
Structured Allocation of Transcatheter Aortic Valve Replacement Patients during Coronavirus Disease 2019 Pandemic: Impact on Patient Selection and Clinical Results

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Preprocedural Period
2.3. Procedure
2.4. Postprocedural Period
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Preprocedural Echocardiography and Computed Tomography
3.3. Procedure
3.4. Postprocedural Data and In-Hospital Follow-Up

4. Discussion
- The implementation of our allocation prioritized sicker patients for TAVR during the pandemic;
- The TAVR procedure showed similar success, despite the higher complexity in the COVID-19 group;
- TAVR during COVID-19 could be performed with a shorter in-hospital stay and similar in-hospital safety results.
4.1. Patient Prioritization through Our Allocation Algorithm
4.2. Higher Complexity of TAVR Procedures during COVID-19
4.3. Safe and Effective TAVR Treatment during COVID-19 with a Shorter In-Hospital Stay and Similar In-Hospital Results
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Guyton, R.A.; O’Gara, P.T.; Ruiz, C.E.; Skubas, N.J.; Sorajja, P.; et al. 2014 AHA/ACC Guideline for the Management of Patients with Valvular Heart Disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 129, 2440–2492. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Thorac. Cardiovasc. Surg. 2021, 162, e183–e353. [Google Scholar] [CrossRef] [PubMed]
- Kanwar, A.; Thaden, J.J.; Nkomo, V.T. Management of Patients with Aortic Valve Stenosis. Mayo Clin. Proc. 2018, 93, 488–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapadia, S.R.; Leon, M.B.; Makkar, R.R.; Tuzcu, E.M.; Svensson, L.G.; Kodali, S.; Webb, J.G.; Mack, M.J.; Douglas, P.S.; Thourani, V.H.; et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): A randomised controlled trial. Lancet 2015, 385, 2485–2491. [Google Scholar] [CrossRef]
- Leon, M.B.; Smith, C.R.; Mack, M.; Miller, D.C.; Moses, J.W.; Svensson, L.G.; Tuzcu, E.M.; Webb, J.G.; Fontana, G.P.; Makkar, R.R.; et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N. Engl. J. Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef] [Green Version]
- Braghiroli, J.; Kapoor, K.; Thielhelm, T.P.; Ferreira, T.; Cohen, M.G. Transcatheter aortic valve replacement in low risk patients: A review of PARTNER 3 and Evolut low risk trials. Cardiovasc. Diagn. Ther. 2020, 10, 59–71. [Google Scholar] [CrossRef]
- Shreenivas, S.; Choo, J.; Answini, G.; Sarembock, I.J.; Griffin, J.; Smith, J.M.; Kereiakes, D. TAVR During the COVID-19 Pandemic: The ACC/SCAI Consensus Statement. JACC Cardiovasc. Interv. 2020, 13, 1605–1606. [Google Scholar] [CrossRef]
- Cardiology, T.E.S.F. ESC Guidance for the Diagnosis and Management of CV Disease during the COVID-19 Pandemic. 2020. Available online: https://www.escardio.org/Education/COVID-19-and-Cardiology/ESC-COVID-19-Guidance (accessed on 12 July 2020).
- Valdebenito, M.; Massalha, E.; Barbash, I.M.; Maor, E.; Fefer, P.; Guetta, V.; Segev, A. Transcatheter Aortic Valve Implantation During the COVID-19 Pandemic. Am. J. Cardiol. 2021, 145, 97–101. [Google Scholar] [CrossRef]
- Rooijakkers, M.J.P.; Li, W.W.; Wollersheim, L.W.; Geuzebroek, G.S.; Gehlmann, H.; van Garsse, L.A.; van Wely, M.H.; Verkroost, M.W.; Morshuis, W.J.; Wertheim, H.; et al. Transcatheter aortic valve replacement during the COVID-19 pandemic-A Dutch single-center analysis. J. Card. Surg. 2021, 36, 48–55. [Google Scholar] [CrossRef]
- Perek, B.; Olasinska-Wisniewska, A.; Misterski, M.; Puslecki, M.; Grygier, M.; Buczkowski, P.; Lesiak, M.; Stankowski, T.; Szarpak, L.; Ruetzler, K.; et al. How the COVID-19 pandemic changed treatment of severe aortic stenosis: A single cardiac center experience. J. Thorac. Dis. 2021, 13, 906–917. [Google Scholar] [CrossRef]
- Khialani, B.; MacCarthy, P. Transcatheter management of severe aortic stenosis during the COVID-19 pandemic. Heart 2020, 106, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Harky, A.; Seyedzenouzi, G.; Sanghavi, R.; Premkumar, G.; Badran, A. COVID-19 and its implications on patient selection for TAVI and SAVR: Are we heading into a new era? J. Card. Surg. 2021, 36, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.B.; Welt, F.G.P.; Mahmud, E.; Phillips, A.; Kleiman, N.S.; Young, M.N.; Sherwood, M.; Batchelor, W.; Wang, D.D.; Davidson, L.; et al. Triage considerations for patients referred for structural heart disease intervention during the COVID-19 pandemic: An ACC/SCAI position statement. Catheter. Cardiovasc. Interv. 2020, 96, 659–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landes, U.; Orvin, K.; Codner, P.; Assali, A.; Vaknin-Assa, H.; Schwartznberg, S.; Levi, A.; Shapira, Y.; Sagie, A.; Kornowski, R. Urgent Transcatheter Aortic Valve Implantation in Patients with Severe Aortic Stenosis and Acute Heart Failure: Procedural and 30-Day Outcomes. Can J. Cardiol. 2016, 32, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Kovach, C.P.; Bell, S.; Reisman, M.; Aldea, G.; McCabe, J.M.; Dvir, D.; Don, C. Outcomes of Emergency Transcatheter Aortic Valve Replacement. J. Interv. Cardiol. 2019, 2019, 7598581. [Google Scholar] [CrossRef] [PubMed]
- Frerker, C.; Schewel, J.; Schlüter, M.; Schewel, D.; Ramadan, H.; Schmidt, T.; Thielsen, T.; Kreidel, F.; Schlingloff, F.; Bader, R.; et al. Emergency transcatheter aortic valve replacement in patients with cardiogenic shock due to acutely decompensated aortic stenosis. EuroIntervention 2016, 11, 1530–1536. [Google Scholar] [CrossRef]
- Kolte, D.; Khera, S.; Vemulapalli, S.; Dai, D.D.; Heo, S.; Goldsweig, A.M.; Aronow, H.D.; Inglessis, I.; Elmariah, S.; Sharaf, B.; et al. Outcomes Following Urgent/Emergent Transcatheter Aortic Valve Replacement: Insights From the STS/ACC TVT Registry. JACC Cardiovasc. Interv. 2018, 11, 1175–1185. [Google Scholar] [CrossRef]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; Van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document (VARC-2). Eur. J. Cardiothorac. Surg. 2012, 42, S45–S60. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2018, 40, 237–269. [Google Scholar] [CrossRef] [Green Version]
- Nashef, S.A.; Roques, F.; Michel, P.; Gauducheau, E.; Lemeshow, S.; Salamon, R. European system for cardiac operative risk evaluation (EuroSCORE). Eur. J. Cardiothorac. Surg. 1999, 16, 9–13. [Google Scholar] [CrossRef]
- Joseph, J.; Kotronias, R.A.; Estrin-Serlui, T.; Cahill, T.J.; Kharbanda, R.K.; Newton, J.D.; Grebenik, C.; Dawkins, S.; Banning, A.P. Safety and operational efficiency of restructuring and redeploying a transcatheter aortic valve replacement service during the COVID-19 pandemic: The Oxford experience. Cardiovasc. Revasc. Med. 2020, 31, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Alperi, A.; Muntané-Carol, G.; Freitas-Ferraz, A.B.; Junquera, L.; del Val, D.; Faroux, L.; Philippon, F.; Rodés-Cabau, J. Overcoming the transcatheter aortic valve replacement Achilles heel: Conduction abnormalities—A systematic review. Ann. Cardiothorac. Surg. 2020, 9, 429–441. [Google Scholar] [CrossRef] [PubMed]
- Mentias, A.; Jneid, H. Transcatheter Aortic Valve Replacement in the Coronavirus Disease 2019 (COVID-19) Era. J. Am. Heart Assoc. 2020, 9, e017121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| 1. Emergency/Urgent | 2. Urgent but Stable | 3. Elective |
|---|---|---|
|
|
|
|
|
|
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| Body Mass Index (BMI) (kg/m2 +/− SD) | 26.5 (+/−5) | 26.8 (+/−4.9) | 0.499 |
| female | 222 (48.7%) | 196 (43.2%) | 0.095 |
| age (years +/− SD) | 80.8 (+/−6.8) | 81.2 (+/−5.8) | 0.367 |
| EuroSCORE (+/− SD) | 10.7 (+/−2.4) | 10.8 (+/−2.3) | 0.665 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| arterial hypertension | 409 (89.7%) | 376 (87.9%) | 0.385 |
| chronic obstructive pulmonary disease (COPD) | 114 (25%) | 126 (29.4%) | 0.138 |
| cerebrovascular disease | 66 (14.5%) | 80 (18.7%) | 0.091 |
| peripheral artery disease | 115 (25.2%) | 87 (20.3%) | <0.001 |
| diabetes mellitus | 125 (27.4%) | 134 (31.3%) | 0.203 |
| frailty | 67 (14.7%) | 48 (11.2%) | 0.124 |
| porcelain aorta | 34 (7.5%) | 21 (4.9%) | 0.117 |
| previous cerebrovascular accident (stroke)/transient ischemic attack (TIA) | 59 (12.9%) | 59 (13.8%) | 0.701 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| coronary heart disease | 336 (73.7%) | 349 (76.5%) | 0.357 |
| previous percutaneous coronary intervention (PCI) | 175 (38.4%) | 178 (41.6%) | 0.330 |
| previous pacemaker/implantable cardioverter defibrillator (ICD) implantation | 65 (14.3%) | 59 (13.8%) | 0.84 |
| New York Heart Association (NYHA) classification Score II, III and IV | 443 (97.1%) | 418 (97.7%) | 0.631 |
| Canadian Cardiovascular Society (CCS) classification Score II, III and IV | 54 (11.8%) | 80 (18.7%) | 0.004 |
| left bundle branch block (LBBB) | 22 (4.8%) | 44 (10.9%) | 0.001 |
| right bundle branch block (RBBB) | 24 (5.3%) | 36 (8.9%) | 0.036 |
| previous cardiac decompensation (in last 12 months) | 66 (14.5%) | 105 (24.5%) | <0.001 |
| cardiogenic shock/cardiac decompensation | 6 (1.3%) | 45 (10.5%) | <0.001 |
| cardiopulmonary resuscitation | 5 (1.1%) | 7 (1.6%) | 0.489 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
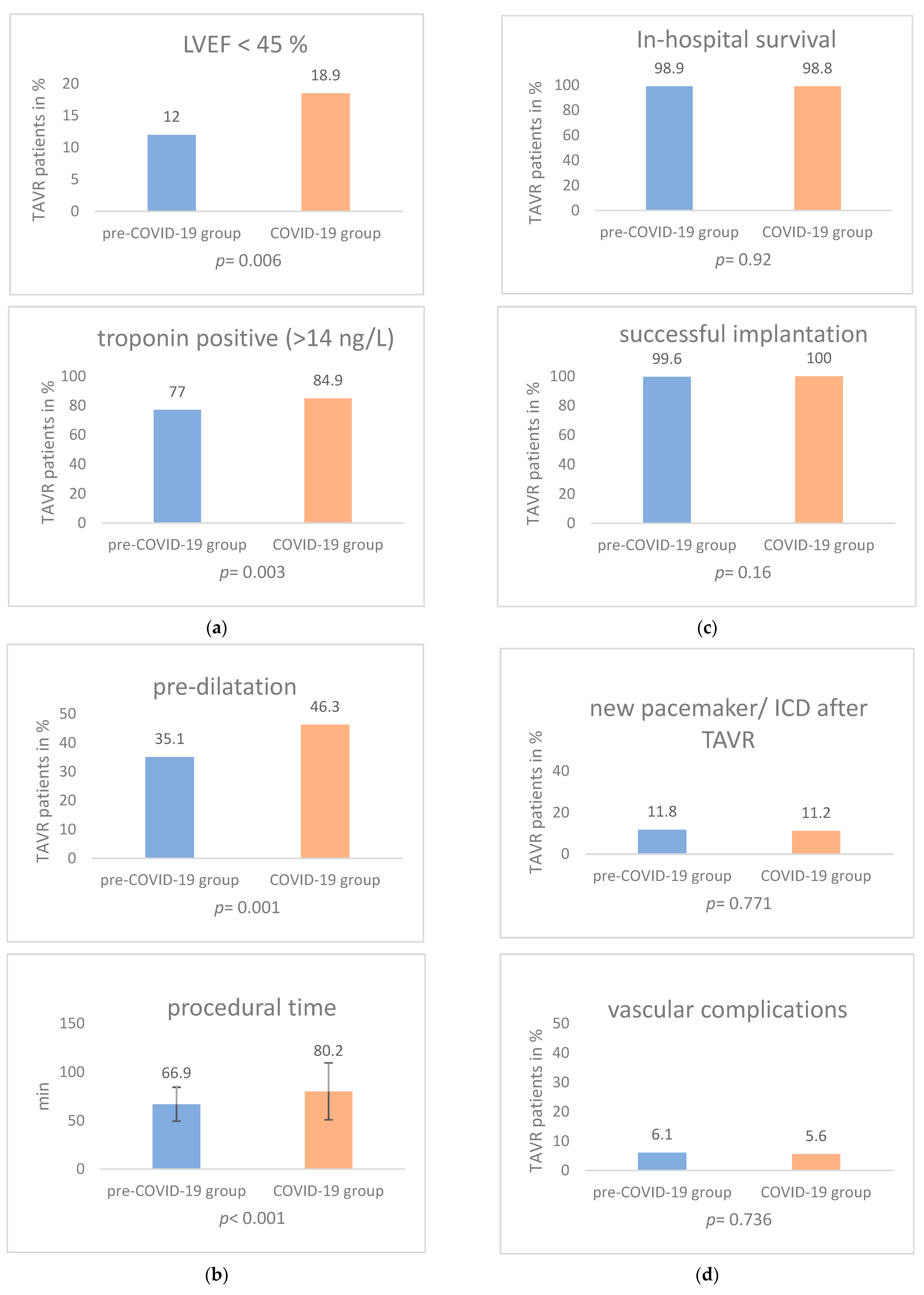
| troponin positive (>14 ng/L) | 351 (77%) | 355 (84.9%) | 0.003 |
| glomerular filtration rate (GFR) (mL/min +/− SD) | 57.2 (+/−21.3) | 58.8 (+/−20.9) | 0.356 |
| hemoglobin (g/dl +/− SD) | 12.3 (+/−1.7) | 12.4 (+/−1.7) | 0.144 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| maximum pressure gradient across the aortic valve (AV maxPG) (mmHg +/− SD) | 62.2 (+/−24.8) | 64.6 (+/−23.3) | 0.152 |
| mean pressure gradient across the aortic valve (AV meanPG) (mmHg +/− SD) | 38.1 (+/−16.4) | 39.4 (+/−15.4) | 0.227 |
| LVEF below 45% | 53 (12%) | 78 (18.9%) | 0.006 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| femoral access site | 447 (98%) | 446 (98.5%) | 0.623 |
| valve in valve | 19 (4.2%) | 9 (2.1%) | 0.080 |
| Valve type | |||
| - Medtronic Evolut | 361 (79.2%) | 310 (72.6%) | 0.022 |
| - Edwards Sapien | 83 (18.2%) | 94 (22%) | 0.157 |
| - Boston Acurate Neo | 12 (2.6%) | 23 (5.4%) | 0.036 |
| predilatation | 160 (35.1%) | 198 (46.3%) | 0.001 |
| fluoroscopy time (min +/− SD) | 18.21 (+/−8.1) | 18.7 (+/−8.9) | 0.391 |
| cumulative dose (cGy*cm2 +/− SD) | 3995.9 (+/−3582.4) | 4275.7 (+/−3781.2) | 0.261 |
| amount of radioactive contrast medium (mL +/− SD) | 83.6 (+/−38.9) | 87.5 (+/−41.6) | 0.155 |
| procedural time (min +/− SD) | 66.9 (+/−17.5) | 80.2 (+/−29.4) | <0.001 |
| postdilatation | 57 (12.5%) | 58 (13.6%) | 0.642 |
| paravalvular leak | |||
| -no | 293 (64.2%) | 270 (64.4%) | 0.955 |
| -mild | 159 (34.9%) | 147 (35.1%) | 0.947 |
| -moderate | 4 (0.9%) | 2 (0.5%) | 0.474 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| conversion to open surgery | 2 (0.4%) | 0 (0%) | 0.170 |
| cardiopulmonary resuscitation | 3 (0.7%) | 3 (0.7%) | 0.938 |
| mechanical circulatory support | 2 (0.4%) | 1 (0.2%) | 0.6 |
| aortic dissection | 0 (0%) | 0 (0%) | |
| cardiac tamponade | 1 (0.2%) | 1 (0.2%) | 0.964 |
| vascular complications | 28 (6.1%) | 24 (5.6%) | 0.736 |
| ventricular perforation | 0 (0.0%) | 1 (0.2%) | 0.302 |
| major bleeding | 4 (0.9%) | 3 (0.7%) | 0.768 |
| life-threatening/disabling bleeding | 6 (0.2%) | 2 (0.5%) | 0.183 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| in-hospital stay (day +/− SD) | 9.5 (+/−9.33) | 8.4 (+/−5.9) | 0.041 |
| TAVR patients per month | 46.11 (+/−7.57) | 39 (+/−4.55) | 0.03 |
| sepsis | 3 (0.7%) | 1 (0.2%) | 0.348 |
| endocarditis | 0 (0%) | 2 (0.5%) | 0.144 |
| myocardial infarction type 1 [20] | 0 (0%) | 0 (0%) | |
| acute kidney injury | 53 (11.6%) | 60 (14.1%) | 0.28 |
| maximum pressure gradient across the aortic valve (AV maxPG) (mmHg +/− SD) | 15.4 (+/−8.5) | 15.4 (+/−8.3) | 0.958 |
| mean pressure gradient across the aortic valve (AV meanPG) (mmHg +/− SD) | 8.2 (+/−4.5) | 8.5 (+/−4.5) | 0.386 |
| left ventricular ejection fraction (LVEF) below 45% | 31 (7.8%) | 52 (13.1%) | 0.014 |
| Pre-COVID-19 (n = 456) | COVID-19 (n = 456) | p-Value | |
|---|---|---|---|
| 30-day mortality | 5 (1.1%) | 5 (1.2%) | 0.92 |
| transient ischemic attack (TIA) (<30 d) | 4 (0.9%) | 6 (1.4%) | 0.461 |
| stroke (<30 d) | 9 (2%) | 12 (2.8%) | 0.418 |
| new left bundle branch block (LBBB) | 34 (7.5%) | 61 (14.3%) | 0.001 |
| new pacemaker/implantable cardioverter defibrillator (ICD) implantation | 54 (11.8%) | 48 (11.2%) | 0.771 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berisha, N.; Klein, K.; Veulemans, V.; Maier, O.; Piayda, K.; Binnebößel, S.; Afzal, S.; Polzin, A.; Westenfeld, R.; Horn, P.; et al. Structured Allocation of Transcatheter Aortic Valve Replacement Patients during Coronavirus Disease 2019 Pandemic: Impact on Patient Selection and Clinical Results. J. Cardiovasc. Dev. Dis. 2022, 9, 189. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060189
Berisha N, Klein K, Veulemans V, Maier O, Piayda K, Binnebößel S, Afzal S, Polzin A, Westenfeld R, Horn P, et al. Structured Allocation of Transcatheter Aortic Valve Replacement Patients during Coronavirus Disease 2019 Pandemic: Impact on Patient Selection and Clinical Results. Journal of Cardiovascular Development and Disease. 2022; 9(6):189. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060189
Chicago/Turabian StyleBerisha, Nora, Kathrin Klein, Verena Veulemans, Oliver Maier, Kerstin Piayda, Stephan Binnebößel, Shazia Afzal, Amin Polzin, Ralf Westenfeld, Patrick Horn, and et al. 2022. "Structured Allocation of Transcatheter Aortic Valve Replacement Patients during Coronavirus Disease 2019 Pandemic: Impact on Patient Selection and Clinical Results" Journal of Cardiovascular Development and Disease 9, no. 6: 189. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060189