
Determinants of Undernutrition and Associated Factors of Low Muscle Mass and High Fat Mass among Older Men and Women in the Colombo District of Sri Lanka


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Size Calculation
2.3. Sampling Technique
2.4. Data Collecting Instruments
2.5. Assessment of the Nutritional Status
2.6. Criteria of Classification of the Older People as Undernourished
2.7. Data Collection
2.8. Data Analysis
3. Results
3.1. Multiple Comparisons of Factors among Older Men and Women in the Sample
3.2. Prevalence of Undernutrition among the Older People
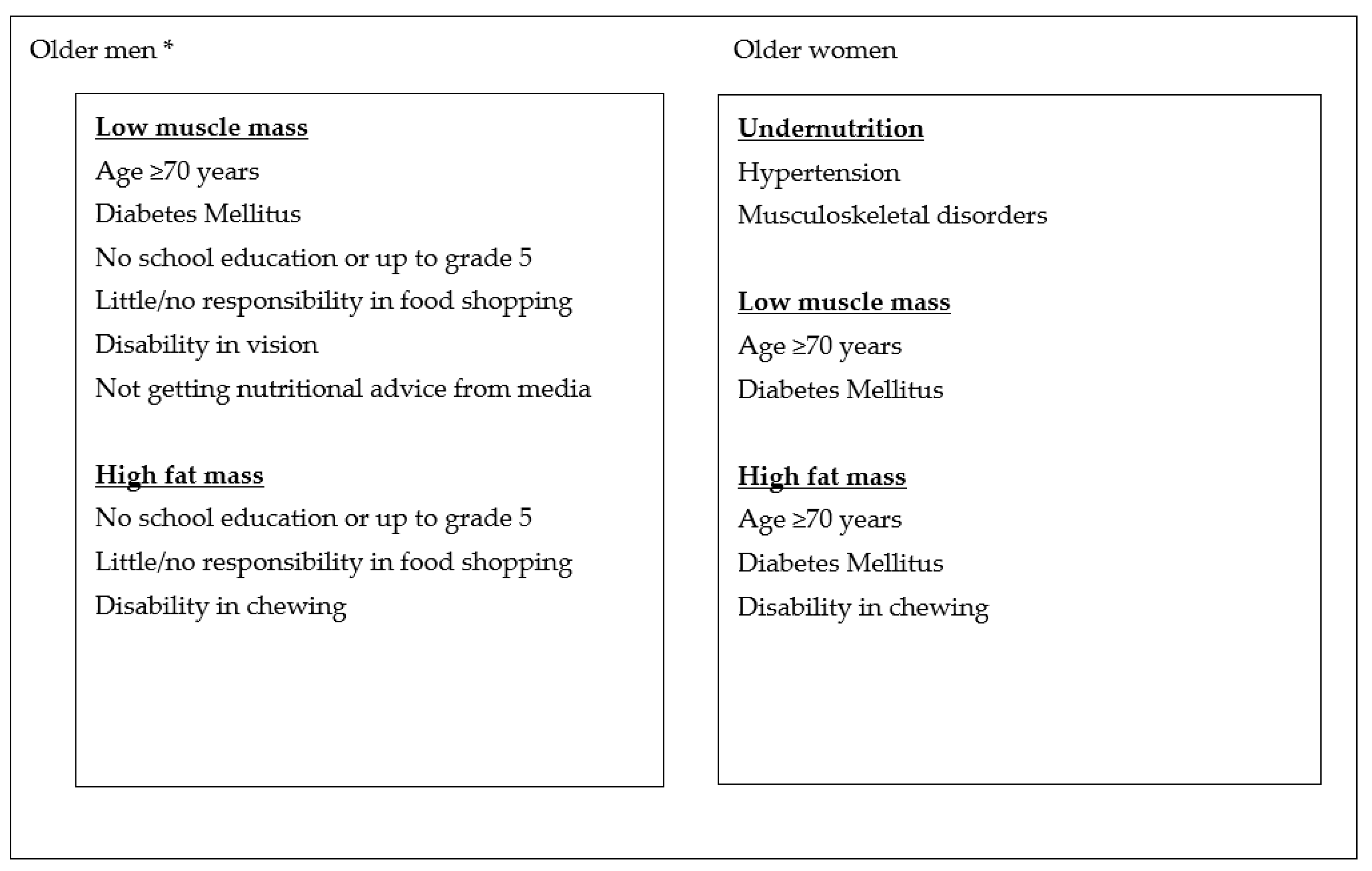
3.3. Determinants of Undernutrition among Older Men and Women
3.4. Factors Associated with Low Skeletal Muscle Mass among Older Men and Women
3.5. Factors Associated with High Fat Mass among Older Men and Women
4. Discussion
4.1. Prevalence of Undernutrition in Sri Lanka
4.2. Identification of Factors Associated with Undernutrition
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Report of Nutrition; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Starr, K.N.P.; McDonald, S.R.; Bales, C.W. Nutritional Vulnerability in Older Adults: A Continuum of Concerns. Curr. Nutr. Rep. 2015, 4, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schols, J. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar]
- Morley, J.E. Anorexia of aging: A key component in the pathogenesis of both sarcopenia and cachexia. J. Cachexia Sarcopenia Muscle 2017, 8, 523–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roh, E.; Choi, K.M. Health Consequences of Sarcopenic Obesity: A Narrative Review. Front. Endocrinol. 2020, 11, 332. Available online: https://www.frontiersin.org/article/10.3389/fendo.2020.00332 (accessed on 5 October 2021). [CrossRef] [PubMed]
- Azzolino, D.; Marzetti, E.; Proietti, M.; Calvani, R.; Barreto, P.D.S.; Rolland, Y.; Cesari, M. Lack of energy is associated with malnutrition in nursing home residents: Results from the INCUR study. J. Am. Geriatr. Soc. 2021, 69, 3242–3248. [Google Scholar] [CrossRef]
- van der Pols-Vijlbrief, R.; Wijnhoven, H.; Schaap, L.; Terwee, C.B.; Visser, M. Determinants of protein-energy malnutrition in community-dwelling older adults: A systematic review of observational studies. Ageing Res. Rev. 2014, 18, 112–131. [Google Scholar] [CrossRef]
- Rathnayake, K.M.; Wimalathunga, M.; Weech, M.; Jackson, K.G.; Lovegrove, J.A. High prevalence of undernutrition and low dietary diversity in institutionalised elderly living in Sri Lanka. Public Health Nutr. 2015, 18, 2874–2880. [Google Scholar] [CrossRef] [Green Version]
- Rajapaksa, L.; Arambepola, C.; Gunawardane, N. Nutritional Status in Sri Lanka, Determinants and Interventions: A Desk Review, 2006–2011; UNICEF Project: Colombo, Sri Lanka, 2011. [Google Scholar]
- Jayalath, W.A.T.A.; Kumara, S.K.G.P.H. Assessment of Nutritional Status of Elderly Hospitalized Patients according to Their Co-Morbid Conditions and Educational Levels Using Mini Nutrition Assessment Tool; Peradeniya University Research Sessions: Peradeniya, Sri Lanka, 2011. [Google Scholar]
- Perera, R.; Ekanayake, L. Distribution and correlates of Body Mass Index in elderly residents in Colombo District. J. Coll. Community Physicians Sri Lanka 2012, 17, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Damayanthi, H.D.W.T.; Moy, F.M.; Katija, L.; Dharmaratne, S.D. Malnutrition and associated factors among community dwelling elderly in Kandy District. Ann. Glob. Health 2017, 83, 7–82. [Google Scholar]
- Jayakody, K.W.G.G. Physical Health Status of the Elderly in the District of Mathale and Risk Factors for Undernutrition among the Rural Elderly. Ph.D. Thesis, University of Colombo, Colombo, Sri Lanka, 2002. [Google Scholar]
- Ithyaranjini, M. , Chandrasekara, G.A.P. Nutritional Status of Free-Living Elderly in an Urban Community. Abstracts of Scientific Sessions; Faculty of Livestock & Fisheries and Nutrition, University of Wayamba: Kuliyapitiya, Sri Lanka, 2007. [Google Scholar]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Measuring Obesity—Classification and Description of Anthropometric Data; Nutrition Unit EUR/ICP/NUT 125: Copenhagen, Denmark; WHO Regional Office for Europe: Geneva, Switzerland, 1989. [Google Scholar]
- Azzolino, D.; Cesari, M. Obesity and COVID-19. Front. Endocrinol. 2020, 11, 581356. Available online: https://www.frontiersin.org/article/10.3389/fendo.2020.581356 (accessed on 3 November 2021). [CrossRef]
- Al-Sofiani, M.; Ganji, S.S.; Kalyani, R.R. Body composition changes in diabetes and aging. J. Diabetes Complicat. 2019, 33, 451–459. [Google Scholar] [CrossRef]
- Department of Census and Statistics. Census of Population and Housing 2012; Department of Census and Statistics: Colombo, Sri Lanka, 2015. [Google Scholar]
- Fang, W.-H.; Yang, J.-R.; Lin, C.-Y.; Hsiao, P.-J.; Tu, M.-Y.; Chen, C.-F.; Tsai, D.-J.; Su, W.; Huang, G.-S.; Chang, H.; et al. Accuracy augmentation of body composition measurement by bioelectrical impedance analyzer in elderly population. Medicine 2020, 99, e19103. [Google Scholar] [CrossRef]
- Keur, P.; Deol, N.S. Assessment of Body Mass Index and resting metabolism of male sedentary and active older adults of Punjab, India. Laplage Revitas (Int.) 2021, 7, 552–564. [Google Scholar] [CrossRef]
- World Health Organization. The Asia Pacific Perspective: Redefining Obesity and Its’ Treatment. Western Pacific Region; International Organization for The Study of Obesity, International Obesity Task Force, Health Communication: Sydney, Australia, 2000. [Google Scholar]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry; WHO Technical Report. Series. No. 851; Report of WHO consultation: Gevewa, Switzerland, 1995. [Google Scholar]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. 2000, 72, 72–694. [Google Scholar] [CrossRef] [PubMed]
- Tichet, J.; Vol, S.; Goxe, D.; Salle, A.; Berrut, G.; Ritz, P. Prevalence of sarcopenia in the French senior population. J. Nutr. Health Ageing 2008, 12, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathew, A.C.; Das, D.; Sampath, S.; Vijayakumar, M.; Ramakrishnan, N.; Ravishankar, S.L. Prevalence and correlates of malnutrition among elderly in an urban area in Coimbatore. Indian J. Public Health 2016, 60, 112–117. [Google Scholar] [CrossRef]
- Ghimire, S.; Baral, B.K.; Callahan, K. Nutritional assessment of community-dwelling older adults in rural Nepal. PLoS ONE 2017, 12, e0172052. [Google Scholar] [CrossRef] [Green Version]
- Torres, M.J.; Dorigny, B.; Kuhn, M.; Berr, C.; Barberger-Gateau, P.; Letenneur, L. Nutritional status in community-dwelling elderly in France in urban and rural areas. PLoS ONE 2014, 9, e105137. [Google Scholar] [CrossRef] [PubMed]
- Gündüz, E.; Eskin, F.; Gunduz, M.; Bentli, R.; Zengin, Y.; Dursun, R.; Guloglu, C. Malnutrition in Community-Dwelling Elderly in Turkey: A Multicenter, Cross-Sectional Study. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2015, 21, 2750–2756. [Google Scholar] [CrossRef] [Green Version]
- De Silva, K.; Liyanage, C.; Wijesinghe, C.; Perera, B. Nutritional status of elders in Galle district, Sri Lanka. Galle Med. J. 2017, 22, 1–5. [Google Scholar] [CrossRef]
- Kim, T.N.; Yang, S.J.; Yoo, H.J.; Lim, K.I.; Kang, H.J.; Song, W.; Seo, J.A.; Kim, S.G.; Kim, N.H.; Baik, S.H.; et al. Prevalence of sarcopenia and sarcopenic obesity in Korean adults the Korean sarcopenic obesity study. Int. J. Obes. 2009, 33, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Wang, X.; Xie, H.; Zheng, S.; Wu, X.; Zhu, X.; Zhang, X.; Xue, S.; Li, H.; Hong, W.; et al. Sex differences in the prevalence and adverse outcomes of sarcopenia and sarcopenic obesity in community dwelling elderly in East China using the AWGS criteria. BMC Endocr. Disord. 2019, 19, 109. [Google Scholar] [CrossRef]
- Hashemi, R.; Gita, S.; Ahmadreza, D.M.; Parvin, P.; Ahmad, E.; Fereydoun, S.; Bagher, L.; Ramin, H. Sarcopenia and its associated factors in Iranian older individuals: Results of SARIR study. Arch. Gerontol. Geriatr. 2016, 66, 18–22. [Google Scholar] [CrossRef]
- Wu, I.-C.; Lin, C.-C.; Hsiung, C.A.; Wang, C.-Y.; Wu, C.-H.; Chan, D.-C.; Li, T.-C.; Lin, W.-Y.; Huang, K.-C.; Chen, C.-Y.; et al. Sarcopenia and Translational Aging Research in Taiwan Team. Epidemiology of sarcopenia among community-dwelling older adults in Taiwan: A pooled analysis for a broader adoption of sarcopenia assessments. Geriatr. Gerontol. Int. 2014, 14 (Suppl. 1), 52–60. [Google Scholar] [CrossRef]
- Tessfamichael, D.; Gete, A.A.; Wassie, M.M. High prevalence of undernutrition among elderly people in North West Ethiopia: A cross-sectional study. Nutr. Health Food Sci. 2014, 2, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, S.; Savabi, G.; Khazaei, S.; Savabi, O.; Esmaillzadeh, A.; Keshteli, A.H. Association between food intake and oral health in elderly: SEPAHAN systematic review no. 8. Dent. Res. J. 2011, 8 (Suppl. 1), S15–S20. [Google Scholar]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Hurvich, C.M.; Tsai, C.L. The impact of model selection on inference in linear regression. Am. Stat. 1990, 44, 214–217. [Google Scholar]
- Roecker, E.B. Prediction error and its estimation for subset-selected models. Technometrics 1991, 33, 459–468. [Google Scholar] [CrossRef]


{kind=link}
| Women 555/800 | Men 245/800 | Chi-Square Value (df = 1) | Effect Size (Phi Value) | p Value | |||
|---|---|---|---|---|---|---|---|
| Factor | N | % | N | % | |||
| Age—equal to or above 70 years | 184 | 33.2 | 101 | 41.2 | 4.828 | 0.08 | 0.028 |
| Ethnicity—Sinhalese | 547 | 98.6 | 230 | 93.9 | 13.338 | 0.13 | 0.001 |
| Marital status—widowed, divorced or unmarried | 204 | 36.8 | 7 | 2.9 | 1.006 | 0.04 | 0.001 |
| Living environment—urban | 212 | 38.5 | 53 | 21.6 | 21.055 | 0.16 | 0.001 |
| Level of school education—none or up to grade 5 | 87 | 15.7 | 32 | 13.1 | 0.918 | 0.03 | 0.338 |
| Unemployment | 498 | 89.7 | 177 | 72.2 | 39.415 | 0.22 | 0.001 |
| Not having a monthly income | 390 | 70.3 | 101 | 41.2 | 60.489 | 0.27 | 0.001 |
| Presence of diabetes | 205 | 36.9 | 88 | 35.9 | 0.076 | 0.01 | 0.783 |
| Presence of hypertension | 242 | 43.6 | 92 | 37.6 | 2.560 | 0.06 | 0.110 |
| Presence of heart disease | 56 | 10.1 | 33 | 13.5 | 1.963 | 0.05 | 0.161 |
| Presence of asthma/COPD | 30 | 5.4 | 7 | 2.9 | 2.502 | 0.06 | 0.114 |
| Disability in hearing | 87 | 15.7 | 34 | 13.9 | 0.428 | 0.02 | 0.513 |
| Disability in vision | 437 | 78.7 | 178 | 72.7 | 3.541 | 0.07 | 0.060 |
| Disability in chewing | 137 | 22.4 | 42 | 17.1 | 5.566 | 0.08 | 0.018 |
| Presence of musculoskeletal disorders | 124 | 22.3 | 43 | 17.6 | 2.362 | 0.05 | 0.124 |
| Current betel chewing | 37 | 6.7 | 72 | 29.4 | 74.559 | 0.31 | 0.001 |
| No responsibility in food shopping | 415 | 74.8 | 208 | 84.9 | 16.109 | 0.14 | 0.001 |
| No responsibility in planning meals | 442 | 79.4 | 190 | 77.6 | 0.447 | 0.02 | 0.504 |
| No responsibility in preparing meals | 495 | 89.2 | 59 | 24.1 | 3.389 | 0.07 | 0.001 |
| Skipping meals | 114 | 20.5 | 50 | 20.4 | 0.002 | 0.00 | 0.966 |
| Getting nutritional advice from GP | 483 | 87.0 | 223 | 91.0 | 2.614 | 0.06 | 0.106 |
| Getting nutritional advice from hospital | 371 | 66.2 | 191 | 80.0 | 14.243 | 0.13 | 0.001 |
| Getting nutritional advice from media | 502 | 90.5 | 229 | 93.5 | 1.966 | 0.05 | 0.161 |
| Women 262/555 | |||||
|---|---|---|---|---|---|
| Univariate Model | Multivariate Model | ||||
| Factor | OR (95% CI) | Effect Size (Cohen’s d Value) | p Value | OR (95% CI) | p Value |
| Age equal to or more than 70 years | 1.56 (1.07–2.19) | 0.114 | 0.018 | 0.61 (0.39–0.94) | 0.027 |
| Ethnicity—Sinhalese | 2.72 (0.54–13.58) | 0.239 | 0.20 | 0.42 (0.07–2.30) | 0.32 |
| Marital status—widowed, divorced or unmarried | 1.02 (0.72–1.44) | 0.005 | 0.90 | 1.01 (0.69–1.49) | 0.96 |
| Urban living environment | 1.39 (0.99–1.97) | 0.079 | 0.06 | 0.86 (0.57–1.30) | 0.48 |
| No school education or up to grade 5 | 0.89 (0.56–1.41) | 0.028 | 0.63 | 1.47 (0.87–2.47) | 0.15 |
| Unemployment | 1.26 (0.72–2.19) | 0.055 | 0.41 | 0.92 (0.41–1.84) | 0.81 |
| Not having a monthly income | 1.32 (0.91–1.90) | 0.066 | 0.14 | 0.81 (0.50–1.30) | 0.38 |
| Presence of diabetes | 1.04 (0.74–1.47) | 0.009 | 0.83 | 0.85 (0.59–1.28) | 0.43 |
| Presence of hypertension | 0.56 (0.40–0.79) | 0.138 | 0.001 | 1.97 (1.36–2.88) | 0.001 |
| Presence of heart disease | 0.89 (0.51–1.55) | 0.038 | 0.68 | 1.23 (0.67–2.26) | 0.50 |
| Presence of asthma/COPD | 1.13 (0.54–2.35) | 0.029 | 0.75 | 1.14 (0.51–2.51) | 0.75 |
| Presence of disability in hearing | 0.84 (0.53–1.34) | 0.042 | 0.47 | 1.37 (0.78–2.40) | 0.27 |
| Presence of disability in vision | 0.91 (0.60–1.36) | 0.023 | 0.63 | 1.25 (0.80–1.95) | 0.32 |
| Presence of disability in chewing | 1.55 (1.05–2.29) | 0.105 | 0.026 | 0.56 (0.34–0.90) | 0.018 |
| Presence of musculoskeletal disorders | 0.54 (0.35–0.81) | 0.137 | 0.003 | 2.19 (1.36–3.53) | 0.001 |
| Current betel chewing | 1.06 (0.55–2.07) | 0.014 | 0.86 | 1.05 (0.51–2.15) | 0.89 |
| Little or no responsibility in food shopping | 1.71 (1.16–2.51) | 0.128 | 0.006 | 0.56 (0.27–1.18) | 0.13 |
| Little or no responsibility in planning meals | 1.61 (1.06–2.44) | 0.114 | 0.024 | 1.36 (0.67–3.24) | 0.49 |
| Little or no responsibility in preparing meals | 1.65 (0.96–2.84) | 0.115 | 0.07 | 0.78 (0.38–1.56) | 0.48 |
| Skipping meals | 0.96 (0.64–1.46) | 0.009 | 0.86 | 0.87 (0.55–1.37) | 0.55 |
| Not getting nutritional advice from GP | 1.48 (0.89–2.40) | 0.094 | 0.13 | 0.78 (0.43–1.39) | 0.39 |
| Not getting nutritional advice from hospital | 0.79 (0.56–1.12) | 0.056 | 0.19 | 1.31 (0.85–2.02) | 0.22 |
| Not getting nutritional advice from media | 1.09 (0.62–1.92) | 0.020 | 0.77 | 0.99 (0.52–1.89) | 0.98 |
| Women 143/555 | Men 63/245 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Model | Multivariate Model | Univariate Model | Multivariate Model | |||||||
| Factor | OR (95% CI) | Effect Size (Cohen’s d Value) | p Value | OR (95% CI) | p Value | OR (95% CI) | Effect Size (Cohen’s d Value) | p Value | OR (95% CI) | p Value |
| Age equal to or more than 70 years | 0.66 (0.42–1.0) | 0.099 | 0.05 | 1.79 (1.18–3.34) | 0.009 | 1.84 (1.03–3.29) | 0.146 | 0.037 | 0.43 (0.20–9.1) | 0.028 |
| Ethnicity—Sinhalese | 0.57 (0.13–2.4) | 0.134 | 0.44 | 0.44 (0.09–2.04) | 0.29 | 0.36 (0.13–1.06) | 0.244 | 0.055 | 2.19 (0.64–7.52) | 0.21 |
| Marital status—widowed, divorced or unmarried | 0.79 (0.53–1.18) | 0.056 | 0.26 | 1.12 (0.75–1.76) | 0.61 | 2.22 (0.48–10.22) | 0.190 | 0.29 | 0.34 (0.05–2.42) | 0.28 |
| Urban living environment | 1.19 (0.81–1.8) | 0.042 | 0.38 | 0.85 (0.53–1.36) | 0.49 | 0.81 (0.39–1.66) | 0.050 | 0.56 | 0.93 (0.35–2.47) | 0.88 |
| No school education or up to grade 5 | 1.04 (0.62–1.8) | 0.009 | 0.88 | 0.64 (0.35–1.15) | 0.13 | 2.6 (1.20–5.60) | 0.228 | 0.012 | 0.27 (0.09–0.76) | 0.014 |
| Unemployment | 0.61 (0.34–1.09) | 0.118 | 0.09 | 1.28 (0.60–2.70) | 0.52 | 1.47 (0.75–2.89) | 0.092 | 0.25 | 1.89 (0.65–5.47) | 0.24 |
| Not having a monthly income | 0.69 (0.46–1.03) | 0.089 | 0.07 | 1.17 (0.69–1.90) | 0.56 | 2.01 (1.12–3.59) | 0.167 | 0.017 | 0.67 (0.28–1.63) | 0.38 |
| Presence of diabetes | 0.63 (0.42–0.96) | 0.110 | 0.03 | 1.77 (1.10–2.84) | 0.017 | 2.12 (1.18–3.81) | 0.179 | 0.011 | 0.34 (0.15–0.77) | 0.010 |
| Presence of hypertension | 1.56 (1.06–2.28) | 0.106 | 0.023 | 0.61 (0.39–0.92) | 0.020 | 1.35 (0.75–2.42) | 0.072 | 0.31 | 0.93 (0.42–2.05) | 0.86 |
| Presence of heart disease | 1.17 (0.63–2.20) | 0.038 | 0.61 | 0.88 (0.46–1.69) | 0.69 | 1.09 (0.48–2.56) | 0.021 | 0.83 | 0.99 (0.35–2.77) | 0.99 |
| Presence of asthma/COPD | 1.25 (0.56–2.80) | 0.053 | 0.59 | 0.60 (0.25–1.43) | 0.25 | 1.16 (0.21–6.13) | 0.035 | 0.86 | 3.22 (0.44–23.68) | 0.25 |
| Presence of disability in hearing | 1.04 (0.62–1.76) | 0.009 | 0.88 | 0.95 (0.51–1.78) | 0.88 | 1.71 (0.79–3.69) | 0.128 | 0.17 | 0.63 (0.21–1.88) | 0.41 |
| Presence of disability in vision | 0.91 (0.58–1.45) | 0.023 | 0.70 | 0.86 (0.52–1.78) | 0.57 | 3.93 (1.69–9.15) | 0.327 | 0.001 | 0.24 (0.08–0.69) | 0.008 |
| Presence of disability in chewing | 0.76 (0.48–1.20) | 0.066 | 0.23 | 1.69 (0.96–2.98) | 0.07 | 1.79 (0.88–3.64) | 0.139 | 0.10 | 0.75 (0.25–2.20) | 0.60 |
| Presence of musculoskeletal disorders | 2.03 (1.32–3.12) | 0.169 | 0.001 | 0.39 (0.24–0.65) | 0.001 | 1.31 (0.63–2.70) | 0.064 | 0.45 | 1.85 (0.59–5.7) | 0.28 |
| Current betel chewing | 0.78 (0.35–1.75) | 0.059 | 0.55 | 1.00 (0.42–2.38) | 0.99 | 0.94 (0.50–1.78) | 0.015 | 0.87 | 0.94 (0.40–2.19) | 0.88 |
| Little or no responsibility in food shopping | 0.75 (0.49–1.15) | 0.059 | 0.18 | 0.75 (0.34–1.67) | 0.48 | 0.33 (0.16–0.69) | 0.265 | 0.002 | 0.11 (0.01–0.67) | 0.017 |
| Little or no responsibility in planning meals | 0.76 (0.48–1.20) | 0.066 | 0.23 | 0.92 (0.36–2.37) | 0.87 | 0.51 (0.22–0.98) | 0.134 | 0.040 | 1.87 (0.37–9.48) | 0.45 |
| Little or no responsibility in preparing meals | 0.66 (0.37–1.17) | 0.099 | 0.15 | 0.82 (0.38–1.76) | 0.61 | 1.10 (0.57–2.13) | 0.023 | 0.77 | 1.65 (0.68–3.99) | 0.26 |
| Skipping meals | 1.16 (0.73–1.80) | 0.035 | 0.52 | 0.94 (0.56–1.58) | 0.82 | 1.16 (0.58–2.33) | 0.035 | 0.67 | 0.65 (0.26–1.62) | 0.36 |
| Not getting nutritional advice from GP | 0.61 (0.36–1.03) | 0.118 | 0.06 | 1.31 (0.71–2.45) | 0.39 | 0.46 (0.18–1.14) | 0.185 | 0.08 | 1.94 (0.57–6.6) | 0.29 |
| Not getting nutritional advice from hospital | 1.11 (0.74–1.67) | 0.025 | 0.61 | 0.92 (0.56–1.51) | 0.75 | 1.08 (0.52–2.24) | 0.018 | 0.82 | 0.58 (0.22–1.54) | 0.27 |
| Not getting nutritional advice from media | 1.07 (0.56–2.07) | 0.016 | 0.83 | 0.72 (0.35–1.51) | 0.39 | 5.57 (0.72–43.04) | 0.410 | 0.06 | 0.07 (0.01–0.95) | 0.045 |
| Women 139/555 | Men 66/245 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Model | Multivariate Model | Univariate Model | Multivariate Model | |||||||
| Factor | OR (95% CI) | Effect Size (Cohen’s d Value) | p Value | OR (95% CI) | p Value | OR (95% CI) | Cohen’s d Value | p Value | OR (95% CI) | p Value |
| Age equal to or more than 70 years | 0.66 (0.43–1.05) | 0.099 | 0.06 | 2.05 (1.21–3.47) | 0.007 | 0.90 (0.50–1.60) | 0.025 | 0.72 | 1.31 (0.62–2.70) | 0.48 |
| Ethnicity—Sinhalese | 1.00 (0.20–5.02) | 0.000 | 0.99 | 0.75 (0.13–4.21) | 0.74 | 1.50 (0.41–5.52) | 0.097 | 0.53 | 0.77 (0.17–3.40) | 0.73 |
| Marital status—widowed, divorced or unmarried | 1.12 (0.76–1.67) | 0.027 | 0.55 | 0.66 (0.42–1.05) | 0.08 | 1.08 (0.20–5.70) | 0.018 | 0.93 | 1.90 (0.20–18.12) | 0.56 |
| Urban living environment | 1.48 (1.00–2.19) | 0.094 | 0.046 | 0.72 (0.45–1.16) | 0.18 | 1.09 (0.55–2.15) | 0.021 | 0.80 | 0.76 (0.32–1.82) | 0.54 |
| No school education or up to grade 5 | 1.17 (0.69–1.96) | 0.038 | 0.55 | 0.50 (0.26–0.92) | 0.026 | 2.41 (1.17–5.17) | 0.210 | 0.022 | 0.29 (0.10–0.85) | 0.024 |
| Unemployment | 0.76 (0.42–1.39) | 0.066 | 0.38 | 1.12 (0.52–2.44) | 0.77 | 0.76 (0.41–1.40) | 0.066 | 0.39 | 2.07 (0.82–5.20) | 0.12 |
| Not having a monthly income | 0.74 (0.49–1.12) | 0.079 | 0.15 | 1.08 (0.63–1.85) | 0.78 | 1.07 (0.60–1.89) | 0.016 | 0.82 | 0.89 (0.38–2.13) | 0.81 |
| Presence of diabetes | 0.57 (0.37–0.86) | 0.134 | 0.007 | 2.20 (1.35–3.59) | 0.002 | 1.46 (0.82–2.60) | 0.090 | 0.19 | 0.69 (0.32–1.49) | 0.36 |
| Presence of hypertension | 1.96 (1.33–2.89) | 0.161 | 0.001 | 0.44 (0.28–0.68) | 0.44 | 1.44 (0.81–2.56) | 0.087 | 0.21 | 1.25 (0.59–2.60) | 0.56 |
| Presence of heart disease | 1.48 (0.81–2.69) | 0.094 | 0.19 | 0.72 (0.38–1.39) | 0.33 | 1.42 (0.65–3.13) | 0.084 | 0.37 | 0.52 (0.20–1.33) | 0.17 |
| Presence of asthma/COPD | 1.53 (0.70–3.36) | 0.102 | 0.28 | 0.46 (0.19–1.09) | 0.08 | 1.08 (0.20–5.74) | 0.018 | 0.92 | 2.58 (0.38–17.36) | 0.33 |
| Presence of disability in hearing | 0.94 (0.55–1.61) | 0.107 | 0.83 | 1.02 (0.54–1.93) | 0.95 | 1.35 (0.62–2.96) | 0.072 | 0.44 | 1.24 (0.41–3.74) | 0.70 |
| Presence of disability in vision | 0.92 (0.58–1.46) | 0.020 | 0.73 | 0.80 (0.48–1.33) | 0.80 | 1.34 (0.65–2.38) | 0.071 | 0.51 | 0.66 (0.28–1.50) | 0.66 |
| Presence of disability in chewing | 0.56 (0.34–0.91) | 0.138 | 0.019 | 2.39 (1.30–4.40) | 0.005 | 2.13 (1.05–4.28) | 0.181 | 0.030 | 0.34 (0.13–0.94) | 0.037 |
| Presence of musculoskeletal disorders | 1.37 (0.88–2.14) | 0.075 | 0.16 | 0.59 (0.35–0.98) | 0.045 | 1.21 (059–2.50) | 0.045 | 0.59 | 1.11 (0.38–3.18) | 0.85 |
| Current betel chewing | 0.68 (0.29–1.59) | 0.092 | 0.37 | 1.29 (0.52–3.2) | 0.58 | 0.70(0.37–1.34) | 0.085 | 0.28 | 1.65 (0.73–3.76) | 0.23 |
| Little or no responsibility in food shopping | 0.86 (0.56–1.33) | 0.036 | 0.51 | 1.20 (0.50–2.89) | 0.67 | 0.36 (0.18–0.75) | 0.244 | 0.005 | 0.05 (0.01–0.35) | 0.002 |
| Little or no responsibility in planning meals | 0.76 (0.48–1.21) | 0.066 | 0.25 | 0.58 (0.21–1.57) | 0.28 | 0.62 (0.33–1.19) | 0.114 | 0.15 | 4.43 (0.79–24.73) | 0.09 |
| Little or no responsibility in preparing meals | 0.76 (0.42–1.36) | 0.066 | 0.35 | 0.97 (0.44–2.14) | 0.94 | 1.01 (0.52–1.96) | 0.002 | 0.97 | 1.57 (0.69–3.58) | 0.29 |
| Skipping meals | 1.36 (0.86–2.15) | 0.074 | 0.19 | 0.69 (0.41–1.16) | 0.16 | 0.72 (0.34–1.50) | 0.078 | 0.38 | 1.15 (0.46–2.86) | 0.77 |
| Not getting nutritional advice from GP | 0.62 (0.37–1.07) | 0.114 | 0.08 | 1.47 (0.78–2.77) | 0.23 | 1.28 (0.45–3.67) | 0.059 | 0.64 | 1.24 (0.34–4.54) | 0.74 |
| Not getting nutritional advice from hospital | 1.00 (0.67–1.51) | 0.000 | 0.97 | 1.03 (0.62–1.69) | 0.91 | 0.71 (0.36–1.40) | 0.082 | 0.31 | 1.23 (0.51–2.98) | 0.65 |
| Not getting nutritional advice from media | 0.83 (0.44–1.56) | 0.044 | 0.56 | 0.96 (0.46–1.97) | 0.90 | 0.79 (0.27–2.39) | 0.056 | 0.69 | 2.03 (0.47–8.70) | 0.34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vijewardane, S.C.; Balasuriya, A.; Myint, P.K.; Johnstone, A.M. Determinants of Undernutrition and Associated Factors of Low Muscle Mass and High Fat Mass among Older Men and Women in the Colombo District of Sri Lanka. Geriatrics 2022, 7, 26. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020026
Vijewardane SC, Balasuriya A, Myint PK, Johnstone AM. Determinants of Undernutrition and Associated Factors of Low Muscle Mass and High Fat Mass among Older Men and Women in the Colombo District of Sri Lanka. Geriatrics. 2022; 7(2):26. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020026
Chicago/Turabian StyleVijewardane, Samantha Chandrika, Aindralal Balasuriya, Phyo Kyaw Myint, and Alexandra M. Johnstone. 2022. "Determinants of Undernutrition and Associated Factors of Low Muscle Mass and High Fat Mass among Older Men and Women in the Colombo District of Sri Lanka" Geriatrics 7, no. 2: 26. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020026