
Effect of Hydroxychloroquine on QTc in Patients Diagnosed with COVID-19: A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Inclusion Criteria
2.2. Data Extraction and Outcomes
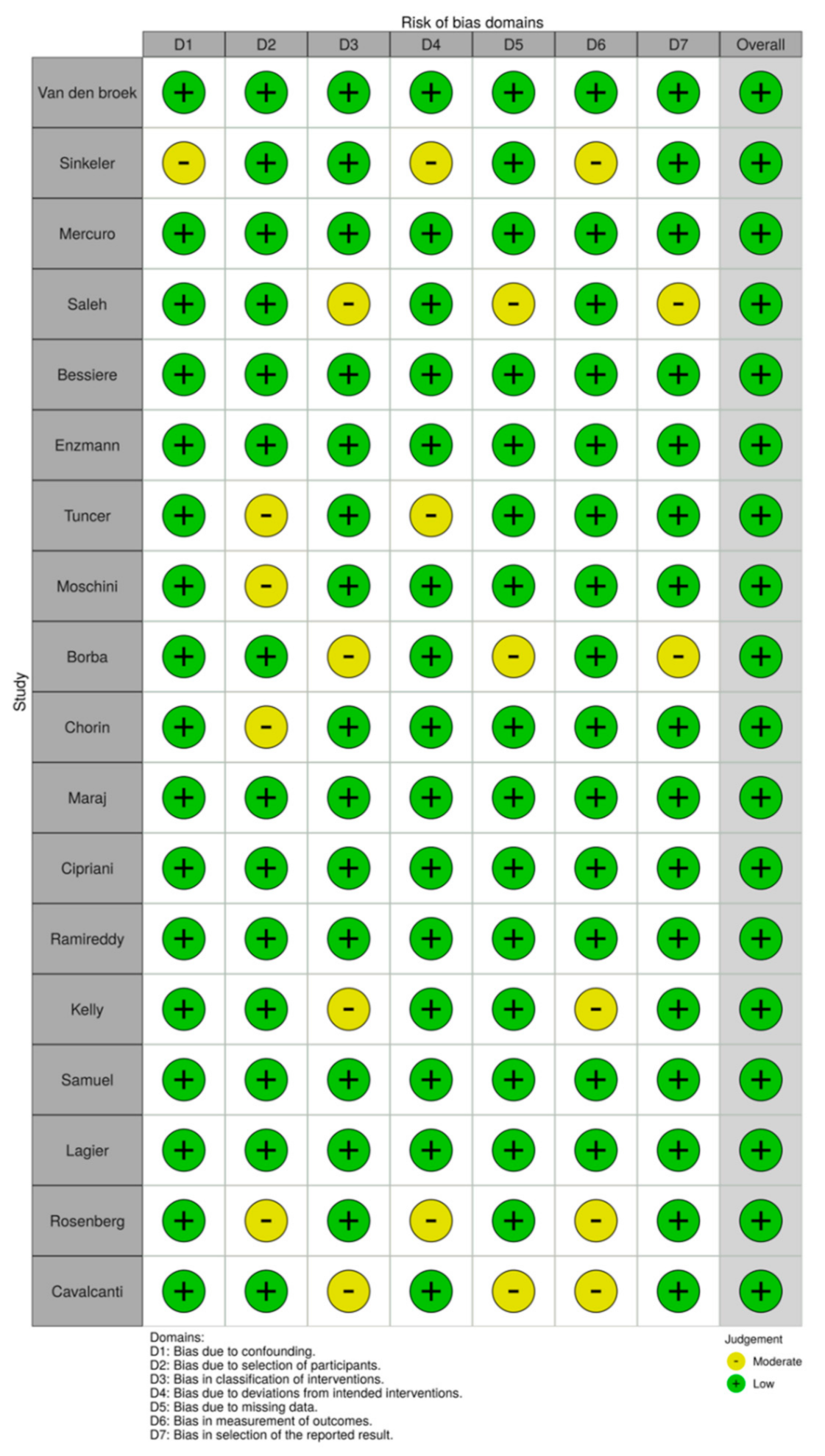
2.3. Risk of Bias Assessment
2.4. Statistical Synthesis and Analysis
3. Results
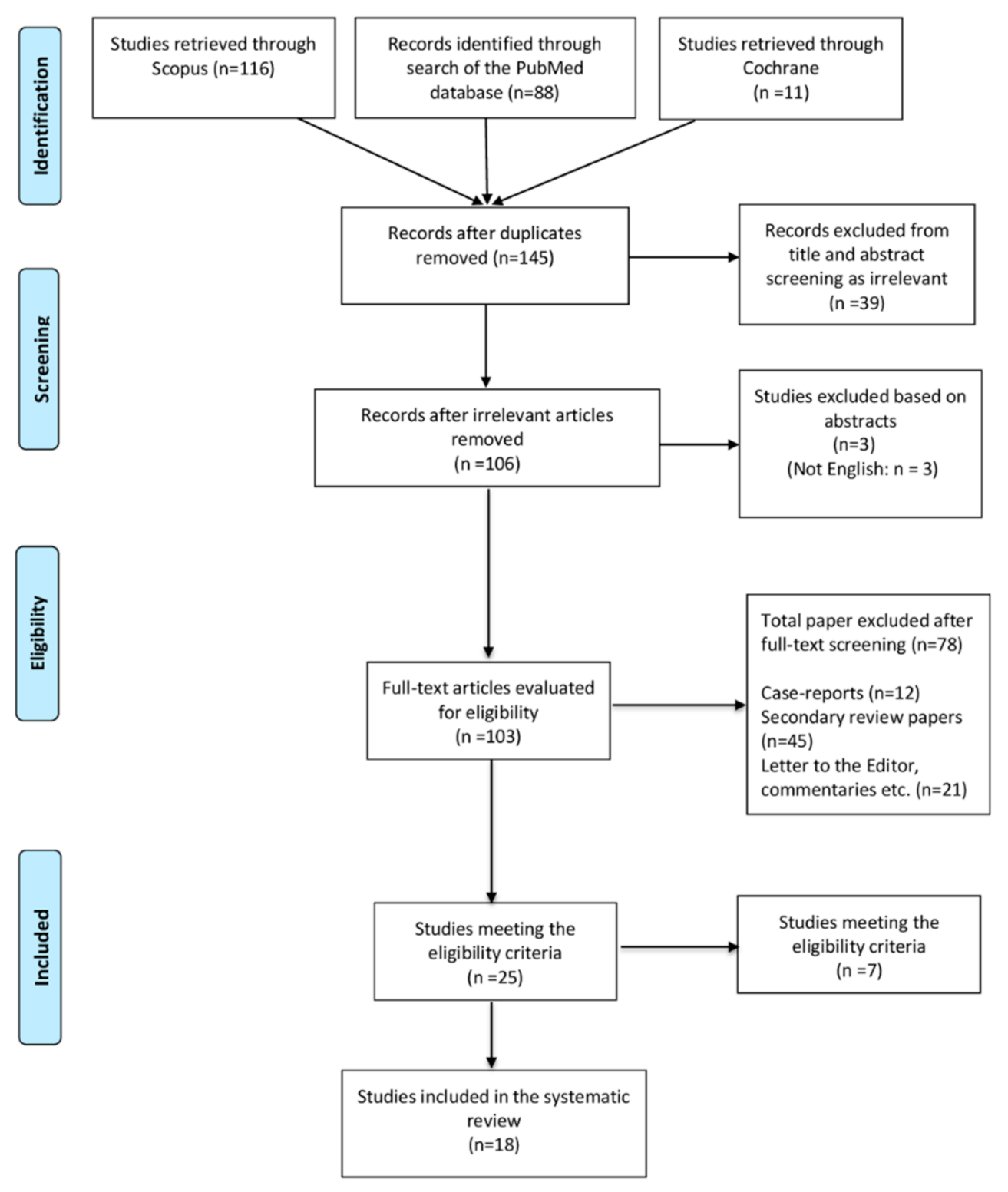
3.1. Search Results
3.2. Characteristics of Studies and Patients
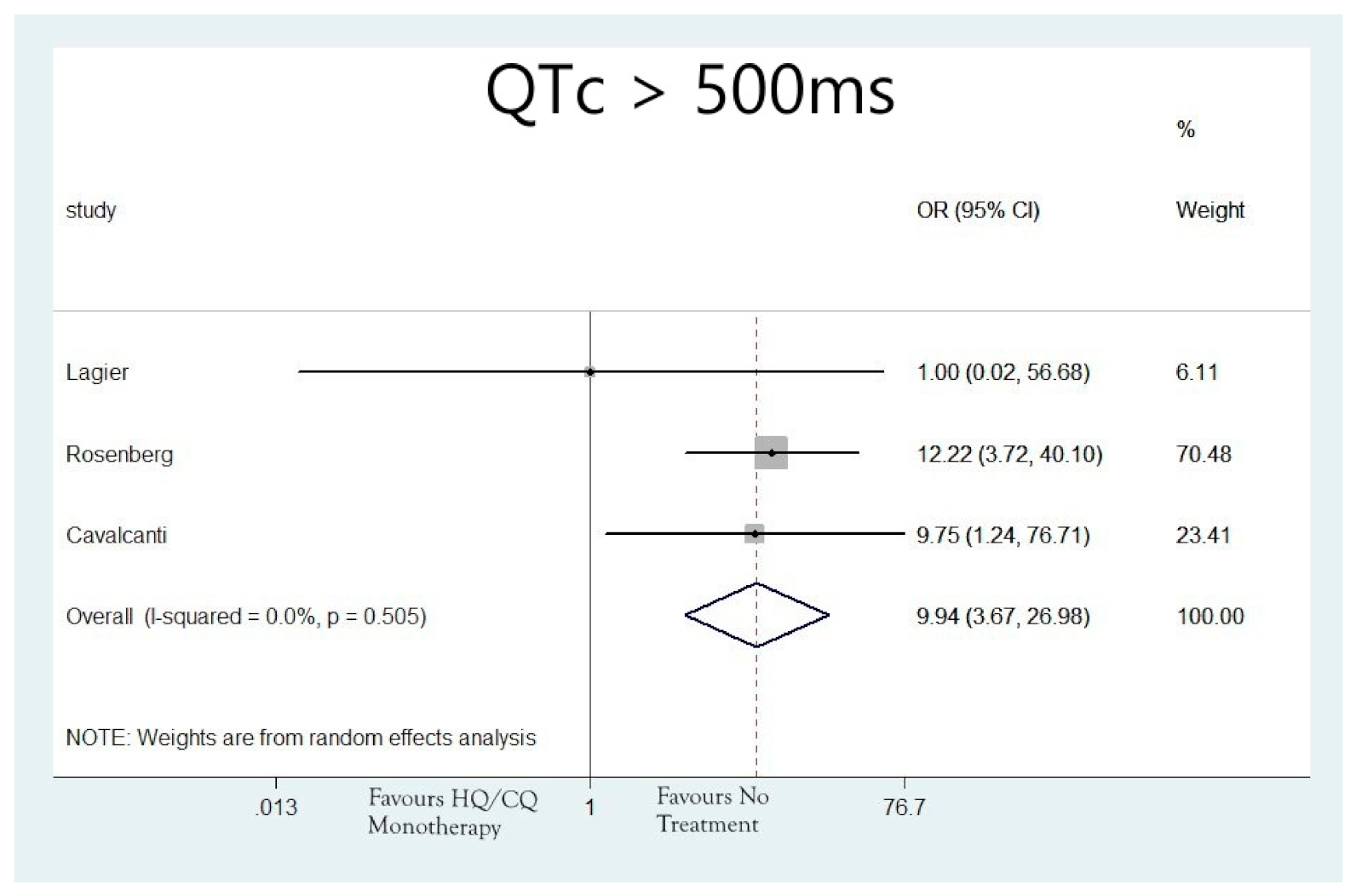
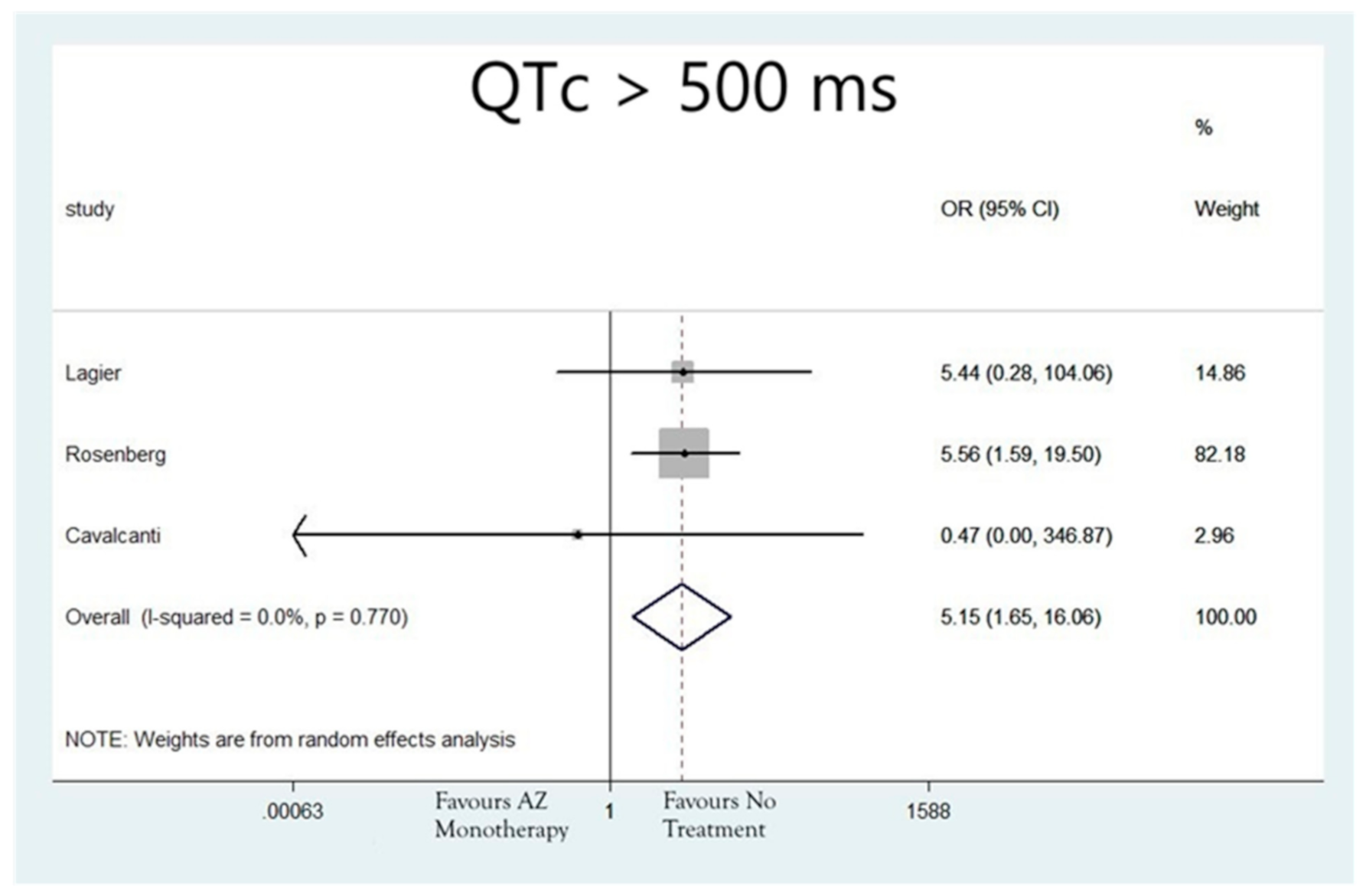
3.3. Outcome Analysis
3.4. Risk of Bias Assessment
4. Discussion
5. Strengths and Limitations
6. Conclusions
Funding
Conflicts of Interest
References
- Colson, P.; Rolain, J.-M.; Lagier, J.-C.; Brouqui, P.; Raoult, D. Chloroquine and hydroxychloroquine as available weapons to fight COVID-2. Int. J. Antimicrob. Agents 2020, 55, 105932. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Lagier, J.-C.; Parola, P.; Hoang, V.T.; Maddeb, B.; Mailhe, M.; Doubier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 56, 105949. [Google Scholar] [CrossRef]
- Colson, P.; Rolain, J.M.; Raoult, D. Chloroquine for the 2019 novel coronavirus SARS-CoV. Int. J. Antimicrob. Agents 2020, 55, 105923. [Google Scholar] [CrossRef]
- Devaux, C.A.; Rolain, J.-M.; Colson, P.; Raoult, D. New insights on the antiviral effects of chloroquine against coronavirus: What to expect for COVID-19? Int. J. Antimicrob. Agents 2020, 55, 105938. [Google Scholar] [CrossRef]
- Perricone, C.; Triggianese, P.; Bartoloni, E.; Cafaro, G.; Bonifacio, A.F.; Bursi, R.; Perricone, R.; Gerli, R. The anti-viral facet of anti-rheumatic drugs: Lessons from COVID-19. J. Autoimmun. 2020, 111, 102468. [Google Scholar] [CrossRef] [PubMed]
- Kezerashvili, A.; Khattak, H.; Barsky, A.; Nazari, R.; Fisher, J.D. Azithromycin as a cause of QT-interval prolongation and torsade de pointes in the absence of other known precipitating factors. J. Interv. Card. Electrophysiol. 2007, 18, 243–246. [Google Scholar] [CrossRef]
- Morgan, N.D.; Patel, S.V.; Dvorkina, O. Suspected Hydroxychloroquine-Associated QT-Interval Prolongation in a Patient with Systemic Lupus Erythematosus. JCR J. Clin. Rheumatol. 2013, 19, 286–288. [Google Scholar] [CrossRef]
- White, N.J. Cardiotoxicity of antimalarial drugs. Lancet Infect. Dis. 2007, 7, 549–558. [Google Scholar] [CrossRef]
- Mason, J.W. Antimicrobials and QT prolongation. J. Antimicrob. Chemother. 2017, 72, 1272–1274. [Google Scholar] [CrossRef] [PubMed]
- Bessière, F.; Roccia, H.; Delinière, A.; Charrière, R.; Chevalier, P.; Argaud, L.; Cour, M. Assessment of QT Intervals in a Case Series of Patients with Coronavirus Disease 2019 (COVID-19) Infection Treated with Hydroxychloroquine Alone or in Combination with Azithromycin in an Intensive Care Unit. JAMA Cardiol. 2020, 5, 1067–1069. [Google Scholar] [CrossRef]
- Borba, M.G.S.; Val, F.F.A.; Sampaio, V.S.; Alexandre, M.M.A.; Melo, G.C.; Brito, M.; Mourano, M.P.G.; Brito-Sousa, J.D.; Baia-de-Silva, D.; Guera, M.V.F.; et al. Effect of High vs. Low Doses of Chloroquine Diphosphate as Adjunctive Therapy for Patients Hospitalized with Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e208857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Chorin, E.; Wadhwani, L.; Magnani, S.; Dai, M.; Shulman, E.; Nadeau-Routhier, C.; Knotts, R.; Bar-Cohen, R.; Kogan, E.; Barbhaiya, C.; et al. QT interval prolongation and torsade de pointes in patients with COVID-19 treated with hydroxychloroquine/azithromycin. Heart Rhythm 2020, 17, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Zorzi, A.; Ceccato, D.; Capone, F.; Parolin, M.; Donato, F.; Fioretto, P.; Pesavento, R.; Previato, L.; Maffei, P.; et al. Arrhythmic profile and 24-hour QT interval variability in COVID-19 patients treated with hydroxychloroquine and azithromycin. Int. J. Cardiol. 2020, 316, 280–284. [Google Scholar] [CrossRef]
- Enzmann, M.O.; Erickson, M.P.; Grindeland, C.J.; Lopez, S.M.C.; Hoover, S.E.; Leedahl, D.D. Treatment and preliminary outcomes of 150 acute care patients with COVID-19 in a rural health system in the Dakotas. Epidemiol. Infect. 2020, 148, e124. [Google Scholar] [CrossRef] [PubMed]
- Kelly, M.; O’Connor, R.; Townsend, L.; Coghlan, M.; Relihan, E.; Moriarty, M.; Carr, B.; Melanophy, G.; Doyle, C.; Bannan, C.; et al. Clinical outcomes and adverse events in patients hospitalised with COVID-19, treated with off-label hydroxychloroquine and azithromycin. Br. J. Clin. Pharmacol. 2021, 87, 1150–1154. [Google Scholar] [CrossRef]
- Lagier, J.-C.; Million, M.; Gautret, P.; Colson, P.; Cortaredona, S.; Giraud-Gatineau, A.; Honoré, S.; Gaubert, J.-Y.; Fournier, P.-E.; Tissot-Dupont, H.; et al. Outcomes of 3,737 COVID-19 patients treated with hydroxychloroquine/azithromycin and other regimens in Marseille, France: A retrospective analysis. Travel Med. Infect. Dis. 2020, 36, 101791. [Google Scholar] [CrossRef] [PubMed]
- Maraj, I.; Hummel, J.P.; Taoutel, R.; Chamoun, R.; Workman, V.; Li, C.; Tran, L.; DelVecchio, A.; Howes, C.; Akar, J.G. Incidence and determinants of QT interval prolongation in COVID-19 patients treated with hydroxychloroquine and azithromycin. J. Cardiovasc. Electrophysiol. 2020, 31, 1904–1907. [Google Scholar] [CrossRef]
- Mercuro, N.J.; Yen, C.F.; Shim, D.J.; Maher, T.R.; McCoy, C.M.; Zimetbaum, P.J.; Gold, H.S. Risk of QT Interval Prolongation Associated with Use of Hydroxychloroquine with or without Concomitant Azithromycin Among Hospitalized Patients Testing Positive for Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1036–1041. [Google Scholar] [CrossRef]
- Moschini, L.; Loffi, M.; Regazzoni, V.; Di Tano, G.; Gherbesi, E.; Battista Danzi, G. Effects on QT interval of hydroxychloroquine associated with ritonavir/darunavir or azithromycin in patients with SARS-CoV-2 infection. Heart Vessels 2020, 16, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Ramireddy, A.; Chugh, H.; Reinier, K.; Ebinger, J.; Park, E.; Thompson, M.; Cingolani, E.; Cheng, S.; Marban, E.; Albert, C.M.; et al. Experience with Hydroxychloroquine and Azithromycin in the Coronavirus Disease 2019 Pandemic: Implications for QT Interval Monitoring. J. Am. Heart Assoc. 2020, 9, e017144. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Dufort, E.M.; Udo, T.; Wilberschied, L.A.; Kumar, J.; Tesoriero, J.; Weinberg, P.; Kirkwood, J.; Muse, A.; DeHovitz, J.; et al. Association of Treatment with Hydroxychloroquine or Azithromycin with In-Hospital Mortality in Patients With COVID-19 in New York State. JAMA 2020, 323, 2493–2502. [Google Scholar] [CrossRef]
- Saleh, M.; Gabriels, J.; Chang, D.; Kim, B.S.; Mansoor, A.; Mahmood, E.; Makker, P.; Ismail, H.; Goldner, B.; Willner, J.; et al. Effect of Chloroquine, Hydroxychloroquine, and Azithromycin on the Corrected QT Interval in Patients with SARS-CoV-2 Infection. Circ. Arrhythmia Electrophysiol. 2020, 13, e008662. [Google Scholar] [CrossRef]
- Samuel, S.; Friedman, R.A.; Sharma, C.; Ganigara, M.; Mitchell, E.; Schleien, C.; Blaufox, A.D. Incidence of arrhythmias and electrocardiographic abnormalities in symptomatic pediatric patients with PCR-positive SARS-CoV-2 infection, including drug-induced changes in the corrected QT interval. Heart Rhythm 2020, 17, 1960–1966. [Google Scholar] [CrossRef]
- Sinkeler, F.S.; Berger, F.A.; Muntinga, H.J.; Jansen, M.M.P.M. The risk of QTc-interval prolongation in COVID-19 patients treated with chloroquine. Neth. Heart J. 2020, 28, 418–423. [Google Scholar] [CrossRef]
- Tuncer, T.; Karaci, M.; Boga, A.; Durmaz, H.; Guven, S. QT interval evaluation associated with the use of hydroxychloroquine with combined use of azithromycin among hospitalised children positive for coronavirus disease Cardiol. Young 2020, 30, 1482–1485. [Google Scholar] [CrossRef] [PubMed]
- Broek, M.P.H.V.D.; Möhlmann, J.E.; Abeln, B.G.S.; Liebregts, M.; Van Dijk, V.F.; Van De Garde, E.M.W. Chloroquine-induced QTc prolongation in COVID-19 patients. Neth. Heart J. 2020, 28, 406–409. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helfenbein, E.D.; Zhou, S.H.; Lindauer, J.M.; Field, D.Q.; Gregg, R.E.; Wang, J.J.; Kresge, S.S.; Michaud, F.P. An algorithm for continuous real-time QT interval monitoring. J. Electrocardiol. 2006, 39, S123–S127. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, I.; Moss, A.J.; Peterson, D.R.; McNitt, S.; Zareba, W.; Andrews, M.L.; Robinson, J.L.; Locati, E.H.; Ackerman, M.J.; Benhorin, J.; et al. Risk Factors for Aborted Cardiac Arrest and Sudden Cardiac Death in Children with the Congenital Long-QT Syndrome. Circulation 2008, 117, 2184–2191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haeusler, I.L.; Chan, X.H.S.; Guérin, P.J.; White, N.J. The arrhythmogenic cardiotoxicity of the quinoline and structurally related antimalarial drugs: A systematic review. BMC Med. 2018, 16, 200. [Google Scholar] [CrossRef]
- Jankelson, L.; Karam, G.; Becker, M.L.; Chinitz, L.A.; Tsai, M.-C. QT prolongation, torsades de pointes, and sudden death with short courses of chloroquine or hydroxychloroquine as used in COVID-19: A systematic review. Heart Rhythm 2020, 17, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Driggin, E.; Madhavan, M.V.; Bikdeli, B.; Chuich, T.; Laracy, J.; Biondi-Zoccai, G.; Brown, T.S.; Der Nigoghossian, C.; Zidar, D.A.; Haythe, J.; et al. Cardiovascular Considerations for Patients, Health Care Workers, and Health Systems during the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 75, 2352–2371. [Google Scholar] [CrossRef]
- Lazzerini, P.E.; Boutjdir, M.; Capecchi, P.L. COVID-19, Arrhythmic Risk, and Inflammation: Mind the Gap! Circulation 2020, 142, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Roden, D.M. Drug-Induced Prolongation of the QT Interval. N. Engl. J. Med. 2004, 350, 1013–1022. [Google Scholar] [CrossRef] [Green Version]
- Roden, D.M.; Harrington, R.A.; Poppas, A.; Russo, A.M. Considerations for Drug Interactions on QTc in Exploratory COVID-19 (Coronavirus Disease 2019) Treatment. Circulation 2020, 141, e906–e907. [Google Scholar] [CrossRef] [Green Version]
- Bonow, R.O.; Hernandez, A.F.; Turakhia, M. Hydroxychloroquine, Coronavirus Disease 2019, and QT Prolongation. JAMA Cardiol. 2020, 5, 986–987. [Google Scholar] [CrossRef]
- Smit, C.; Peeters, M.Y.M.; van den Anker, J.N.; Knibbe, C.A.J. Chloroquine for SARS-CoV-2: Implications of Its Unique Pharmacokinetic and Safety Properties. Clin. Pharmacokinet. 2020, 59, 659–669. [Google Scholar] [CrossRef]
- Milberg, P.; Eckardt, L.; Bruns, H.-J.; Biertz, J.; Ramtin, S.; Reinsch, N.; Fleischer, D.; Kirchhof, P.; Fabritz, L.; Breithardt, G.; et al. Divergent Proarrhythmic Potential of Macrolide Antibiotics Despite Similar QT Prolongation: Fast Phase 3 Repolarization Prevents Early Afterdepolarizations and Torsade de Pointes. J. Pharmacol. Exp. Ther. 2002, 303, 218–225. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Menchaca, A.A.; Navarro-Polanco, R.A.; Ferrer-Villada, T.; Rupp, J.; Sachse, F.B.; Tristani-Firouzi, M.; Sánchez-Chapula, J.A. The molecular basis of chloroquine block of the inward rectifier Kir2.1 channel. Proc. Natl. Acad. Sci. USA 2008, 105, 1364–1368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Xie, M.; Li, S.; Gao, Y.; Xue, S.; Huang, H.; Chen, K.; Liu, F.; Chen, L. Electrophysiologic Studies on the Risks and Potential Mechanism Underlying the Proarrhythmic Nature of Azithromycin. Cardiovasc. Toxicol. 2017, 17, 434–440. [Google Scholar] [CrossRef]
- Capel, R.A.; Herring, N.; Kalla, M.; Yavari, A.; Mirams, G.R.; Douglas, G.; Bub, G.; Channon, K.; Paterson, D.J.; Terrar, D.A.; et al. Hydroxychloroquine reduces heart rate by modulating the hyperpolarization-activated current If: Novel electrophysiological insights and therapeutic potential. Heart Rhythm 2015, 12, 2186–2194. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Region/Country | Month, Year | Study Design | QTc Formula | Total N of pts | HQ/CQ Alone, N of pts | HQ/CQ + AZ, N of pts | AZ Alone, N of pts | No Treatment, N of pts |
|---|---|---|---|---|---|---|---|---|---|
| Van den Broek | Utrecht, Netherlands | April, 2020 | R OBS | Bazett | 95 | 95 | 0 | 0 | 0 |
| Sinkeler | Tilburg and Amersfoort, Netherlands | July, 2020 | R OBS (2 centers) | Postema and Wilde method | 397 | 397 | 0 | 0 | 0 |
| Mercuro | Massachusetts, USA | May 2020 | R OBS | Bazett | 90 | 37 | 53 | 0 | 0 |
| Saleh | 3 hospitals within Northwell Health System, NY, USA | April 2020 | P OBS | Bazett | 191 | 72 | 119 | 0 | 0 |
| Bessiere | Lyon, France | May 2020 | R OBS | Bazett | 40 | 18 | 22 | 0 | 0 |
| Enzmann | Fargo, ND, USA | June 2020 | R OBS | NR | 75 | 9 | 66 | 0 | 0 |
| Tuncer | Istanbul, Turkey (pediatric only) | June 2020 | R OBS | Bazett | 21 | 2 | 19 | 0 | 0 |
| Moschini | Cremona, Italy | July 2020 | R OBS | Bazett | 113 | 61 | 52 | 0 | 0 |
| Borba | Manaus, Brazil | April 2020 | P single-center | Fridericia | 81 | 0 | 81 | 0 | 0 |
| Chorin | NY, USA (NYU Langone Health); Milan, Italy | May 2020 | R OBS | Bazett | 251 | 0 | 251 | 0 | 0 |
| Maraj | New Haven, USA | May 2020 | R OBS | Bazett | 91 | 0 | 91 | 0 | 0 |
| Cipriani | Padua, Italy | May 2020 | R OBS | Bazett and Fridericia (if HR > 100) | 22 | 0 | 22 | 0 | 0 |
| Ramireddy | California, USA | May 2020 | R OBS | Bazett and Fridericia | 98 | 10 | 61 | 27 | 0` |
| Kelly | Dublin, Ireland | July 2020 | R OBS | NR | 134 | 0 | 82 | 0 | 52 |
| Samuel | NY, USA (Cohen Children’s Medical Center, pediatric only) | July 2020 | R OBS | Bazett | 36 | 16 | 9 | 0 | 11 |
| Lagier | Marseille, France | June 2020 | R OBS | Bazett | 3737 | 101 | 3337 | 137 | 162 |
| Rosenberg | NYC, Nassau County, Suffolk County, Westchester County, USA | May 2020 | R multicenter OBS | NR | 1438 | 271 | 735 | 211 | 221 |
| Cavalcanti | Brazil | July 2020 | P multicenter OBS * | NR | 269 | 89 | 116 | 6 | 58 |
| Study | N of Participants (Total) | Age | Male n (%) | BMI | Diabetes n (%) | HTN n (%) | CAD n (%) | CHF n (%) | Asthma/COPD n (%) | CKD II-IV or ESRD n (%) | Other QTc Prolonging Agents n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Van den Broek | 95 | 65 | 63 (66) | NR | NR | NR | 11 (12) | 9 (11) | NR | NR | NR |
| Sinkeler | 397 | 67.8 (12.5) | 262 (66) | 28.5 (5.6) | NR | NR | 32 (8) | 32 (8) | NR | 116 (29.2) | 106 (27) |
| Mercuro | 90 | 60.1 (16.7) | 46 (51.1) | 31.5 (6.6) | 26 (28.9) | 48 (53.3) | 10 (11.1) | 9 (10.0) | 18 (20.0) | NR | 90 (100) |
| Saleh | 191 | 58.6 (9.1) | 115 (60.2) | 28.2 (2.8) | 65 (32.3) | 121 (60.2) | 23 (11.4) | 15 (7.9) | 30 (15.7) | 10 (5.2) | 81 (42.4) |
| Bessiere | 40 | 66.7 (11.9) | 32 (80) | 28.7 (5.9) | 16 (40) | 23 (57.5) | NR | NR | NR | NR | 20 (50) |
| Enzmann | 75 | 56 | 43 (57.3) | NR | 22 (28.7) | NR | NR | 8 (10.7) | 22 (29.3) | 4 (5.3) | NR |
| Tuncer | 21 | 14.16 | 9 (42.8) | 23.7 | NR | NR | NR | NR | 2 (9.5) | 0 (0) | |
| Moschini | 113 | 67.7 (9.6) | 85 (75) | NR | 16 (14) | 32 (28) | NR | NR | 4 (3.5) | 6 (5.3) | 61 (53.9) |
| Borba | 81 | 51.1 (13.9) | 61 (75.3) | 28.6 (6.4) | 14(25.5) | 25 * (45.5) | NR | NR | NR | NR | 81 (100) |
| Chorin | 251 | 64.3 (20) | 188 (75) | NR | 67 (27) | 135 (54) | 30 (12) | 8 (3) | 18 (7) | 28 (11.1) | 73 (29) |
| Maraj | 91 | 62.7 (15.1) | 51 (66) | NR | 26 (29) | 42 (46) | 13 (14) | NR | 6 (7) | 25 (27.4) | 38 (42) |
| Cipriani | 22 | 63.3 (10.37) | 18 (82) | 28.3 (4.4) | 6 (27) | 12 (55) | NR | NR | 1 (5) | 1 (5) | 0 (0) |
| Ramireddy | 98 | 62.3 (17) | 60 (61) | 27.8 (6.6) | 22 (22) | 59 (60) | NR | 20 (20.4) | 25 (26) | 14 (14.3) | 74 (75.5) |
| Kelly | 134 | 66.04 | 51 (38) | NR | NR | NR | NR | NR | NR | NR | 3 (2.2) |
| Samuel | 36 | 12.6 (6) | 20 (55.5) | NR | NR | 0 (0) | 0 (0) | NR | 3 (8) | NR | 2 (5.5) |
| Lagier | 3737 | 45.3 (16.8) | 1704 (45.6) | NR | 312 (8.3) | 561 (15) | NR | NR | 338 (11) | NR | 45 (1.2) |
| Rosenberg | 1438 | NR | 858 (59.7) | NR | 504 (35) | 816 (56.7) | 173 (12) | 96 (6.6) | 259 (18) | NR | NR |
| Cavalcanti | 269 | 50.3 (14.6) | 157 (58.3) | NR | 51 (18.9) | 104 (38.7) | 11 (12) | 4 (1.5) | 21 (7.8) | 2 (0.7) | NR |
| Study | Torsades De Point n (%) | Ventricular Arrhythmia n (%) |
|---|---|---|
| Van den Broek | 0 (0) | 0 (0) |
| Sinkeler | NR | 1 (0.2) |
| Mercuro | 1 (11) | NR |
| Saleh | 0 (0) | 7 (3.7) (non-sustained) 1 (0.5) (sustained) |
| Bessiere | 0 (0) | 0 (0) |
| Enzmann | NR | 14 (18.7) |
| Tuncer | 0 (0) | 0 (0) |
| Moschini | 1 (11) | 2 (1.8) |
| Borba | NR | NR |
| Chorin | 1 (0.4) | NR |
| Maraj | 1 (11) | 2 (2) |
| Cipriani | NR | NR |
| Ramireddy | 0 (0) | NR |
| Kelly | NR | NR |
| Samuel | 0 (0) | 6 (16.7) |
| Lagier | 0 (0) | NR |
| Rosenberg | NR | NR |
| Cavalcanti | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arfaras-Melainis, A.; Tzoumas, A.; Kokkinidis, D.G.; Salgado Guerrero, M.; Varrias, D.; Xu, X.; Cerna, L.; Avendano, R.; Kemal, C.; Palaiodimos, L.; et al. Effect of Hydroxychloroquine on QTc in Patients Diagnosed with COVID-19: A Systematic Review and Meta-Analysis. J. Cardiovasc. Dev. Dis. 2021, 8, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8050055
Arfaras-Melainis A, Tzoumas A, Kokkinidis DG, Salgado Guerrero M, Varrias D, Xu X, Cerna L, Avendano R, Kemal C, Palaiodimos L, et al. Effect of Hydroxychloroquine on QTc in Patients Diagnosed with COVID-19: A Systematic Review and Meta-Analysis. Journal of Cardiovascular Development and Disease. 2021; 8(5):55. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8050055
Chicago/Turabian StyleArfaras-Melainis, Angelos, Andreas Tzoumas, Damianos G. Kokkinidis, Maria Salgado Guerrero, Dimitrios Varrias, Xiaobo Xu, Luis Cerna, Ricardo Avendano, Cameron Kemal, Leonidas Palaiodimos, and et al. 2021. "Effect of Hydroxychloroquine on QTc in Patients Diagnosed with COVID-19: A Systematic Review and Meta-Analysis" Journal of Cardiovascular Development and Disease 8, no. 5: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8050055