Filamentous Fungal Infections in a Tertiary Care Setting: Epidemiology and Clinical Outcome

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Setting
2.4. Outcomes
2.5. Microbiological Diagnostics, Data Sources, and Variables
2.6. Statistial Analyses
3. Results
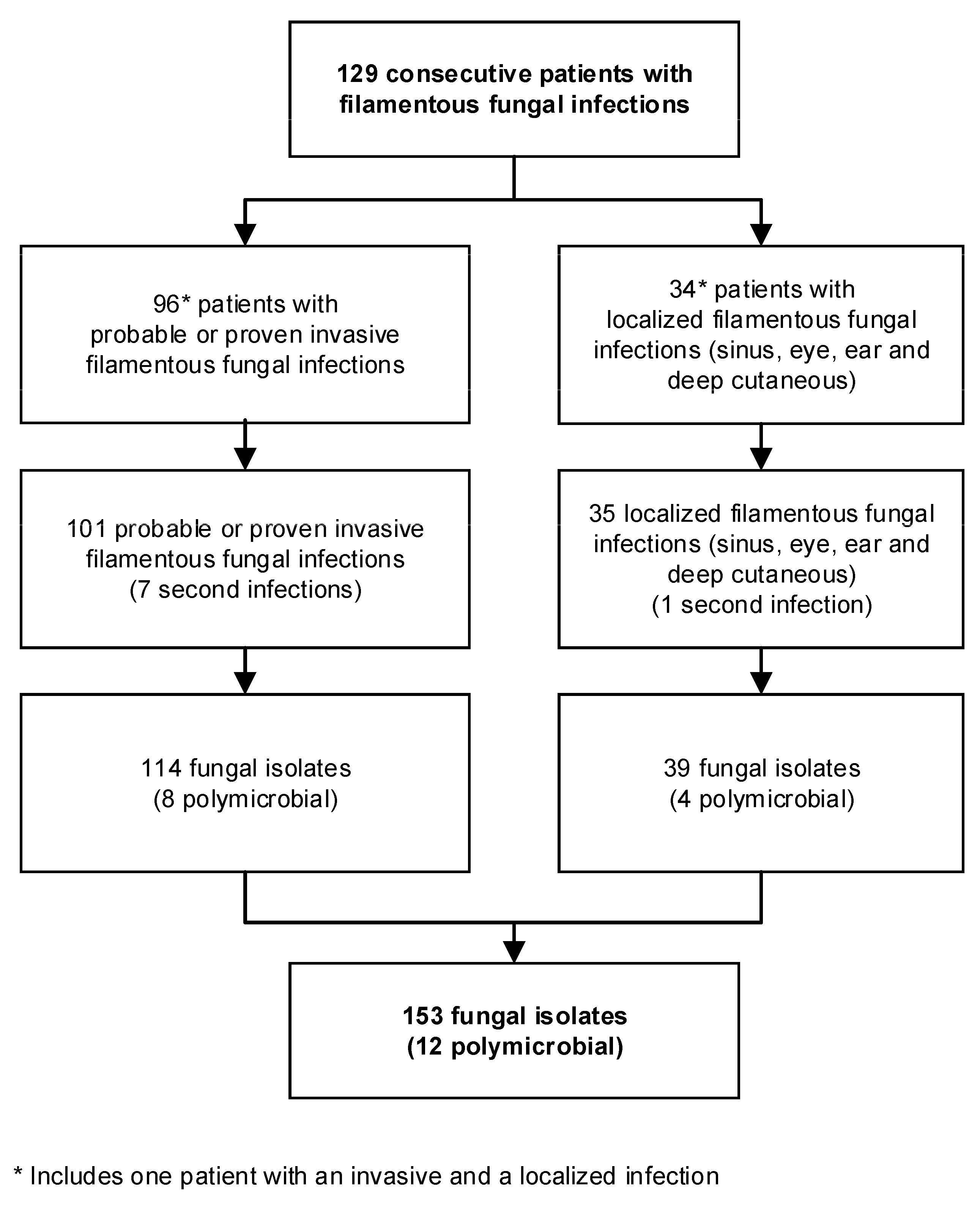
3.1. Patient Characteristics
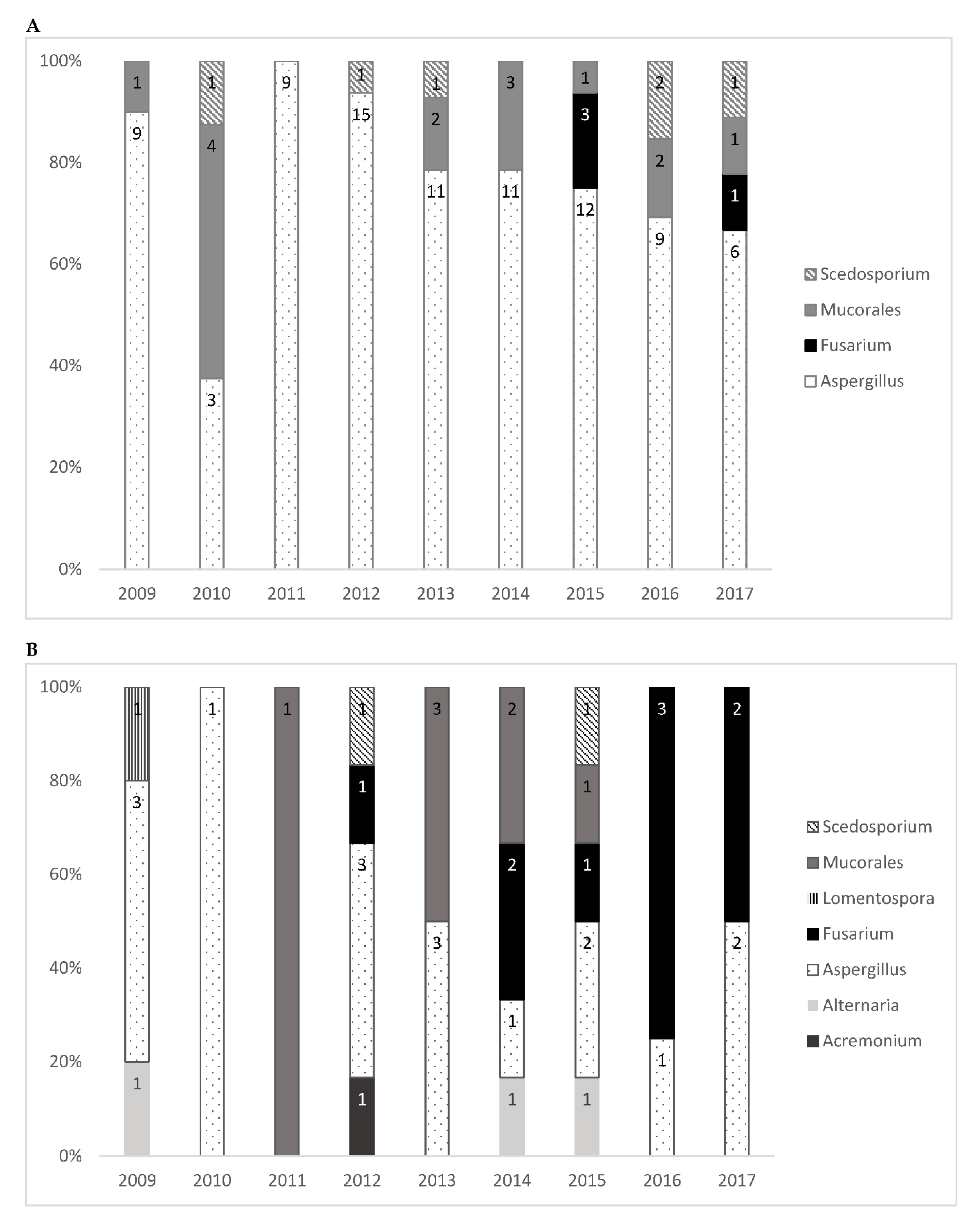
3.2. Number and Species of Isolated Filamentous Fungi
3.3. Organs Affected by Filamentous Fungi
3.4. Diagnostic Methods
3.5. Mortality among Patients with Probable or Proven Invasive Filamentous Fungal Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|
| Alternaria spp. 1 | - | 1 | - | - | - | - | - | - | - | 1 (0.9%) |
| Aspergillus spp. | 9 | 3 | 9 | 15 | 11 | 11 | 12 | 9 | 6 | 85 (74.6%) |
| Aspergillus flavus | 1 | - | - | 2 | 2 | 1 | - | - | - | 6 (5.3%) |
| Aspergillus fumigatus | 7 | 3 | 7 | 10 | 8 | 8 | 10 | 7 | 6 | 66 (57.9%) |
| Aspergillus nidulans | - | - | - | 1 | - | 1 | - | - | - | 2 (1.8%) |
| Aspergillus niger | 1 | - | - | 1 | 1 | 1 | 2 | 2 | - | 8 (7.0%) |
| Aspergillus terreus | - | - | 2 | 1 | - | - | - | - | - | 3 (2.6%) |
| Fusarium spp. | - | - | - | - | - | - | 3 | 1 | 1 | 4 (3.5%) |
| Fusarium oxysporum species complex | - | - | - | - | - | - | 1 | - | - | 1 (0.9%) |
| Fusarium fujikuroi species complex (F. proliferatum) | - | - | - | - | - | - | 1 | - | - | 1 (0.9%) |
| Fusarium solani species complex | - | - | - | - | - | - | 1 | - | - | 1 (0.9%) |
| Other 1 | - | - | - | - | - | - | - | - | 1 | 1 (0.9%) |
| Histoplasma spp. | - | - | - | - | 1 | - | - | - | - | 1 (0.9%) |
| Histoplasma capsulatum | - | - | - | - | 1 | - | - | - | - | 1 (0.9%) |
| Mucorales | 1 | 4 | - | - | 2 | 3 | 1 | 2 | 1 | 14 (13.2%) |
| Lichtheimia corymbifera | - | - | - | - | - | 1 | - | - | - | 1 (0.9%) |
| Lichtheimia ramosa | - | - | - | - | 1 | - | - | - | - | 1 (0.9%) |
| Rhizomucor pusillus | - | - | - | - | - | - | - | 1 | - | 1 (0.9%) |
| Rhizopus arrhizus | - | 3 | - | - | - | 2 | - | - | - | 6 (5.3%) |
| Rhizopus microsporus | 1 | - | - | - | 1 | - | 1 | - | 1 | 4 (3.5%) |
| Rhizopus spp. 1 | - | 1 | - | - | - | - | - | - | - | 1 (0.9%) |
| Paecilomyces spp. | - | - | - | 1 | - | - | - | - | - | 1 (0.9%) |
| Paecilomyces variotii | - | - | - | 1 | - | - | - | - | - | 1 (0.9%) |
| Scedosporium spp. | - | 1 | - | 1 | 1 | - | - | 2 | 1 | 6 (5.3%) |
| Scedosporium apiospermum | - | 1 | - | 1 | 1 | - | - | 2 | 1 | 6 (5.3%) |
| Schizophyllum spp. | - | - | - | - | 1 | - | - | - | - | 1 (0.9%) |
| Schizophyllum commune | - | - | - | - | 1 | - | - | - | - | 1 (0.9%) |
| Trichoderma spp. 1 | 1 | - | - | - | - | - | - | - | - | 1 (0.9%) |
| Total | 11 (9.6%) | 9 (7.9%) | 9 (7.9%) | 17 (14.9%) | 16 (14.0%) | 14 (12.3%) | 16 (14.0%) | 13 (11.9%) | 9 (7.9%) | 114 |
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | Total | |
|---|---|---|---|---|---|---|---|---|---|---|
| Acremonium spp. 1 | - | - | - | 1 | - | - | - | - | - | 1 (2.6%) |
| Alternaria spp. 1 | 1 | - | - | - | - | 1 | 1 | - | - | 3 (7.7%) |
| Alternaria alternata | 1 | - | - | - | - | - | - | - | - | 1 (2.6%) |
| Alternaria infectoria | - | - | - | - | - | - | 1 | - | - | 1 (2.6%) |
| Other 1 | - | - | - | - | - | 1 | - | - | - | 1 (2.6%) |
| Aspergillus spp. | 3 | 1 | - | 3 | 3 | 1 | 2 | 1 | 2 | 16 (41.0%) |
| Aspergillus flavus | - | 1 | - | - | - | - | 1 | - | 1 | 3 (7.7%) |
| Aspergillus fumigatus | 3 | - | - | 2 | 2 | 1 | 1 | 1 | 1 | 11 (28.2%) |
| Aspergillus nidulans | - | - | - | - | 1 | - | - | - | - | 1 (2.6%) |
| Aspergillus terreus | - | - | - | 1 | - | - | - | - | - | 1 (2.6%) |
| Fusarium spp. | - | - | - | 1 | - | 2 | 1 | 3 | 2 | 9 (23.1%) |
| Fusarium oxysporum species complex | - | - | - | 1 | - | 1 | - | 1 | - | 3 (7.7%) |
| Fusarium fujikuroi species complex (F. proliferatum) | - | - | - | - | - | - | - | - | 1 | 1 (2.6%) |
| Fusarium solani species complex | - | - | - | - | - | - | 1 | 1 | - | 2 (5.1%) |
| Other 1 | - | - | - | - | - | 1 | - | 1 | 1 | 3 (7.7%) |
| Lomentospora spp. | 1 | - | - | - | - | - | - | - | - | 1 (2.6%) |
| Lomentospora prolificans | 1 | - | - | - | - | - | - | - | - | 1 (2.6%) |
| Mucorales | - | - | 1 | - | 3 | 2 | 1 | - | - | 6 (15.4%) |
| Lichtheimia corymbifera | - | - | 1 | - | 2 | - | - | - | - | 3 (7.7%) |
| Mucor circinelloides | - | - | - | - | 1 | - | - | - | - | 1 (2.6%) |
| Rhizomucor pusillus | - | - | - | - | - | 1 | - | - | - | 1 (2.6%) |
| Rhizopus arrhizus | - | - | - | - | - | 1 | 1 | - | - | 2 (5.1%) |
| Scedosporium spp. | 1 | - | - | 1 | - | - | 1 | - | - | 2 (5.1%) |
| Scedosporium apiospermum | - | - | - | 1 | - | - | 1 | - | - | 2 (5.1%) |
| Total | 5 (11.4%) | 1 (2.6%) | 1 (2.6%) | 6 (15.4%) | 6 (15.4%) | 6 (15.4%) | 6 (15.4%) | 4 (10.3%) | 4 (10.3%) | 39 |
References
- Pfaller, M.A.; Pappas, P.G.; Wingard, J.R. Invasive Fungal Pathogens: Current Epidemiological Trends. Clin. Infect. Dis. 2006, 43, S3–S14. [Google Scholar] [CrossRef]
- Lass-Flörl, C.; Cuenca-Estrella, M. Changes in the epidemiological landscape of invasive mould infections and disease. J. Antimicrob. Chemother. 2017, 72, i5–i11. [Google Scholar] [CrossRef] [PubMed]
- Klingspor, L.; Saaedi, B.; Ljungman, P.; Szakos, A. Epidemiology and outcomes of patients with invasive mould infections: A retrospective observational study from a single centre (2005–2009). Mycoses 2015, 58, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Montagna, M.T.; Lovero, G.; Coretti, C.; Martinelli, D.; Delia, M.; De Giglio, O.; Caira, M.; Puntillo, F.; D’Antonio, D.; Venditti, M.; et al. SIMIFF study: Italian fungal registry of mold infections in hematological and non-hematological patients. Infection 2014, 42, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Neofytos, D.; Treadway, S.; Ostrander, D.; Alonso, C.D.; Dierberg, K.L.; Nussenblatt, V.; Durand, C.M.; Thompson, C.B.; Marr, K.A. Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: A 10-year, single-center experience. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2013, 15, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvanitis, M.; Anagnostou, T.; Fuchs, B.B.; Caliendo, A.M.; Mylonakis, E. Molecular and nonmolecular diagnostic methods for invasive fungal infections. Clin. Microbiol. Rev. 2014, 27, 490–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ascioglu, S.; Rex, J.H.; de Pauw, B.; Bennett, J.E.; Bille, J.; Crokaert, F.; Denning, D.W.; Donnelly, J.P.; Edwards, J.E.; Erjavec, Z.; et al. Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: An international consensus. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2002, 34, 7–14. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2008, 46, 1813–1821. [Google Scholar] [CrossRef]
- Brown, G.D.; Denning, D.W.; Gow, N.A.; Levitz, S.M.; Netea, M.G.; White, T.C. Hidden killers: Human fungal infections. Sci. Transl. Med. 2012, 4, 165rv113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, D.Z.P.; Schwartz, I.S. Emerging Fungal Infections: New Patients, New Patterns, and New Pathogens. J. Fungi 2019, 5, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongomin, F.; Gago, S.; Oladele, R.O.; Denning, D.W. Global and Multi-National Prevalence of Fungal Diseases-Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Perkhofer, S.; Lass-Flörl, C.; Hell, M.; Russ, G.; Krause, R.; Hönigl, M.; Geltner, C.; Auberger, J.; Gastl, G.; Mitterbauer, M.; et al. The Nationwide Austrian Aspergillus Registry: A prospective data collection on epidemiology, therapy and outcome of invasive mould infections in immunocompromised and/or immunosuppressed patients. Int. J. Antimicrob. Agents 2010, 36, 531–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skiada, A.; Pagano, L.; Groll, A.; Zimmerli, S.; Dupont, B.; Lagrou, K.; Lass-Florl, C.; Bouza, E.; Klimko, N.; Gaustad, P.; et al. Zygomycosis in Europe: Analysis of 230 cases accrued by the registry of the European Confederation of Medical Mycology (ECMM) Working Group on Zygomycosis between 2005 and 2007. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2011, 17, 1859–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2015, 70, 270–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skiada, A.; Pavleas, I.; Drogari-Apiranthitou, M. Epidemiology and Diagnosis of Mucormycosis: An Update. J. Fungi 2020, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Walther, G.; Stasch, S.; Kaerger, K.; Hamprecht, A.; Roth, M.; Cornely, O.A.; Geerling, G.; Mackenzie, C.R.; Kurzai, O.; von Lilienfeld-Toal, M. Fusarium Keratitis in Germany. J. Clin. Microbiol. 2017, 55, 2983–2995. [Google Scholar] [CrossRef] [PubMed] [Green Version]


| Female | Male | Total | |
|---|---|---|---|
| Patients with probable or proven invasive infections | n = 44 | n = 52 | n = 96 |
| Age (years), median (IQR) | 50.0 (36.0–60.0) | 58.0 (34.5–65.8) | 52.5 (35.3–64) |
| Age, group, n (%) | |||
| 0–20 | 3 (6.8%) | 6 (11.5%) | 9 (9.4%) |
| 21–45 | 13 (29.5%) | 12 (23.0%) | 25 (26.0%) |
| 46–65 | 21 (47.7%) | 21 (40.4%) | 42 (43.8%) |
| 66-85 | 7 (15.9%) | 13 (25.0%) | 20 (20.8%) |
| Medical history, n (%) 1 | |||
| Solid organ transplantation | 19 (33.2%) | 26 (50%) | 45 (46.9%) |
| Hematologic malignancies 2 | 6 (13.6%) | 6 (11.5%) | 12 (12.5%) |
| Allogeneic stem cell transplantation | 1 (2.3%) | 4 (7.7%) | 5 (5.2%) |
| Solid cancer 3 | 3 (3.1%) | 8 (8.3%) | 11 (11.5%) |
| Chemotherapy or radiotherapy 4 | 7 (15.9%) | 8 (15.4%) | 15 (15.6%) |
| Diabetes | 7 (15.9%) | 9 (17.3%) | 16 (16.7%) |
| Cystic fibrosis | 4 (9.1%) | 1 (1.9%) | 5 (5.2%) |
| COPD | 6 (13.6%) | 15 (28.8%) | 21 (15.5%) |
| Heart disease | 16 (36.4%) | 10 (19.2%) | 26 (21.9%) |
| HIV infection | - | - | 0 (0.0%) |
| Congenital or acquired immunosuppression | 23 (52.3%) | 29 (55.8%) | 52 (54.2%) |
| Surgery within 30 days prior to diagnosis of fungal infection | 9 (20.5%) | 12 (23.1%) | 21 (21.9%) |
| Patients with localized infections | n = 18 | n = 16 | n = 34 |
| Age (years), median (IQR) | 45.5 (30.3–67.5) | 59.0 (42.8–64.8) | 53.5 (33.8–65.5) |
| Age, group, n (%) | |||
| 0–20 | 3 (16.7%) | 1 (6.3%) | 4 (11.8%) |
| 21–45 | 6 (33.3%) | 4 (25.0%) | 10 (29.4%) |
| 46–65 | 4 (41.0%) | 8 (50.0%) | 12 (35.3%) |
| 66–85 | 5 (27.8%) | 3 (18.8%) | 8 (23.5%) |
| Medical history, n (%) 1 | |||
| Solid organ transplantation | 2 (11.1%) | 3 (18.8%) | 5 (14.7%) |
| Hematologic malignancies 5 | 3 (16.7%) | 3 (18.8%) | 6 (17.6%) |
| Allogeneic stem cell transplantation | 1 (5.6%) | - | 1 (2.9%) |
| Solid cancer 6 | 1 (5.6%) | 2 (12.5%) | 3 (8.8%) |
| Chemotherapy or radiotherapy 4 | 4 (41.0%) | 2 (12.5%) | 6 (17.6%) |
| Diabetes | - | 2 (12.5%) | 2 (5.9%) |
| Cystic fibrosis | - | 1 (6.3%) | 1 (2.9%) |
| COPD | - | - | 0 (0.0%) |
| Heart disease | 2 (11.1%) | 1 (6.3%) | 3 (8.8%) |
| HIV infection | - | - | 0 (0.0%) |
| Congenital or acquired immunosuppression | 6 (33.3%) | 5 (31.3%) | 11 (32.4%) |
| Surgery within 30 days prior to diagnosis of fungal infection | 1 (5.6%) | 5 (31.3%) | 6 (17.6%) |
| Detected Fungus | Proven and Probable Invasive | Localized Infections (Sinus, Eye, Ear, and Deep Cutaneous) | Total |
|---|---|---|---|
| Acremonium spp. 1 | - | 1 (2.6%) | 1 (0.7%) |
| Alternaria spp. | 1 (0.9%) | 3 (7.7%) | 4 (2.6%) |
| Alternaria alternata | - | 1 (2.6%) | 1 (0.7%) |
| Alternaria infectoria | - | 1 (2.6%) | 1 (0.7%) |
| Other 1 | 1 (0.9%) | 1 (2.6%) | 2 (1.3%) |
| Aspergillus spp. | 85 (74.6%) | 16 (41.0%) | 101 (66.0%) |
| Aspergillus flavus | 6 (5.3%) | 3 (7.7%) | 9 (5.9%) |
| Aspergillus fumigatus | 66 (57.9%) | 11 (28.2%) | 77 (50.3%) |
| Aspergillus nidulans | 2 (1.8%) | 1 (2.6%) | 3 (2.0%) |
| Aspergillus niger | 8 (7.0%) | - | 8 (5.2%) |
| Aspergillus terreus | 3 (2.6%) | 1 (2.6%) | 4 (2.6%) |
| Fusarium spp. | 4 (3.5%) | 9 (23.1%) | 13 (8.5%) |
| Fusarium oxysporum species complex | 1 (0.9%) | 3 (7.7%) | 4 (2.6%) |
| Fusarium fujikuroi species complex (F. proliferatum) | 1 (0.9%) | 1 (2.6%) | 2 (1.3%) |
| Fusarium solani species complex | 1 (0.9%) | 2 (5.1%) | 3 (2.0%) |
| Other 1 | 1 (0.9%) | 3 (7.7%) | 4 (2.6%) |
| Histoplasma spp. | 1 (0.9%) | - | 1 (0.7%) |
| Histoplasma capsulatum | 1 (0.9%) | - | 1 (0.7%) |
| Lomentospora spp. | - | 1 (2.6%) | 1 (0.7%) |
| Lomentospora prolificans | - | 1 (2.6%) | 1 (0.7%) |
| Mucorales | 14 (12.3%) | 7 (17.9%) | 21 (13.7%) |
| Lichtheimia corymbifera | 1 (0.9%) | 3 (7.7%) | 4 (2.6%) |
| Lichtheimia ramosa | 1 (0.9%) | - | 1 (0.7%) |
| Mucor circinelloides | - | 1 (2.6%) | 1 (0.7%) |
| Rhizomucor pusillus | 1 (0.9%) | 1 (2.6%) | 2 (1.3%) |
| Rhizopus arrhizus | 6 (5.3%) | 1 (2.6%) | 8 (5.2%) |
| Rhizopus microsporus | 4 (3.5%) | - | 4 (2.6%) |
| Rhizopus spp. 1 | 1 (0.9%) | - | 1 (0.7%) |
| Paecilomyces spp. | 1 (0.9%) | - | 1 (0.7%) |
| Paecilomyces variotii | 1 (0.9%) | - | 1 (0.7%) |
| Scedosporium spp. | 6 (5.3%) | 3 (7.7%) | 8 (5.2%) |
| Scedosporium apiospermum | 6 (5.3%) | 2 (5.1%) | 8 (5.2%) |
| Schizophyllum spp. | 1 (0.9%) | - | 1 (0.7%) |
| Schizophyllum commune | 1 (0.9%) | - | 1 (0.7%) |
| Trichoderma spp. 1 | 1 (0.9%) | - | 1 (0.7%) |
| Total | 114 | 39 | 153 |
| Genus/Order of Fungi | Hematologic Malignancies 1 | Allogeneic Stem Cell Transplantation | Lung Transplantation | Heart Transplantation | Combined Heart and Lung Transplantation | Kidney Transplantation |
|---|---|---|---|---|---|---|
| Aspergillus spp. | 9 | 4 | 34 | 1 | 3 | 4 |
| Fusarium spp. | - | 1 | 2 | - | - | - |
| Mucorales | 4 | 1 | 3 | 2 | 1 | 1 |
| Scedosporium spp. | - | - | 3 | - | - | - |
| Total | 13 | 6 | 42 | 3 | 4 | 5 |
| Genus/Order of Fungi | Proven and Probable Invasive Infections | Localized Infections | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lung | Disseminated | CNS | Heart | Soft Tissue and Wounds 1 | Stomach 1 | Sinus 1 | Eye 1 | Sinus and Ear | Eye | Deep Cutaneous | |
| Alternaria spp. | - | - | - | - | 1 | - | - | - | - | 1 | 2 |
| Aspergillus spp. | 82 | 11 | 3 | 2 | 1 | 1 | 1 | 1 | 13 | 3 | - |
| Fusarium spp. | 3 | 1 | - | - | - | - | - | - | - | 8 | 1 |
| Histoplasma spp. | 1 | 1 | - | 1 | - | - | - | - | - | - | - |
| Lomentospora spp. | - | - | - | - | - | - | - | - | - | 1 | - |
| Mucorales | 11 | 4 | 1 | 2 | 4 | 1 | - | - | 6 | - | 1 |
| Paecilomyces spp. | - | 1 | - | - | - | - | - | - | - | - | - |
| Scedosporium spp. | 5 | 1 | - | 1 | 2 | - | - | - | 1 | 1 | - |
| Schizophyllum spp. | 1 | - | - | - | - | - | - | - | - | - | - |
| Trichoderma spp. | 1 | - | - | - | - | - | - | - | - | - | - |
| Total | 104 | 19 | 4 | 6 | 8 | 2 | 1 | 1 | 20 | 14 | 4 |
| Genus/Order of Fungi | Number of Fungal Isolates | Culture | PCR | Histology | Galactomannan Assay |
|---|---|---|---|---|---|
| Probable or proven invasive infections | |||||
| Alternaria spp. | 1 (0.9%) | 1 | 1 | 1 | - |
| Aspergillus spp. | 85 (74.6%) | 75 | 10 | 22 | 7 |
| Fusarium spp. | 4 (3.5%) | 4 | - | - | - |
| Histoplasma spp. | 1 (0.9%) | 1 | - | 1 | - |
| Mucorales | 14 (12.3%) | 11 | 3 | 7 | - |
| Paecilomyces spp. | 1 (0.9%) | 1 | - | - | - |
| Scedosporium spp. | 6 (5.3%) | 6 | - | 1 | - |
| Schizophyllum spp. | 1 (0.9%) | 1 | - | - | - |
| Trichoderma spp. | 1 (0.9%) | 1 | - | - | - |
| Localized infections | |||||
| Acremonium spp. | 1 (2.6%) | 1 | - | - | - |
| Alternaria spp. | 3 (7.7%) | 3 | - | - | - |
| Aspergillus spp. | 16 (41.0%) | 16 | 1 | 4 | - |
| Fusarium spp. | 9 (23.1%) | 8 | 3 | 1 | - |
| Lomentospora spp. | 1 (2.6%) | 1 | - | 1 | - |
| Mucorales | 7 (17.9%) | 7 | 1 | 4 | - |
| Scedosporium spp. | 2 (5.1%) | 2 | - | 1 | - |
| 30 Days | 90 Days | ||||
|---|---|---|---|---|---|
| n | n Died | % (95% CI) | n Died | % (95% CI) | |
| Invasive fungal infection | 96 | 29 | 30.2% (22.1–40.5) | 41 | 42.7% (33.5–53.2) |
| Aspergillus spp. 1 | 76 | 20 | 26.3% (17.9–37.8) | 30 | 39.5% (29.5–51.4) |
| Mucorales 1 | 11 | 9 | 81.8% (55.8–97.2) | 10 | 90.9% (66.7–99.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van den Nest, M.; Wagner, G.; Riesenhuber, M.; Dolle, C.; Presterl, E.; Gartlehner, G.; Moertl, D.; Willinger, B. Filamentous Fungal Infections in a Tertiary Care Setting: Epidemiology and Clinical Outcome. J. Fungi 2021, 7, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010040
Van den Nest M, Wagner G, Riesenhuber M, Dolle C, Presterl E, Gartlehner G, Moertl D, Willinger B. Filamentous Fungal Infections in a Tertiary Care Setting: Epidemiology and Clinical Outcome. Journal of Fungi. 2021; 7(1):40. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010040
Chicago/Turabian StyleVan den Nest, Miriam, Gernot Wagner, Martin Riesenhuber, Constantin Dolle, Elisabeth Presterl, Gerald Gartlehner, Deddo Moertl, and Birgit Willinger. 2021. "Filamentous Fungal Infections in a Tertiary Care Setting: Epidemiology and Clinical Outcome" Journal of Fungi 7, no. 1: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7010040