
Factors Influencing Length of Stay and Discharge Destination of Patients with Hip Fracture Rehabilitating in a Private Care Setting


Abstract
:1. Introduction
- (i)
- The evaluation of UK hip fracture treatment is based on incomplete data. In 2015, only 57.3% patients with hip fractures had a rehabilitation record [15]. Patient characteristics, including socioeconomic status, are associated with an increased risk of hip fracture and might impact access to private rehabilitation [20]. Patients who utilise private rehabilitation are recorded as being discharged into care, disregarding whether they later return home [15]. These data are used by NHS commissioning groups to determine the clinical/cost effectiveness of treatment, while the National Hip Fracture Database also perform audits for service development recommendations. Incomplete data may camouflage inefficiency, resulting in poor quality treatment and impaired policy/management decisions.
- (ii)
- Anecdotal evidence indicates that private rehabilitation processes are obscured, private facilities may fail to appreciate the services required and new clients remain ignorant of likely progress and costings, while staff and family struggle to set realistic goals and/or meet discharge needs.
- (iii)
- The understanding of patient perspectives remains limited [16]. Anecdotal evidence shows that patients with hip fractures often expect a similar recovery experience to patients with hip replacements and are disappointed when theirs is longer and less restorative. Private patients’ chosen lengths of stay may reflect desirable treatment times; possibly, NHS rehabilitation is too short for full treatment benefit, causing greater long-term healthcare use [18].
2. Methods
2.1. Study Sample
2.2. Variables
Study Outcomes
2.3. Independent Variables
2.4. Bias and Reliability
2.5. Statistical Methods
3. Results
3.1. Sample Characteristics
3.2. Factors Affecting Length of Stay (LoS)
3.3. Factors Affecting Discharge Destination (DD)
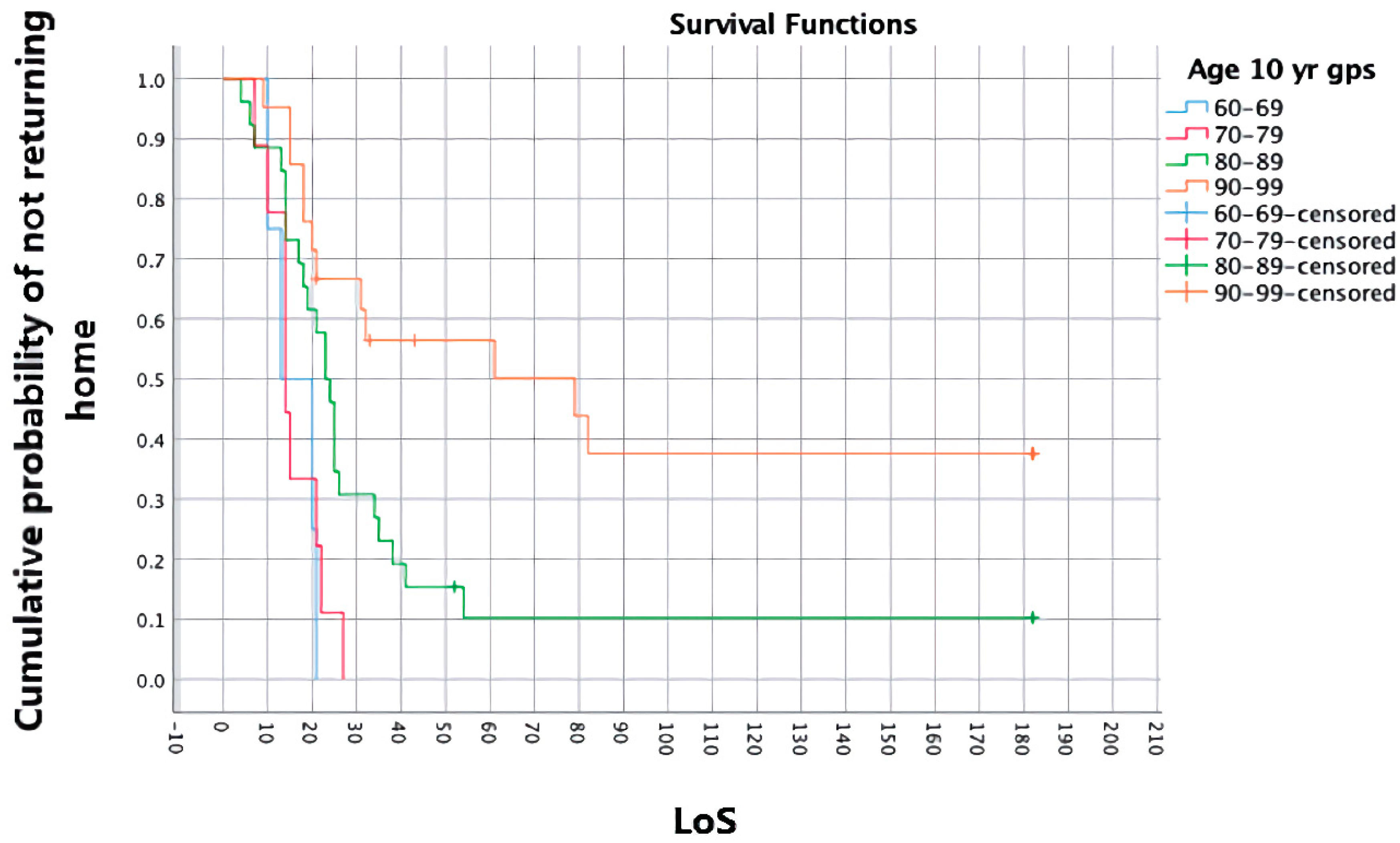
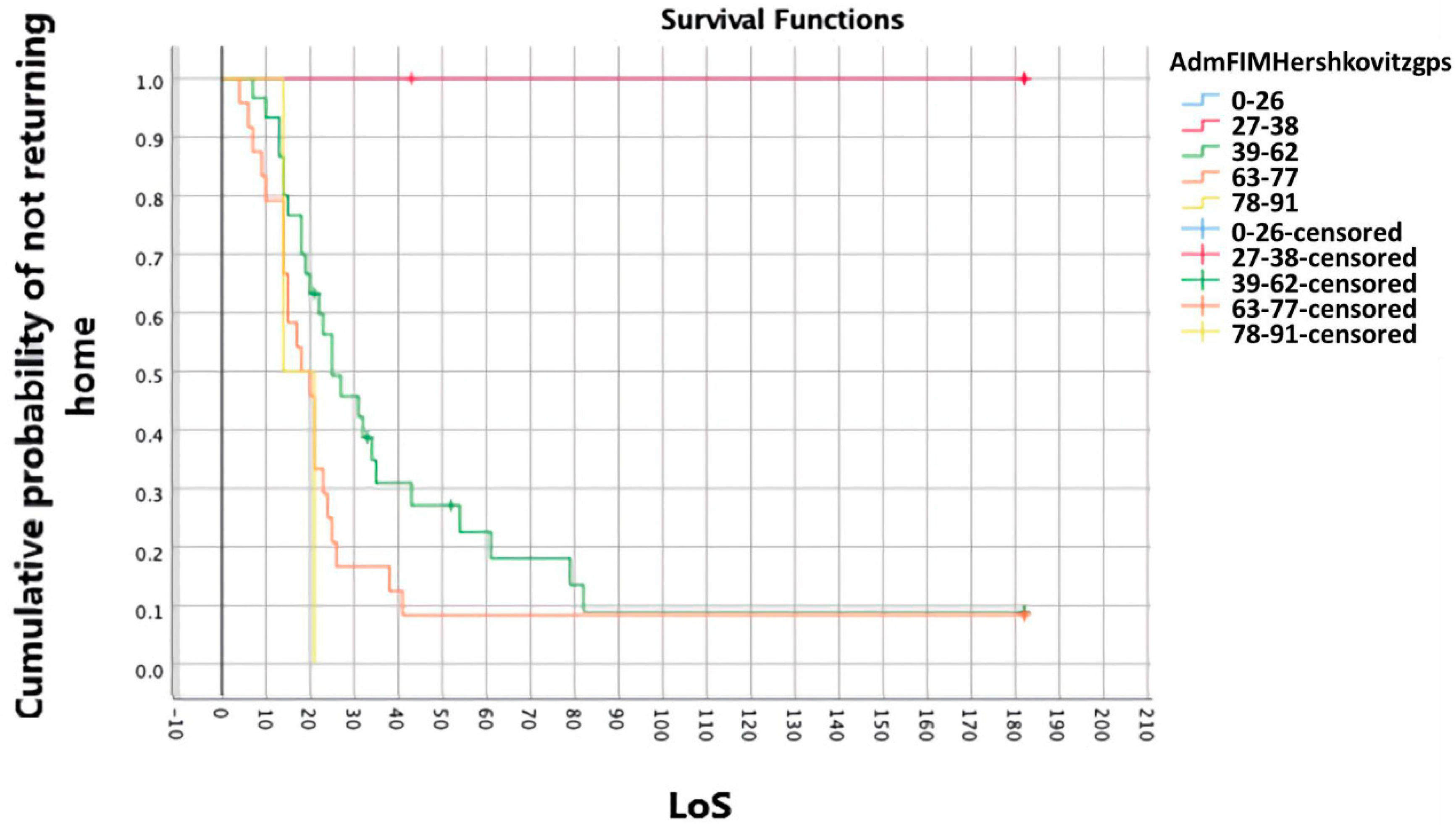
3.4. Survivor Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Royal College of Physicians. National Hip Fracture Database (NHFD) Annual Report 2017. Available online: https://nhfd.co.uk/files/2017ReportFiles/NHFD-AnnualReport2017.pdf (accessed on 16 August 2019).
- Royal College of Physicians. National Hip Fracture Database National Report 2011. Available online: https://www.nhfd.co.uk/20/hipfractureR.nsf/945b5efcb3f9117580257ebb0069c820/53e0ba402226ef27802578c500308c66/$FILE/NHFDNationalReport2011Final.pdf (accessed on 19 September 2018).
- Schulz, C.; Büchele, G.; Rehm, M.; Rothenbacher, D.; Roigk, P.; Rapp, K.; Günster, C.; König, H.-H.; Reber, K. Patient characteristics as indicator for care dependence after hip fracture: A retrospective cohort study using health insurance claims data from Germany. J. Am. Med. Dir. Assoc. 2019, 20, 451–455.e3. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Physicians. National Hip Fracture Database Annual Report 2018; RCP: London, UK, 2018; Available online: https://www.nhfd.co.uk/files/2018ReportFiles/NHFD-2018-Annual-Report-v101.pdf (accessed on 24 June 2019).
- Handoll, H.H.G.; Sherrington, C.; Mak, J.C.S. Interventions for improving mobility after hip fracture surgery in adults. Cochrane Database Syst. Rev. 2011, CD001704. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Physicians. Hip Fracture: Management—NICE Guideline. 2011. Available online: https://www.rcplondon.ac.uk/guidelines-policy/hip-fracture-management-nice-guideline (accessed on 17 April 2018).
- Oldmeadow, L.B.; Edwards, E.R.; Kimmel, L.; Kipen, E.; Robertson, V.J.; Bailey, M. No rest for the wounded: Early ambulation after hip surgery accelerates recovery. ANJ J. Surg. 2006, 76, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Gerety, M.B.; Soderholm-Difatte, V.; Winograd, C.H. Impact of prospective payment and discharge location on the outcome of hip fracture. J. Gen. Intern. Med. 1989, 4, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Dodds, C.; Foo, I.; Jones, K.; Singh, S.K.; Waldmann, C. Peri-operative care of elderly patents—An urgent need for change: A consensus statement to provide guidance for specialist and non-specialist anaesthetists. Periopr. Med. 2013, 2, 1–6. Available online: https://0-perioperativemedicinejournal-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/2047-0525-2-6 (accessed on 6 December 2017).
- Kondo, A.; Zierler, B.K.; Hagino, H. Relationship between the length of hospital stay after hip fracture surgery and ambulatory ability or mortality after discharge in Japan. Jpn. J. Nurs. Sci. 2010, 7, 96–107. [Google Scholar] [CrossRef]
- Kronborg, L.; Bandholm, T.; Palm, H.; Kehlet, H.; Kristensen, M.T. Physical activity in the acute ward following hip fracture surgery is associated with less fear of falling. J. Ageing Phys. Act. 2016, 24, 525–532. [Google Scholar] [CrossRef]
- Kristensen, M.T. Factors affecting functional prognosis of patients with hip fracture. Eur. J. Phys. Rehabil. Med. 2011, 47, 257–264. [Google Scholar]
- Royal College of Physicians. National Hip Fracture Database Annual Report 2016. RCP: London, UK. Available online: https://www.rcplondon.ac.uk/projects/outputs/national-hip-fracture-database-annual-report-2016 (accessed on 24 November 2018).
- Chartered Society of Physiotherapy. Hip Fracture Rehabilitation in Physiotherapy Practice: From Hospital to Home. 2018. Available online: https://www.csp.org.uk/system/files/publication_files/001563_Hip%20Fracture%20Standards_Full%20version_A4_V4_5-8-19_0.pdf (accessed on 28 July 2019).
- Wakeman, R. Improving Our Understanding of the Care and Rehabilitation of Hip Fracture Patients; Report; Royal College of Physicians: London, UK, 2017; Available online: https://www.rcplondon.ac.uk/news/improving-our-understanding-care-and-rehabilitation-hip-fracture-patients (accessed on 15 July 2019).
- Griffiths, F.; Mason, V.; Boardman, F.; Dennick, K.; Haywood, K.; Achten, J.; Parsons, N.; Griifin, X.; Costa, M. Evaluaing recovery following hip fracture: A qualitative interview study of what is important to patients. BMJ Open 2014, 5. Available online: https://0-bmjopen-bmj-com.brum.beds.ac.uk/content/5/1/e005406 (accessed on 17 August 2018).
- GK Strategy. A Private Choice: The Changing Face of the UK Health Market. 2017. Available online: https://gkstrategy.com/report/uk-health-a-private-choice/ (accessed on 20 July 2019).
- Mallinson, T.; Deutsch, A.; Bateman, J.; Tseng, H.-Y.; Manheim, L.; Almagor, O.; Heinemann, A.W. Comparison of discharge functional status after rehabilitation in skilled nursing, home health and medical rehabilitation facilities for patients after hip fracture. Arch. Phys. Med. Rehabil. 2014, 95, 209–217. [Google Scholar] [CrossRef]
- Cameron, L.D.; Kurrle, S.; March, L. Rehabilitation length of stay after hip fracture. Aust. N. Z. J. Med. 1998, 28, 480. [Google Scholar] [CrossRef] [PubMed]
- Richards, T.; Glendenning, A.; Benson, D.; Alexander, S.; Thati, S. The independent patient factors that affect length of stay following hip fractures. Ann. R. Coll. Surg. Engl. 2018, 100, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Newson, R.; Soljak, H.; Soljak, M. Associations between post-operative rehabilitation of hip fracture and outcomes: National database analysis. BMC Musculoskelet. Disord. 2018, 19. Available online: https://0-bmcmusculoskeletdisord-biomedcentral-com.brum.beds.ac.uk/articles/10.1186/s12891-018-2093-8 (accessed on 29 July 2019).
- Lu, M.; Sajobi, T.; Lucyk, K.; Lorenzetti, D.; Quan, H. Systematic review of risk adjustment models of hospital length of stay (LOS). Med. Care 2015, 53, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Clarke, A. Length of in-hospital stay and its relationship to quality of care. BMJ Qual. Saf. 2002, 11, 209–210. Available online: https://0-qualitysafety-bmj-com.brum.beds.ac.uk/content/11/3/209 (accessed on 28 July 2019). [CrossRef]
- Lindberg, L.; Ekstrom, W.; Hedstrom, M.; Flodin, L.; Lofgren, S.; Ryd, L. Changing caring behaviours in rehabilitation after a hip fracture—A tool for empowerment? Psychol. Health Med. 2017, 22, 663–672. [Google Scholar] [CrossRef]
- Dodds, T.A.; Martin, D.P.; Stolov, W.C.; Deyo, R.A. A validation of the functional independence measurement and its performance among rehabilitation inpatients. Arch. Phys. Med. Rehabil. 1993, 74, 531–536. [Google Scholar] [CrossRef]
- Petrella, R.J.; Overend, T.; Chesworth, B. FIM after hip fracture. Am. J. Phys. Med. Rehabil. 2002, 81, 639–644. [Google Scholar] [CrossRef]
- Gerrard, P.; Goldstein, R.; DiVita, M.A.; Slocum, C.; Ryan, C.M.; Mix, J.; Niewczyk, P.; Kazis, L.; Zafonte, R.; Schneider, J.C. Functional status and readmissions in unilateral hip fractures. Am. J. Manag. Care 2015, 21, e282–e287. Available online: https://www.ajmc.com/journals/issue/2015/2015-vol21-n4/functional-status-and-readmissions-in-unilateral-hip-fractures (accessed on 12 February 2019).
- Vadassery, S.J.; Kong, K.H.; Ho, W.M.L.; Seneviratna, A. Interview functional independence measure score: Self-reporting as a simpler alternative to multidisciplinary functional assessment. Singap. Med. J. 2019, 60, 199–201. [Google Scholar] [CrossRef]
- Bujang, M.A.; Baharum, N. A simplified guide to determination of sample size requirement for estimating the value of intraclass correlation coefficient: A review. Arch. Orofac. Sci. 2017, 12, 1–11. Available online: https://www.researchgate.net/publication/318788161_A_simplified_guide_to_determination_of_sample_size_requirements_for_estimating_the_value_of_intraclass_correlation_coefficient_A_review (accessed on 27 May 2019).
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, R.P.H.; Ng, B.H.P.; Cheung, L.R.C. Factors predicting rehabilitation outcomes of elderly patients with hip fractures. Hong Kong Med. J. 2008, 14, 209–215. [Google Scholar] [PubMed]
- Canadian Institute for Health Information. Factors Predicting Return Home from Inpatient Rehabilitation Following Hip Fracture Surgery. 2015. Available online: https://secure.cihi.ca/free_products?NRS_Hips_2015_EN_web.pdf (accessed on 18 April 2019).
- Ariza-Vega, P.; Jimenez-Moleon, J.J.; Kristensen, M.T. Change of residence and functional status within three months and one year following hip fracture surgery. Disabil. Rehabil. 2012, 36, 685–690. Available online: https://0-doi-org.brum.beds.ac.uk/10.3109/09638288.2013.813081 (accessed on 27 August 2019).
- Hershkovitz, A.; Kaladariov, Z.; Hermush, V.; Weiss, R.; Brill, S. Factors affecting short-term rehabilitation outcomes of disabled elderly patients with proximal hip fracture. Arch. Phys. Med. Rehabil. 2007, 88, 916–921. [Google Scholar] [CrossRef]
- Hayashi, H.; Iwai, M.; Matsuoka, H.; Nakashima, D.; Nakamura, S.; Kubo, A.; Tomiyama, N. Factors affecting the discharge destination of hip fracture patient who live alone and have been admitted to an inpatient rehabilitation unit. J. Phys. Ther. Sci. 2016, 28, 1228–1232. [Google Scholar] [CrossRef] [Green Version]
- Cree, A.K.; Nade, S. How to predict return to the community after fracture of proximal femur in the elderly. Aust. N. Z. J. Surg. 1999, 69, 723–725. [Google Scholar] [CrossRef]
- Ireland, A.W.; Kelly, P.J.; Cumming, R.G. Total hospital stay for hip fracture measuring the variations due to pre-fracture residence, rehabilitation, complications and comorbidities. BMC Health Serv. Res. 2015, 15, 17. Available online: https://0-doi-org.brum.beds.ac.uk/10.1186/s12913-015-0697-3 (accessed on 6 April 2019).
- Wang, C.Y.; Graham, J.E.; Karmarkar, A.M.; Reistetter, T.A.; Protas, E.J.; Ottenbacher, K.J. FIM motor scores for classifying community discharge after inpatient rehabilitation for hip fracture. PM&R 2014, 6, 493–497. [Google Scholar] [CrossRef]
- Edelstein, D.M.; Aharanoff, G.B.; Karp, A.; Capla, E.L.; Zuckerman, J.D.; Koval, K.J. Effect of postoperative delirium on outcome after hip fracture. Clin. Orthop. Relat. Res. 2004, 422, 195–200. [Google Scholar] [CrossRef]
- Everink, I.H.J.; van Haastregt, J.C.M.; van Hoof, S.J.M.; Schols, J.M.G.A.; Kempen, G.I.J.M. Factors influencing home discharge after inpatient rehabilitation of older patients: A systematic review. BMC Geriatr. 2016, 16, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Y.-L.; Saw, H.-M. Hip fractures: A review of predictors affecting FIM, ambulation & rehabilitation length of stay during inpatient rehabilitation at Singapore General Hospital. Proc. Singap. Healthc. 2016, 25, 13–18. [Google Scholar]
- Kolt, G.S.; McEvoy, J.F. Adherence to rehabilitation in patients with low back pain. Man. Ther. 2003, 8, 110–116. [Google Scholar] [CrossRef]
- Quah, C.; Boulton, C.; Moran, C. The influence of socioeconomic status on the incidence, outcome and mortality of fractures of the hip. J. Bone Joint Surg. 2011, 93-B, 801–805. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Physicians. Recovering After a Hip Fracture: Helping People Understand Physiotherapy in the NHS; Physiotherapy ‘Hip Sprint’ Audit Report 2017; RCP: London, UK, 2018; Available online: https://www.fffap.org.uk/FFFAP/landing.nsf/phfsa.html (accessed on 20 July 2019).
- Amundson, J.; Brunner, A.; Huffman, S. FIM scores as an indicator of length of stay and discharge destimation in CVA patients: A retroactive outcomes study. 2004. Available online: https://www.semanticscholar.org/paper/FIM-Scores-as-an-Indicator-of-Length-of-Stay-and-in-Amundson-Brunner/3e8048bc33e1dd94e4beeacd56b7a08ae3072650 (accessed on 18 May 2018).
- Auais, M.A.; Eilayyan, O.; Mayo, N.E. Extended exercise rehabilitation after hip fracture improves patients’ physical function: A systematic review and meta-analysis. Phys. Ther. 2012, 92, 1437–1451. [Google Scholar] [CrossRef] [Green Version]
- McGilton, K.S.; Mahomed, N.; Davis, A.M.; Flannery, J.; Calabrese, S. Outcomes for older adults in an inpatient rehabilitation facility following hip fracture surgery. Arch. Gerontol. Geriatr. 2009, 49, e23–e31. [Google Scholar] [CrossRef]
- Kiely, D.K.; Bergmann, M.A.; Jones, R.N.; Murphy, K.M.; Orav, E.J.; Marcantonio, E.R. Characteristics associated with delirium persistence among newly admitted post-acute facility patients. J. Gerentol. Biol. Sci. Med. Sci. 2004, 59, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Ringdal, G.I.; Ringdal, K.; Juliebo, V.; Wyller, T.B.; Hjermstad, M.J.; Loge, J.H. Using the mini- mental state examination to screen for delirium in elderly patients with hip fracture. Dement. Geriatr. Cogn. Disord. 2011, 32, 394–400. [Google Scholar] [CrossRef]
- Bellilli, G.; Morandi, A.; Davis, D.H.J.; Mazzola, P.; Turco, R.; Gentile, S.; Ryan, T.; Cash, H.; Guerini, F.; Torpilliesi, T.; et al. Validation of the 4AT, a new instrument for rapid delirium screening: A study in 234 hospitalised older people. Age Ageing 2014, 43, 496–502. [Google Scholar] [CrossRef] [Green Version]
- MacLullich, A.M.J. 4AT Rapid Clinical Test for Delirium. 2011. Available online: https://www.the4at.com/authors (accessed on 16 August 2019).
- Harrell, M.C.; Bradley, M.A. Data Collection Methods: Semi-Structured Interviews and Focus Groups; RAND Corporation: Santa Monica, CA, USA, 2009; Available online: https://www.rand.org/pubs/technical_reports/TR718.html (accessed on 16 August 2019).
- Sajobi, T.; Lu, M.; Jiang, J.; Quan, H. Improving the accuracy of length of stay risk adjustment models using linked data. Int. J. Popul. Data Sci. 2017, 1, 360. Available online: https://ijpds.org/article/view/382/363 (accessed on 5 July 2019). [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variable | All | Home (DD = 1) | Long-Term Care (DD = 2) |
|---|---|---|---|
| Age, median (IQR) | 87.0 | 86.0 (8) | 92.5 (5.3) |
| Gender, n = male (%) | 18 (29.5) | 12 (66.7) | 6 (50) |
| Comorbidities, median (IQR) | 4.0 | 3.0 (2.25) | 5.5 (3) |
| Delirium, n = Yes (%) | 11 (18) | 6 | 5 |
| Fracture treatment, n (%) | |||
| Fixation | 12 (19.7) | 10 (20.4) | 2 (16.7) |
| Mobile fixation | 20 (32.8) | 16 (32.7) | 4 (33.3) |
| Arthroplasty | 27 (44.3) | 22 (44.9) | 5 (41.7) |
| Conservative | 2 (3.3) | 1 (2.0) | 1 (8.3) |
| Latency, median (IQR) (days fracture to treatment) | 1.0 (1.0) | 1.0 (1.0) | 2.0 (7.0) |
| LoSacute, median (IQR) | 15.0 (10.5) | 15.0 (9.5) | 19.5 (25.5) |
| FIMpre-fracture, median (IQR) | 88.0 (7.0) | 89.0 (5.0) | 81.0 (22.0) |
| FIMadmission, median (IQR) | 61.0 (24.0) | 62.0 (9.5) | 46.0 (21.75) |
| FIM%change, median (IQR) | 29.7 (11.7) | 29.7 (11.1) | 32.0 (30.1) |
| Home support, n (%) | |||
| Live-in | 23 (37.7) | 18 (36.7) | 5 (41.7) |
| Visiting | 28 (45.9) | 23 (46.9) | 5 (41.7) |
| Alone | 9 (14.8) | 8 (16.3) | 1 (8.3) |
| Dependent spouse | 1 (1.6) | 0 (0.0) | 1 (8.3) |
| Stairs, n = Yes (%) | 36 (59.0) | 29 (59.2) | 7 (58.3) |
| Physio sessions/wk, median (IQR) | 5 (2.0) | 5 (2.0) | 5 (1.75) |
| Length of stay (LoS), median (IQR) | 22.0 (27.5) | 20.0 (12.5) | 182.0 (136.75) |
| Independent Variable | Tests | Outcome | |
|---|---|---|---|
| LoS | DD | ||
| Age | Spearman’s r/Mann-W U | cc 0.365, p = 0.004 ** | U = 146.500, p = 0.007 ** |
| Gender | Mann–W U/Chi2 (2 × 2) | U = 298.00, p = 0.158 | c2 = 3.016, p = 0.082 |
| Co-morbidities | Mann–W U/Chi2 (2 × 2) | cc 0.332, p = 0.009 ** | c2 = 11.680, p = 0.020 * |
| Delirium | Mann–W U/Chi2 (2 × 2) | U = 197.00, p = 0.143 | c2 = 5.645, p = 0.018 * |
| Fracture treatment | Kruskal–Wallis H/Chi2 (r × c) | p = 0.251 | c2 = 1.257, p = 0.739 |
| Latency | Spearman’s r/Mann–W U | cc −0.085, p = 0.521 | U = 208.5, p = 0.431 |
| LoSacute | Spearman’s r/Mann–W U | cc 0.220, p = 0.088 | U = 181.500, p = 0.041 * |
| FIMpre-fracture | Spearman’s r/Mann–W U | cc 0.242, p = 0.062 | U = 95.500, p = 0.000 ** |
| FIMadmission | Spearman’s r/Mann–W U | cc 0.414, p = 0.001 ** | U = 95.500, p = 0.000 ** |
| FIM%change | Spearman’s r/Mann–W U | cc 0.299, p = 0.019 * | U = 217.00, p = 0.162 |
| Stairs | Mann–W U/Chi2 (2 × 2) | U = 429.00, p = 0.758 | c2 = 0.003, p = 0.957 |
| Support | Kruskal–Wallis H/Chi2 (r × c) | p = 0.440 | c2 = 4.621, p = 0.536 |
| Treatment/wk | Spearman’s r/Mann–W U | cc 0.170, p = 0.191 | U = 264.500, p = 0.839 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thornburgh, Z.; Samuel, D. Factors Influencing Length of Stay and Discharge Destination of Patients with Hip Fracture Rehabilitating in a Private Care Setting. Geriatrics 2022, 7, 44. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020044
Thornburgh Z, Samuel D. Factors Influencing Length of Stay and Discharge Destination of Patients with Hip Fracture Rehabilitating in a Private Care Setting. Geriatrics. 2022; 7(2):44. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020044
Chicago/Turabian StyleThornburgh, Zoe, and Dinesh Samuel. 2022. "Factors Influencing Length of Stay and Discharge Destination of Patients with Hip Fracture Rehabilitating in a Private Care Setting" Geriatrics 7, no. 2: 44. https://0-doi-org.brum.beds.ac.uk/10.3390/geriatrics7020044