
The Effect of Vitamin D on Coronary Atherosclerosis: A Propensity Score Matched Case–Control Coronary CTA Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- Patients with low-to-intermediate Atherosclerotic Cardiovascular Disease (ASCVD) risk [22], non-specific, atypical, or stable chest pain complaints, and/or suspected coronary heart disease based on other prior tests (ECG-stress test, treadmill, or myocardial perfusion test);
- Availability of conventional coronary risk factors according to standardized ESC criteria: arterial hypertension [23] (systolic blood pressure >140 mmHg or diastolic >90 mmHg), dyslipidemia [24] (total cholesterol >200 mg/dL and high-density lipoprotein (HDL) <40 mg/dL; and/or c-low-density lipoprotein (c-LDL) >160 mg/dL), family history (myocardial infarction or sudden cardiac death in an immediate male relative <55 years or female <65 years), smoker (current or quit within the last 6 months), and diabetes. HDL, total cholesterol, c-LDL, and triglyceride levels were determined as well.
2.2. Computed Tomography Angiography (CTA)
2.3. CTA Image Analysis
- (1)
- Coronary stenosis severity was scored on a 5-point scale as: (1) minimal (<25%), (2) mild (25–49%); (3) intermediate (50–69.9%); (4) severe (≥ 70%); and (5) occluded (100%) according to the standardized Coronary Artery Disease Reporting and Data System (CAD-RADSTM) classification [16] per-coronary segment (AHA-modified-16-segment classification) [26].
- (2)
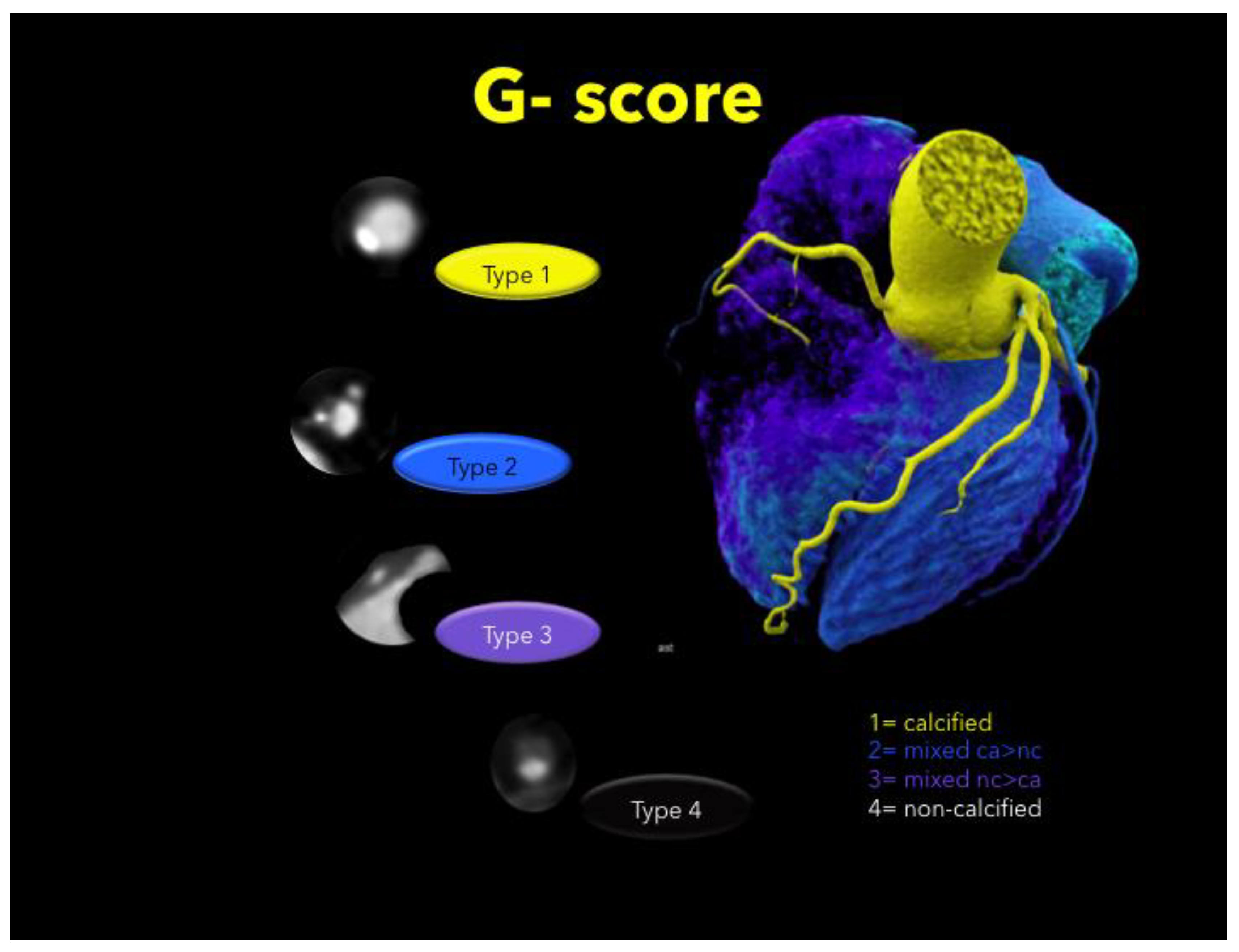
- Plaque types were defined as: calcified (T1), mixed (dominantly calcified > non-calcified, T2), mixed (dominantly non-calcified > calcified, T3), or non-calcified (T4) per coronary segment. Calcified and non-calcified plaque were defined as hyper-and hypoattenuating lesions with more and less than 150 HU [27], respectively. Total plaque burden was expressed by the coronary segment involvement (SIS) score [28], and the total mixed plaque burden weighted for the non-calcified plaque component was calculated as previously described [21] (sum of plaque types T1–4 for each segment, G-score) (Figure 1), per-coronary segment (AHA-modified-16-segment classification) [26].
- (3)
- Low attenuation plaque, hypodense to the artery lumen, was screened by utilizing the “pixel-lens” for the lowest CT-density (HU) area [18], and then a ROI was drawn as large as possible, while sparing areas affected by motion, beam hardening or partial volume artifacts. The HU ROI was measured on 3 consecutive images (1 mm slice thickness). Low attenuation plaque was defined as “non-calcified” if density was below 150 HU [27];
- Napkin Ring Sign was defined [17] as low attenuation plaque with a hyperdense rim and hypodense LAP core;
- Spotty calcification was defined as calcification <3 mm size;
- The remodeling index was calculated as the ratio of the maximal cross-sectional vessel diameter, including the plaque and the lumen, and its closest proximal (or distal: in ostial lesions) normal reference vessel lumen diameter.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Judd, S.E.; Tangpricha, V. Vitamin D Deficiency and Risk for Cardiovascular Disease. Am. J. Med Sci. 2009, 338, 40–44. [Google Scholar] [CrossRef] [Green Version]
- Vacek, J.L.; Vanga, S.R.; Good, M.; Lai, S.M.; Lakkireddy, D.; Howard, P.A. Vitamin D deficiency and supplementation and relation to cardiovascular health. Am. J. Cardiol. 2012, 109, 359–363. [Google Scholar] [CrossRef]
- Hsu, J.J.; Tintut, Y.; Demer, L.L. Vitamin D and Osteogenic Differentiation in the Artery Wall. Clin. J. Am. Soc. Nephrol. 2008, 3, 1542–1547. [Google Scholar] [CrossRef] [Green Version]
- Price, P.A.; Faus, S.A.; Williamson, M.K. Warfarin-Induced Artery Calcification Is Accelerated by Growth and Vitamin D. Arter. Thromb. Vasc. Biol. 2000, 20, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Song, Y.; Manson, J. Circulating 25-Hydroxy-Vitamin D and Risk of Cardiovascular Disease: A Meta-Analysis of Prospective Studies. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Lee, B.-K. Vitamin D deficiency is an independent risk factor for cardiovascular disease in Koreans aged ≥ 50 years: Results from the Korean National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2012, 6, 162–168. [Google Scholar] [CrossRef]
- Moradi, M.; Foroutanfar, A. Evaluation of vitamin D levels in relation to coronary CT angiographic findings in an Iranian population. Vasc. Health Risk Manag. 2017, 13, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Ho, J.S.; Cannaday, J.J.; Barlow, C.E.; Reinhardt, D.B.; Wade, W.A.; Ellis, J.R. Low 25-OH vitamin D levels are not associated with coronary artery calcium or obstructive stenoses. Coron. Artery Dis. 2015, 26, 521–525. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Vitamin D and cardiovascular diseases: Causality. J. Steroid Biochem. Mol. Biol. 2018, 175, 29–43. [Google Scholar] [CrossRef]
- Brøndum-Jacobsen, P.; Benn, M.; Jensen, G.B.; Nordestgaard, B.G. 25-hydroxyvitamin d levels and risk of ischemic heart disease, myocardial infarction, and early death: Population-based study and meta-analyses of 18 and 17 studies. Arter. Thromb. Vasc. Biol. 2012, 32, 2794–2802. [Google Scholar] [CrossRef] [Green Version]
- Sokol, S.I.; Tsang, P.; Aggarwal, V.; Melamed, M.L.; Srinivas, V.S. Vitamin D status and risk of cardiovascular events: Lessons learned via systematic review and meta-analysis. Cardiol. Rev. 2011, 19, 192–201. [Google Scholar] [CrossRef]
- Elamin, M.B.; Abu Elnour, N.O.; Elamin, K.B.; Fatourechi, M.M.; Alkatib, A.A.; Almandoz, J.; Liu, H.; Lane, M.A.; Mullan, R.J.; Hazem, A.; et al. Vitamin D and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2011, 96, 1931–1942. [Google Scholar] [CrossRef] [Green Version]
- Barbarawi, M.; Kheiri, B.; Zayed, Y.; Barbarawi, O.; Dhillon, H.; Swaid, B.; Yelangi, A. Vitamin D Supplementation and Car-diovascular Disease Risks in More Than 83 000 Individuals in 21 Randomized Clinical Trials: A Meta-analysis. JAMA Cardiol. 2019, 4, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.A.; MacLennan, G.S.; Avenell, A.; Bolland, M.; Grey, A.; Witham, M. Cardiovascular disease and vitamin D supple-mentation: Trial analysis, systematic review, and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 746–755. [Google Scholar] [CrossRef]
- Beveridge, L.A.; Struthers, A.D.; Khan, F.; Jorde, R.; Scragg, R.; Macdonald, H.M. Effect of Vitamin D Supplementation on Blood Pressure: A Systematic Review and Meta-analysis Incorporating Individual Patient Data. JAMA Intern Med. 2015, 175, 745–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cury, R.C.; Abbara, S.; Achenbach, S.; Agatston, A.; Berman, D.S.; Budoff, M.J.; Dill, K.E.; Jacobs, J.E.; Maroules, C.D.; Rubin, G.D.; et al. CAD-RADSTM Coronary Artery Disease—Reporting and Data System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. J. Cardiovasc. Comput. Tomogr. 2016, 10, 269–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurovich-Horvat, P.; Schlett, C.L.; Alkadhi, H.; Nakano, M.; Otsuka, F.; Stolzmann, P. The napkin-ring sign indicates ad-vanced atherosclerotic lesions in coronary CT angiography. JACC Cardiovasc Imaging 2012, 5, 1243–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.C.; Kwiecinski, J.; Doris, M.; McElhinney, P.; D’Souza, M.S.; Cadet, S. Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART). Circulation 2020, 141, 1452–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadi, A.; Leipsic, J.; Øvrehus, K.A.; Gaur, S.; Bagiella, E.; Ko, B. Lesion-Specific and Vessel-Related Determinants of Frac-tional Flow Reserve Beyond Coronary Artery Stenosis. JACC Cardiovasc. Imaging 2018, 11, 521–530. [Google Scholar] [CrossRef]
- Hell, M.M.; Motwani, M.; Otaki, Y.; Cadet, S.; Gransar, H.; Miranda-Peats, R.; Valk, J.; Slomka, P.J.; Cheng, V.Y.; Rozanski, A.; et al. Quantitative global plaque characteristics from coronary computed tomography angiography for the prediction of future cardiac mortality during long-term follow-up. Eur. Hear. J. Cardiovasc. Imaging 2017, 18, 1331–1339. [Google Scholar] [CrossRef] [Green Version]
- Feuchtner, G.M.; Barbieri, F.; Langer, C.; Beyer, C.; Widmann, G.; Friedrich, G.J. Non obstructive high-risk plaque but not calci-fied by coronary CTA, and the G-score predict ischemia. J. Cardiovasc. Comput. Tomogr. 2019, 13, 305–314. [Google Scholar] [CrossRef]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B., Sr.; Gibbons, R.; Greenland, P. 2013 ACC/AHA Guide-line on the Assessment of Cardiovascular Risk. J. Am. Coll Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [Green Version]
- Catapano, A.L.; Graham, I.; De Backer, G.; Wiklund, O.; Chapman, M.J.; Drexel, H. 2016 ESC/EAS Guidelines for the Manage-ment of Dyslipidaemias. Eur. Heart J. 2016, 37, 2999–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Agatston, A.S.; Janowitz, F.W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Austen, W.G.; Edwards, J.E.; Frye, R.L.; Gensini, G.G.; Gott, V.L.; Griffith, L.S.; McGoon, D.C.; Murphy, M.L.; Roe, B.B. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975, 51, 5–40. [Google Scholar] [CrossRef] [Green Version]
- Leber, A.W.; Knez, A.; Becker, A.; Becker, C.; von Ziegler, F.; Nikolaou, K. Accuracy of multidetector spiral computed to-mo-graphy in identifying and differentiating the composition of coronary atherosclerotic plaques: A comparative study with in-tracoronary ultrasound. J. Am. Coll Cardiol. 2004, 43, 1241–1247. [Google Scholar] [CrossRef] [Green Version]
- Schlett, C.L.; Maurovich-Horvat, P.; Ferencik, M.; Alkadhi, H.; Stolzmann, P.; Scheffel, H. Histogram analysis of lipid-core plaques in coronary computed tomographic angiography: Ex vivo validation against histology. Invest Radiol. 2013, 48, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, C.; Abdulla, J. Characteristics of high-risk coronary plaques identified by computed tomographic angiography and associated prognosis: A systematic review and meta-analysis. Eur. Heart J. Cardiovasc. Imaging 2015, 17, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Feuchtner, G.; Kerber, J.; Burghard, P.; Dichtl, W.; Friedrich, G.; Bonaros, N.; Plank, F. The high-risk criteria low-attenuation plaque <60 HU and the napkin-ring sign are the most powerful predictors of MACE: A long-term follow-up study. Eur. Heart J. Cardiovasc Imaging 2017, 18, 772–779. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.-J.; Lin, F.Y.; Lee, S.-E.; Andreini, D.; Bax, J.; Cademartiri, F.; Chinnaiyan, K.; Chow, B.; Conte, E.; Cury, R.C.; et al. Coronary Atherosclerotic Precursors of Acute Coronary Syndromes. J. Am. Coll. Cardiol. 2018, 71, 2511–2522. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, R.A.; van Rosendael, A.R.; Lu, Y.; Andreini, D.; Al-Mallah, M.H.; Cademartiri, F. Non-obstructive high-risk plaques in-crease the risk of future culprit lesions comparable to obstructive plaques without high-risk features: The ICONIC study. Eur. Heart J. Cardiovasc Imaging 2020, 21, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, R.; Gransar, H.; Berman, D.S.; Cheng, V.Y.; Lin, F.Y.; Achenbach, S. Relationship of low- and high-density lipopro-teins to coronary artery plaque composition by CT angiography. J. Cardiovasc Comput. Tomogr. 2013, 7, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; van der Werf, N.R.; Nieman, K.; Greuter, M.J.; Koweek, L.M.; Fleischmann, D. Coronary artery calcium: A technical argument for a new scoring method. J. Cardiovasc. Comput. Tomogr. 2019, 13, 347–352. [Google Scholar] [CrossRef]
- Senoner, T.; Plank, F.; Beyer, C.; Langer, C.; Birkl, K.; Steinkohl, F.; Widmann, G.; Barbieri, F.; Adukauskaite, A.; Friedrich, G.; et al. Does coronary calcium score zero reliably rule out coronary artery disease in low-to-intermediate risk patients? A coronary CTA study. J. Cardiovasc. Comput. Tomogr. 2020, 14, 155–161. [Google Scholar] [CrossRef]
- Van Rosendaehl, A.R.; Narula, J.; Lin, F.Y.; van den Hoogen, I.J.; Gianni, U.; Al Hussein Alawamlh, O. Association of High-Density Calcified 1K Plaque With Risk of Acute Coronary Syndrome. JAMA Cardiol. 2020, 5, 282–290. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vitamin D (n = 82) | Controls (n = 82) | p-Value | |
|---|---|---|---|
| Age in years | 63.2 ± 10.3 | 61.7 ± 10.5 | 0.358 |
| Females | 57 (69.5%) | 51 (62.2%) | 0.410 |
| Body mass index in kg/cm2 | 24.9 ± 3.5 | 26.1 ± 4.6 | 0.081 |
| Arterial hypertension | 29 (35.3) | 42 (51.2) | 0.058 |
| Smoking | 12 (14.6) | 18 (21.9) | 0.314 |
| Positive family history | 47 (57.3) | 42 (51.2) | 0.531 |
| Dyslipidemia | 49 (59.7) | 46 (56.1) | 0.751 |
| Diabetes | 5 (1.2) | 7 (8.5) | 0.764 |
| Total cholesterol in mg/dL | 202.6 ± 55 | 218.5 ± 45 | 0.180 |
| Low density lipoprotein in mg/dL | 141.1 ± 41 | 117.2 ± 47 | 0.020 |
| High density lipoprotein in mg/dL | 61.0 ± 18 | 58.4 ± 19 | 0.552 |
| Atherosclerotic cardiovascular disease risk | 11.8 ± 1.3 | 11.2 ± 1.4 | 0.935 |
| Vitamin D (n = 82) | Controls (n = 82) | p-Value | |
|---|---|---|---|
| Atherosclerosis | 62 (75.6%) | 61 (74.3%) | 0.999 |
| CAD-RADSTM | |||
| 0 | 20 (24.4%) | 21 (25.6%) | |
| 1 | 18 (22.0%) | 10 (12.2%) | |
| 2 | 30 (36.6%) | 25 (30.5%) | 0.106 |
| 3 | 7 (8.5%) | 4 (4.9%) | |
| 4/5 | 7 (8.5%) | 22 (26.8%) | |
| Total >50% | 14 (17.1%) | 26 (31.7%) | 0.046 |
| CAD RADSTM | 1.54 ± 1.2 | 1.95 ± 1.5 | 0.106 |
| Total plaque burden(SIS) | 2.7 ± 2.9 | 3.5 ± 3.0 | 0.002 |
| Mixed plaque burden (G-score) | 2.8 ± 3.2 | 5.3 ± 5.0 | 0.002 |
| Coronary artery calcium score (Agatston Units) | 69.7 ± 18.1 | 118.6 ± 264 | 0.301 |
| High risk plaque | 2 (2.4%) | 12 (14.6%) | 0.012 |
| CT density ROI in Hounsfield Units | 158.0 ± 68 | 75.1 ± 35 | <0.001 |
| CT density lens in Hounsfield Units | 144.5 ± 68 | 59.7 ± 36 | <0.001 |
| CT density ROI (mean **) in Hounsfield Units | 157.9 ± 59 | 67.2 ± 24 | <0.001 |
| Spotty calcification | 2 (2.4%) | 5 (6.1%) | 0.443 |
| Napkin ring sign | 1 (1.2%) | 4 (4.9%) | 0.367 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feuchtner, G.; Suppersberger, S.; Langer, C.; Beyer, C.; Rauch, S.; Thurner, T.; Friedrich, G.; Dichtl, W.; Widmann, G.; Plank, F.; et al. The Effect of Vitamin D on Coronary Atherosclerosis: A Propensity Score Matched Case–Control Coronary CTA Study. J. Cardiovasc. Dev. Dis. 2021, 8, 85. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080085
Feuchtner G, Suppersberger S, Langer C, Beyer C, Rauch S, Thurner T, Friedrich G, Dichtl W, Widmann G, Plank F, et al. The Effect of Vitamin D on Coronary Atherosclerosis: A Propensity Score Matched Case–Control Coronary CTA Study. Journal of Cardiovascular Development and Disease. 2021; 8(8):85. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080085
Chicago/Turabian StyleFeuchtner, Gudrun, Simon Suppersberger, Christian Langer, Christoph Beyer, Stefan Rauch, Theresa Thurner, Guy Friedrich, Wolfgang Dichtl, Gerlig Widmann, Fabian Plank, and et al. 2021. "The Effect of Vitamin D on Coronary Atherosclerosis: A Propensity Score Matched Case–Control Coronary CTA Study" Journal of Cardiovascular Development and Disease 8, no. 8: 85. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080085