Malignant Arrhythmic Mitral Valve Prolapse: A Continuum of Clinical Challenges from Diagnosis to Risk Stratification and Patient Management


{kind=link}
{kind=link}
Abstract
:1. Introduction
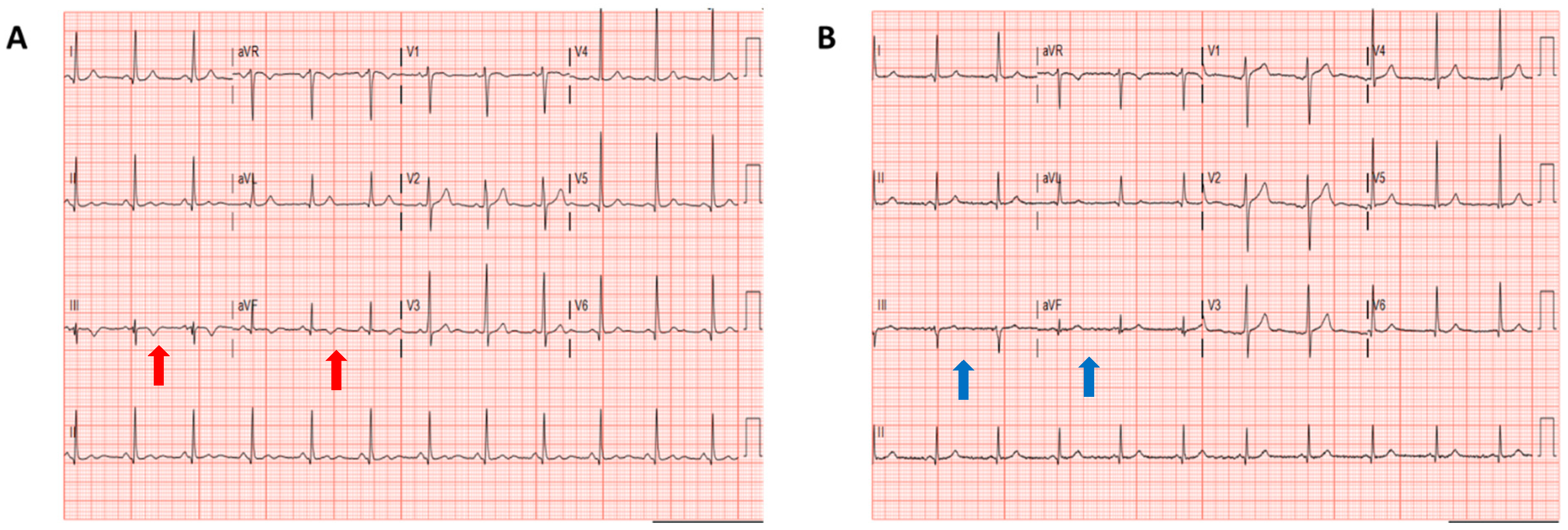
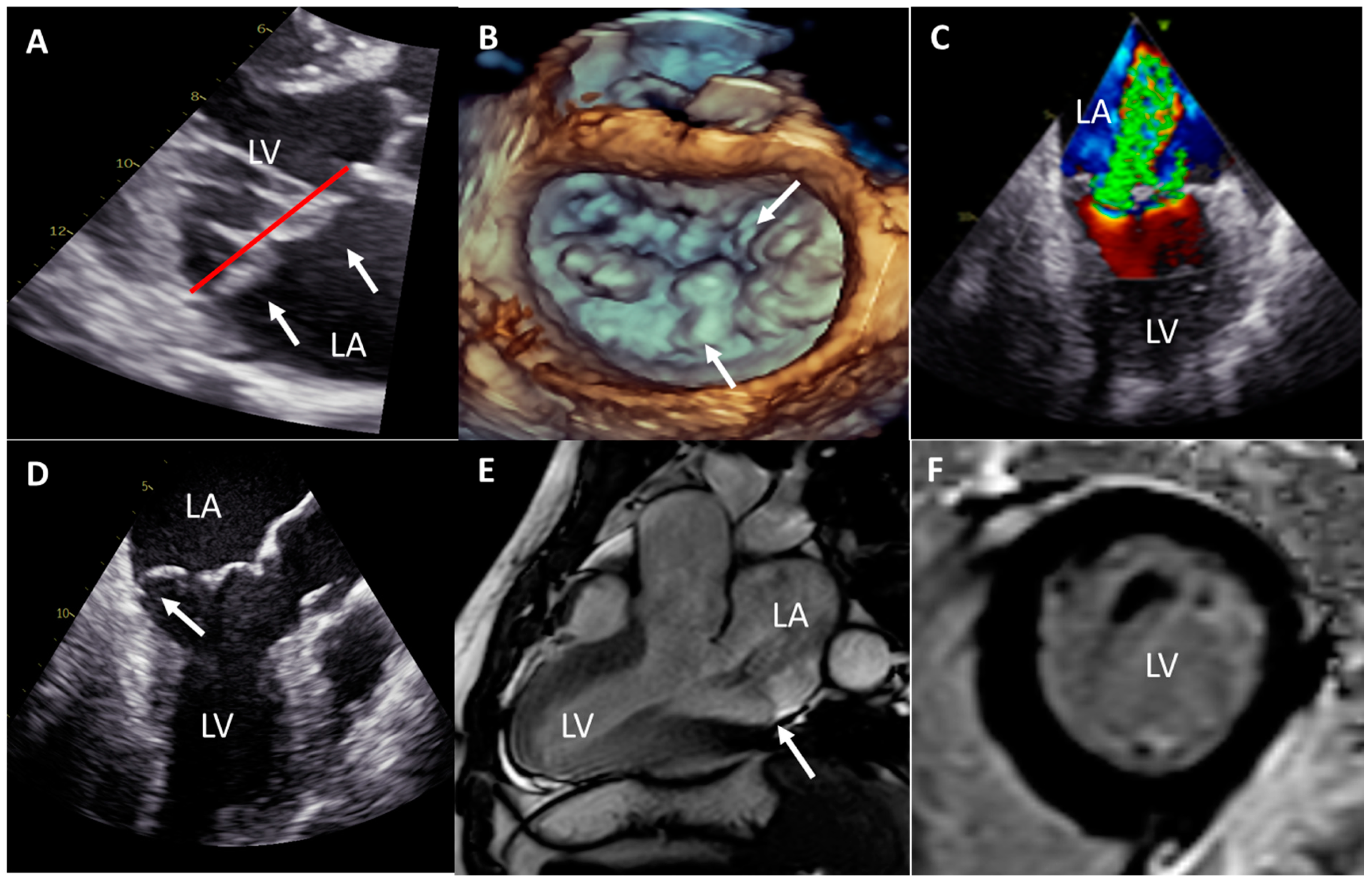
2. Case Report
3. Discussion
3.1. Risk Stratification for Ventricular Arrhythmias in MVP Patients
3.2. How to Improve Risk Stratification for Ventricular Arrhythmias in MVP Patients
3.3. Therapeutic Options for Ventricular Arrhythmias in MVP Patients
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishimura, R.A.; McGoon, M.D.; Shub, C.; Miller, F.A.; Ilstrup, D.M.; Tajik, A. Echocardiographically Documented Mitral-Valve Prolapse. N. Engl. J. Med. 1985, 313, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Grigioni, F.; Enriquez-Sarano, M.; Ling, L.H.; Bailey, K.R.; Seward, J.B.; Tajik, A.; Frye, R.L. Sudden death in mitral regurgitation due to flail leaflet. J. Am. Coll. Cardiol. 1999, 34, 2078–2085. [Google Scholar] [CrossRef] [Green Version]
- Sriram, C.S.; Syed, F.F.; Ferguson, M.E.; Johnson, J.N.; Enriquez-Sarano, M.; Cetta, F.; Cannon, B.C.; Asirvatham, S.J.; Ackerman, M.J. Malignant Bileaflet Mitral Valve Prolapse Syndrome in Patients With Otherwise Idiopathic Out-of-Hospital Cardiac Arrest. J. Am. Coll. Cardiol. 2013, 62, 222–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, H.; Ha, F.J.; Teh, A.W.; Calafiore, P.; Jones, E.F.; Johns, J.; Koshy, A.N.; O’Donnell, D.; Hare, D.L.; Farouque, O.; et al. Mitral Valve Prolapse and Sudden Cardiac Death: A Systematic Review. J. Am. Heart Assoc. 2018, 7, e010584. [Google Scholar] [CrossRef] [Green Version]
- Nordhues, B.D.; Siontis, K.C.; Scott, C.J.; Nkomo, V.T.; Ackerman, M.J.; Asirvatham, S.J.; Noseworthy, P.A. Bileaflet Mitral Valve Prolapse and Risk of Ventricular Dysrhythmias and Death. J. Cardiovasc. Electrophysiol. 2016, 27, 463–468. [Google Scholar] [CrossRef]
- Muthukumar, L.; Jahangir, A.; Jan, M.F.; Moreno, A.C.P.; Khandheria, B.K.; Tajik, A.J. Association between Malignant Mitral Valve Prolapse and Sudden Cardiac Death: A Review. JAMA Cardiol. 2020, 5, 1053–1061. [Google Scholar] [CrossRef]
- Essayagh, B.; Sabbag, A.; Antoine, C.; Benfari, G.; Yang, L.-T.; Maalouf, J.; Asirvatham, S.; Michelena, H.; Enriquez-Sarano, M. Presentation and Outcome of Arrhythmic Mitral Valve Prolapse. J. Am. Coll. Cardiol. 2020, 76, 637–649. [Google Scholar] [CrossRef]
- Narayanan, K.; Uy-Evanado, A.; Teodorescu, C.; Reinier, K.; Nichols, G.A.; Gunson, K.; Jui, J.; Chugh, S.S. Mitral valve prolapse and sudden cardiac arrest in the community. Heart Rhythm. 2016, 13, 498–503. [Google Scholar] [CrossRef] [Green Version]
- Wijngaarden, A.L.; Riva, M.; Hiemstra, Y.L.; Bijl, P.; Fortuni, F.; Bax, J.J.; Delgado, V.; Marsan, N.A. Parameters associated with ventricular arrhythmias in mitral valve prolapse with significant regurgitation. Heart 2020, in press. [Google Scholar] [CrossRef]
- Dejgaard, L.A.; Skjolsvik, E.T.; Lie, O.H.; Ribe, M.; Stokke, M.K.; Hegbom, F.; Scheirlynck, E.S.; Gjertsen, E.; Andresen, K.; Helle-Valle, T.M.; et al. The Mitral Annulus Disjunction Arrhythmic Syn-drome. J. Am. Coll. Cardiol. 2018, 72, 1600–1609. [Google Scholar] [CrossRef]
- Alqarawi, W.; Birnie, D.H.; Burwash, I.G. Mitral valve repair results in suppression of ventricular arrhythmias and normalization of repolarization abnormalities in mitral valve prolapse. Heart Case Rep. 2018, 4, 191–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avierinos, J.-F.; Detaint, D.; Messika-Zeitoun, D.; Mohty, D.; Enriquez-Sarano, M. Risk, Determinants, and Outcome Implications of Progression of Mitral Regurgitation After Diagnosis of Mitral Valve Prolapse in a Single Community. Am. J. Cardiol. 2008, 101, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Marra, M.P.; Rizzo, S.; De Lazzari, M.; Giorgi, B.; Cipriani, A.; Frigo, A.; Rigato, I.; Migliore, F.; Pilichou, K.; et al. Arrhythmic Mitral Valve Prolapse and Sudden Cardiac Death. Circulation 2015, 132, 556–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guglielmo, M.; Fusini, L.; Muscogiuri, G.; Baessato, F.; Loffreno, A.; Cavaliere, A.; Rizzon, G.; Baggiano, A.; Rabbat, M.G.; Muratori, M.; et al. T1 mapping and cardiac magnetic resonance feature tracking in mitral valve prolapse. Eur. Radiol. 2020, 1–10, in press. [Google Scholar] [CrossRef] [PubMed]
- Bui, A.H.; Roujol, S.; Foppa, M.; Kissinger, K.V.; Goddu, B.; Hauser, T.H.; Zimetbaum, P.J.; Ngo, L.H.; Manning, W.J.; Nezafat, R.; et al. Diffuse myocardial fibrosis in patients with mitral valve prolapse and ventricular arrhythmia. Heart 2017, 103, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, D.D.; Levy, D.; Garrison, R.J.; Castelli, W.P.; Kligfield, P.; Devereux, R.B.; Anderson, S.J.; Kannel, W.B.; Feinleib, M. Mitral valve prolapse in the general population. 3. Dysrhythmias: The Framingham Study. Am. Heart J. 1983, 106, 582–586. [Google Scholar] [CrossRef]
- Hiemstra, Y.L.; Van Wijngaarden, A.; Bos, M.W.; Schalij, M.J.; Klautz, R.J.; Bax, J.J.; Delgado, V.; Barge-Schaapveld, D.Q.; Marsan, N.A. Familial occurrence of mitral regurgitation in patients with mitral valve prolapse undergoing mitral valve surgery. Eur. J. Prev. Cardiol. 2020, 27, 272–280. [Google Scholar] [CrossRef] [Green Version]
- Wijngaarden, A.L.; Hiemstra, Y.L.; Koopmann, T.T.; Ruivenkamp, C.A.L.; Aten, E.; Schalij, M.J.; Bax, J.J.; Delgado, V.; Barge-Schaapveld, D.Q.C.M.; Marsan, N.A. Identification of known and unknown genes associated with mitral valve prolapse using an exome slice methodology. J. Med. Genet. 2020, 57, 843–850. [Google Scholar] [CrossRef]
- Bains, S.; Tester, D.J.; Asirvatham, S.J.; Noseworthy, P.A.; Ackerman, M.J.; Giudicessi, J.R. A Novel Truncating Variant in FLNC-Encoded Filamin C May Serve as a Proarrhythmic Genetic Substrate for Arrhythmogenic Bileaflet Mitral Valve Prolapse Syndrome. Mayo Clin. Proc. 2019, 94, 906–913. [Google Scholar] [CrossRef] [Green Version]
- Scheirlynck, E.; Dejgaard, L.A.; Skjolsvik, E.; Lie, O.H.; Motoc, A.; Hopp, E.; Tanaka, K.; Ueland, T.; Ribe, M.; Collet, C.; et al. Increased levels of sST2 in patients with mitral annulus disjunction and ventricular arrhythmias. OpenHeart 2019, 6, e001016. [Google Scholar] [CrossRef]
- Syed, F.F.; Ackerman, M.J.; McLeod, C.J.; Kapa, S.; Mulpuru, S.K.; Sriram, C.S.; Cannon, B.C.; Asirvatham, S.J.; Noseworthy, P.A. Sites of Successful Ventricular Fibrillation Ablation in Bileaflet Mitral Valve Prolapse Syndrome. Circ. Arrhythmia Electrophysiol. 2016, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pocock, W.A.; Barlow, J.B.; Marcus, R.H.; Barlow, C.W. Mitral valvuloplasty for life-threatening ventricular arrhythmias in mitral valve prolapse. Am. Heart J. 1991, 121, 199–202. [Google Scholar] [CrossRef]
- Vaidya, V.R.; DeSimone, C.V.; Damle, N.; Naksuk, N.; Syed, F.F.; Ackerman, M.J.; Ponamgi, S.P.; Nkomo, V.T.; Suri, R.M.; Noseworthy, P.A.; et al. Reduction in malignant ventricular arrhythmia and appropriate shocks following surgical correction of bileaflet mitral valve prolapse. J. Interv. Card. Electrophysiol. 2016, 46, 137–143. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yedidya, I.; van Wijngaarden, A.L.; Ajmone Marsan, N. Malignant Arrhythmic Mitral Valve Prolapse: A Continuum of Clinical Challenges from Diagnosis to Risk Stratification and Patient Management. J. Cardiovasc. Dev. Dis. 2021, 8, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010002
Yedidya I, van Wijngaarden AL, Ajmone Marsan N. Malignant Arrhythmic Mitral Valve Prolapse: A Continuum of Clinical Challenges from Diagnosis to Risk Stratification and Patient Management. Journal of Cardiovascular Development and Disease. 2021; 8(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010002
Chicago/Turabian StyleYedidya, Idit, Aniek L. van Wijngaarden, and Nina Ajmone Marsan. 2021. "Malignant Arrhythmic Mitral Valve Prolapse: A Continuum of Clinical Challenges from Diagnosis to Risk Stratification and Patient Management" Journal of Cardiovascular Development and Disease 8, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010002