Critical Assessment of the Concepts and Misconceptions of the Cardiac Conduction System over the Last 100 Years: The Personal Quest of Robert H. Anderson



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Atrioventricular Nodal Bypass Tracts
3.2. The Pathways Described by Ivan Mahaim
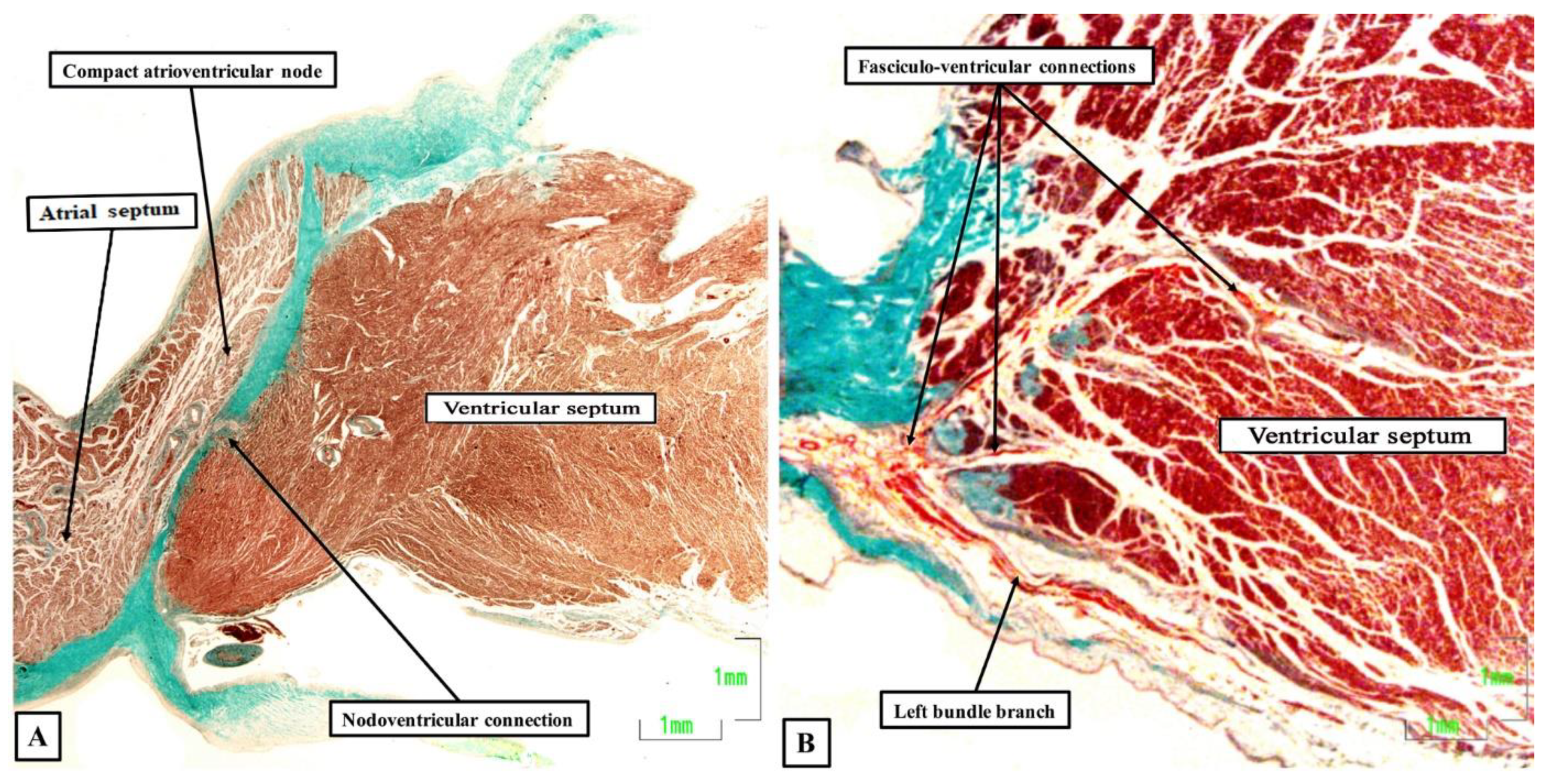
3.2.1. Fasciculo-Ventricular and Nodo-Ventricular Pathways
3.2.2. Accessory Atrioventricular Node or Atriofascicular Pathway
3.3. Specialized Tracts for Internodal Atrial Conduction
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tawara, S. Das Reitzleitungssystem Des Saugetierherzens: Eine Anatomisch Histologische Studie Uber Das Atrioventrikularbundel und Die Purkinjeschen Faden; Gustav Fischer: Jena, Germany, 1906; pp. 135–136. [Google Scholar]
- Keith, A.; Flack, M. The form and nature of the muscular connections between the primary divisions of the vertebrate heart. J. Anat. Physiol. 1907, 41, 172–189. [Google Scholar] [PubMed]
- Aschoff, L. Bericht über die Untersuchungen des Herrn Dr. Tawara, die Brückenfasern betreffend, und Demonstration der zugehörigen mikroskopischen Präparate. Zentralbl. Physiol. 1905, 19, 298–301. [Google Scholar]
- Mönckeberg, J.G. Beitrage zur normalen und pathologischen Anatomie des Herzens. Verh. Dtsch. Pathol. Ges 1910, 14, 64–71. [Google Scholar]
- Anderson, R.H.; Becker, A.E.; Brechenmacher, C.; Davies, M.J.; Rossi, L. Ventricular pre-excitation. A proposed nomenclature for its substrates. Eur. J. Cardiol. 1975, 3, 27–36. [Google Scholar] [PubMed]
- Anderson, R.H.; Becker, A.E.; Wenink, A.C.G.; Janse, M.J. The development of the cardiac specialized tissue. In The Conduction System of the Heart–Structure, Function and Clinical Implications; Wellens, H.J.J., Lie, K., Janse, M.J., Eds.; HE Stenfert Kroese B.V.: Leiden, The Netherlands, 1976; pp. 3–28. [Google Scholar]
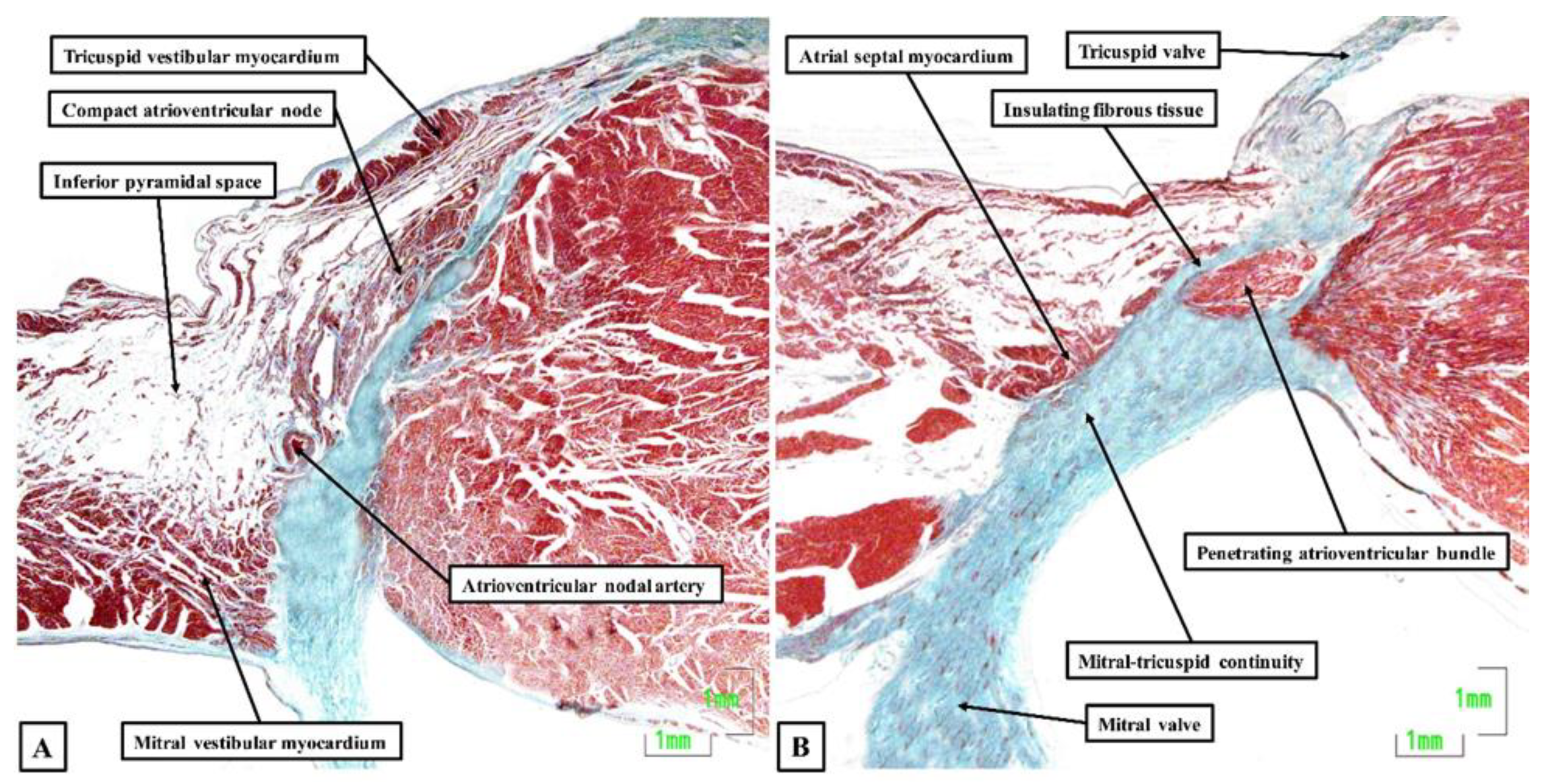
- Becker, A.E.; Anderson, R.H. Morphology of the human atrioventricular junctional area. In The Conduction System of the Heart–Structure, Function and Clinical Implications; Wellens, H.J.J., Lie, K., Janse, M.J., Eds.; HE Stenfert Kroese B.V.: Leiden, The Netherlands, 1976; pp. 263–286. [Google Scholar]
- James, T. Morphology of the human atrioventricular node, with remarks pertinent to its electrophysiology. Am. Heart. J. 1961, 62, 756. [Google Scholar] [CrossRef]
- Brechenmacher, C.; Laham, J.; Iris, L.; Gerbaux, A.; Lenegre, J. Histological study of abnormal conduction pathways in the Wolff-Parkinson-White syndrome and Lown-Ganong-Levine syndrome. Arch. Mal. Coeur. Vaiss. 1974, 67, 507–519. [Google Scholar]
- Brechenmacher, C. Atrio-His bundle tracts. Br. Heart J. 1975, 37, 853–855. [Google Scholar] [CrossRef] [Green Version]
- Scherf, D.; Cohen, J. The Atrioventricular Node and Selected Cardiac Arrhythmias; Grune & Straton: New York, NY, USA, 1964; pp. 1–466. [Google Scholar]
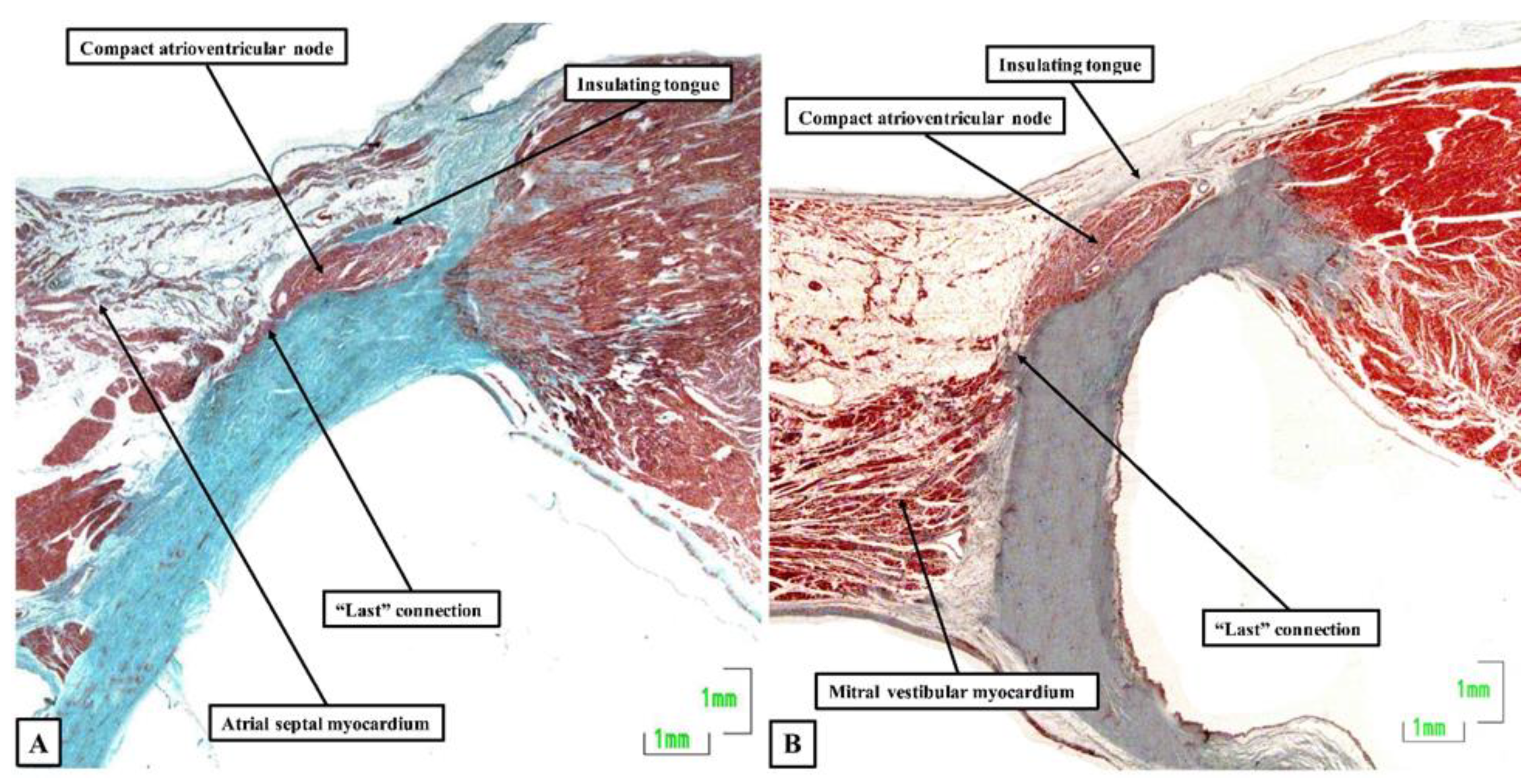
- Anderson, R.H.; Sanchez-Quintana, D.; Mori, S.; Cabrera, J.A.; Back Sternick, E. Re-evaluation of the structure of the atrioventricular node and its connections with the atrium. Europace 2020, 22, 821–830. [Google Scholar] [CrossRef]
- Katritsis, D.G.; Becker, A. The circuit of atrioventricular nodal reentrant tachycardia: A proposal. Heart Rhythm 2007, 4, 1354–1360. [Google Scholar] [CrossRef]
- Mahaim, I.; Benatt, A. Nouvelles recherches sur les connexions supérieures de la branche gauche du faisceau de His-Tawara avec cloison interventriculaire. Cardiologia 1938, 1, 61–76. [Google Scholar] [CrossRef]
- Mahaim, I. Kent’s fibers and the A-V paraspecific conduction through the upper connections of the bundle of His-Tawara. Am. Heart J. 1947, 33, 6553. [Google Scholar] [CrossRef]
- Anderson, R.H.; Bouton, J.; Burrow, C.T.; Smith, A. Sudden death in infancy: A study of the cardiac specialized tissue. Br. Med. J. 1974, 2, 135–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellens, H.J.J. Electrical Stimulation of the Heart in the Study and Treatment of Tachycardias; University Park Press: Baltimore, MD, USA, 1971; pp. 97–109. [Google Scholar] [CrossRef] [Green Version]
- Gmeiner, R.; Keung, C.; Hammer, I.; Becker, A.E. Tachycardia caused by an accessory nodoventricular tract: A clinico-pathologic correlation. Eur. Heart J. 1984, 5, 233–242. [Google Scholar] [CrossRef] [PubMed]
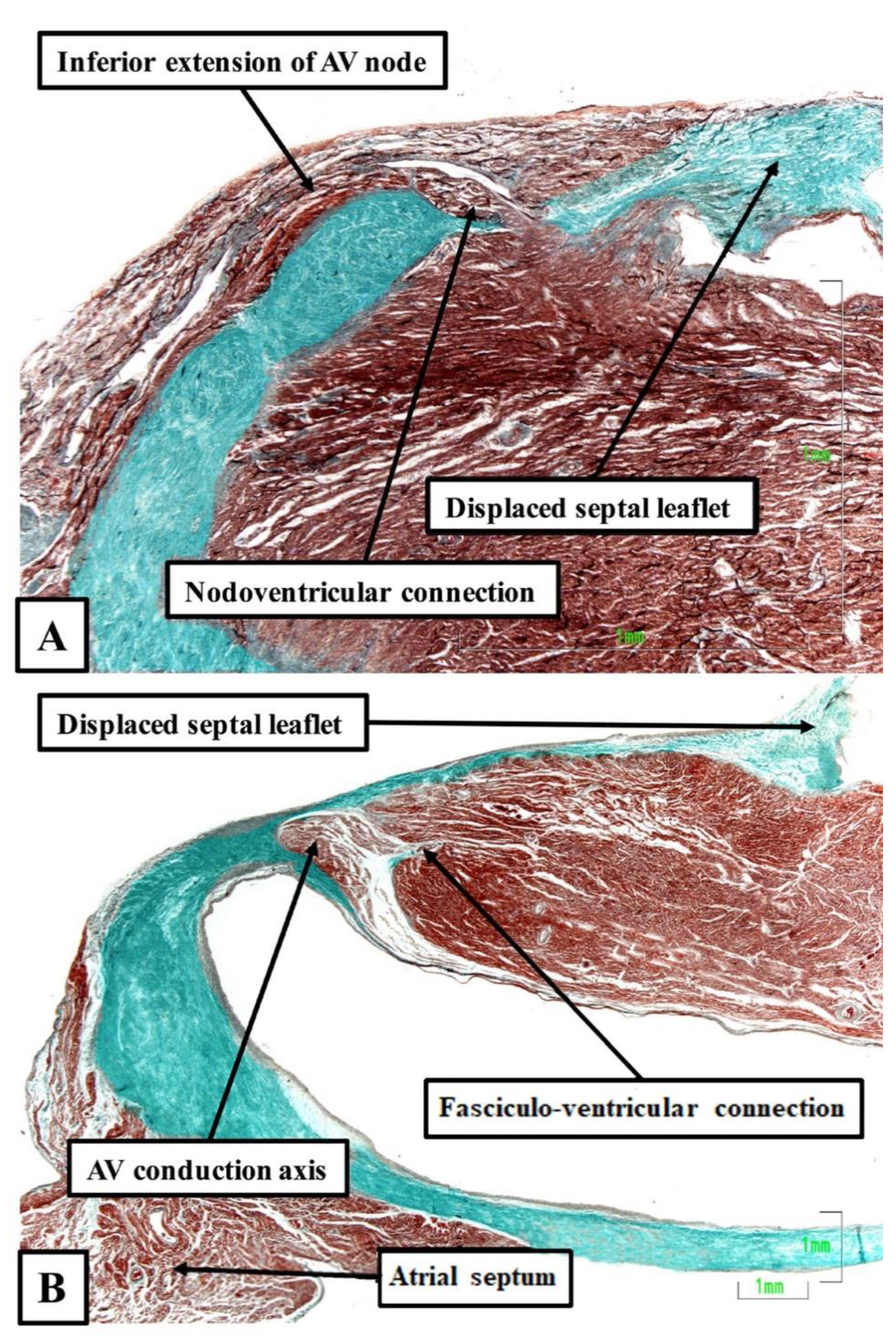
- Sánchez-Quintana, D.; Cabrera, J.A.; Picazo-Angelin, B.; Cabrera, A.; Anderson, R.H. Histological examination of the potential arrhythmic substrates in the setting of Ebstein’s malformation. J. Anat. 2020, 237, 155–165. [Google Scholar] [CrossRef]
- Becker, A.E.; Anderson, R.H.; Durrer, D.; Wellens, H.J.J. The anatomical substrates of Wolff Parkinson White Syndrome. A clinicopathologic correlation in seven patients. Circulation 1978, 57, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Gillette, P.C.; Garson, A.; Cooley, D.A.; McNamara, D.G. Prolonged and decremental anterograde conduction properties in right anterior accessory connections: Wide QRS antidromic tachycardia of left bundle branch block pattern without Wolff-Parkinson-White configuration in sinus rhythm. Am. Heart J. 1982, 103, 66–74. [Google Scholar] [CrossRef]
- Klein, G.J.; Guiraudon, G.M.; Kerr, C.R.; Sharma, A.D.; Yee, R.; Szabo, T.; Wah, J.A. “Nodoventricular” accessory pathway: Evidence for a distinct accessory atrioventricular pathway with atrioventricular node-like properties. J. Am. Coll. Cardiol. 1988, 11, 1035–1040. [Google Scholar] [CrossRef] [Green Version]
- James, T.N. The connecting pathways between the sinus node and A-V node and between the right and left atrium in the human heart. Am. Heart J. 1963, 66, 498–508. [Google Scholar] [CrossRef]
- James, T.N. The internodal pathways of the human heart. Prog. Cardiovasc. Dis. 2001, 43, 495–535. [Google Scholar] [CrossRef]
- Dürrer, D.; van Dam, R.T.; Freud, G.E.; Janse, M.J.; Meijler, F.L.; Arzbaecher, R.C. Total excitation of the isolated human heart. Circulation 1970, 61, 899–912. [Google Scholar] [CrossRef] [Green Version]
- Janse, M.J.; Anderson, R.H. Specialized internodal atrial pathways- fact or fiction? Eur. J. Cardiol. 1974, 2, 117–136. [Google Scholar]
- Spach, M.S. Anisotropy of cardiac tissue: A major determinant of conduction? J. Cardiovasc. Electrophysiol. 1999, 10, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.H.; Sanchez-Quintana, D.; Mori, S.; Lokhandwala, Y.; Correa, F.S.; Wellens, H.J.J.; Back Sternick, E. Unusual variants of pre-excitation: From anatomy to ablation: Part I—Understanding the anatomy of the variants of ventricular pre-excitation. J. Cardiovasc. Electrophysiol. 2019, 30, 2170–2180. [Google Scholar] [CrossRef] [PubMed]
- Correa, F.S.; Lokhandwala, Y.; Filho, F.C.; Sánchez-Quintana, D.; Mori, S.; Anderson, R.H.; Wellens, H.J.J.; Back Sternick, E. Unusual variants of pre-excitation; Part II—Clinical presentation, electrophysiologic characteristics, and when and how to ablate atriofascicular pathways and long and short decrementally conducting accessory pathways. J. Cardiovasc. Electrophysiol. 2019, 30, 3079–3096. [Google Scholar] [CrossRef]
- Correa, F.S.; Lokhandwala, Y.; Filho, F.C.; Sánchez-Quintana, D.; Mori, S.; Anderson, R.H.; Wellens, H.J.J.; Back Sternick, E. Unusual variants of pre-excitation: From anatomy to ablation: Part III—Clinical presentation, electrophysiologic characteristics, when and how to ablate nodoventricular, nodofascicular, fasciculoventricular pathways, along with considerations of permanent junctional reciprocating tachycardia. J. Cardiovasc. Electrophysiol. 2019, 30, 3097–3115. [Google Scholar] [CrossRef]
- Suzuki, T.; Nakamura, Y.; Yoshida, S.; Yoshida, Y.; Shintaku, H. Differentiating fasciculoventricular pathway from Wolff-Parkinson-White syndrome by electrocardiography. Heart Rhythm 2014, 11, 686–690. [Google Scholar] [CrossRef]
- Yanni, J.; Boyett, M.R.; Anderson, R.H.; Dobrzynski, H. The extent of the specialized atrioventricular ring tissues. Heart Rhythm 2009, 6, 672–680. [Google Scholar] [CrossRef]
- Bohora, S.; Lokhandwala, Y.; Back Sternick, E.; Anderson, R.H.; Wellens, H.J.J. Reappraisal and new observations on atrial tachycardia ablated from the non-coronary aortic sinus of Valsalva. Europace 2018, 20, 124–133. [Google Scholar] [CrossRef]
- Anderson, R.H.; Davies, M.J.; Becker, A.E. Atrioventricular ring specialized tissue in the human heart. Eur. J. Cardiol. 1974, 2, 219–230. [Google Scholar]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sternick, E.B.; Sánchez-Quintana, D. Critical Assessment of the Concepts and Misconceptions of the Cardiac Conduction System over the Last 100 Years: The Personal Quest of Robert H. Anderson. J. Cardiovasc. Dev. Dis. 2021, 8, 5. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010005
Sternick EB, Sánchez-Quintana D. Critical Assessment of the Concepts and Misconceptions of the Cardiac Conduction System over the Last 100 Years: The Personal Quest of Robert H. Anderson. Journal of Cardiovascular Development and Disease. 2021; 8(1):5. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010005
Chicago/Turabian StyleSternick, Eduardo Back, and Damián Sánchez-Quintana. 2021. "Critical Assessment of the Concepts and Misconceptions of the Cardiac Conduction System over the Last 100 Years: The Personal Quest of Robert H. Anderson" Journal of Cardiovascular Development and Disease 8, no. 1: 5. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8010005