]
- Cameron, I.D.; Dyer, S.M.; Panagoda, C.E.; Murray, G.R.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for Preventing Falls in Older People in Care Facilities and Hospitals (Review); John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2020. [Google Scholar]
- Veuas, B.J.; Wayne, S.J.; Romero, L.J.; Baumgartner, R.N.; Garry, P.J.P.; Vellas, B.J.; Wayne, S.J.; Romero, L.J.; Baumgartner, R.N.; Garry, P.J.P. Fear of falling and restriction of mobility in elderly fallers. Age Ageing 1997, 26, 189–193. [Google Scholar]
- Van Moorselaar, D.; Olivers, C.N.L.; Theeuwes, J.; Lamme, V.A.F.; Sligte, I.G. Forgotten but Not Gone: Retro-Cue Costs and Benefits in a Double-Cueing Paradigm Suggest Multiple States in Visual Short-Term Memory. J. Exp. Psychol. Learn. Mem. Cogn. 2015, 41, 1755–1763. [Google Scholar] [CrossRef]
- Lipsitz, L.A.; Jonsson, P.V.; Kelley, M.M.; Koestner, J.S. Causes and Correlates of Recurrent Falls in Ambulatory Frail Elderly. J. Gerontol. 1991, 46, M114–M122. [Google Scholar] [CrossRef]
- Van Schoor, N.M.; Smit, J.H.; Pluijm, S.M.F.F.; Jonker, C.; Lips, P. Different cognitive functions in relation to falls among older persons Immediate memory as an independent risk factor for falls. J. Clin. Epidemiol. 2002, 55, 855–862. [Google Scholar] [CrossRef]
- Brown, L.A.; Shumway-Cook, A.; Woollacott, M.H. Attentional demands and postural recovery: The effects of aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1999, 54, 165–171. [Google Scholar] [CrossRef] [Green Version]
- Baris Deger, T.; Fulden Saraç, Z.; Sumru Sava, E.; Fehmi Akçiçek, S. The Relationship of Balance Disorders with Falling, the Effect of Health Problems, and Social Life on Postural Balance in the Elderly Living in a District in Turkey. Geriatrics 2019, 4, 1–10. [Google Scholar]
- Shumway-Cook, A.; Baldwin, M.; Polissar, N.L.; Gruber, W. Predicting the probability for falls in community-dwelling older adults. Phys. Ther. 1997, 77, 812–819. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.K.A.; Pillai, S.G.K.; Tan, S.T.; Tai, C.C.; Shahar, S. Association between physiological falls risk and physical performance tests among community-dwelling older adults. Clin. Interv. Aging 2015, 10, 1319–1326. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Molinero, A.; Galvez-Barrón, C.; Narvaiza, L.; Miñarro, A.; Ruiz, J.; Valldosera, E.; Gonzalo, N.; Ng, T.; Sanguino, M.J.; Yuste, A. A two-question tool to assess the risk of repeated falls in the elderly. PLoS ONE 2017, 12, e0176703. [Google Scholar] [CrossRef] [Green Version]
- Lundin-Olsson, L.; Nyberg, L.; Gustafson, Y. “Stops walking when talking” as a predictor of falls in elderly people. Lancet 1997, 349, 617. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed] [Green Version]
- Kim, J.C.; Chon, J.; Kim, H.S.; Lee, J.H.; Yoo, S.D.; Kim, D.H.; Lee, S.A.; Han, Y.J.; Lee, H.S.; Lee, B.Y.; et al. The association between fall history and physical performance tests in the community-dwelling elderly: A cross-sectional analysis. Ann. Rehabil. Med. 2017, 41, 239–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hooren, B.; Venner, P.; Bosch, F. De dynamische systeemtheorie in fysieke training. Deel I: Onderliggende concepten. Sportgericht 2017, 71, 12–19. [Google Scholar]
- Van Hooren, B.; Meijer, K.; McCrum, C. Attractive gait training: Applying dynamical systems theory to the improvement of locomotor performance across the lifespan. Front. Physiol. 2019, 9, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Furuki, D.; Takiyama, K. Decomposing motion that changes over time into task-relevant and task-irrelevant components in a data-driven manner: Application to motor adaptation in whole-body movements. Sci. Rep. 2019, 9, 1–17. [Google Scholar] [CrossRef]
- Runge, M.; Hunger, G. Determinants of musculoskeletal frailty and the risk of falls in old age. J. Musculoskelet. Neuronal Interact. 2006, 6, 167–173. [Google Scholar]
- Balzer, K.; Bremer, M.; Schramm, S.; Lühmann, D.; Raspe, H. Falls prevention for the elderly. GMS Health Technol. Assess. 2012, 8, 1–8. [Google Scholar]
- Chang, J.T.; Morton, S.C.; Rubenstein, L.Z.; Mojica, W.A.; Maglione, M.; Suttorp, M.J.; Roth, E.A.; Shekelle, P.G. Interventions for the prevention of falls in older adults: Systematic review and meta-analysis of randomised clinical trials. Br. Med. J. 2004, 328, 680–683. [Google Scholar] [CrossRef] [Green Version]
- Woollacott, M.H. Editorial: Systems Contributing to Balance Disorder in Older adults. J. Gerontol. Med. Sci. 2000, 55A, M424–M428. [Google Scholar] [CrossRef] [Green Version]
- Zecevic, A.A.; Salmoni, A.W.; Speechley, M.; Vandervoort, A.A. Defining a fall and reasons for falling: Comparisons among the Views of Seniors, Health Care Providers, and the Research Literature. Gerontologist 2006, 46, 367–376. [Google Scholar] [CrossRef]
- Beauchet, O.; Dubost, V.; Aminian, K.; Gonthier, R.; Kressig, R.W. Dual-task-related gait changes in the elderly: Does the type of cognitive task matter? J. Mot. Behav. 2005, 37, 259–264. [Google Scholar]
- Beauchet, O.; Berrut, G. Marche et double tâche: Définition, intérêts et perspectives. Psychol. Neuropsychiatr. Vieil. 2006, 4, 215–225. [Google Scholar]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. Do we always prioritize balance when walking? Towards an integrated model of task prioritization. Mov. Disord. 2012, 27, 765–777. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Giladi, N.; Gruendlinger, L.; Hausdorff, J.M. The contribution of postural control and bilateral coordination to the impact of dual tasking on gait. Exp. Brain Res. 2013, 226, 81–93. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Sprecher, E.; Kodesh, E. The Effect of External and Internal Focus of Attention on Gait Variability in Older Adults. J. Mot. Behav. 2017, 49, 179–184. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M. Attentional demands and postural control: The effect of sensory context. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 54, M10–M16. [Google Scholar]
- Dubost, V.; Kressig, R.W.; Gonthier, R.; Herrmann, F.R.; Aminian, K.; Najafi, B.; Beauchet, O. Relationships between dual-task related changes in stride velocity and stride time variability in healthy older adults. Hum. Mov. Sci. 2006, 25, 372–382. [Google Scholar] [CrossRef]
- Priest, A.W.; Salamon, K.B.; Hollman, J.H. Age-related differences in dual task walking: A cross sectional study. J. Neuroeng. Rehabil. 2008, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hausdorff, J.M.; Schweiger, A.; Herman, T.; Yogev-Seligmann, G.; Giladi, N. Dual-task decrements in gait: Contributing factors among healthy older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 1335–1343. [Google Scholar] [CrossRef]
- Zijlstra, A.; Ufkes, T.; Skelton, D.A.; Lundin-Olsson, L.; Zijlstra, W. Do dual tasks have an added value over single tasks for balance assessment in fall prevention programs? A mini-review. Gerontology 2008, 54, 40–49. [Google Scholar] [CrossRef]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Yogev-Seligmann, G.; Rotem-Galili, Y.; Mirelman, A.; Dickstein, R.; Giladi, N.; Hausdorff, J.M. How Does Explicit Prioritization Alter Walking During Dual-Task Performance? Effects of Age and Sex on Gait Speed and Variability. Phys. Ther. 2010, 90, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Beauchet, O.; Annweiler, C.; Dubost, V.; Allali, G.; Kressig, R.W.; Bridenbaugh, S.; Berrut, G.; Assal, F.; Herrmann, F.R. Stops walking when talking: A predictor of falls in older adults? Eur. J. Neurol. 2009, 16, 786–795. [Google Scholar] [CrossRef]
- Segev-Jacubovski, O.; Herman, T.; Yogev-Seligmann, G.; Mirelman, A.; Giladi, N.; Hausdorff, J.M. The interplay between gait, falls and cognition: Can cognitive therapy reduce fall risk? Expert Rev. Neurother. 2011, 11, 1057–1075. [Google Scholar] [CrossRef] [Green Version]
- Classen, J.; Gerloff, C.; Honda, M.; Hallett, M. Integrative Visuomotor Behavior Is Associated with Interregionally Coherent Oscillations in the Human Brain. J. Neurophysiol. 1998, 79, 1567–1573. [Google Scholar] [CrossRef]
- Feng, G. Is there a common control mechanism for anti-saccades and reading eye movements? Evidence from distributional analyses. Vis. Res. 2012, 57, 35–50. [Google Scholar] [CrossRef] [Green Version]
- Honda, T.; Nagao, S.; Hashimoto, Y.; Ishikawa, K.; Yokota, T.; Mizusawa, H.; Ito, M. Tandem internal models execute motor learning in the cerebellum. Proc. Natl. Acad. Sci. USA 2018, 115, 7428–7433. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.R.; Chen, Y.C.; Lee, C.S.; Cheng, S.J.; Wang, R.Y. Dual-task-related gait changes in individuals with stroke. Gait Posture 2007, 25, 185–190. [Google Scholar] [CrossRef]
- Van Iersel, M.B.; Ribbers, H.; Munneke, M.; Borm, G.F.; Olde Rikkert, M.G. The Effect of Cognitive Dual Tasks on Balance During Walking in Physically Fit Elderly People. Arch. Phys. Med. Rehabil. 2007, 88, 187–191. [Google Scholar] [CrossRef]
- Makizako, H.; Kaneko, F.; Aoki, N.; Ihira, H. Age-related Differences in Reaction Time Responses under Simple- and Dual-task Conditions in Middle-aged Ski Marathon Amateur Males. Int. J. Sport Health Sci. 2013, 11, 33–38. [Google Scholar] [CrossRef]
- Hinault, T.; Larcher, K.; Bherer, L.; Courtney, S.M.; Dagher, A. Age-related differences in the structural and effective connectivity of cognitive control: A combined fMRI and DTI study of mental arithmetic. Neurobiol. Aging 2019, 82, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Pijnappels, M.; Reeves, N.D.; Maganaris, C.N.; van Dieën, J.H. Tripping without falling; lower limb strength, a limitation for balance recovery and a target for training in the elderly. J. Electromyogr. Kinesiol. 2008, 18, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Kannape, O.A.; Barré, A.; Aminian, K.; Blanke, O. Cognitive loading affects motor awareness and movement kinematics but not locomotor trajectories during goal-directed walking in a virtual reality environment. PLoS ONE 2014, 9, e85560. [Google Scholar] [CrossRef]
- Punt, M.; Bruijn, S.M.; Van Schooten, K.S.; Pijnappels, M.; Van De Port, I.G.; Wittink, H.; Van Dieën, J.H. Characteristics of daily life gait in fall and non fall-prone stroke survivors and controls. J. Neuroeng. Rehabil. 2016, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Nashner, L.M.; Woollacott, M.; Tuma, G. Organization of rapid responses to postural and locomotor-like perturbations of standing man. Exp. Brain Res. 1979, 36, 463–476. [Google Scholar] [CrossRef]
- Camicioli, R.; Howieson, D.; Lehman, S.; Kaye, J. Talking while walking: The effect of a dual task in aging and Alzheimer’s disease. Neurology 1997, 48, 955–958. [Google Scholar] [CrossRef]
- Aivar, M.P.; Brenner, E.; Smeets, J.B.J. Hitting a target is fundamentally different from avoiding obstacles. Vis. Res. 2015, 110, 166–178. [Google Scholar] [CrossRef] [Green Version]
- Persichetti, A.S.; Dilks, D.D. Dissociable Neural Systems for Recognizing Places and Navigating through Them. J. Neurosci. 2018, 38, 10295–10304. [Google Scholar] [CrossRef] [Green Version]
- Jana, S.; Gopal, A.; Murthy, A. Evidence of common and separate eye and hand accumulators underlying flexible eye-hand coordination. J. Neurophysiol. 2017, 117, 348–364. [Google Scholar] [CrossRef] [Green Version]
- Jana, S.; Gopal, A.; Murthy, A. A Computational Framework for Understanding Eye-Hand Coordination. J. Indian Inst. Sci. 2017, 97, 543–554. [Google Scholar] [CrossRef]
- Gopal, A.; Jana, S.; Murthy, A. Contrasting speed-accuracy tradeoffs for eye and hand movements reveal the optimal nature of saccade kinematics. J. Neurophysiol. 2017, 118, 1664–1676. [Google Scholar] [CrossRef]
- Di Carlo, A.; Baldereschi, M.; Amaducci, L.; Maggi, S.; Grigoletto, F.; Scarlato, G.; Inzitari, D. Cognitive impairment without dementia in older people: Prevalence, vascular risk factors, impact on disability. The Italian Longitudinal Study on Aging. J. Am. Geriatr. Soc. 2000, 48, 775–782. [Google Scholar] [CrossRef]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2016, 63, 67–83. [Google Scholar] [CrossRef] [Green Version]
- Annweiler, C.; Beauchet, O.; Bartha, R.; Montero-Odasso, M. Slow gait in MCI is associated with ventricular enlargement: Results from the Gait and Brain Study. J. Neural Transm. 2013, 120, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Myint, P.K.; Welch, A.A. Healthier ageing. Br. Med. J. 2012, 344, 42–45. [Google Scholar] [CrossRef]
- Gorniak, S.L. The relationship between task difficulty and motor performance complexity. Atten. Percept. Psychophys. 2018, 81, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Carpenter, C.R.; McFarland, F.; Avidan, M.; Berger, M.; Inouye, S.K.; Karlawish, J.; Lin, F.R.; Marcantonio, E.; Morris, J.C.; Reuben, D.B.; et al. Impact of Cognitive Impairment Across Specialties: Summary of a Report from the U13 Conference Series. J. Am. Geriatr. Soc. 2019, 67, 2011–2017. [Google Scholar] [CrossRef] [Green Version]
- Van Der Velde, N.; Stricker, B.H.C.; Pols, H.A.P.; Van Der Cammen, T.J.M. Risk of falls after withdrawal of fall-risk-increasing drugs: A prospective cohort study. Br. J. Clin. Pharmacol. 2006, 63, 232–237. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Lee, K.W.; Khang, P. Preventing falls in the geriatric population. Perm. J. 2013, 17, 37–39. [Google Scholar] [CrossRef]
- Dury, S.; Dierckx, E.; Van Der Vorst, A.; Van Der Elst, M.; Fret, B.; Duppen, D.; Hoeyberghs, L.; De Roeck, E.; Lambotte, D.; Smetcoren, A.-S.; et al. Detecting frail, older adults and identifying their strengths: Results of a mixed-methods study. BMC Public Health 2018, 18, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Selinger, J.C.; O’Connor, S.M.; Wong, J.D.; Donelan, J.M. Humans Can Continuously Optimize Energetic Cost during Walking. Curr. Biol. 2015, 25, 2452–2456. [Google Scholar] [CrossRef] [Green Version]
- Vachon, C.M.; Modchalingam, S.; ’t Hart, B.M.; Henriques, D.Y.P. The effect of age on visuomotor learning processes. PLoS ONE 2020, 15, e0239032. [Google Scholar] [CrossRef]
- Brenner, E.; Abalo Rodriguez, I.; Muñoz, V.E.; Schootemeijer, S.; Mahieu, Y.; Veerkamp, K.; Zandbergen, M.; Van Der Zee, T.; Smeets, J.B.J. How Can People Be so Good at Intercepting Accelerating Objects if They Are so Poor at Visually Judging Acceleration? i-Perception 2016, 7, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Dostalek, M.; Fliegel, K.; Dusek, L.; Lukes, T.; Hejda, J.; Duchackova, M.; Hozman, J.; Autrata, R. Influence of artificially generated interocular blur difference on fusion stability under vergence stress. J. Eye Mov. Res. 2019, 12, 1–15. [Google Scholar]
- Kolers, P.A.; Rosner, B.S. On visual masking (metacontrat): Dichoptic observation. Am. J. Psychol. 1960, 73, 2–21. [Google Scholar] [CrossRef]
- Tatler, B.W.; Kuhn, G. Don’t look now: The Magic of Misdirection. In Eye Movements: A Window on Mind and Brain; van Gompel, R.P.G., Fischer, M.H., Murray, W.S., Hill, R.L., Eds.; Elsevier Ltd.: Amsterdam, The Netherlands, 2007; pp. 697–714. ISBN 9780080449807. [Google Scholar]
- Davis, J.; Wang, S.; Festa, E.; Luo, G.; Moharrer, M.; Bernier, J.; Ott, B. Detection of Risky Driving Behaviors in the Naturalistic Environment in Healthy Older Adults and Mild Alzheimer’s Disease. Geriatrics 2018, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Carr, D.B.; Grover, P. The role of eye tracking technology in assessing older driver safety. Geriatrics 2020, 5, 36. [Google Scholar] [CrossRef] [PubMed]
- Priya Venkataraman, A.; Lewis, P.; Unsbo, P.; Lundström, L. Peripheral resolution and contrast sensitivity: Effects of stimulus drift. Vis. Res. 2017, 133, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Tadin, D.; Park, W.J.; Dieter, K.C.; Melnick, M.D.; Lappin, J.S.; Blake, R. Spatial suppression promotes rapid figure-ground segmentation of moving objects. Nat. Commun. 2019, 10, 2732. [Google Scholar] [CrossRef] [PubMed]
- Koppelaar, H.; Kordestani-Moghadan, P.; Khan, K.; Kouhkani, S.; Segers, G.; van Warmerdam, M. Reaction Time Improvements by Neural Bistability. Behav. Sci. 2019, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- DeLoss, D.J.; Watanabe, T.; Anderson, G.J. Improving Vision Among Older Adults: Behavioral Training to Improve Sight. Psychol. Sci. 2015, 26, 456–466. [Google Scholar] [CrossRef] [Green Version]
- Nemoto, M.; Sasai, H.; Yabushita, N.; Tsuchiya, K.; Hotta, K.; Fujita, Y.; Kim, T.; Tsujimoto, T.; Arai, T.; Tanaka, K. A Novel Exercise for Enhancing Visuospatial Ability in Older Adults with Frailty: Development, Feasibility, and Effectiveness. Geriatrics 2020, 5, 29. [Google Scholar] [CrossRef]
- Pedroli, E.; Greci, L.; Colombo, D.; Serino, S.; Cipresso, P.; Arlati, S.; Mondellini, M.; Boilini, L.; Giussani, V.; Goulene, K.; et al. Characteristics, Usability, and Users Experience of a System Combining Cognitive and Physical Therapy in a Virtual Environment: Positive Bike. Sensors 2018, 18, 2343. [Google Scholar] [CrossRef] [Green Version]
- Ayed, I.; Ghazel, A.; Jaume-I-Capó, A.; Moya-Alcover, G.; Varona, J.; Martínez-Bueso, P. Feasibility of Kinect-Based Games for Balance Rehabilitation: A Case Study. J. Healthc. Eng. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Noohu, M.M.; Dey, A.B.; Hussain, M.E. Relevance of balance measurement tools and balance training for fall prevention in older adults. J. Clin. Gerontol. Geriatr. 2014, 5, 31–35. [Google Scholar] [CrossRef] [Green Version]
- Diamond, J.S.; Wolpert, D.M.; Flanagan, J.R. Rapid target foraging with reach or gaze: The hand looks further ahead than the eye. PLoS Comput. Biol. 2017, 13, e1005504. [Google Scholar] [CrossRef] [Green Version]
- Clément, G.; Reschke, M.F. Neurosensory and sensory-motor functions. In Biological and Medical Research in Space; Moore, D., Bie, P., Oser, H., Eds.; Springer: Berlin/Heidelberg, Germany, 1996; pp. 178–258. [Google Scholar]
- Fisher, B.; Ramsperger, E.; Fischer, B.; Ramsperger, E. Human express saccades: Extremely short reaction times of goal direction eye movements. Exp. Brain Res. 1984, 57, 191–195. [Google Scholar] [CrossRef]
- Fischer, B.; Weber, H. Express saccades and visual attention. Behav. Brain Sci. 1993, 16, 553–610. [Google Scholar] [CrossRef] [Green Version]
- Kingstone, A.; Klein, R.M. What are human express saccades? Percept. Psychophys. 1993, 54, 260–273. [Google Scholar] [CrossRef] [Green Version]
- Paré, M.; Munoz, D.P.; Pare, M.; Munoz, D.P. Saccadic reaction time in the monkey: Advanced preparation of oculomotor programs is primarily responsible for express saccade occurrence. J. Neurophysiol. 1996, 76, 3666–3681. [Google Scholar] [CrossRef]
- Marino, R.A.; Levy, R.; Munoz, D.P. Linking express saccade occurance to stimulus properties and sensorimotor integration in the superior colliculus. J. Neurophysiol. 2015, 114, 879–892. [Google Scholar] [CrossRef] [Green Version]
- Pijnappels, M.A.G.M.M.; Bobbert, M.F.M.F.; van Dieen, J.H.; van Dieën, J.H. Push-off reactions in recovery after tripping discriminate young subjects, older non-fallers and older fallers. Gait Posture 2005, 21, 388–394. [Google Scholar] [CrossRef]
- Peel, T.R.; Dash, S.; Lomber, S.G.; Corneil, B.D. Frontal Eye Field Inactivation Diminishes Superior Colliculus Activity, But Delayed Saccadic Accumulation Governs Reaction Time Increases. J. Neurosci. 2017, 37, 11715–11730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nibbeling, N.; Oudejans, R.R.D.; Daanen, H.A.M. Effects of anxiety, a cognitive secondary task, and expertise on gaze behavior and performance in a far aiming task. Psychol. Sport Exerc. 2012, 13, 427–435. [Google Scholar] [CrossRef]
- Richardson, L. Fear of Falling. Qual. Inq. 2014, 20, 1133–1140. [Google Scholar] [CrossRef]
- Gotardi, G.C.; Polastri, P.F.; Schor, P.; Oudejans, R.R.D.; Van Der Kamp, J.; Savelsbergh, G.J.P.; Navarro, M.; Rodrigues, S.T. Adverse effects of anxiety on attentional control differ as a function of experience: A simulated driving study. Appl. Ergon. 2019, 74, 41–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duijnhouwer, J. Studies on the Rotation Problem in Self-Motion Perception. Ph.D. Thesis, Radboud University, Nijmegen, The Netherlands, 2013. Available online: https://repository.ubn.ru.nl/handle/2066/121139 (accessed on 25 June 2021).
- Duijnhouwer, J.; Krekelberg, B. Evidence and counterevidence in motion perception. Cereb. Cortex 2016, 26, 4602–4612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullen, K.E.; Brooks, J.X.; Jamali, M.; Carriot, J.; Massot, C. Internal models of self-motion: Computations that suppress vestibular reafference in early vestibular processing. Exp. Brain Res. 2011, 210, 377–388. [Google Scholar] [CrossRef]
- Cullen, K.E.; Taube, J.S. Our sense of direction: Progress, controversies and challenges. Nat. Neurosci. 2017, 20, 1465–1473. [Google Scholar] [CrossRef]
- Fait, P.E.; McFadyen, B.J.; Zabjek, K.; Reed, N.; Taha, T.; Keightley, M. Increasing task complexity and ice hockey skills of youth athletes. Percept. Mot. Skills 2011, 112, 29–43. [Google Scholar] [CrossRef]
- Cao, L.; Händel, B. Walking enhances peripheral visual processing in humans. PLoS Biol. 2019, 17, e3000511. [Google Scholar] [CrossRef] [Green Version]
- Ceylan, H.I.; Saygin, O. Examining the effects of proprioceptive training on coincidence anticipation timing, reaction time and hand-eye coordination. Anthropologist 2015, 20, 437–445. [Google Scholar] [CrossRef]
- Liu, Y.; Chan, J.S.Y.; Yan, J.H.; Sharma, H.S. Neuropsychological mechanisms of falls in older adults. Front. Neurosci. 2014, 6, 1–8. [Google Scholar] [CrossRef]
- Gao, Y.; Huber, C.; Sabel, B.A. Stable microsaccades and microsaccade-induced global alpha band phase reset across the life span. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2032–2041. [Google Scholar] [CrossRef] [Green Version]
- Poth, C.H.; Herwig, A.; Schneider, W.X. Breaking Object Correspondence Across Saccadic Eye Movements Deteriorates Object Recognition. Front. Syst. Neurosci. 2015, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Irwin, D.E. Where does attention go when you blink? Atten. Percept. Psychophys. 2011, 73, 1374–1384. [Google Scholar] [CrossRef]
- Costela, F.M.; Otero-Millan, J.; McCamy, M.B.; Macknik, S.L.; Troncoso, X.G.; Jazi, A.N.; Crook, S.M.; Martinez-Conde, S. Fixational eye movement correction of blink-induced gaze position errors. PLoS ONE 2014, 9, e110889. [Google Scholar] [CrossRef]
- Khazali, M.F.; Pomper, J.K.; Thier, P. Blink associated resetting eye movements (BARMs) are functionally complementary to microsaccades in correcting for fixation errors. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.C.; Cao, B.; Dali, V.; Gagliardi, C.; Barthelemy, O.J.; Salazar, R.D.; Pomplun, M.; Cronin-Golomb, A.; Yazdanbakhsh, A. Eye movement control during visual pursuit in Parkinson’s disease. PeerJ 2018, 6, e5442. [Google Scholar] [CrossRef]
- Irwin, D.E.; Robinson, M.M. Perceiving a continuous visual world across voluntary eye blinks. J. Exp. Psychol. Hum. Percept. Perform. 2016, 42, 1490–1496. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Robinson, M.M. How post-saccadic target blanking affects the detection of stimulus displacements across saccades. Vis. Res. 2018, 142, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, E. Visual mislocalization during double-step saccades. Front. Syst. Neurosci. 2015, 9, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, E.; Morrone, M.C.; Binda, P. Perception during double-step saccades. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atsma, J.; Maij, F.; Koppen, M.; Irwin, D.E.; Medendorp, W.P. Causal Inference for Spatial Constancy across Saccades. PLoS Comput. Biol. 2016, 12, e1004766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cronin, D.A.; Irwin, D.E. Visual working memory supports perceptual stability across saccadic eye movements. J. Exp. Psychol. Hum. Percept. Perform. 2018, 44, 1739–1759. [Google Scholar] [CrossRef] [Green Version]
- Herwig, A. Transsaccadic integration and perceptual continuity. J. Vis. 2015, 15, 1–6. [Google Scholar] [CrossRef]
- Paeye, C.; Collins, T.; Cavanagh, P.; Herwig, A. Calibration of peripheral perception of shape with and without saccadic eye movements. Atten. Percept. Psychophys. 2018, 80, 723–737. [Google Scholar] [CrossRef]
- Poth, C.H.; Schneider, W.X. Breaking object correspondence across saccades impairs object recognition: The role of color and luminance. J. Vis. 2016, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- White, A.L.; Rolfs, M. Oculomotor inhibition covaries with conscious detection. J. Neurophysiol. 2016, 116, 1507–1521. [Google Scholar] [CrossRef] [Green Version]
- Wurtz, R.H. Corollary Discharge Contributions to Perceptual Continuity Across Saccades. Annu. Rev. Vis. Sci. 2018, 4, 215–237. [Google Scholar] [CrossRef] [Green Version]
- Puntiroli, M.; Kerzel, D.; Born, S. Perceptual enhancement prior to intended and involuntary saccades. J. Vis. 2015, 15, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Bozhkova, V.P.; Surovicheva, N.S.; Nikolaev, D.P.; Nikolaev, I.P.; Bolshakov, A.S. Smooth Pursuit in Elderly Adults Studied with Apparent Motion. Perception 2015, 44, 1040–1053. [Google Scholar] [CrossRef]
- Braun, J.; Mattia, M. NeuroImage Attractors and noise: Twin drivers of decisions and multistability. Neuroimage 2010, 52, 740–751. [Google Scholar] [CrossRef]
- Bremmer, F.; Churan, J.; Lappe, M. Heading representations in primates are compressed by saccades. Nat. Commun. 2017, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, C.; Klingenhoefer, S.; Bremmer, F. Preattentive and Predictive Processing of Visual Motion. Sci. Rep. 2018, 8, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Matziridi, M.; Brenner, E.; Smeets, J.B.J. Moving your head reduces perisaccadic compression. J. Vis. 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ivanov, I.V.; Kramer, D.J.; Mullen, K.T. The role of the foreshortening cue in the perception of 3D object slant. Vis. Res. 2014, 94, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Gabbard, C.; Robinson, K.; Fox, A. A Program to Improve Reach Estimation and Reduce Fall Risk in the Elderly. Geriatrics 2016, 1, 14. [Google Scholar] [CrossRef]
- Maruta, J.; Spielman, L.A.; Rajashekar, U.; Ghajar, J. Visual Tracking in Development and Aging. Front. Neurol. 2017, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Saftari, L.N.; Kwon, O.S. Ageing vision and falls: A review. J. Physiol. Anthropol. 2018, 37, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Fischer, J.; Whitney, D. Serial dependence in visual perception. Nat. Neurosci. 2014, 17, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fritsche, M.; Mostert, P.; de Lange, F.P. Opposite Effects of Recent History on Perception and Decision. Curr. Biol. 2017, 27, 590–595. [Google Scholar] [CrossRef] [Green Version]
- Alais, D.; Kong, G.; Palmer, C.; Clifford, C. Eye gaze direction shows a positive serial dependency. J. Vis. 2018, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Thiamwong, L.; Suwanno, J. Effects of simple balance training on balance performance and fear of falling in rural older adults. Int. J. Gerontol. 2014, 8, 143–146. [Google Scholar] [CrossRef]
- Gusi, N.; Carmelo Adsuar, J.; Corzo, H.; del Pozo-Cruz, B.; Olivares, P.R.; Parraca, J.A. Balance training reduces fear of falling and improves dynamic balance and isometric strength in institutionalised older people: A randomised trial. J. Physiother. 2012, 58, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Ebitz, R.B.; Platt, M.L. Neuronal activity in primate dorsal anterior cingulate cortex signals task conflict and predicts adjustments in pupil-linked arousal. Neuron 2015, 85, 628–640. [Google Scholar] [CrossRef] [Green Version]
- Maki, B.E.; McIlroy, W.E. Control of rapid limb movements for balance recovery: Age-related changes and implications for fall prevention. Age Ageing 2006, 35, ii12–ii18. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.D.; Pack, C.C. The Contribution of Area MT to Visual Motion Perception Depends on Training. Neuron 2017, 95, 436–446. [Google Scholar] [CrossRef] [Green Version]
- Wollesen, B.; Wildbredt, A.; Van Schooten, K.S.; Lim, M.L.; Delbaere, K. The effects of cognitive-motor training interventions on executive functions in older people: A systematic review and meta-analysis. Eur. Rev. Aging Phys. Act. 2020, 17, 1–22. [Google Scholar] [CrossRef]
- Rodríguez-Molinero, A.; Herrero-Larrea, A.; Miñarro, A.; Narvaiza, L.; Gálvez-Barrón, C.; León, N.G.; Valldosera, E.; De Mingo, E.; Macho, O.; Aivar, D.; et al. The spatial parameters of gait and their association with falls, functional decline and death in older adults: A prospective study. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandormael, H.; Herce Castañón, S.; Balaguer, J.; Li, V.; Summerfield, C. Robust sampling of decision information during perceptual choice. Proc. Natl. Acad. Sci. USA 2017, 114, 2771–2776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köpke, S.; Meyer, G. The Tinetti test: Babylon in geriatric assessment. Z. Gerontol. Geriatr. 2006, 39, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Faber, M.J.; Bosscher, R.J.; van Wieringen, P.C.W. Clinimetric Properties of the Performance-Oriented Mobility Assessment. Phys. Ther. 2006, 86, 944–954. [Google Scholar] [CrossRef] [Green Version]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and Gait Speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar]
- Milanovic, Z.; Pantelic, S.; Milanović, Z.; Pantelić, S.; Trajković, N.; Sporiš, G.; Kostić, R.; James, N. Age-related decrease in physical activity and functional fitness among elderly men and women. Clin. Interv. Aging 2013, 3, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Siu, K.C.; Woollacott, M.H. Attentional demands of postural control: The ability to selectively allocate information-processing resources. Gait Posture 2007, 25, 121–126. [Google Scholar] [CrossRef]
- Mirelman, A.; Weiss, A.; Buchman, A.S.; Bennett, D.A.; Giladi, N.; Hausdorff, J.M. Association between performance on timed up and go subtasks and mild cognitive impairment: Further insights into the links between cognitive and motor function. J. Am. Geriatr. Soc. 2014, 62, 673–678. [Google Scholar] [CrossRef]
- Cohen, H.; Blatchly, C.A.; Laurie, L.C. A Study of the Clinical Test of Sensory Interaction and Balance. Phys. Ther. 1993, 73, 346–351. [Google Scholar] [CrossRef]
- Delignières, D.; Torre, K.; Bernard, P.L. Transition from persistent to anti-persistent correlations in postural sway indicates velocity-based control. PLoS Comput. Biol. 2011, 7, e1001089. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed Up and Go: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Mathias, S.; Nayak, U.S.; Isaacs, B. Balance in Elderly Patients: The “Get-Up and Go” Test. Arch. Phys. Med. Rehabil. 1986, 67, 387–389. [Google Scholar]
- Northridge, M.E.; Nevitt, M.C.; Kelsey, J.L.; Link, B. Home hazards and falls in the elderly: The role of health and functional status. Am. J. Public Health 1995, 85, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Graafmans, W.C.; Ooms, M.E.; Hofstee, H.M.A.; Bezemer, P.D.; Bouter, L.M.; Lips, P. Falls in the elderly: A Prospective Study of Risk Factors and Risk Profiles. Am. J. Epidemiol. 1996, 143, 1129–1136. [Google Scholar] [CrossRef] [Green Version]
- Dzhafarov, E.N. The Structure of Simple Reaction Time to Step-Function Signals. J. Math. Psychol. 1992, 36, 235–268. [Google Scholar] [CrossRef]
- Dzhafarov, E.N. Visual Kinematics I. Visual Space Metric in Visual Motion. J. Math. Psychol. 1992, 36, 471–497. [Google Scholar] [CrossRef]
- Dzhafarov, E.N. Visual Kinematics II. Space Contraction in Motion and Visual Velocity. J. Math. Psychol. 1992, 36, 498–523. [Google Scholar] [CrossRef]
- Dzhafarov, E.N. Visual Kinematics III. Transformation of Spatiotemporal Coordinates in Motion. J. Math. Psychol. 1992, 36, 524–546. [Google Scholar] [CrossRef]
- Paquette, M.R.; Li, Y.; Hoekstra, J.; Bravo, J. An 8-week reactive balance training program in older healthy adults: A preliminary investigation. J. Sport Health Sci. 2015, 4, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Excel. Available online: https://office.com/ (accessed on 7 June 2021).
- Maple. Available online: https://www.maplesoft.com/products/Maple/ (accessed on 7 June 2021).
- Liu-Ambrose, T.; Donaldson, M.G.; Ahamed, Y.; Graf, P.; Cook, W.L.; Close, J.; Lord, S.R.; Khan, K.M. Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J. Am. Geriatr. Soc. 2008, 56, 1821–1830. [Google Scholar] [CrossRef]
- Gardner, M.M.; Robertson, M.C.; McGee, R.; Campbell, A.J. Application of a falls prevention program for older people to primary health care practice. Prev. Med. 2002, 34, 546–553. [Google Scholar] [CrossRef]
- Faber, M.J.; Bosscher, R.J.; Chin A Paw, M.J.; van Wieringen, P.C. Effects of Exercise Programs on Falls and Mobility in Frail and Pre-Frail Older Adults: A Multicenter Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2006, 87, 885–896. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Tiedemann, A. Physiotherapy in the prevention of falls in older people. J. Physiother. 2015, 61, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Gleeson, M.; Sherrington, C.; Keay, L. Exercise and physical training improve physical function in older adults with visual impairments but their effect on falls is unclear: A systematic review. J. Physiother. 2014, 60, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Coubard, O.A.; Coto-Montes, A.M.; Gowen, E. Fall prevention modulates decisional saccadic behavior in aging. Front. Aging Neurosci. 2012, 4, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Harrison, W.J.; Bex, P.J. Integrating Retinotopic Features in Spatiotopic Coordinates. J. Neurosci. 2014, 34, 7351–7360. [Google Scholar] [CrossRef] [Green Version]
- Ruff, D.A.; Brainard, D.H.; Cohen, M.R. Neuronal population mechanisms of lightness perception. J. Neurophysiol. 2018, 120, 2296–2310. [Google Scholar] [CrossRef] [Green Version]
- Molina, K.I.; Ricci, N.A.; Albuquerque De Moraes, S.; Rodrigues Perracini, M. Virtual reality using games for improving physical functioning in older adults: A systematic review. J. Neuroeng. Rehabil. 2014, 11, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Mirelman, A.; Rochester, L.; Maidan, I.; Del Din, S.; Alcock, L.; Nieuwhof, F.; Rikkert, M.O.; Bloem, B.R.; Pelosin, E.; Avanzino, L.; et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): A randomised controlled trial. Lancet 2016, 388, 1170–1182. [Google Scholar] [CrossRef] [Green Version]
- Van Diest, M.; Lamoth, C.J.; Stegenga, J.; Verkerke, G.J.; Postema, K. Exergaming for balance training of elderly: State of the art and future developments. J. Neuroeng. Rehabil. 2013, 10, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Willaert, J.; De Vries, A.W.; Tavernier, J.; Van Dieen, J.H.; Jonkers, I.; Verschueren, S. Does a novel exergame challenge balance and activate muscles more than existing off-the-shelf exergames? J. Neuroeng. Rehabil. 2020, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, J.A.; Woollacott, M. Effect of high-intensity strength-training on functional measures of balance ability in balance-impaired older adults. J. Manip. Physiol. Ther. 2005, 28, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Bai, J.J. Balance training in the intervention of fall risk in elderly with diabetic peripheral neuropathy: A review. Int. J. Nurs. Sci. 2014, 1, 441–445. [Google Scholar] [CrossRef] [Green Version]
- Schoene, D.; Valenzuela, T.; Lord, S.R.; De Bruin, E.D. The effect of interactive cognitive-motor training in reducing fall risk in older people: A systematic review. BMC Geriatr. 2014, 14, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inglin, B.; Woollacott, M. Age-related changes in anticipatory postural adjustments associated with arm movements. J. Gerontol. 1988, 43, M105–M113. [Google Scholar] [CrossRef]
- Montgomery, G.; McPhee, J.; Pääsuke, M.; Sipilä, S.; Maier, A.B.; Hogrel, J.-Y.; Degens, H. Determinants of Performance in the Timed Up-and-Go and Six-Minute Walk Tests in Young and Old Healthy Adults. J. Clin. Med. 2020, 9, 61. [Google Scholar] [CrossRef]
- Heindorf, M.; Arber, S.; Keller, G.B. Mouse Motor Cortex Coordinates the Behavioral Response to Unpredicted Sensory Feedback. Neuron 2018, 99, 1040–1054.e5. [Google Scholar] [CrossRef] [Green Version]
- Kordestani-Moghadam, P.; Koppelaar, H.; Kouhkani, S.; Segers, G. When does the Brain Ask for Help from the Eyes? J. Phys. Med. Rehabil. 2020, 2, 1–6. [Google Scholar]
- Fogt, N.F.; Zimmerman, A.B. A Method to Monitor Eye and Head Tracking Movements in College Baseball Players. Optom. Vis. Sci. 2014, 91, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Fogt, N.; Kuntsch, E.; Zimmerman, A. Horizontal Head and Eye Rotations of Non-Expert Baseball Batters. Optom. Vis. Perform. 2019, 7, 29–46. [Google Scholar]
- Hogg, R.V.; Craig, A.T. Introduction to Mathematical Statistics, 7th ed.; The Macmillan Company: London, UK, 1972. [Google Scholar]
- McSorley, E.; Morriss, J. What you see is what you want to see: Motivationally relevant stimuli can interrupt current resource allocation. Cogn. Emot. 2017, 31, 168–174. [Google Scholar] [CrossRef]
- McSorley, E.; Morriss, J.; van Reekum, C.M. Eye spy with my little eye: Motivational relevance of visual stimuli guide eye-movements at different processing stages. Biol. Psychol. 2017, 123, 8–14. [Google Scholar] [CrossRef] [Green Version]
- Morriss, J.; Mcsorley, E.; Van Reekum, C.M. I don’t know where to look: The impact of intolerance of uncertainty on saccades towards non-predictive emotional face distractors. Cogn. Emot. 2017, 32, 1–11. [Google Scholar] [CrossRef]
- Morriss, J.; McSorley, E. Intolerance of uncertainty is associated with reduced attentional inhibition in the absence of direct threat. Behav. Res. Ther. 2019, 118, 1–6. [Google Scholar] [CrossRef]
- Liu, Z.X.; Shen, K.; Olsen, R.K.; Ryan, J.D. Age-related changes in the relationship between visual exploration and hippocampal activity. Neuropsychologia 2018, 119, 81–91. [Google Scholar] [CrossRef]
- Wynn, J.S.; Olsen, R.K.; Binns, M.A.; Buchsbaum, B.R.; Ryan, J.D. Fixation reinstatement supports visuospatial memory in older adults. J. Exp. Psychol. Hum. Percept. Perform. 2018, 44, 1119–1127. [Google Scholar] [CrossRef]
- Melnik, A.; Schüler, F.; Rothkopf, C.A.; König, P. The World as an External Memory: The Price of Saccades in a Sensorimotor Task. Front. Behav. Neurosci. 2018, 12, 1–8. [Google Scholar] [CrossRef]
- Clark, A.; Chalmers, D. The extended mind. Analysis 1998, 58, 10–23. [Google Scholar] [CrossRef]
- Ryan, J.D.; Shen, K.; Liu, Z.X. The intersection between the oculomotor and hippocampal memory systems: Empirical developments and clinical implications. Ann. N. Y. Acad. Sci. 2020, 1464, 115–141. [Google Scholar] [CrossRef] [Green Version]
- Hopf, S.; Liesenfeld, M.; Schmidtmann, I.; Ashayer, S.; Pitz, S. Age dependent normative data of vertical and horizontal reflexive saccades. PLoS ONE 2018, 13, e0204008. [Google Scholar] [CrossRef] [Green Version]
- Sherback, M.; Valero-Cuevas, F.J.; D’Andrea, R. Slower visuomotor corrections with unchanged latency are consistent with optimal adaptation to increased endogenous noise in the elderly. PLoS Comput. Biol. 2010, 6, e1000708. [Google Scholar] [CrossRef]
- Fiehler, K.; Brenner, E.; Spering, M. Prediction in goal-directed action. J. Vis. 2019, 19, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Klever, L.; Voudouris, D.; Fiehler, K.; Billino, J. Age effects on sensorimotor predictions: What drives increased tactile suppression during reaching? J. Vis. 2019, 19, 1–17. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, 239–243. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Williams, C.S. Falls, Injuries due to falls, and the Risk of Admission to a Nursing Home. N. Engl. J. Med. 2015, 337, 1279–1284. [Google Scholar] [CrossRef] [Green Version]
- Harezlak, K.; Kasprowski, P. Searching for Chaos Evidence in Eye Movement Signals. Entropy 2018, 20, 32. [Google Scholar] [CrossRef] [Green Version]
- Reschke, M.F.; Kolev, O.I.; Clément, G. Eye-Head Coordination in 31 Space Shuttle Astronauts during Visual Target Acquisition. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef]
- Wilkins, A.J.; Nimmo-Smith, I.; Slater, A.I.; Bedocs, L. Fluorescent lighting, headaches and eyestrain. Light. Res. Technol. 1989, 21, 11–18. [Google Scholar] [CrossRef]
- Wilkins, L.; Appelbaum, L.G. An early review of stroboscopic visual training: Insights, challenges and accomplishments to guide future studies. Int. Rev. Sport Exerc. Psychol. 2019, 13, 1–16. [Google Scholar] [CrossRef]
- Pijnappels, M.A.G.M.; van der Burg, J.C.E.; Reeves, N.D.; van Dieen, J.H. Identification of elderly fallers by muscle strength measures. Eur. J. Appl. Physiol. 2008, 102, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rispens, S.M.; van Schooten, K.S.; Pijnappels, M.; Daffertshofer, A.; Beek, P.J.; van Dieën, J.H. Do extreme values of daily-life gait characteristics provide more information about fall risk than median values? JMIR Res. Protoc. 2015, 4, e4. [Google Scholar] [CrossRef]
- Van Schooten, K.S.; Pijnappels, M.; Rispens, S.M.; Elders, P.J.M.; Lips, P.; Daffertshofer, A.; Beek, P.J.; van Dieën, J.H. Daily-Life Gait Quality as Predictor of Falls in Older People: A 1-Year Prospective Cohort Study. PLoS ONE 2016, 11, e0158623. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SPPB | TUG | POMA |
|---|---|---|
| 7.67 (±2.65) | 8.66 (±2.60) | 24.2 (±3.07) |
| 5.17 (±2.64) | 10.3 (±5.51) | 20.7 (±4.50) |
| 8.44 (±2.01) | 7.40 (±2.23) | 24.1 (±2.93) |
| SPPB | TUG | POMA |
|---|---|---|
| 10.8 (±1.30) | 6.90 (±1.95) | 26.2 (±2.82) |
| 9.00 (±2.53) | 9.62 (±3.89) | 24.2 (±3.19) |
| 10.8 (±1.72) | 6.16 (±1.81) | 26.0 (±1.32) |
| Test | Statistic | Critical Value | Probability |
|---|---|---|---|
| FitLight®Static | 0.542256 | 12.5916 | 0.997286 |
| FitLight®Dyn. | 0.838832 | 12.5916 | 0.990992 |
| Periph. Step | 0.148314 | 12.5916 | 0.999936 |
| Fusion Flex. | 0.345730 | 12.5916 | 0.999243 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koppelaar, H.; Kordestani-Moghadam, P.; Kouhkani, S.; Irandoust, F.; Segers, G.; de Haas, L.; Bantje, T.; van Warmerdam, M. Proof of Concept of Novel Visuo-Spatial-Motor Fall Prevention Training for Old People. Geriatrics 2021, 6, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6030066
Koppelaar H, Kordestani-Moghadam P, Kouhkani S, Irandoust F, Segers G, de Haas L, Bantje T, van Warmerdam M. Proof of Concept of Novel Visuo-Spatial-Motor Fall Prevention Training for Old People. Geriatrics. 2021; 6(3):66. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6030066
Chicago/Turabian StyleKoppelaar, Henk, Parastou Kordestani-Moghadam, Sareh Kouhkani, Farnoosh Irandoust, Gijs Segers, Lonneke de Haas, Thijmen Bantje, and Martin van Warmerdam. 2021. "Proof of Concept of Novel Visuo-Spatial-Motor Fall Prevention Training for Old People" Geriatrics 6, no. 3: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics6030066