
Effects of Different Exercise Interventions on Cardiac Autonomic Control and Secondary Health Factors in Middle-Aged Adults: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Analysis
2.3.1. Selection of Studies
2.3.2. Data Extraction
2.3.3. Quality Assessment
2.3.4. Data Synthesis and Analysis
3. Results
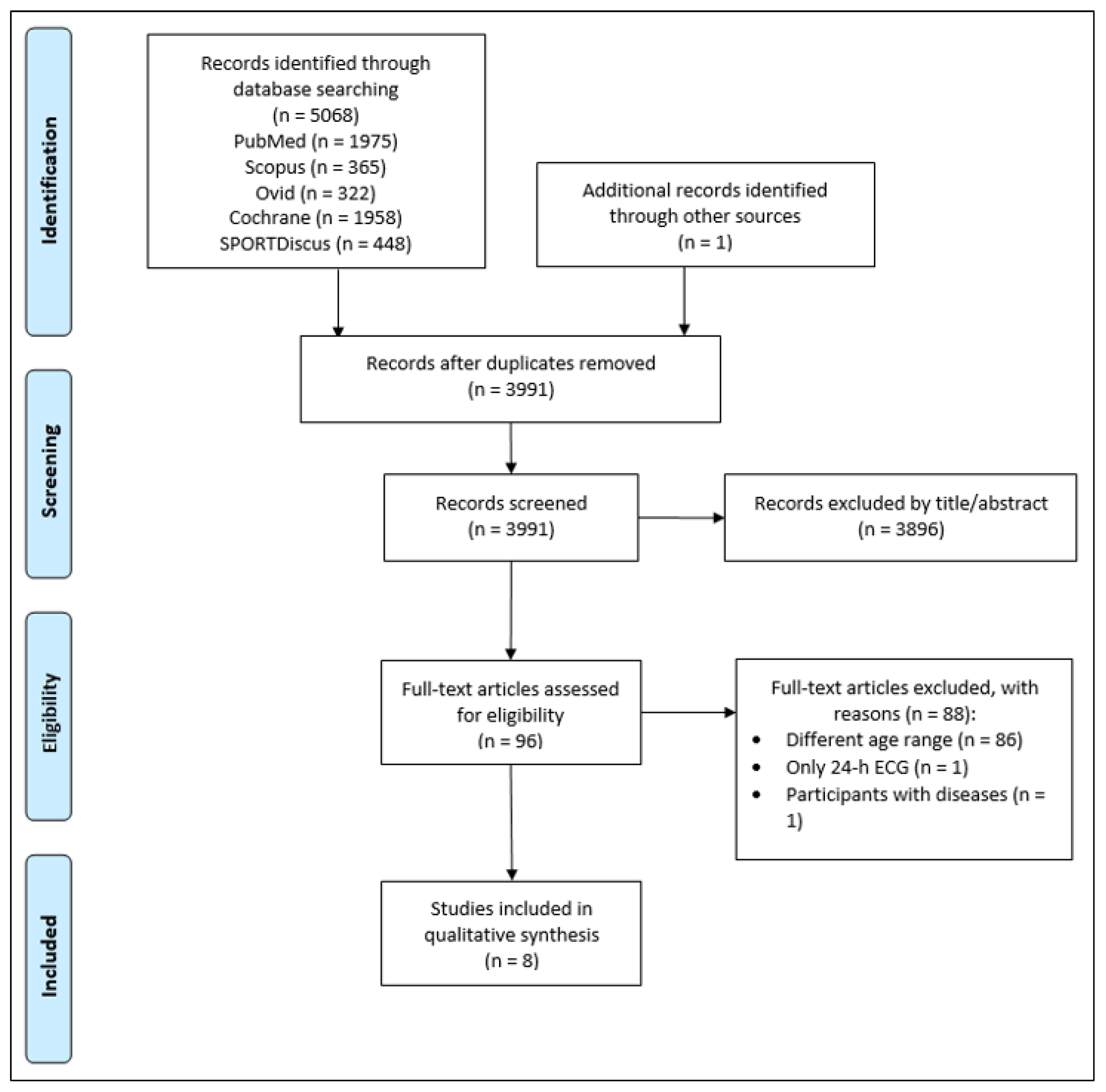
3.1. Study Selection
3.2. Study Characteristics
3.3. Heart Rate-Related Variables
3.3.1. Endurance Training
3.3.2. Resistance Training
3.3.3. Coordinative Training
3.3.4. Multimodal Training
3.4. Secondary Health Factors
3.4.1. Endurance Training
3.4.2. Resistance Training
3.4.3. Coordinative Training
3.4.4. Multimodal Training
3.5. Quality Assessment
4. Discussion
4.1. Purpose and Main Findings
4.2. Heart Rate-Related Variables
4.2.1. Endurance Training
4.2.2. Resistance Training
4.2.3. Coordinative Training
4.2.4. Multimodal Training
4.3. Secondary Health Factors
4.3.1. Endurance Training
4.3.2. Resistance Training
4.3.3. Coordinative Training
4.3.4. Multimodal Training
4.4. Possible Mechanisms behind Autonomic and Cardiovascular Adaptations
4.5. Quality Assessment
4.5.1. TESTEX
4.5.2. STARDHRV
4.6. Strengths and Limitations
4.7. Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- Fluckiger, L.; Boivin, J.M.; Quilliot, D.; Jeandel, C.; Zannad, F. Differential effects of aging on heart rate variability and blood pressure variability. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1999, 54, B219–B24. [Google Scholar] [CrossRef] [Green Version]
- Bertel, O.; Bühler, F.R.; Kiowski, W.; Lütold, B.E. Decreased Beta-adrenoreceptor responsiveness as related to age, blood pressure, and plasma catecholamines in patients with essential hypertension. Hypertension 1980, 2, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Karavirta, L.; Costa, M.D.; Goldberger, A.L.; Tulppo, M.P.; Laaksonen, D.E.; Nyman, K.; Keskitalo, M.; Häkkinen, A.; Häkkinen, K. Heart rate dynamics after combined strength and endurance training in middle-aged women: Heterogeneity of responses. PLoS ONE 2013, 8, e72664. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.D.; Tanaka, H.; Dinenno, F.A.; Seals, D.R. Central arterial compliance is associated with age- and habitual exercise-related differences in cardiovagal baroreflex sensitivity. Circulation 2001, 104, 1627–1632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, Y.; Galbreath, M.M.; Shibata, S.; Jarvis, S.S.; VanGundy, T.B.; Meier, R.L.; Vongpatanasin, W.; Levine, B.D.; Fu, Q. Relationship between sympathetic baroreflex sensitivity and arterial stiffness in elderly men and women. Hypertension 2012, 59, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Hunt, B.E.; Farquhar, W.B.; Taylor, J.A. Does reduced vascular stiffening fully explain preserved cardiovagal baroreflex function in older, physically active men? Circulation 2001, 103, 2424–2427. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.P.; Christou, D.D.; Jordan, J.; Seals, D.R. Baroreflex buffering is reduced with age in healthy men. Circulation 2003, 107, 1770–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Rovere, M.T.; Bigger, J.T.; Marcus, F.I.; Mortara, A.; Schwartz, P.J. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet 1998, 351, 478–484. [Google Scholar] [CrossRef]
- Lakatta, E.G.; Levy, D. Arterial and cardiac aging: Major shareholders in cardiovascular disease enterprises: Part I: Aging arteries: A “set up” for vascular disease. Circulation 2003, 107, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Arnett, D.K.; Boland, L.L.; Evans, G.W.; Riley, W.; Barnes, R.; Tyroler, H.A.; Heiss, G. Hypertension and arterial stiffness: The atherosclerosis risk in communities study. Am. J. Hypertens. 2000, 13, 317–323. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic stiffness is an independent predictor of all-cause and cardiovascular mortality in hypertensive patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [Green Version]
- Leon, A.S. Interaction of Aging and Exercise on the Cardiovascular System of Healthy Adults. Am. J. Lifestyle Med. 2012, 6, 368–375. [Google Scholar] [CrossRef]
- Warburton, D.E.; Charlesworth, S.; Ivey, A.; Nettlefold, L.; Bredin, S.S. A systematic review of the evidence for Canada’s Physical Activity Guidelines for Adults. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef] [PubMed]
- Piercy, K.L.; Troiano, R.P.; Ballard, R.M.; Carlson, S.A.; Fulton, J.E.; Galuska, D.A.; George, S.M.; Olson, R.D. The Physical Activity Guidelines for Americans. JAMA 2018, 320, 2020–2028. [Google Scholar] [CrossRef] [PubMed]
- Craighead, D.H.; Heinbockel, T.C.; Hamilton, M.N.; Bailey, E.F.; MacDonald, M.J.; Gibala, M.J.; Seals, D.R. Time-efficient physical training for enhancing cardiovascular function in midlife and older adults: Promise and current research gaps. J. Appl. Physiol. 2019, 127, 1427–1440. [Google Scholar] [CrossRef]
- McCraty, R.; Shaffer, F. Heart rate variability: New perspectives on physiological mechanisms, assessment of self-regulatory capacity, and health risk. Glob. Adv. Health Med. 2015, 4, 46–61. [Google Scholar] [CrossRef] [Green Version]
- Draghici, A.E.; Taylor, J.A. The physiological basis and measurement of heart rate variability in humans. J. Physiol. Anthropol. 2016, 35, 22. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [Green Version]
- Pumprla, J.; Howorka, K.; Groves, D.; Chester, M.; Nolan, J. Functional assessment of heart rate variability: Physiological basis and practical applications. Int. J. Cardiol. 2002, 84, 1–14. [Google Scholar] [CrossRef]
- Ernst, G. Heart-Rate Variability-More than Heart Beats? Front. Public Health 2017, 5, 240. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Cripps, T.R.; Malik, M.; Farrell, T.G.; Camm, A.J. Prognostic value of reduced heart rate variability after myocardial infarction: Clinical evaluation of a new analysis method. Br. Heart J. 1991, 65, 14–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algra, A.; Tijssen, J.G.; Roelandt, J.R.; Pool, J.; Lubsen, J. Heart rate variability from 24-hour electrocardiography and the 2-year risk for sudden death. Circulation 1993, 88, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, H.; Venditti, F.J.; Manders, E.S.; Evans, J.C.; Larson, M.G.; Feldman, C.L.; Levy, D. Reduced heart rate variability and mortality risk in an elderly cohort: The Framingham heart study. Circulation 1994, 90, 878–883. [Google Scholar] [CrossRef] [Green Version]
- Dekker, J.M.; Schouten, E.G.; Klootwijk, P.; Pool, J.; Swenne, C.A.; Kromhout, D. Heart rate variability from short electrocardiographic recordings predicts mortality from all causes in middle-aged and elderly men. The Zutphen Study. Am. J. Epidemiol. 1997, 145, 899–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huikuri, H.V.; Mäkikallio, T.H.; Airaksinen, K.E.; Seppänen, T.; Puukka, P.; Räihä, I.J.; Sourander, L.B. Power-law relationship of heart rate variability as a predictor of mortality in the elderly. Circulation 1998, 97, 2031–2036. [Google Scholar] [CrossRef] [Green Version]
- Lahiri, M.K.; Kannankeril, P.J.; Goldberger, J.J. Assessment of autonomic function in cardiovascular disease: Physiological basis and prognostic implications. J. Am. Coll. Cardiol. 2008, 51, 1725–1733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes de Godoy, M. Nonlinear Analysis of Heart Rate Variability: A Comprehensive Review. J. Cardiol. Ther. 2016, 3, 528–533. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnemeier, H.; Richardt, G.; Potratz, J.; Wiegand, U.K.H.; Brandes, A.; Kluge, N.; Katus, H.A. Circadian profile of cardiac autonomic nervous modulation in healthy subjects: Differing effects of aging and gender on heart rate variability. J. Cardiovasc. Electrophysiol. 2003, 14, 791–799. [Google Scholar] [CrossRef]
- Acharya, U.R.; Kannathal, N.; Sing, O.W.; Ping, L.Y.; Chua, T. Heart rate analysis in normal subjects of various age groups. Biomed. Eng. Online 2004, 3, 24. [Google Scholar] [CrossRef] [Green Version]
- Antelmi, I.; de Paula, R.S.; Shinzato, A.R.; Peres, C.A.; Mansur, A.J.; Grupi, C.J. Influence of age, gender, body mass index, and functional capacity on heart rate variability in a cohort of subjects without heart disease. Am. J. Cardiol. 2004, 93, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Moodithaya, S.; Avadhany, S.T. Gender differences in age-related changes in cardiac autonomic nervous function. J. Aging Res. 2012, 2012, 679345. [Google Scholar] [CrossRef] [Green Version]
- Voss, A.; Schroeder, R.; Heitmann, A.; Peters, A.; Perz, S. Short-term heart rate variability—Influence of gender and age in healthy subjects. PLoS ONE 2015, 10, e0118308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenfors, C.U.D.; Hanson, L.M.; Theorell, T.; Osika, W.S. Executive Cognitive Functioning and Cardiovascular Autonomic Regulation in a Population-Based Sample of Working Adults. Front. Psychol. 2016, 7, 1536. [Google Scholar] [CrossRef] [Green Version]
- Sammito, S. Alters- und Geschlechtsabhängige Referenzwerte für die Herzfrequenzvariabilität; Otto-von-Guericke-Universität Magdeburg: Magdeburg, Germany, 2017. [Google Scholar]
- Abhishekh, H.A.; Nisarga, P.; Kisan, R.; Meghana, A.; Chandran, S.; Trichur, R.; Sathyaprabha, T.N. Influence of age and gender on autonomic regulation of heart. J. Clin. Monit. Comput. 2013, 27, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Fatisson, J.; Oswald, V.; Lalonde, F. Influence diagram of physiological and environmental factors affecting heart rate variability: An extended literature overview. Heart Int. 2016, 11, e32–e40. [Google Scholar] [CrossRef]
- Sammito, S.; Böckelmann, I. Factors influencing heart rate variability. ICFJ 2016, 6, 242. [Google Scholar] [CrossRef]
- Grässler, B.; Thielmann, B.; Böckelmann, I.; Hökelmann, A. Effects of different training interventions on heart rate variability and cardiovascular health and risk factors in young and middle-aged adults: A systematic review. Front. Physiol. 2021, 12, 532. [Google Scholar] [CrossRef]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training programs in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef] [PubMed]
- Raffin, J.; Barthélémy, J.-C.; Dupré, C.; Pichot, V.; Berger, M.; Féasson, L.; Busso, T.; Da Costa, A.; Colvez, A.; Montuy-Coquard, C.; et al. Exercise Frequency Determines Heart Rate Variability Gains in Older People: A Meta-Analysis and Meta-Regression. Sports Med. 2019, 49, 719–729. [Google Scholar] [CrossRef]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Merellano-Navarro, E.; Gusi, N. Physical Exercise Improves Heart Rate Variability in Patients with Type 2 Diabetes: A Systematic Review. Curr. Diab. Rep. 2017, 17, 110. [Google Scholar] [CrossRef]
- Belvederi Murri, M.; Folesani, F.; Zerbinati, L.; Nanni, M.G.; Ounalli, H.; Caruso, R.; Grassi, L. Physical Activity Promotes Health and Reduces Cardiovascular Mortality in Depressed Populations: A Literature Overview. Int. J. Environ. Res. Public Health 2020, 17, 5545. [Google Scholar] [CrossRef]
- Palma, S.; Keilani, M.; Hasenoehrl, T.; Crevenna, R. Impact of supportive therapy modalities on heart rate variability in cancer patients—A systematic review. Disabil. Rehabil. 2020, 42, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Laborde, S.; Mosley, E.; Thayer, J.F. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research—Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Front. Psychol. 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Levy, W.C.; Cerqueira, M.D.; Harp, G.D.; Johannessen, K.-A.; Abrass, I.B.; Schwartz, R.S.; Stratton, J.R. Effect of endurance exercise training on heart rate variability at rest in healthy young and older men. Am. J. Cardiol. 1998, 82, 1236–1241. [Google Scholar] [CrossRef]
- Soares-Miranda, L.; Sattelmair, J.; Chaves, P.; Duncan, G.E.; Siscovick, D.S.; Stein, P.K.; Mozaffarian, D. Physical activity and heart rate variability in older adults: The Cardiovascular Health Study. Circulation 2014, 129, 2100–2110. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int. J. Evid. Based Healthc. 2015, 13, 9–18. [Google Scholar] [CrossRef]
- Dobbs, W.C.; Fedewa, M.V.; MacDonald, H.V.; Holmes, C.J.; Cicone, Z.S.; Plews, D.J.; Esco, M.R. The Accuracy of Acquiring Heart Rate Variability from Portable Devices: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 417–435. [Google Scholar] [CrossRef]
- Karavirta, L.; Tulppo, M.P.; Laaksonen, D.E.; Nyman, K.; Laukkanen, R.T.; Kinnunen, H.; Häkkinen, A.; Häkkinen, K. Heart rate dynamics after combined endurance and strength training in older men. Med. Sci. Sports Exerc. 2009, 41, 1436–1443. [Google Scholar] [CrossRef]
- Shen, T.-W.; Wen, H.-J. Aerobic exercise affects T-wave alternans and heart rate variability in postmenopausal women. Int. J. Sports Med. 2013, 34, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- De Rezende Barbosa, M.; Vanderlei, L.; Neves, L.M.; Takahashi, C.; Torquato, P.; Fortaleza, A.; Freitas Junior, I.F.; Sorpreso, I.; Abreu, L.C.; Perez Riera, A.R. Impact of functional training on geometric indices and fractal correlation property of heart rate variability in postmenopausal women. Ann. Noninvasive Electrocardiol. 2018, 23, 12469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, V.A.; Verheyden, B.; Aubert, A.E.; Fagard, R.H. Effects of aerobic training intensity on resting, exercise and post-exercise blood pressure, heart rate and heart-rate variability. J. Hum. Hypertens. 2010, 24, 175–182. [Google Scholar] [CrossRef]
- Deley, G.; Picard, G.; Taylor, J.A. Arterial baroreflex control of cardiac vagal outflow in older individuals can be enhanced by aerobic exercise training. Hypertension 2009, 53, 826–832. [Google Scholar] [CrossRef] [Green Version]
- Jakubec, A.; Stejskal, P.; Kovácová, L.; Elfmark, M.; Rehová, I.; Botek, M.; Petr, M. Changes in heart rate variability after a six month long aerobic dance or step-dance programm in women 40-65 years old: The influence of different degrees of adherence, intensity and initial levels. Acta Univ. Palacki. Olomuc. Gymnica 2008, 38, 35–44. [Google Scholar]
- Gerhart, H.; Tai, Y.L.; Fennell, C.; Mayo, X.; Kingsley, J.D. Autonomic Modulation in Older Women: Using Resistance Exercise as a Countermeasure. Int. J. Exerc. Sci. 2017, 10, 178–187. [Google Scholar]
- Huikuri, H.V.; Pikkujämsä, S.M.; Airaksinen, K.E.; Ikäheimo, M.J.; Rantala, A.O.; Kauma, H.; Lilja, M.; Kesäniemi, Y.A. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 1996, 94, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Fagard, R.H. A population-based study on the determinants of heart rate and heart rate variability in the frequency domain. Verh. K. Acad. Geneeskd. Belg. 2001, 63, 57–89, discussion 90–91. [Google Scholar]
- Okazaki, K.; Iwasaki, K.-I.; Prasad, A.; Palmer, M.D.; Martini, E.R.; Fu, Q.; Arbab-Zadeh, A.; Zhang, R.; Levine, B.D. Dose-response relationship of endurance training for autonomic circulatory control in healthy seniors. J. Appl. Physiol. 2005, 99, 1041–1049. [Google Scholar] [CrossRef]
- Iwasaki, K.-I.; Zhang, R.; Zuckerman, J.H.; Levine, B.D. Dose-response relationship of the cardiovascular adaptation to endurance training in healthy adults: How much training for what benefit? J. Appl. Physiol. 2003, 95, 1575–1583. [Google Scholar] [CrossRef] [Green Version]
- Uusitalo, A.L.T.; Laitinen, T.; Väisänen, S.B.; Länsimies, E.; Rauramaa, R. Physical training and heart rate and blood pressure variability: A 5-yr randomized trial. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H1821–H1826. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, B.; Eijnde, B.O.; Beckers, F.; Vanhees, L.; Aubert, A.E. Low-dose exercise training does not influence cardiac autonomic control in healthy sedentary men aged 55–75 years. J. Sports Sci. 2006, 24, 1137–1147. [Google Scholar] [CrossRef]
- Martinmaki, K.; Hakkinen, K.; Mikkola, J.; Rusko, H. Effect of low-dose endurance training on heart rate variability at rest and during an incremental maximal exercise test. Eur. J. Appl. Physiol. 2008, 104, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Da Costa de Rezende Barbosa, M.P.; da Silva, A.K.F.; Bernardo, A.F.B.; de Souza, N.M.; Neto Junior, J.; Pastre, C.M.; Vanderlei, L.C.M. Influence of resistance training on cardiac autonomic modulation: Literature review. Med. Express 2014, 1, 284–288. [Google Scholar] [CrossRef] [Green Version]
- Taylor, A.C.; McCartney, N.; Kamath, M.V.; Wiley, R.L. Isometric training lowers resting blood pressure and modulates autonomic control. Med. Sci. Sports Exerc. 2003, 35, 251–256. [Google Scholar] [CrossRef]
- Nürnberger, J.; Kribben, A.; Philipp, T.; Erbel, R. Die arterielle Compliance (Gefässsteifigkeit) zur Aufdeckung einer subklinischen Atherosklerose. Herz 2007, 32, 379–386. [Google Scholar] [CrossRef]
- Sandercock, G.R.H.; Bromley, P.D.; Brodie, D.A. Effects of exercise on heart rate variability: Inferences from meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Hottenrott, K.; Hoos, O.; Esperer, H.D. Heart rate variability and physical exercise. Current status. Herz 2006, 31, 544–552. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Boukhris, O.; Halfpaap, N.; Labott, B.K.; Langhans, C.; Herold, F.; Grässler, B.; Müller, P.; Trabelsi, K.; Chtourou, H.; et al. Four Weeks of Detraining Induced by COVID-19 Reverse Cardiac Improvements from Eight Weeks of Fitness-Dance Training in Older Adults with Mild Cognitive Impairment. Int. J. Environ. Res. Public Health 2021, 18, 5930. [Google Scholar] [CrossRef] [PubMed]
- Cooke, W.H.; Carter, J.R. Strength training does not affect vagal-cardiac control or cardiovagal baroreflex sensitivity in young healthy subjects. Eur. J. Appl. Physiol. 2005, 93, 719–725. [Google Scholar] [CrossRef]
- Badrov, M.B.; Bartol, C.L.; DiBartolomeo, M.A.; Millar, P.J.; McNevin, N.H.; McGowan, C.L. Effects of isometric handgrip training dose on resting blood pressure and resistance vessel endothelial function in normotensive women. Eur. J. Appl. Physiol. 2013, 113, 2091–2100. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Fahs, C.A.; Shinsako, K.K.; Jae, S.Y.; Fernhall, B. Heart rate recovery and heart rate complexity following resistance exercise training and detraining in young men. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H3180–H3186. [Google Scholar] [CrossRef] [Green Version]
- Heffernan, K.S.; Jae, S.Y.; Vieira, V.J.; Iwamoto, G.A.; Wilund, K.R.; Woods, J.A.; Fernhall, B. C-reactive protein and cardiac vagal activity following resistance exercise training in young African-American and white men. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2009, 296, R1098–R1105. [Google Scholar] [CrossRef] [Green Version]
- Valenzuela, T. Efficacy of progressive resistance training interventions in older adults in nursing homes: A systematic review. J. Am. Med. Dir. Assoc. 2012, 13, 418–428. [Google Scholar] [CrossRef]
- Milburn, S.; Butts, N.K. A comparison of the training responses to aerobic dance and jogging in college females. Med. Sci. Sports Exerc. 1983, 15, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; McKinney, J.S.; Carleton, R.A. Is aerobic dance an effective alternative to walk-jog exercise training? J. Sports Med. Phys. Fit. 1992, 32, 136–141. [Google Scholar]
- Filliau, C.; Younes, M.; Blanchard, A.-L.; Piscione, J.; van de Louw, A.; Seguret, C.; Israel, J.; Cottin, F. Effect of “Touch Rugby” Training on the Cardiovascular Autonomic Control In Sedentary Subjects. Int. J. Exerc. Sci. 2015, 36, 567–572. [Google Scholar] [CrossRef]
- Katona, P.G.; McLean, M.; Dighton, D.H.; Guz, A. Sympathetic and parasympathetic cardiac control in athletes and nonathletes at rest. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1982, 52, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Junior, A.F.; Schamne, J.C.; Perandini, L.A.B.; Chimin, P.; Okuno, N.M. Effects of Walking Training with Restricted Blood Flow on HR and HRV Kinetics and HRV Recovery. Int. J. Sports Med. 2019, 40, 585–591. [Google Scholar] [CrossRef]
- Darr, K.C.; Bassett, D.R.; Morgan, B.J.; Thomas, D.P. Effects of age and training status on heart rate recovery after peak exercise. Am. J. Physiol. 1988, 254, H340–H343. [Google Scholar] [CrossRef] [PubMed]
- Routledge, F.S.; Campbell, T.S.; McFetridge-Durdle, J.A.; Bacon, S.L. Improvements in heart rate variability with exercise therapy. Can. J. Cardiol. 2010, 26, 303–312. [Google Scholar] [CrossRef] [Green Version]
- De Abreu, R.M.; Rehder-Santos, P.; Simões, R.P.; Catai, A.M. Can high-intensity interval training change cardiac autonomic control? A systematic review. Braz. J. Phys. Ther. 2019, 23, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Cornelissen, V.A.; Fagard, R.H. Effects of endurance training on blood pressure, blood pressure-regulating mechanisms, and cardiovascular risk factors. Hypertension 2005, 46, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Gronwald, T.; Rogers, B.; Hoos, O. Fractal Correlation Properties of Heart Rate Variability: A New Biomarker for Intensity Distribution in Endurance Exercise and Training Prescription? Front. Physiol. 2020, 11, 550572. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.D.; Dinenno, F.A.; Tanaka, H.; Clevenger, C.M.; DeSouza, C.A.; Seals, D.R. Regular aerobic exercise modulates age-associated declines in cardiovagal baroreflex sensitivity in healthy men. J. Physiol. 2000, 529, 263–271. [Google Scholar] [CrossRef]
- Martins, D.; Nelson, K.; Pan, D.; Tareen, N.; Norris, K. The effect of gender on age-related blood pressure changes and the prevalence of isolated systolic hypertension among older adults: Data from NHANES III. J. Gend. Specif. Med. 2001, 4, 10–13, 20. [Google Scholar] [PubMed]
- Eckel, R.H.; Jakicic, J.M.; Ard, J.D.; de Jesus, J.M.; Houston Miller, N.; van Hubbard, S.; Lee, I.-M.; Lichtenstein, A.H.; Loria, C.M.; Millen, B.E.; et al. 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk. J. Am. Pharm. Assoc. 2014, 63, 2960–2984. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study | Participants (Sample Size, Age (Year), and Gender) | HRV Protocol (Method, Respiration, Position, and Sampling Frequency) | HRV Measures | Secondary Outcomes | Analysis Length | Intervention (Type, Duration, and Sessions/Week) | Control Group |
|---|---|---|---|---|---|---|---|
| [3] | 90 (E: 26; R: 26; ER: 21; CG: 17) Age: 49−52 ± 6-8 (E: 52 ± 7; S: 52 ± 8; ES: 49 ± 6; CG: 52 ± 8) 100% women | Polar RS810i belt Spontaneous Supine n. r. | CI, HF, LF, LF/HF, RHR, and SDNN | Approx. 600 beats | Endurance, strength, and combined endurance and strength 21 weeks E and R: 2, ER: 4 sessions | yes | |
| [55] | 93 (E: 23; R: 25; ER: 29; CG: 16) Age: 55.6 ± 7.4 100% men | Polar RS810i belt Spontaneous Supine 1.000 Hz | ln HF, ln LF, RHR, and α1 | VO2 max | 5 min | Endurance, strength, and combined endurance and strength 21 weeks E and R: 2, ER: 4 sessions | yes |
| [56] | 44 (TG 22; CG 22) Age: 58.48 ± 0.53 (EG: 57.86 ± 0.64; CG: 59.10 ± 0.83) 100% women | 3-lead ECG n. r. n. r. 500 Hz | CV, HF nu, LF nu, LF/HF, mRR, NN20, NN50, pNN20, pNN50, RHR, RMSSD, SDNN, SDSD, TP, and VLF | BF, BMI, BM, and VO2 max | 5 min | Coordinative (step aerobics) 10 weeks 3 sessions | yes |
| [57] | 39 (TG: 19; CG: 20) Age: TG: 50 ± 4.5; CG: 58.45 ± 4.8 100% women | Polar RS800 belt Spontaneous Supine n.r. | DFA total, RRTri, SD1, SD2, SD1/SD2, TINN, α1, α2, and α1/α2 | 1000 consecutive beats | Multimodal (functional training and walking) 16 weeks 3 sessions | yes | |
| [58] | 36 Age: 59 (range: 55–71) 19 women, 17 men | 3-lead ECG Spontaneous Sitting n.r. | HF%, LF%, ln LF/HF, RHR, and TP | HRR, SBP at rest and during ergometer test | 512 consecutive beats | Endurance (walking, jogging, running, cycling, and stepping); crossover design: 10 weeks LI or HI + 10 weeks sedentary + 10 weeks HI or LI 10 weeks 3 sessions | crossover design |
| [59] | 12 Age: 59 ± 5 5 women, 7 men | ECG 15 breaths/min n.r. n.r. | mRR, RHR, and RSA | BM, BMI, BR, DBP, SBP, VO2 max, and WR | 5 min | Endurance (treadmill, elliptical trainer, or bicycle) 24 weeks 4 sessions | no |
| [60] | 44 Age: 47.3 ± 5.4 100% women | Varia Cardio TF4, ECG belt n.r. Supine n.r. | HF, HF%, LF, LF/HF, LF%, MSSD, RHR, TP, VLF, VLF%, VLF/HF, and VLF/LF | BM, BMI, and VO2 max | 5 min | Coordinative (aerobic dance or step-dance) 24 weeks 3 sessions | no |
| [61] | 23 Age: 59 ± 6 100% women | ECG 12 breaths/min Supine 1.000 Hz | HF nu, LF nu, LF/HF, ln HF, ln LF, ln TP, RHR, and SampEn | BP | 5 min | Resistance 12 weeks 2 sessions | no |
| Author, Year | Heart Rate-Related Parameters | Secondary Health Factors | TESTEX | STARDHRV |
|---|---|---|---|---|
| [3] | E: ↑ CI, HF, and LF; ↓ LF/HF, RHR, and SDNN. R: ↑ CI, HF, LF, and SDNN; ↓ LF/HF, and RHR. ER: ↑ LF/HF; ↔ RHR; ↓ CI, HF, LF, and SDNN, | 9 | 20 | |
| [55] | E: ↑ ln HF; ↔ ln LF; ↓ RHR* and α1. R: ↔ α1; ↓ ln HF, ln LF, and RHR. ER: ↑ ln HF; ↓ ln LF, RHR*, and α1* | ↑ VO2 max (E* and ER*); ↔ VO2 max (R) | 7.5 | 20 |
| [56] | ↑ HF nu* and RHR; ↓ CV*, LF nu*, and LF/HF*, mRR, NN20*, NN50, pNN20, pNN50*, RMSSD, SDSD, SDNN*, TP, and VLF | ↑ BF and VO2 max*; ↓ BM and BMI | 9 | 18 |
| [57] | ↑ RRTri, SD1*, SD2, SD1/SD2, α1*, and α1/α2*; ↓ DFA total, TINN, and α2 | 6 | 19 | |
| [58] | LI and HI: ↑ ln LF/HF and TP (LI*); ↓ HF%, LF% and RHR* | LI and HI: ↑ HRR*; ↓ SBP (rest*, 40 W*, 80 W and 120 W) | 5 | 19.5 |
| [59] | ↑ mRR* and RSA*; ↓ RHR* | ↑ VO2 max*; ↓ BF*, BM*, BMI*, BR*, DBP, SBP* and WR | 8 | 16.5 |
| [60] | ↑ HF, HF%, LF/HF, LF%, and VLF/HF; ↔ RR; ↓ LF, MSSD, TP, VLF, VLF/LF, and VLF% | ↓ BM* and BMI*; ↑ VO2 max* | 4.5 | 15 |
| [61] | ↑ LF nu, LF/HF, and SampEn; ↔ ln LF and ln TP; ↓ HF nu, ln HF, and RHR | ↑ SBP; ↓ DBP | 7 | 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grässler, B.; Thielmann, B.; Böckelmann, I.; Hökelmann, A. Effects of Different Exercise Interventions on Cardiac Autonomic Control and Secondary Health Factors in Middle-Aged Adults: A Systematic Review. J. Cardiovasc. Dev. Dis. 2021, 8, 94. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080094
Grässler B, Thielmann B, Böckelmann I, Hökelmann A. Effects of Different Exercise Interventions on Cardiac Autonomic Control and Secondary Health Factors in Middle-Aged Adults: A Systematic Review. Journal of Cardiovascular Development and Disease. 2021; 8(8):94. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080094
Chicago/Turabian StyleGrässler, Bernhard, Beatrice Thielmann, Irina Böckelmann, and Anita Hökelmann. 2021. "Effects of Different Exercise Interventions on Cardiac Autonomic Control and Secondary Health Factors in Middle-Aged Adults: A Systematic Review" Journal of Cardiovascular Development and Disease 8, no. 8: 94. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd8080094