MixInYeast: A Multicenter Study on Mixed Yeast Infections

 , , , , , , ,
, , , , , , ,  , , , ,
, , , ,  , , , ,
, , , ,  , , , ,
, , , ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Molecular Identification
2.4. Antifungal Susceptibility
2.5. FKS Amplification and Sequencing
2.6. Data Analysis
3. Results
3.1. Study Population and Clinical Characteristics
3.2. Species Distribution and MY Combinations
3.3. Antifungal Susceptibility Testing
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lamoth, F.; Lockhart, S.R.; Berkow, E.L.; Calandra, T. Changes in the epidemiological landscape of invasive candidiasis. J. Antimicrob. Chemother. 2018, 73, i4–i13. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C. Epidemiology of invasive candidiasis. Curr. Opin. Crit. Care 2010, 16, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Lionakis, M.S.; Arendrup, M.C.; Ostrosky-Zeichner, L.; Kullberg, B.J. Invasive candidiasis. Nat. Rev. Dis. Prim. 2018, 4, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2015, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Andes, D.R.; Diekema, D.J.; Horn, D.L.; Reboli, A.C.; Rotstein, C.; Franks, B.; Azie, N.E. Epidemiology and outcomes of invasive candidiasis due to non-albicans species of Candida in 2,496 patients: Data from the Prospective Antifungal Therapy (PATH) registry 2004–2008. PLoS ONE 2014, 9, e0101510. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Diekema, D.J.; Turnidge, J.D.; Castanheira, M.; Jones, R.N. Twenty Years of the SENTRY Antifungal Surveillance Program: Results for Candida Species From 1997-2016. Open Forum Infect. Dis. 2019, 6, S79–S94. [Google Scholar] [CrossRef] [Green Version]
- Klotz, S.A.; Chasin, B.S.; Powell, B.; Gaur, N.K.; Lipke, P.N. Polymicrobial bloodstream infections involving Candida species: Analysis of patients and review of the literature. Diagn. Microbiol. Infect. Dis. 2007, 59, 401–406. [Google Scholar] [CrossRef]
- Andes, D.R.; Safdar, N.; Baddley, J.W.; Alexander, B.; Brumble, L.; Freifeld, A.; Hadley, S.; Herwaldt, L.; Kauffman, C.; Lyon, G.M.; et al. The epidemiology and outcomes of invasive Candida infections among organ transplant recipients in the United States: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Transpl. Infect. Dis. 2016, 18, 921–931. [Google Scholar] [CrossRef] [Green Version]
- Cassagne, C.; Normand, A.C.; Bonzon, L.; L’Ollivier, C.; Gautier, M.; Jeddi, F.; Ranque, S.; Piarroux, R. Routine identification and mixed species detection in 6,192 clinical yeast isolates. Med. Mycol. 2016, 54, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Guinea, J.; Zaragoza, Ó.; Escribano, P.; Martín-Mazuelos, E.; Pemán, J.; Sánchez-Reus, F.; Cuenca-Estrella, M. Molecular identification and antifungal susceptibility of yeast isolates causing fungemia collected in a population-based study in Spain in 2010 and 2011. Antimicrob. Agents Chemother. 1990, 58, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.-L.; Chu, W.-L.; Lin, C.-C.; Zhou, Z.-L.; Chen, P.-N.; Lo, H.-J.; Hospitals, T. Mixed yeast infections in Taiwan. Med. Mycol. 2018, 56, 770–773. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Muñoz, P.; Guinea, J.; Rodríguez-Créixemes, T.; Bouza, E. Mixed Fungemia: Incidence, Risk Factors, and Mortality in a General Hospital. Clin. Infect. Dis. 2007, e109, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, T.J.; Bruns, T.; Lee, S.; Taylor, J. Amplicication and Direct Sequiencing of Fungal Ribosomal RNA Genes for Phylogenetics; Academic Press, Inc.: Cambridge, MA, USA, 1990; Volume 2. [Google Scholar]
- Rodriguez-Tudela, J.; Arendrup, M.; Barchiesi, F.; Bille, J.; Chryssanthou, E.; Cuenca-Estrella, M.; Dannaoui, E.; Denning, D.; Donnelly, J.; Dromer, F.; et al. EUCAST DEFINITIVE DOCUMENT EUCAST Definitive Document EDef 7.1: Method for the determination of broth dilution MICs of antifungal agents for fermentative yeasts Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST)*. Clin. Microbiol. Infect. 2008, 14, 398–405. [Google Scholar] [CrossRef]
- Desnos-Ollivier, M.; Bretagne, S.; Raoux, D.; Hoinard, D.; Dromer, F.; Dannaoui, E. Mutations in the fks1 gene in Candida albicans, C. tropicalis, and C. krusei correlate with elevated caspofungin MICs uncovered in AM3 medium using the method of the European Committee on Antibiotic Susceptibility testing. Antimicrob. Agents Chemother. 2008, 52, 3092–3098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawrot, U.; Pajączkowska, M.; Fleischer, M.; Przondo-Mordarska, H.; Samet, A.; Piasecka-Pazik, D.; Komarnicka, J.; Sulik-Tyszka, B.; Swoboda-Kopeć, E.; Cieślik, J.; et al. Candidaemia in polish hospitals—A multicentre survey. Mycoses 2013, 56, 576–581. [Google Scholar] [CrossRef]
- Mohr, A.; Simon, M.; Joha, T.; Hanses, F.; Salzberger, B.; Hitzenbichler, F. Epidemiology of candidemia and impact of infectious disease consultation on survival and care. Infection 2020, 48, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Siopi, M.; Tarpatzi, A.; Kalogeropoulou, E.; Damianidou, S.; Vasilakopoulou, A.; Vourli, S.; Pournaras, S.; Meletiadis, J. Epidemiological trends of fungemia in Greece with a focus on candidemia during the recent financial crisis: A 10-year survey in a tertiary care academic hospital and review of literature. Antimicrob. Agents Chemother. 2020, 64, 1–17. [Google Scholar] [CrossRef]
- Gülmez, D.; Alp, S.; Gursoy, G.; Ayaz, C.M.; Dogan, O.; Arikan-Akdagli, S.; Akova, M. Mixed fungaemia: An 18-year report from a tertiary-care university hospital and a systematic review. Clin. Microbiol. Infect. 2020, 26, 833–841. [Google Scholar] [CrossRef]
- Pulimood, S.; Ganesan, L.; Alangaden, G.; Chandrasekar, P. Polymicrobial candidemia. Diagn. Microbiol. Infect. Dis. 2002, 44, 353–357. [Google Scholar] [CrossRef]
- Tati, S.; Davidow, P.; McCall, A.; Hwang-Wong, E.; Rojas, I.G.; Cormack, B.; Edgerton, M. Candida glabrata Binding to Candida albicans Hyphae Enables Its Development in Oropharyngeal Candidiasis. PLOS Pathog. 2016, 12, e1005522. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Perlin, D.S. Echinocandin resistance: An emerging clinical problem? Curr. Opin. Infect. Dis. 2014, 27, 484–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornely, O.A.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.J.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; et al. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Non-neutropenic adult patients. Clin. Microbiol. Infect. 2012, 18 (Suppl. 7), 19–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perlin, D.S. Echinocandin Resistance, Susceptibility Testing and Prophylaxis: Implications for Patient Management. Drugs 2014, 74, 1573–1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnelli, C.; Guinea, J.; Valerio, M.; Escribano, P.; Bouza, E.; Muñoz, P. Infectious endocarditis caused by Candida glabrata: Evidence of in vivo development of echinocandin resistance. Rev. Esp. Quimioter 2019, 32, 395–397. [Google Scholar]
- Rivero-Menendez, O.; Navarro-Rodriguez, P.; Bernal-Martinez, L.; Martin-Cano, G.; Lopez-Perez, L.; Sanchez-Romero, I.; Perez-Ayala, A.; Capilla, J.; Zaragoza, O.; Alastruey-Izquierdo, A. Clinical and Laboratory Development of Echinocandin Resistance in Candida glabrata: Molecular Characterization. Front. Microbiol. 2019, 10, 1585. [Google Scholar] [CrossRef] [Green Version]
- Arendrup, M.C.; Dzajic, E.; Jensen, R.H.; Johansen, H.K.; Kjaeldgaard, P.; Knudsen, J.D.; Kristensen, L.; Leitz, C.; Lemming, L.E.; Nielsen, L.; et al. Epidemiological changes with potential implication for antifungal prescription recommendations for fungaemia: Data from a nationwide fungaemia surveillance programme. Clin. Microbiol. Infect. 2013, 19, e343–e353. [Google Scholar] [CrossRef] [Green Version]
- Accoceberry, I.; Couzigou, C.; Fitton-Ouhabi, V.; Biteau, N.; Noël, T. Challenging SNP impact on caspofungin resistance by full-length FKS1 allele replacement in Candida lusitaniae. J. Antimicrob. Chemother. 2019, 74, 618–624. [Google Scholar] [CrossRef]
- Perlin, D.S. Echinocandin Resistance in Candida. Clin. Infect. Dis. 2015, 61, S612–S617. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Country | No. Centers | No. of Yeast Cultures | Yeast Culture (+) | MY | |
|---|---|---|---|---|---|
| n | % (Range) | ||||
| Europe | |||||
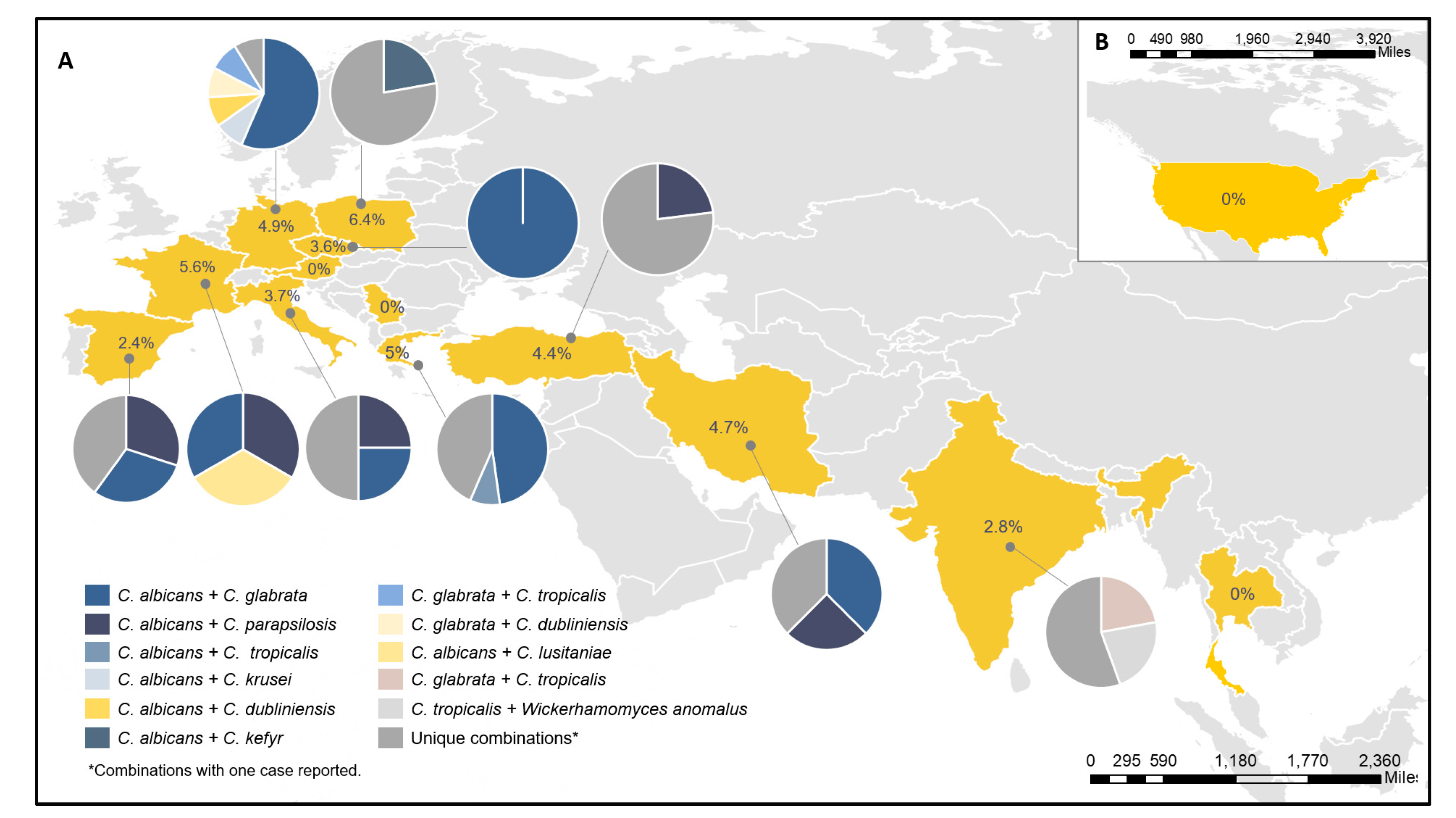
| Poland | 2 | 3257 | 188 | 12 | 6.4% (5.7%–10.0%) |
| France | 4 | 75,899 | 444 | 25 | 5.6% (3.8%–7.5%) |
| Greece | 2 | 6824 | 298 | 15 | 5% (0.5%–14.3%) |
| Germany | 1 | 32,190 | 491 | 24 | 4.9% (4.9%) |
| Turkey | 3 | 1853 | 296 | 13 | 4.4% (3.2%–7.0%) |
| Italy | 2 | 17,596 | 164 | 6 | 3.7% (2.8%–8.7%) |
| Czech Republic | 1 | 3834 | 56 | 2 | 3.6% (3.6%) |
| Spain | 11 | 121,579 | 869 | 21 | 2.4% (0%–4.8%) |
| Austria | 1 | 3479 | 23 | 0 | 0% (0%) |
| Serbia | 1 | 68 | 11 | 0 | 0% (0%) |
| Total Europe | 28 | 266,579 | 2840 | 118 | 4.2% (0%–6.4%) |
| Other countries | |||||
| Iran | 3 | 3420 | 383 | 18 | 4.7% (2.8%–30%) |
| India | 1 | 25,149 | 505 | 14 | 2.8% (2.8%) |
| Thailand | 1 | 12,602 | 10 | 0 | 0% (0%) |
| The United States | 1 | 51,936 | 3157 | 0 | 0% (0%) |
| Total | 34 | 359,686 | 6895 | 150 | 2.2% (0%–6.4%) |
| Variable | n | % |
|---|---|---|
| Sex | ||
| Male | 80 | 53.3 |
| Female | 70 | 46.7 |
| Age, median years (IQR) | 63 (40–74) | |
| Underlying conditions | ||
| Immunosuppression | ||
| Hematological disease | 53 | 35.5 |
| Neutropenia | 6 | 4.0 |
| Solid organ transplantation | 5 | 3.3 |
| Major surgery | 85 | 56.6 |
| Chronic disease/Behavioral factor | ||
| Alcoholism | 10 | 6.6 |
| Chronic cardiovascular disease | 21 | 14.0 |
| Chronic liver disease | 10 | 6.6 |
| Chronic pulmonary disease | 16 | 10.6 |
| Chronic renal disease | 9 | 6.0 |
| Diabetes mellitus | 22 | 14.6 |
| IV drug abuse | 3 | 2.0 |
| Treatment in ICU | 69 | 46.0 |
| Central venous catheter | 72 | 48.0 |
| No risk factor reported | 10 | 6.6 |
| Principal site of infection | ||
| Blood | 85 | 56.7 |
| Peritoneal fluid | 50 | 33.3 |
| Biliary tract | 12 | 8.0 |
| Deep soft tissue | 8 | 5.3 |
| Lung | 6 | 4.0 |
| Other body sites | 11 | 7.3 |
| Species Combination | N | % |
|---|---|---|
| Candida albicans+ | ||
| Candida glabrata | 42 | 34.4% |
| Candida parapsilosis | 17 | 13.9% |
| Candida tropicalis | 5 | 4.1% |
| Candida kefyr | 5 | 4.1% |
| Candida krusei | 5 | 4.1% |
| Candida dubliniensis | 3 | 2.5% |
| Candida inconspicua | 2 | 1.6% |
| Candida lusitaniae | 1 | 0.8% |
| Candida orthopsilosis | 1 | 0.8% |
| Saccharomyces cerevisiae | 1 | 0.8% |
| Candida glabrata + Candida krusei | 1 | 0.8% |
| Candida glabrata + Candida tropicalis | 2 | 1.6% |
| Candida glabrata+ | ||
| Candida tropicalis | 8 | 6.6% |
| Candida krusei | 3 | 2.5% |
| Candida dubliniensis | 2 | 1.6% |
| Candida parapsilosis | 2 | 1.6% |
| Candida kefyr | 2 | 1.6% |
| Candida lusitaniae | 1 | 0.8% |
| Cyberlindnera jadinii | 1 | 0.8% |
| Candida parapsilosis+ | ||
| Candida lusitaniae | 3 | 2.5% |
| Candida tropicalis | 2 | 1.6% |
| Lodderomyces elongisporus | 1 | 0.8% |
| Meyerozyma guilliermondii | 1 | 0.8% |
| Trichosporon asahii | 1 | 0.8% |
| Candida krusei+ | ||
| Candida lusitaniae | 1 | 0.8% |
| Candida tropicalis | 1 | 0.8% |
| Candida tropicalis + Saccharomyces cerevisiae | 1 | 0.8% |
| Dipodascus geotrichum + Pichia barkeri | 1 | 0.8% |
| Dipodascus geotrichum | 1 | 0.8% |
| Candida kefyr | 1 | 0.8% |
| Candida tropicalis+ | ||
| Wickerhamomyces anomalus | 2 | 1.6% |
| Candida dubliniensis | 1 | 0.8% |
| Saccharomyces cerevisiae + Candida dubliniensis | 1 | 0.8% |
| Total | 122 | 100% |
| Species (No.) | AMB | 5FC | FZ | ITC | ISAV | PSC | VRC | ANF | CPF | MCF |
|---|---|---|---|---|---|---|---|---|---|---|
| C. albicans (82) | ||||||||||
| GM | 0.19 | 0.16 | 0.19 | 0.02 | 0.02 | 0.02 | 0.02 | 0.01 | 0.21 | 0.006 |
| MIC50 | 0.25 | 0.12 | 0.12 | 0.015 | 0.015 | 0.015 | 0.015 | 0.007 | 0.25 | 0.007 |
| MIC90 | 0.25 | 0.25 | 0.25 | 0.03 | 0.06 | 0.03 | 0.015 | 0.015 | 0.25 | 0.007 |
| MIC Range | 0.06–0.5 | 0.12–64 | 0.12–32 | 0.015–1 | 0.015–8 | 0.015–1 | 0.015–0.25 | 0.007–0.060 | 0.004–1 | 0.004–0.060 |
| R/N–WT *, n (%) | 0 (0%) | NA | 4 (4.9%) | 6 (7.3%) | NA | 6 (7.3%) | 0 (0%) | 1 (1.2%) | 1 (1.2%) | 1 (1.2%) |
| C. glabrata (64) | ||||||||||
| GM | 0.33 | 0.12 | 2.30 | 0.213 | 0.06 | 0.21 | 0.06 | 0.02 | 0.38 | 0.01 |
| MIC50 | 0.5 | 0.12 | 2 | 0.25 | 0.06 | 0.25 | 0.06 | 0.015 | 0.5 | 0.007 |
| MIC90 | 0.5 | 0.12 | 4 | 0.5 | 0.25 | 0.5 | 0.120 | 0.06 | 0.5 | 0.015 |
| MIC Range | 0.12–0.5 | 0.12–2 | 0.5–64 | 0.015–4 | 0.015–4 | 0.015–4 | 0.015–2 | 0.007–0.06 | 0.25–0.5 | 0.007–0.030 |
| R/N–WT *, n (%) | 0 (0%) | NA | 1 (1.6%) | 1 (1.6%) * | NA | 2 (3.1%) * | 2 (3.1%) * | 0 (0%) | 0 (0%) | 0 (0%) |
| C. parapsilosis (27) | ||||||||||
| GM | 0.41 | 0.12 | 0.50 | 0.05 | 0.02 | 0.03 | 0.02 | 0.97 | 1.2 | 1.02 |
| MIC50 | 0.5 | 0.12 | 0.50 | 0.06 | 0.015 | 0.03 | 0.015 | 2 | 1 | 1 |
| MIC90 | 0.5 | 0.12 | 2 | 0.12 | 0.015 | 0.06 | 0.03 | 4 | 2 | 2 |
| MIC Range | 0.12–1 | 0.12–0.25 | 0.25–16 | 0.015–0.25 | 0.015–0.06 | 0.015–0.25 | 0.015–0.25 | 0.015–4 | 0.25–2 | 0.007–2 |
| R/N–WT *, n (%) | 0 (0%) | NA | 1 (3.7%) | 1 (3.7%) | NA | 2 (7.4%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| C. tropicalis (22) | ||||||||||
| GM | 0.30 | 0.29 | 0.94 | 0.03 | 0.03 | 0.03 | 0.06 | 0.01 | 0.24 | 0.02 |
| MIC50 | 0.25 | 0.12 | 0.5 | 0.03 | 0.015 | 0.03 | 0.5 | 0.015 | 0.25 | 0.015 |
| MIC90 | 0.5 | 2 | 16 | 0.120 | 0.5 | 0.12 | 0.5 | 0.03 | 0.25 | 0.03 |
| MIC Range | 0.12–0.5 | 0.12–32 | 0.12–64 | 0.015–0.25 | 0.015–2 | 0.015–0.5 | 0.015–8 | 0.007–0.125 | 0.12–1 | 0.007–2 |
| R/N–WT *, n (%) | 0 (0%) | NA | 4 (18.2%) | 2 (9%) | NA | 4 (18.2%) | 3 (13.6%) | 1 (4.5%) | ––- | 1 (4.5%) * |
| C. krusei (15) | ||||||||||
| GM | 0.48 | 2.64 | 26.60 | 0.14 | 0.08 | 0.25 | 0.25 | 0.03 | 0.66 | 0.09 |
| MIC50 | 0.5 | 2 | 32 | 0.12 | 0.120 | 0.12 | 0.25 | 0.03 | 0.5 | 0.125 |
| MIC90 | 0.5 | 4 | 32 | 0.5 | 0.25 | 0.25 | 0.5 | 0.06 | 1 | 0.125 |
| MIC Range | 0.12–0.1 | 1–4 | 16–64 | 0.03–0.5 | 0.015–0.25 | 0.015–0.25 | 0.12–0.5 | 0.015–0.06 | 0.5–1 | 0.007–0.12 |
| R/N-WT *, n (%) | 0 (0%) | NA | 15 (100%) & | 0 (0%) * | NA | 0 (0%) * | 0 (0%) * | 0 (0%) | 0 (0%) * | |
| Other (35) | ||||||||||
| GM | 0.26 | 0.30 | 1.05 | 0.08 | 0.04 | 0.07 | 0.04 | 0.05 | 0.40 | 0.06 |
| MIC50 | 0.25 | 0.12 | 0.25 | 0.06 | 0.015 | 0.06 | 0.015 | 0.03 | 0.25 | 0.06 |
| MIC90 | 0.5 | 4 | 32 | 0.5 | 0.25 | 0.5 | 0.25 | 4 | 1 | 1 |
| MIC Range | 0.03–1 | 0.12–32 | 0.12–64 | 0.015–1 | 0.015–1 | 0.015–1 | 0.015–1 | 0.007–4 | 0.03–16 | 0.007–2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medina, N.; Soto-Debrán, J.C.; Seidel, D.; Akyar, I.; Badali, H.; Barac, A.; Bretagne, S.; Cag, Y.; Cassagne, C.; Castro, C.; et al. MixInYeast: A Multicenter Study on Mixed Yeast Infections. J. Fungi 2021, 7, 13. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010013
Medina N, Soto-Debrán JC, Seidel D, Akyar I, Badali H, Barac A, Bretagne S, Cag Y, Cassagne C, Castro C, et al. MixInYeast: A Multicenter Study on Mixed Yeast Infections. Journal of Fungi. 2021; 7(1):13. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010013
Chicago/Turabian StyleMedina, Narda, Juan Carlos Soto-Debrán, Danila Seidel, Isin Akyar, Hamid Badali, Aleksandra Barac, Stéphane Bretagne, Yasemin Cag, Carole Cassagne, Carmen Castro, and et al. 2021. "MixInYeast: A Multicenter Study on Mixed Yeast Infections" Journal of Fungi 7, no. 1: 13. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010013