
Influence of Discontinuation of Cardiac Rehabilitation in Elderly Outpatients Due to the COVID-19 Pandemic

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. CR Program
2.3. Patient Characteristics before Restart CR
2.4. Body Composition
2.5. Staging of Locomotive Syndrome
2.6. One-Leg Standing Time with Eyes Open Test
2.7. FFQ
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics before Discontinuation
3.2. Changes in the FFQ Findings at Restart of CR and after 3 Months
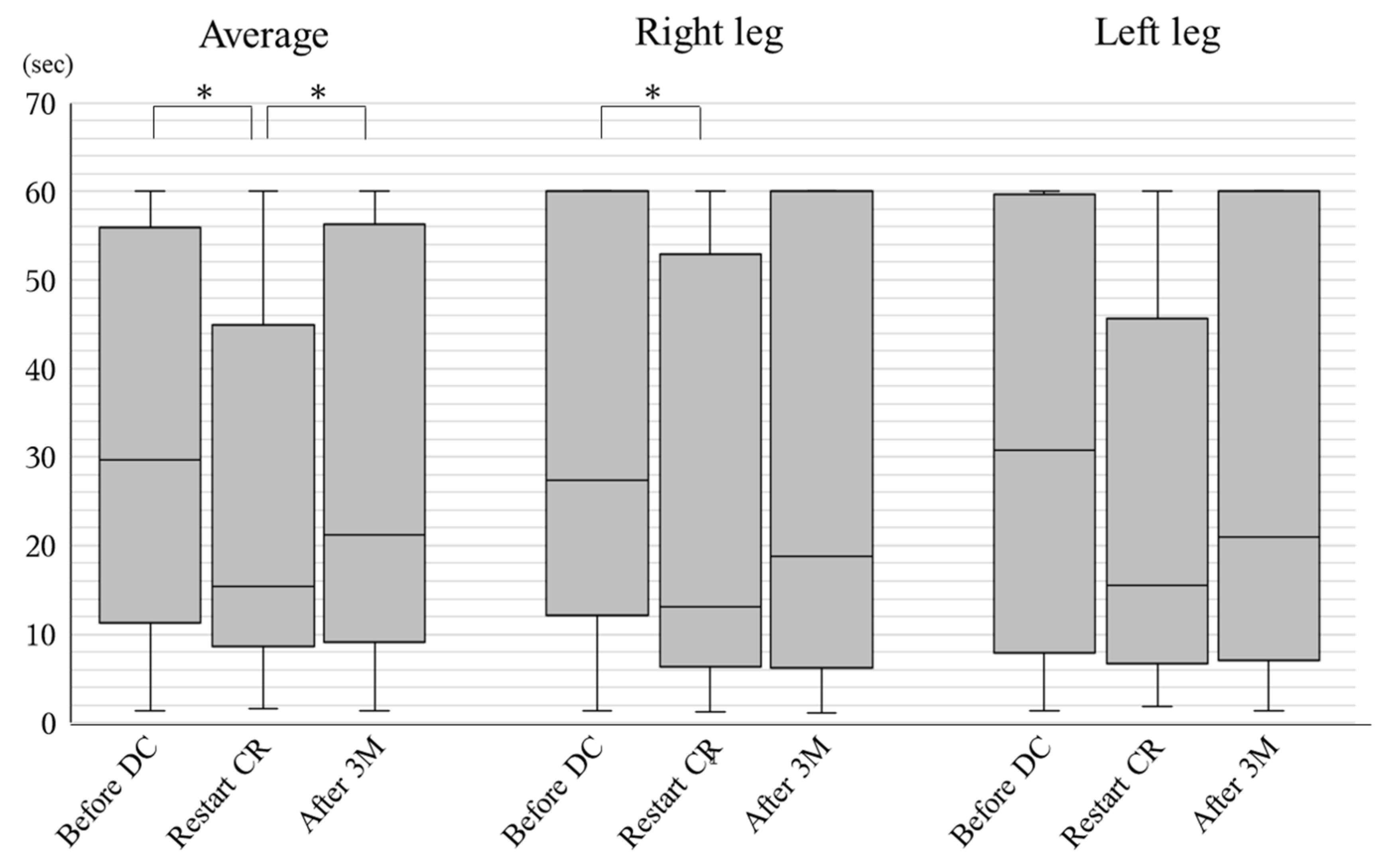
3.3. Changes in Physical Activity at Restart of CR and after 3 Months
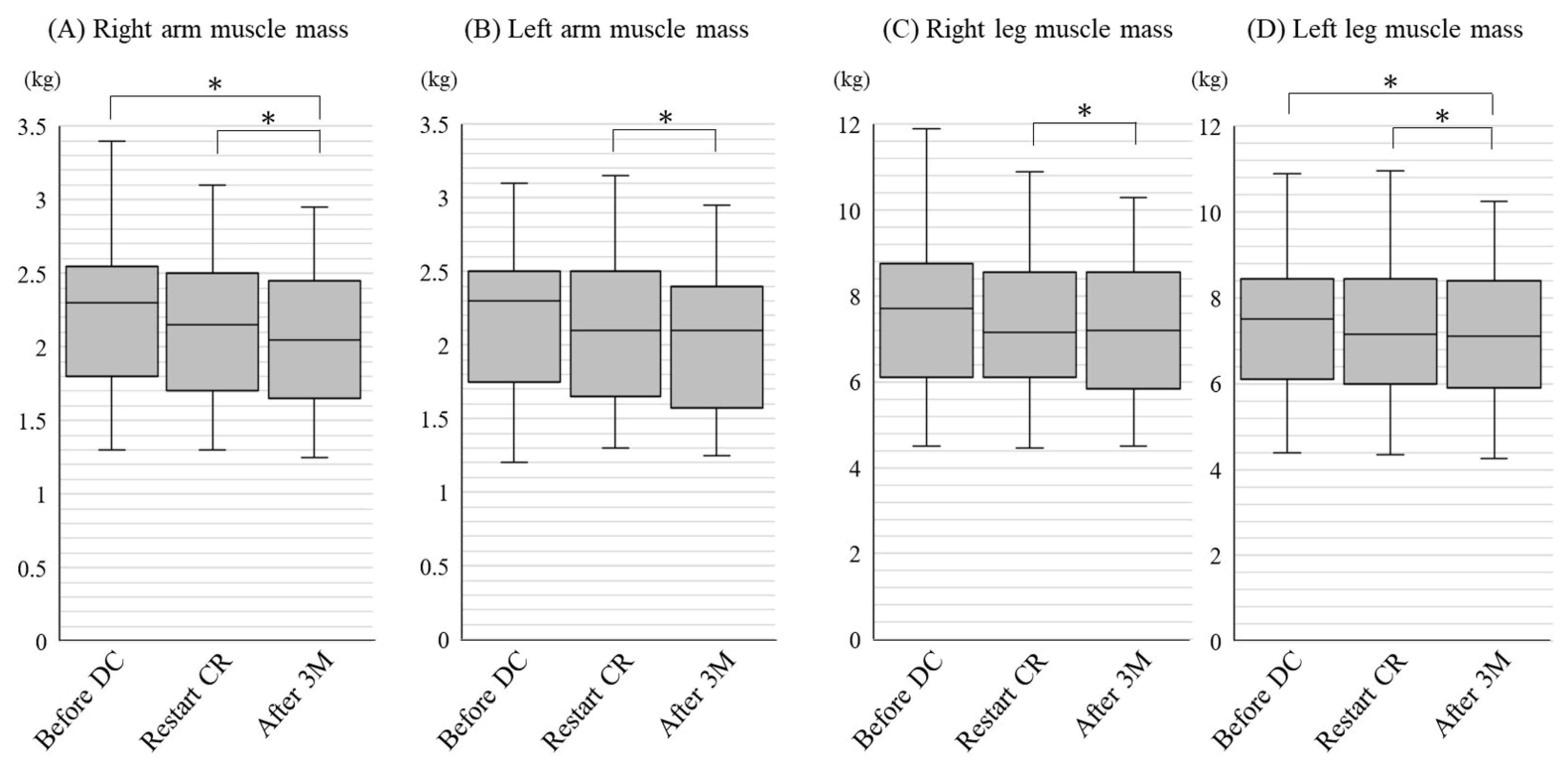
3.4. Change in Body Composition at Restart of CR and after 3 Months
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Clemente-Suárez, V.J.; Beltrán-Velasco, A.I.; Ramos-Campo, D.J.; Mielgo-Ayuso, J.; Nikolaidis, P.A.; Belando, N.; Tornero-Aguilera, J.F. Physical activity and COVID-19. The basis for an efficient intervention in times of COVID-19 pandemic. Physiol. Behav. 2022, 244, 113667. [Google Scholar] [CrossRef]
- Dibben, G.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.D.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2021, 11, CD001800. [Google Scholar]
- Acton, R.B.; Vanderlee, L.; Cameron, A.J.; Goodman, S.; Jáuregui, A.; Sacks, G.; White, C.M.; White, M.; Hammond, D. Self-reported impacts of the COVID-19 pandemic on diet-related behaviours and food security in five countries: Results from the International Food Policy Study 2020. J. Nutr. 2022, 152, 35S–46S. [Google Scholar] [CrossRef]
- Ishibashi, H. Locomotive syndrome in Japan. Osteoporos. Sarcopenia 2018, 4, 86–94. [Google Scholar] [CrossRef]
- Nakamura, K.; Ogata, T. Locomotive Syndrome: Definition and Management. Clin. Rev. Bone Miner. Metab. 2016, 14, 56–67. [Google Scholar] [CrossRef] [Green Version]
- Eto, M.; Miyauchi, S. Relationship between occlusal force and falls among community-dwelling elderly in Japan: A cross-sectional correlative study. BMC Geriatr. 2018, 18, 111. [Google Scholar] [CrossRef]
- JCS/JACR 2021 Guideline on Rehabilitation in Patients with Cardiovascular Disease. Available online: https://www.j-circ.or.jp/cms/wp-content/uploads/2021/03/JCS2021_Makita.pdf (accessed on 31 March 2022).
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 Epidemic on Physical Activity in Community-Dwelling Older Adults in Japan: A Cross-Sectional Online Survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. The Influence of the COVID-19 Pandemic on Physical Activity and New Incidence of Frailty among Initially Non-Frail Older Adults in Japan: A Follow-Up Online Survey. J. Nutr. Health Aging 2021, 25, 751–756. [Google Scholar] [CrossRef]
- Buckingham, S.A.; Taylor, R.S.; Jolly, K.; Zawada, A.; Dean, S.; Cowie, A.; Norton, R.J.; Dalal, H.M. Home-based versus centre-based cardiac rehabilitation: Abridged Cochrane systematic review and meta-analysis. Open Heart 2016, 3, e000463. [Google Scholar] [CrossRef] [Green Version]
- Snoek, J.A.; Prescott, E.I.; van der Velde, A.E.; Eijsvogels, T.M.; Mikkelsen, N.; Prins, L.F.; Bruins, W.; Meindersma, E.; Gonzalez-Juanatey, J.R.; Pena-Gil, C.; et al. Effectiveness of Home-Based Mobile Guided Cardiac Rehabilitation as Alternative Strategy for Nonparticipation in Clinic-Based Cardiac Rehabilitation Among Elderly Patients in Europe: A Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 463–468. [Google Scholar] [CrossRef]
- Li, J.; Liu, B.; Wang, Z.; El-Ansary, D.; Adams, R.; Han, J.; Meng, S. Efficacy of a 6-Week Home-Based Online Supervised Exercise Program Conducted During COVID-19 in Patients with Post Percutaneous Coronary Intervention: A Single-Blind Randomized Controlled Trial. Front. Cardiovasc. Med. 2022, 9, 853376. [Google Scholar] [CrossRef]
- Mukaino, M.; Tatemoto, T.; Kumazawa, N.; Tanabe, S.; Katoh, M.; Saitoh, E.; Otaka, Y. An Affordable, User-friendly Telerehabilitation System Assembled Using Existing Technologies for Individuals Isolated With COVID-19: Development and Feasibility Study. JMIR Rehabil. Assist. Technol. 2020, 7, e24960. [Google Scholar] [CrossRef]
- Nishitani, M.; Shimada, K.; Masaki, M.; Sunayama, S.; Kume, A.; Fukao, K.; Sai, E.; Onishi, T.; Shioya, M.; Sato, H.; et al. Effect of cardiac rehabilitation on muscle mass, muscle strength, and exercise tolerance in diabetic patients after coronary artery bypass grafting. J. Cardiol. 2013, 61, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Omura, T.; Araki, A. Skeletal muscle as a treatment target for older adults with diabetes mellitus: The importance of a multimodal intervention based on functional category. Geriatr. Gerontol. Int. 2022, 22, 110–120. [Google Scholar] [CrossRef]
- Calatayud, J.; Borreani, S.; Moya, D.; Colado, J.C.; Triplett, N.T. Exercise to Improve Bone Mineral Density. Strength Cond. J. 2013, 35, 70–74. [Google Scholar] [CrossRef]
- Michikawa, T.; Nishiwaki, Y.; Takebayashi, T.; Toyama, Y. One-leg standing test for elderly populations. J. Orthop. Sci. 2009, 14, 675–685. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M. Motor Control: Theory and Practical Applications, 2nd ed.; Lippincott, Williams and Wilkens: Baltimore, MD, USA, 2000. [Google Scholar]
- Ivanenko, Y.; Gurfinkel, V.S. Human Postural Control. Front. Neurosci. 2018, 12, 171. [Google Scholar] [CrossRef]
- Bijlsma, A.Y.; Pasma, J.; Lambers, D.; Stijntjes, M.; Blauw, G.J.; Meskers, C.G.; Maier, A. Muscle strength rather than muscle mass is associated with standing balance in elderly outpatients. J. Am. Med. Dir. Assoc. 2013, 14, 493–498. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Jeyakumar, D.T.; Jayawardena, R.; Chourdakis, M. The impact of COVID-19 lockdown on snacking habits, fast-food and alcohol consumption: A systematic review of the evidence. Clin. Nutr. 2021; in press. [Google Scholar] [CrossRef]
- Cosgrove, K.; Wharton, C. Predictors of COVID-19-Related Perceived Improvements in Dietary Health: Results from a US Cross-Sectional Study. Nutrients 2021, 13, 2097. [Google Scholar] [CrossRef]
- Visser, M.; Schaap, L.A.; Wijnhoven, H.A.H. Self-Reported Impact of the COVID-19 Pandemic on Nutrition and Physical Activity Behaviour in Dutch Older Adults Living Independently. Nutrients 2020, 12, 3708. [Google Scholar] [CrossRef]
- Otaki, N.; Yano, M.; Yokoro, M.; Tanino, N.; Fukuo, K. Relationship Between Dietary Variety and Frailty in Older Japanese Women During the Period of Restriction on Outings Due to COVID-19. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e256–e262. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Martinez-Ferran, M.; de la Guía-Galipienso, F.; Sanchis-Gomar, F.; Pareja-Galeano, H. Metabolic Impacts of Confinement during the COVID-19 Pandemic Due to Modified Diet and Physical Activity Habits. Nutrients 2020, 12, 1549. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n = 78 |
|---|---|
| Age, years | 74.1 ± 8.5 |
| Male, n (%) | 49 (62.8) |
| Smoking, n (%) | 6 (9.1) |
| Hypertension, n (%) | 67 (85.9) |
| Diabetes mellitus, n (%) | 37 (47.4) |
| Dyslipidemia, n (%) | 66 (84.6) |
| Chronic kidney disease, n (%) | 46 (59.0) |
| COPD, n (%) | 2 (2.6) |
| Ischemic heart disease, n (%) | 45 (57.7) |
| Heart failure, n (%) | 40 (51.3) |
| Cardiomyopathy, n (%) | 8 (10.3) |
| Macrovascular disease, n (%) | 12 (15.4) |
| Peripheral artery disease, n (%) | 8 (10.3) |
| BNP, pg/mL | 79.7 (49–198) |
| LVEF, % | 60.9 ± 12.5 |
| Before DC | Restart CR | After 3 Months | p Value | p Value | p Value | |
|---|---|---|---|---|---|---|
| n = 10 | n = 74 | n = 63 | Before DC vs. Restart CR | Restart CR vs. after 3 months | Before DC vs. after 3 months | |
| Total calorie intake, kcal | 1775 ± 323 | 1769 ± 436 | 1735 ± 362 | 0.49 | 0.11 | 0.11 |
| Protein calorie, % | 14.7 ± 2.6 | 14.4 (13.3–15.9) | 14.6 (13.2–15.7) | 0.26 | 0.99 | 0.24 |
| Fat calorie, % | 28.6 ± 5.5 | 29.8 ± 5.1 | 30.6 ± 4.5 | 0.48 | 0.29 | 0.85 |
| Carbohydrate calorie, % | 56.7 ± 7.0 | 55.7 ± 5.9 | 54.8 ± 5.4 | 0.99 | 0.37 | 0.76 |
| Salt intake, g | 8.77 ± 3.0 | 9.35 (7.0–12.0) | 9.3 (7.1–11.4) | 0.83 | 0.53 | 0.70 |
| Calorie expenditure, kcal | 2095 ± 489 | 2225 ± 564 | 2049 (1813–2541) | 0.59 | 0.36 | 0.55 |
| due to exercise, kcal | 0 (0–138) | 39 (0–92) | 55 (0–150) | 0.95 | 0.14 | 0.69 |
| due to active living activities, kcal | 315 ± 248 | 343 (155–728) | 380 (192–606) | 0.32 | 0.67 | 0.35 |
| due to normal living activities, kcal | 225 ± 97 | 284 (210–428) | 293 ± 117 | 0.28 | 0.08 | 0.50 |
| due to rest living activities, kcal | 1441 ± 180 | 1340 ± 183 | 1341 ± 183 | 0.16 | 0.55 | 0.58 |
| Before DC | Restart CR | After 3 Months | p Value | p Value | p Value | |
|---|---|---|---|---|---|---|
| n = 41 | n = 67 | n = 61 | Before DC vs. Restart CR | Restart CR vs. After 3 months | Before DC vs. After 3 months | |
| Body weight, kg | 63.0 (54.3–67.5) | 60.7 ± 10.8 | 60.2 ± 10.6 | 0.94 | 0.49 | 0.87 |
| Body mass index, kg/m2 | 23.4 (22.3–25.9) | 23.6 (21.9–25.6) | 23.5 (21.9–25.0) | 0.71 | 0.84 | 0.61 |
| Body fat mass, kg | 16.6 ± 6.4 | 15.8 (13.3–20.1) | 15.7 (13.3–18.5) | 0.63 | 0.24 | 0.25 |
| Percent body fat, % | 26.6 ± 7.6 | 26.9 ± 8.3 | 27.2 (23.2–31.1) | 0.74 | 0.13 | 0.16 |
| Body muscle mass, kg | 44.5 (37.0–48.6) | 41.7 ± 7.2 | 41.6 ± 7.2 | 0.41 | 0.25 | 0.20 |
| Estimated bone mass, kg | 2.50 (2.20–2.70) | 2.35 (2.15–2.65) | 2.35 (2.10–2.60) | <0.001 | 0.17 | 0.009 |
| Basal metabolic rate, kcal | 1240 ± 200 | 1215 ± 187 | 1208 ± 187 | 0.84 | 0.10 | 0.32 |
| Trunk muscle mass, kg | 24.5 (19.8–26.5) | 23.2 (19.9–25.7) | 23.5 (20.4–26.3) | 0.65 | 0.60 | 0.94 |
| Trunk fat mass, kg | 9.83 ± 3.97 | 9.30 (7.85–11.8) | 9.85 (7.90–11.30) | 0.63 | 0.06 | 0.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mouri, N.; Suematsu, Y.; Yano, Y.; Morita, K.; Shirosaki, M.; Fujita, M.; Matsuda, T.; Matsuo, S.; Tazawa, R.; Fujimi, K.; et al. Influence of Discontinuation of Cardiac Rehabilitation in Elderly Outpatients Due to the COVID-19 Pandemic. J. Cardiovasc. Dev. Dis. 2022, 9, 194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060194
Mouri N, Suematsu Y, Yano Y, Morita K, Shirosaki M, Fujita M, Matsuda T, Matsuo S, Tazawa R, Fujimi K, et al. Influence of Discontinuation of Cardiac Rehabilitation in Elderly Outpatients Due to the COVID-19 Pandemic. Journal of Cardiovascular Development and Disease. 2022; 9(6):194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060194
Chicago/Turabian StyleMouri, Noriyuki, Yasunori Suematsu, Yuiko Yano, Kai Morita, Miki Shirosaki, Masaomi Fujita, Takuro Matsuda, Sakiko Matsuo, Rie Tazawa, Kanta Fujimi, and et al. 2022. "Influence of Discontinuation of Cardiac Rehabilitation in Elderly Outpatients Due to the COVID-19 Pandemic" Journal of Cardiovascular Development and Disease 9, no. 6: 194. https://0-doi-org.brum.beds.ac.uk/10.3390/jcdd9060194