
A Systematic Review of Adherence to Immunosuppression among Pediatric Heart Transplant Patients


Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection and Data Extraction
2.5. Assessment of Risk of Bias
2.6. Data Synthesis
3. Results
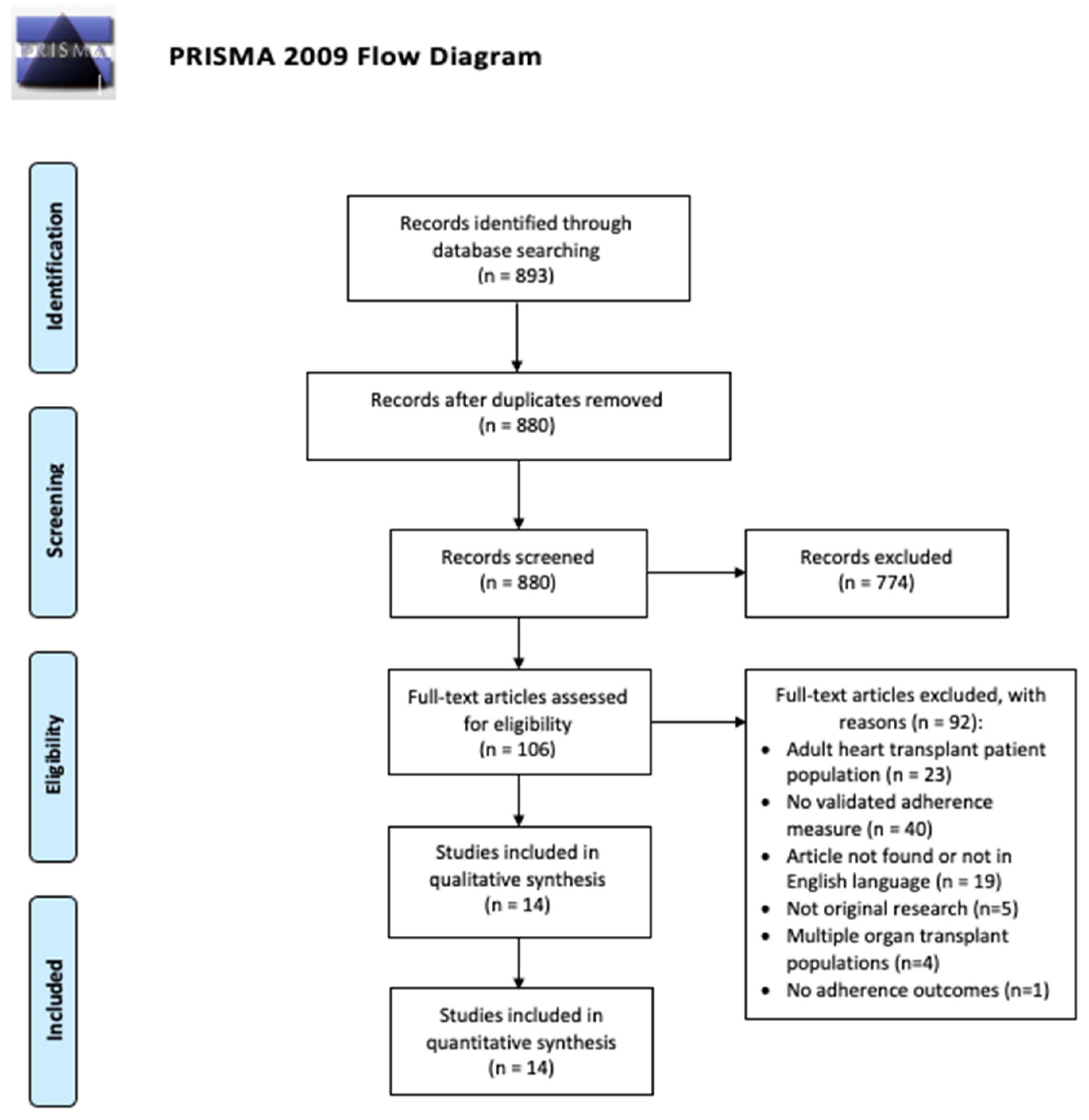
3.1. Literature Search
3.2. Study Characteristics
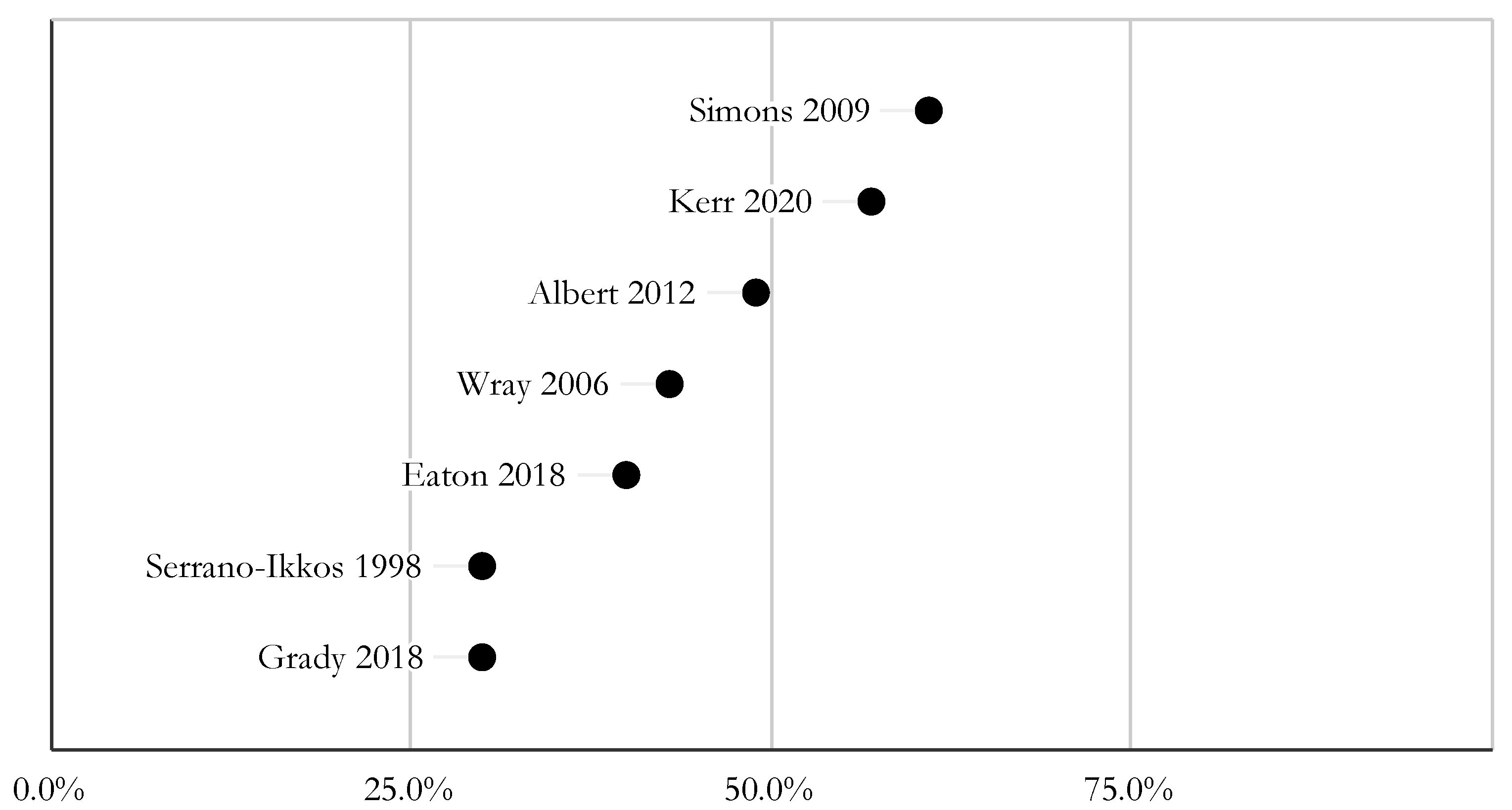
3.3. Measures and Rates of Nonadherence
3.4. CNI Levels as a Marker for Nonadherence and Poor Outcomes
3.5. Impact of Nonadherence on Quality of Life and Mental Health
3.6. The Effect of Transition Programs on Adherence
3.7. Studies’ Methodological Quality
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
- #1
- MeSH descriptor: [Heart Transplantation] explode all trees
- #2
- “heart transplant*”:ti,ab
- #3
- #1 OR #2
- #4
- MeSH descriptor: [Organ Transplantation] explode all trees
- #5
- transplant*:ti,ab
- #6
- MeSH descriptor: [Heart] explode all trees
- #7
- heart:ti,ab
- #8
- #4 OR #5
- #9
- #6 OR #7
- #10
- #8 AND #9
- #11
- #3 OR #10
- #12
- MeSH descriptor: [Medication Adherence] explode all trees
- #13
- MeSH descriptor: [Patient Compliance] explode all trees
- #14
- (“adherence” OR “nonadherence” OR “non adherence” OR “compliance” OR “noncompliance” OR “non compliance”).ti,ab
References
- Thrush, P.T.; Hoffman, T.M. Pediatric heart transplantation-indications and outcomes in the current era. J. Thorac. Dis. 2014, 6, 1080–1096. [Google Scholar] [CrossRef] [PubMed]
- D’Addese, L.; Joong, A.; Burch, M.; Pahl, E. Pediatric heart transplantation in the current era. Curr. Opin. Pediatr. 2019, 31, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Rossano, J.W.; Singh, T.P.; Cherikh, W.S.; Chambers, D.C.; Harhay, M.O.; Hayes, D., Jr.; Hsich, E.; Khush, K.K.; Meiser, B.; Potena, L.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Twenty-second pediatric heart transplantation report-2019; Focus theme: Donor and recipient size match. J. Heart Lung Transplant. 2019, 38, 1028–1041. [Google Scholar] [CrossRef] [PubMed]
- Azzi, J.R.; Sayegh, M.H.; Mallat, S.G. Calcineurin Inhibitors: 40 Years Later, Can’t Live without …. J. Immunol. 2013, 191, 5785–5791. [Google Scholar] [CrossRef] [Green Version]
- Oliva, M.; Singh, T.P.; Gauvreau, K.; Vanderpluym, C.J.; Bastardi, H.J.; Almond, C.S. Impact of medication non-adherence on survival after pediatric heart transplantation in the U.S.A. J. Heart Lung Transplant. 2013, 32, 881–888. [Google Scholar] [CrossRef]
- Simons, L.E.; Gilleland, J.; Blount, R.L.; Amaral, S.; Berg, A.; Mee, L.L. Multidimensional Adherence Classification System: Initial development with adolescent transplant recipients. Pediatr. Transplant. 2009, 13, 590–598. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 September 2021).
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Anton, C.M.; Anton, K.; Butts, R.J. Preparing for transition: The effects of a structured transition program on adolescent heart transplant patients’ adherence and transplant knowledge. Pediatr. Transplant. 2019, 23, e13544. [Google Scholar] [CrossRef]
- Devine, K.A.; Reed-Knight, B.; Loiselle, K.A.; Simons, L.E.; Mee, L.L.; Blount, R.L. Predictors of long-term health-related quality of life in adolescent solid organ transplant recipients. J. Pediatr. Psychol. 2011, 36, 891–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, C.K.; Gutierrez-Colina, A.M.; Quast, L.F.; Liverman, R.; Lee, J.L.; Mee, L.L.; Reed-Knight, B.; Cushman, G.; Chiang, G.; Romero, R.; et al. Multimethod Assessment of Medication Nonadherence and Barriers in Adolescents and Young Adults with Solid Organ Transplants. J. Pediatr. Psychol. 2018, 43, 789–799. [Google Scholar] [CrossRef] [PubMed]
- Flippin, M.S.; Canter, C.E.; Balzer, D.T. Increased morbidity and high variability of cyclosporine levels in pediatric heart transplant recipients. J. Heart Lung Transplant. 2000, 19, 343–349. [Google Scholar] [CrossRef]
- Grady, K.L.; Andrei, A.C.; Shankel, T.; Chinnock, R.; Miyamoto, S.D.; Ambardekar, A.V.; Anderson, A.; Addonizio, L.; Latif, F.; Lefkowitz, D.; et al. Pediatric Heart Transplantation: Transitioning to Adult Care (TRANSIT): Feasibility of a Pilot Randomized Controlled Trial. J. Card. Fail. 2019, 25, 948–958. [Google Scholar] [CrossRef]
- Grady, K.L.; Hof, K.V.; Andrei, A.C.; Shankel, T.; Chinnock, R.; Miyamoto, S.; Ambardekar, A.V.; Anderson, A.; Addonizio, L.; Latif, F.; et al. Pediatric Heart Transplantation: Transitioning to Adult Care (TRANSIT): Baseline Findings. Pediatr. Cardiol. 2018, 39, 354–364. [Google Scholar] [CrossRef]
- Kerr, S.M.; Jorgensen, N.W.; Hong, B.J.; Friedland-Little, J.M.; Albers, E.L.; Newland, D.M.; Law, Y.M.; Kemna, M.S. Assessment of rejection risk following subtherapeutic calcineurin inhibitor levels after pediatric heart transplantation. Pediatr. Transplant. 2020, 24, e13616. [Google Scholar] [CrossRef]
- McCormick, A.D.; Schumacher, K.R.; Zamberlan, M.; Uzark, K.; Yu, S.; Lowery, R.; Rottach, N.; Cousino, M.K. Generalized and specific anxiety in adolescents following heart transplant. Pediatr. Transplant. 2020, 24, e13647. [Google Scholar] [CrossRef]
- Ringewald, J.M.; Gidding, S.S.; Crawford, S.E.; Backer, C.L.; Mavroudis, C.; Pahl, E. Nonadherence is associated with late rejection in pediatric heart transplant recipients. J. Pediatr. 2001, 139, 75–78. [Google Scholar] [CrossRef]
- Wolfe, K.R.; Kelly, S.L.; Steinberg, E.; Pliego, J.; Everitt, M.D. Predictors of neuropsychological functioning and medication adherence in pediatric heart transplant recipients referred for neuropsychological evaluation. Pediatr. Transplant. 2020, 24, e13615. [Google Scholar] [CrossRef]
- Wray, J.; Waters, S.; Radley-Smith, R.; Sensky, T. Adherence in adolescents and young adults following heart or heart-lung transplantation. Pediatr. Transplant. 2006, 10, 694–700. [Google Scholar] [CrossRef]
- Serrano-Ikkos, E.; Lask, B.; Whitehead, B.; Eisler, I. Incomplete adherence after pediatric heart and heart-lung transplantation. J. Heart Lung Transplant. 1998, 17, 1177–1183. [Google Scholar] [PubMed]
- Albert, W.; Hudalla, A.; Traue, K.; Hetzer, R. Impact of heart transplantation in infancy and adolescence on quality of life and compliance. HSR Proc. Intensive Care Cardiovasc. Anesth. 2012, 4, 125–129. [Google Scholar] [PubMed]
- Goetzmann, L.; Klaghofer, R.; Spindler, A.; Wagner-Huber, R.; Scheuer, E.; Buddeberg, C. The “Medication Experience Scale for Immunosuppressants” (MESI): Initial results for a new screening instrument in transplant medicine. Psychother. Psychosom. Med. Psychol. 2006, 56, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Zelikovsky, N.; Schast, A.P. Eliciting accurate reports of adherence in a clinical interview: Development of the Medical Adherence Measure. Pediatr. Nurs. 2008, 34, 141–146. [Google Scholar]
- Shemesh, E.; Bucuvalas, J.C.; Anand, R.; Mazariegos, G.V.; Alonso, E.M.; Venick, R.S.; Reyes-Mugica, M.; Annunziato, R.A.; Shneider, B.L. The Medication Level Variability Index (MLVI) Predicts Poor Liver Transplant Outcomes: A Prospective Multi-Site Study. Am. J. Transplant. 2017, 17, 2668–2678. [Google Scholar] [CrossRef]
- Grady, K.L.; Jalowiec, A.; White-Williams, C. Patient compliance at one year and two years after heart transplantation. J. Heart Lung Transplant. 1998, 17, 383–394. [Google Scholar]
- Hussain, T.; Nassetta, K.; O’Dwyer, L.C.; Wilcox, J.E.; Badawy, S.M. Adherence to immunosuppression in adult heart transplant recipients: A systematic review. Transplant. Rev. 2021, 35, 100651. [Google Scholar] [CrossRef]
- Peipert, J.D.; Badawy, S.M.; Baik, S.H.; Oswald, L.B.; Efficace, F.; Garcia, S.F.; Mroczek, D.K.; Wolf, M.; Kaiser, K.; Yanez, B.; et al. Development of the NIH Patient-Reported Outcomes Measurement Information System (PROMIS) Medication Adherence Scale (PMAS). Patient Prefer. Adherence 2020, 14, 971–983. [Google Scholar] [CrossRef]
- Gueta, I.; Markovits, N.; Yarden-Bilavsky, H.; Raichlin, E.; Freimark, D.; Lavee, J.; Loebstein, R.; Peled, Y. High tacrolimus trough level variability is associated with rejections after heart transplant. Am. J. Transplant. 2018, 18, 2571–2578. [Google Scholar] [CrossRef] [Green Version]
- Sirota, M.; Heyrend, C.; Ou, Z.; Masotti, S.; Griffiths, E.; Molina, K. Impact of tacrolimus variability on pediatric heart transplant outcomes. Pediatr. Transplant. 2021, 25, e14043. [Google Scholar] [CrossRef]
- Dipchand, A.I.; Laks, J.A. Pediatric heart transplantation: Long-term outcomes. Indian J. Thorac. Cardiovasc. Surg. 2020, 36, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Shuker, N.; Bouamar, R.; Hesselink, D.A.; van Gelder, T.; Caliskan, K.; Manintveld, O.C.; Balk, A.H.; Constantinescu, A.A. Intrapatient Variability in Tacrolimus Exposure Does Not Predict The Development of Cardiac Allograft Vasculopathy After Heart Transplant. Exp. Clin. Transplant. 2018, 16, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pahl, E.; Naftel, D.C.; Kuhn, M.A.; Shaddy, R.E.; Morrow, W.R.; Canter, C.E.; Kirklin, J.; Pediatric Heart Transplant Study. The impact and outcome of transplant coronary artery disease in a pediatric population: A 9-year multi-institutional study. J. Heart Lung Transplant. 2005, 24, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Schmauss, D.; Weis, M. Cardiac allograft vasculopathy: Recent developments. Circulation 2008, 117, 2131–2141. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Thompson, A.A.; Kuhns, L.M. Medication Adherence and Technology-Based Interventions for Adolescents With Chronic Health Conditions: A Few Key Considerations. JMIR Mhealth Uhealth 2017, 5, e202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badawy, S.M.; Kuhns, L.M. Texting and Mobile Phone App Interventions for Improving Adherence to Preventive Behavior in Adolescents: A Systematic Review. JMIR Mhealth Uhealth 2017, 5, e50. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.C.; O’Dwyer, L.C.; Badawy, S.M. Telemedicine in Malignant and Nonmalignant Hematology: Systematic Review of Pediatric and Adult Studies. JMIR Mhealth Uhealth 2021, 9, e29619. [Google Scholar] [CrossRef]
- Badawy, S.M.; Abebe, K.Z.; Reichman, C.A.; Checo, G.; Hamm, M.E.; Stinson, J.; Lalloo, C.; Carroll, P.; Saraf, S.L.; Gordeuk, V.R.; et al. Comparing the Effectiveness of Education Versus Digital Cognitive Behavioral Therapy for Adults with Sickle Cell Disease: Protocol for the Cognitive Behavioral Therapy and Real-time Pain Management Intervention for Sickle Cell via Mobile Applications (CaRISMA) Study. JMIR Res. Protoc. 2021, 10, e29014. [Google Scholar] [CrossRef]
- Shah, A.C.; Badawy, S.M. Telemedicine in Pediatrics: Systematic Review of Randomized Controlled Trials. JMIR Pediatr. Parent. 2021, 4, e22696. [Google Scholar] [CrossRef]
- Badawy, S.M.; Radovic, A. Digital Approaches to Remote Pediatric Health Care Delivery During the COVID-19 Pandemic: Existing Evidence and a Call for Further Research. JMIR Pediatr. Parent. 2020, 3, e20049. [Google Scholar] [CrossRef]
- Alberts, N.M.; Badawy, S.M.; Hodges, J.; Estepp, J.H.; Nwosu, C.; Khan, H.; Smeltzer, M.P.; Homayouni, R.; Norell, S.; Klesges, L.; et al. Development of the InCharge Health Mobile App to Improve Adherence to Hydroxyurea in Patients With Sickle Cell Disease: User-Centered Design Approach. JMIR Mhealth Uhealth 2020, 8, e14884. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, W.A.; Heidelberg, R.E.; Gilbert, A.M.; Heneghan, M.B.; Badawy, S.M.; Alberts, N.M. eHealth and mHealth interventions in pediatric cancer: A systematic review of interventions across the cancer continuum. Psychooncology 2020, 29, 17–37. [Google Scholar] [CrossRef] [PubMed]
- Radovic, A.; Badawy, S.M. Technology Use for Adolescent Health and Wellness. Pediatrics 2020, 145, S186–S194. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Morrone, K.; Thompson, A.; Palermo, T.M. Computer and mobile technology interventions to promote medication adherence and disease management in people with thalassemia. Cochrane Database Syst. Rev. 2019, 6, CD012900. [Google Scholar] [CrossRef]
- Badawy, S.M.; Cronin, R.M.; Hankins, J.; Crosby, L.; DeBaun, M.; Thompson, A.A.; Shah, N. Patient-Centered eHealth Interventions for Children, Adolescents, and Adults With Sickle Cell Disease: Systematic Review. J. Med. Internet Res. 2018, 20, e10940. [Google Scholar] [CrossRef] [Green Version]
- Badawy, S.M.; Barrera, L.; Sinno, M.G.; Kaviany, S.; O’Dwyer, L.C.; Kuhns, L.M. Text Messaging and Mobile Phone Apps as Interventions to Improve Adherence in Adolescents With Chronic Health Conditions: A Systematic Review. JMIR Mhealth Uhealth 2017, 5, e66. [Google Scholar] [CrossRef] [Green Version]
- Gomis-Pastor, M.; Mirabet Perez, S.; Roig Minguell, E.; Brossa Loidi, V.; Lopez Lopez, L.; Ros Abarca, S.; Galvez Tugas, E.; Mas-Malagarriga, N.; Mangues Bafalluy, M.A. Mobile Health to Improve Adherence and Patient Experience in Heart Transplantation Recipients: The mHeart Trial. Healthcare 2021, 9, 463. [Google Scholar] [CrossRef]
- Abasi, S.; Yazdani, A.; Kiani, S.; Mahmoudzadeh-Sagheb, Z. Effectiveness of mobile health-based self-management application for posttransplant cares: A systematic review. Health Sci. Rep. 2021, 4, e434. [Google Scholar] [CrossRef]
- Stehlik, J.; Kobashigawa, J.; Hunt, S.A.; Reichenspurner, H.; Kirklin, J.K. Honoring 50 Years of Clinical Heart Transplantation in Circulation. Circulation 2018, 137, 71–87. [Google Scholar] [CrossRef]
- Kobashigawa, J.; Miller, L.; Renlund, D.; Mentzer, R.; Alderman, E.; Bourge, R.; Costanzo, M.; Eisen, H.; Dureau, G.; Ratkovec, R.; et al. A randomized active-controlled trial of mycophenolate mofetil in heart transplant recipients. Mycophenolate Mofetil Investigators. Transplantation 1998, 66, 507–515. [Google Scholar] [CrossRef]
- Doesch, A.O.; Mueller, S.; Akyol, C.; Erbel, C.; Frankenstein, L.; Ruhparwar, A.; Ehlermann, P.; Dengler, T.J.; Katus, H.A. Increased adherence eight months after switch from twice daily calcineurin inhibitor based treatment to once daily modified released tacrolimus in heart transplantation. Drug Des. Devel. Ther. 2013, 7, 1253–1258. [Google Scholar] [CrossRef] [PubMed]
- Godinas, L.; Dobbels, F.; Hulst, L.; Verbeeck, I.; De Coninck, I.; Berrevoets, P.; Schaevers, V.; Yserbyt, J.; Dupont, L.J.; Verleden, S.E.; et al. Once daily tacrolimus conversion in lung transplantation: A prospective study on safety and medication adherence. J. Heart Lung Transplant. 2021, 40, 467–477. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Author/Year | Population | Study Design and Number of HTx Participants | Participant Age | Measure of Adherence | Duration and Attrition Rate |
|---|---|---|---|---|---|
| Albert (2012) [23] | 38 patients who received heart transplantation between 1–18 yo and were 16–34 yo at time of participation in Berlin, Germany | Cross sectional, 38 | 16–34 years | Medication Experience Scale for Immunosuppressants (MESI) | N/A, N/A |
| Anton (2019) [11] | 12 patients in Dallas, TX | Retrospective cohort, 12 | 16–22 years | Immunosuppressant drug levels, Medical Condition and Medication Knowledge Questionnaire | 2 years, N/A |
| Devine (2011) [12] | Adolescent patients between 11–20 years old who received solid organ transplants (47 kidney, 20 liver, 14 heart, 1 double lung) and parents in Atlanta, GA | Cohort, 14 | 11–20 years and their parents | The Medication and Clinic Attendance Modules of the Medication Adherence Measure (MAM), Parent and adolescent reports of missing doses or late doses (adherence determined as number of doses taken on time divided by number prescribed), Rescheduled clinic appointments | 18 months, 19% (16/82) |
| Eaton (2018) [13] | 47 patients who received solid organ transplant and their caregivers (47 AYA-caregiver dyads, 94 total participants) in Atlanta, GA | Cross sectional, 13 | 12–19 years | The Medication Adherence Measure (MAM), The Medication Level Variability Index (MLVI) for tacrolimus | N/A, N/A |
| Flippin (2000) [14] | 49 patients in St. Louis, MO | Retrospective cohort, 49 | 0–18 years | Immunosuppressant drug levels | Follow up ranged from 6–138 months, N/A |
| Grady (2019) [15] | 88 patients at six pediatric heart transplant programs in the USA (East, Midwest and West) | Randomized Controlled Trial, 88 | Mean age 21 years with SD 3 years | Immunosuppressant drug levels, The Patient Assessment of Problems with the HT Regimen | 4 months, 11.3% (10/88) |
| Grady (2018) [16] | 88 patients at six pediatric heart transplant programs in the USA (East, Midwest and West) | Cross sectional, 88 | Mean age 21 years with SD 3 years | Immunosuppressant drug levels, The Patient Assessment of Problems with the HT Regimen | N/A, N/A |
| Kerr (2020) [17] | 138 patients > 12 months out from transplant in Seattle, WA | Retrospective cohort, 138 | Mean age 5.6 ± 6.1 years | Immunosuppressant drug levels | Mean 5.5 ± 3.6 years, N/A |
| McCormick (2019) [18] | 30 patients in Ann Arbor, MI | Cross sectional, 30 | Median age 17.5 years (15.6–19.2) | Immunosuppressant drug levels, Patient self-reported adherence during clinic visits by answering “how many missed or late immunosuppression doses have you had in the last week” | N/A, N/A |
| Ringewald (2001) [19] | 50 patients in Chicago, IL | Retrospective cohort, 50 | For the rejection group, age at heart transplant 8.9 ± 6.1 years. For the nonrejection group, age at transplant 6 ± 6.4 years | Immunosuppressant drug levels and voluntary admission of irregular medication administration. Patients were stratified by episodes of late rejection. | N/A, N/A |
| Serrano-Ikkos (1998) [22] | 53 patients who received heart transplant or heart-lung transplant in London, United Kingdom | Prospective cohort, 29 | Mean age 10.2 years, SD 5.0 years | Self-reported adherence, review of patient diaries and cyclosporine levels | Followed for 12 months, N/A |
| Simons (2009) [6] | 82 adolescent solid organ transplant recipients and 68 parent/adolescent dyads in the USA | Cross sectional, 14 | 11–21 years (mean 15.8, SD 2.4 years) | Immunosuppressant drug levels, Medication Module of the Medication Adherence Measure (MAM), Multidimensional Adherence Classification System (MACS) | N/A, 13.4% (11/82) |
| Wolfe (2020) [20] | 27 patients in Aurora, CO | Cross-sectional, 27 | 4–18 years old (mean 9.3, SD 3.7 years) | Immunosuppressant drug levels | N/A, N/A |
| Wray (2006) [21] | 50 patients who had undergone heart or heart-lung transplantation in London, United Kingdom | Cross sectional, 33 | 12.3–24.9 years old (mean 17.87, SD 3.41 years) | Immunosuppressant drug levels | N/A, 20% (10/50) |
| Name | Overview |
|---|---|
| Medication Experience Scale for Immunosuppressants (MESI) [24] |
|
| The Medication Adherence Measure (MAM) [25] |
|
| The Medication Level Variability Index (MLVI) for tacrolimus [26] |
|
| The Patient Assessment of Problems with the Heart Transplant Regimen [27] |
|
| Multidimensional Adherence Classification System (MACS) [6] |
|
| Medical Condition and Medication Knowledge Questionnaire [11] |
|
| Author (Year) | Adherence Measure | Outcomes |
|---|---|---|
| Simons (2009) [6] | Immunosuppressant drug levels (Tacrolimus and Cyclosporine) |
|
| Medication Module of the Medication Adherence Measure (MAM) |
| |
| Multidimensional Adherence Classification System (MACS) |
| |
| Ringewald (2001) [19] | Immunosuppressant drug levels (Tacrolimus and Cyclosporine) and variability (defined as the ratios of non-therapeutic CSA levels over total number of levels analyzed per patient) |
|
| Voluntary admission of irregular medication administration |
| |
| Kerr (2020) [17] | Immunosuppressant drug levels (Tacrolimus and Cyclosporine) |
|
| Flippin (2000) [14] | Cyclosporine levels and variability (defined as the ratios of non-therapeutic CSA levels over total number of levels analyzed per patient). |
|
| Author/Year | Measure of Adherence | Assessments of QOL and Mental Health | Main Outcomes |
|---|---|---|---|
| Albert (2012) [23] | Medication Experience Scale for Immunosuppressants (MESI) | The Short Form Health Survey (SF-36) |
|
| Giessen Subjective Complaints List (GBB) |
| ||
| Health Questionnaire for Children and Young People (KIDSCREEN-27) |
| ||
| Devine (2011) [12] | The Medication and Clinic Attendance Modules of the Medication Adherence Measure (MAM) | The Child Health Questionnaire-Child Form 87 (CHQ-CF87) |
|
| The Child Health Questionnaire-Parent Form 50 (CHQ-PF50) | |||
| Parent and adolescent reports of missing doses or late doses (adherence determined as number of doses taken on time divided by number prescribed) | Family Environment Scale (FES) | ||
| Rescheduled clinic appointments | End-Stage Renal Disease Symptom Checklist-Transplant Module (ESRD-SCL) | ||
| Eaton (2018) [13] | The Medication Adherence Measure (MAM) | The Adolescent Medication Barriers Scale (AMBS) contains three factors: -Disease Frustration/Adolescent Issues (DF) -Regimen Adaptation/Cognitive Issues(RA) -Ingestion Issues (II) |
|
| Parent Medication Barriers Scale (PMBS) Contains four factors: -Disease Frustration/ Adolescent Issues (DF) -Regimen Adaptation/ Cognitive Issues (RA) -Ingestion Issues (II), -Parent Reminder (PR) | |||
| The Behavior Assessment System of Children-2nd Edition Self-Report of Personality, Adolescent Version (BASC-2-SRP-A) | |||
| The Medication Level Variability Index (MLVI) for tacrolimus | The Brief Symptom Inventory-18 (BSI-18) | ||
| McCormick (2019) [18] | Immunosuppression trough levels (a standard deviation of trough levels was calculated) | Generalized anxiety disorder-7 scale (GAD-7) PedsQL 4.0 Generic Core Scales PedsQL 3.0 Cardiac Module Post heart transplant fears questionnaire (PHTF) |
|
| Self-reported adherence during clinic visits | |||
| Serrano-Ikkos (1998) [22] | Self-reported adherence, review of patient diaries | Camberwell Family Interview Schedule (CFI) Semi-structured psychiatric interview of children Patients’ diaries were checked for medication dosage, pulmonary function measurement, and daily completion |
|
| Cyclosporine levels | |||
| Wolfe (2020) [20] | Immunosuppression trough levels (tacrolimus and cyclosporine) | Wechsler Intelligence Scale for Children (WISC) Wechsler Adult Intelligence Scale (WAIS) Wechsler Adult Intelligence Scale (WPPSI) Wechsler Individual Achievement Test (WIAT) California Verbal Learning Test (CVLT) Behavior Rating Inventory of Executive Function (BRIEF) National Institute of Child Health Questionnaire (NICHQ) Adaptive Behavior Assessment System (ABAS) |
|
| Wray (2006) [21] | Immunosuppression levels (tacrolimus and cyclosporine) | Beliefs about Medication Questionnaire (BMQ) Perceived Illness Experience (PIE) |
|
| Author (Year) | Measure of Adherence | Transition Program | Main Outcomes |
|---|---|---|---|
| Anton (2019) [11] | Immunosuppression levels (tacrolimus and cyclosporine) | 2-year structured transition program to improve patients overall medical knowledge, medication adherence, readiness to transition, and parental perceptions of child’s readiness to transition. Consisted of 7 2-hr sessions. |
|
| Medical Condition and Medication Knowledge Questionnaire | |||
| Grady (2018) [16] | Immunosuppression levels | Only discussed baseline data in this paper |
|
| Self-report (Assessment of Problems with the HT Regimen) | |||
| Grady (2019) [15] | Immunosuppression levels | A standardized tailored transition program focused on increasing HT knowledge, self-care and self-advocacy skills and enhancing social support. It was designed to improve outcomes (i.e., adherence to immunosuppression and the medical regimen) for emerging adults who underwent HT as children and transferred to adult care |
|
| Self-report (Assessment of Problems with the HT Regimen) |
| File Name | Representativeness of the Exposed Cohort | Selection of Nonexposed Cohort | Ascertainment of Exposure | Demonstration That Outcome of Interest Was Not Present at the Start of the Study | Comparability | Assessment of Outcome | Length of Follow-Up | Adequacy of Follow-Up | Bias Rating | Bias Reasoning |
|---|---|---|---|---|---|---|---|---|---|---|
| Anton (2019) | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 out of 9 | No controls/adjustment |
| Devine (2011) | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 1 | 8 out of 9 | Self-reported outcomes |
| Flippin (2000) | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 out of 9 | No controls/adjustment |
| Kerr (2020) | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 out of 9 | N/A |
| Ringewald (2001) | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 out of 9 | No controls/adjustment |
| Serrano-Ikkos (1998) | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 out of 9 | No controls/adjustment |
| File Name | Representativeness of the Sample | Sample Size | Non-Respondents | Ascertainment of the Exposure (Risk Factor) | Comparability | Assessment of the Outcome | Statistical Test | Bias Rating | Bias Reasoning |
|---|---|---|---|---|---|---|---|---|---|
| Albert (2012) | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 6 out of 10 | No description of non-respondents, no controls/adjustments done, self-reported outcomes only, p values provided but no confidence intervals |
| Eaton (2018) | 1 | 1 | 1 | 2 | 0 | 2 | 0 | 7 out of 10 | No controls/adjustments done, p values provided but no confidence intervals |
| Grady (2018) | 1 | 1 | 0 | 2 | 0 | 2 | 1 | 7 out of 10 | No description of non-respondents, no controls/adjustments done |
| McCormick (2019) | 1 | 1 | 1 | 2 | 0 | 2 | 1 | 8 out of 10 | No controls/adjustments done |
| Simons (2008) | 1 | 1 | 0 | 2 | 0 | 2 | 0 | 6 out of 10 | No description of non-respondents, no controls/adjustments done, p values not provided |
| Wolfe (2019) | 1 | 1 | 0 | 2 | 1 | 2 | 1 | 8 out of 10 | No description of non-respondents, incomplete controls/adjustments |
| Wray (2006) | 1 | 1 | 1 | 2 | 0 | 2 | 0 | 7 out of 10 | No controls/adjustments done, p values not consistently provided |
| File Name | Randomization Process | Effect of Assignment | Missing Outcome Data | Outcome Measurement | Reported Result | Overall Risk |
|---|---|---|---|---|---|---|
| Grady (2019) | Low risk 1.1: Used computer based block randomization 1:3: No differences between intervention groups | Low risk 2.1, 2.2: Nonblinded to participants and researchers 2.3: No deviations occurred 2.6: Appears that intention-to-treat was done | Low risk 3.1: Nearly all participants completed the study | Some concerns 4.1/4.2: Measurement was appropriate and did not differ between groups 4.3/4.4: Assessors were aware of intervention and allocation 4.5: Seems unlikely outcome was affected by knowledge of intervention | Low risk 5.1/5.2/5.3: One pre-specified analysis of the data | Low risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nassetta, K.; Hussain, T.; Gambetta, K.; Le, K.; O’Dwyer, L.C.; Badawy, S.M. A Systematic Review of Adherence to Immunosuppression among Pediatric Heart Transplant Patients. J. Cardiovasc. Dev. Dis. 2022, 9, 165. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050165
Nassetta K, Hussain T, Gambetta K, Le K, O’Dwyer LC, Badawy SM. A Systematic Review of Adherence to Immunosuppression among Pediatric Heart Transplant Patients. Journal of Cardiovascular Development and Disease. 2022; 9(5):165. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050165
Chicago/Turabian StyleNassetta, Keira, Tasmeen Hussain, Katheryn Gambetta, Kevin Le, Linda C. O’Dwyer, and Sherif M. Badawy. 2022. "A Systematic Review of Adherence to Immunosuppression among Pediatric Heart Transplant Patients" Journal of Cardiovascular Development and Disease 9, no. 5: 165. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9050165