
Evaluation of Three Commercial PCR Assays for the Detection of Azole-Resistant Aspergillus fumigatus from Respiratory Samples of Immunocompromised Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Specimens
2.2. Conventional Diagnostic
2.3. DNA Extraction
2.4. Real-Time PCR Assays
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bodey, G.; Bueltmann, B.; Duguid, W.; Gibbs, D.; Hanak, H.; Hotchi, M.; Mall, G.; Martino, P.; Meunier, F.; Milliken, S.; et al. Fungal infections in cancer patients: An international autopsy survey. Eur. J. Clin. Microbiol. Infect. Dis. 1992, 11, 99–109. [Google Scholar] [CrossRef]
- Ullmann, A.J.; Lipton, J.H.; Vesole, D.H.; Chandrasekar, P.; Langston, A.; Tarantolo, S.R.; Greinix, H.; Morais de Azevedo, W.; Reddy, V.; Boparai, N.; et al. Posaconazole or fluconazole for prophylaxis in severe graft-versus-host disease. N. Eng. J. Med. 2007, 356, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Maertens, J.; Winston, D.J.; Perfect, J.; Ullmann, A.J.; Walsh, T.J.; Helfgott, D.; Holowiecki, J.; Stockelberg, D.; Goh, Y.T.; et al. Posaconazole vs. Fluconazole or itraconazole prophylaxis in patients with neutropenia. N. Engl. J. Med. 2007, 356, 348–359. [Google Scholar] [CrossRef] [Green Version]
- Neofytos, D.; Treadway, S.; Ostrander, D.; Alonso, C.D.; Dierberg, K.L.; Nussenblatt, V.; Durand, C.M.; Thompson, C.B.; Marr, K.A. Epidemiology, outcomes, and mortality predictors of invasive mold infections among transplant recipients: A 10-year, single-center experience. Transpl. Infect. Dis. 2013, 15, 233–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koehler, P.; Cornely, O.A.; Bottiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. Covid-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Schauwvlieghe, A.; Rijnders, B.J.A.; Philips, N.; Verwijs, R.; Vanderbeke, L.; Van Tienen, C.; Lagrou, K.; Verweij, P.E.; Van de Veerdonk, F.L.; Gommers, D.; et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: A retrospective cohort study. Lancet Respir. Med. 2018, 6, 782–792. [Google Scholar] [CrossRef]
- Pagano, L.; Caira, M.; Candoni, A.; Offidani, M.; Fianchi, L.; Martino, B.; Pastore, D.; Picardi, M.; Bonini, A.; Chierichini, A.; et al. The epidemiology of fungal infections in patients with hematologic malignancies: The seifem-2004 study. Haematologica 2006, 91, 1068–1075. [Google Scholar] [PubMed]
- Kontoyiannis, D.P.; Marr, K.A.; Park, B.J.; Alexander, B.D.; Anaissie, E.J.; Walsh, T.J.; Ito, J.; Andes, D.R.; Baddley, J.W.; Brown, J.M.; et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: Overview of the transplant-associated infection surveillance network (transnet) database. Clin. Infect. Dis. 2010, 50, 1091–1100. [Google Scholar] [CrossRef]
- Ruhnke, M.; Behre, G.; Buchheidt, D.; Christopeit, M.; Hamprecht, A.; Heinz, W.; Heussel, C.P.; Horger, M.; Kurzai, O.; Karthaus, M.; et al. Diagnosis of invasive fungal diseases in haematology and oncology: 2018 update of the recommendations of the infectious diseases working party of the german society for hematology and medical oncology (agiho). Mycoses 2018, 61, 796–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Florl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 escmid-ecmm-ers guideline. Clin. Microbiol. Infect. 2018, 24 (Suppl. 1), e1–e38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, T.R.; Morton, C.O.; Springer, J.; Conneally, E.; Heinz, W.; Kenny, C.; Frost, S.; Einsele, H.; Loeffler, J. Combined real-time pcr and galactomannan surveillance improves diagnosis of invasive aspergillosis in high risk patients with haematological malignancies. Br. J. Haematol. 2013, 161, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Aguado, J.M.; Vazquez, L.; Fernandez-Ruiz, M.; Villaescusa, T.; Ruiz-Camps, I.; Barba, P.; Silva, J.T.; Batlle, M.; Solano, C.; Gallardo, D.; et al. Serum galactomannan versus a combination of galactomannan and polymerase chain reaction-based Aspergillus DNA detection for early therapy of invasive aspergillosis in high-risk hematological patients: A randomized controlled trial. Clin. Infect. Dis. 2015, 60, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Boch, T.; Spiess, B.; Cornely, O.A.; Vehreschild, J.J.; Rath, P.M.; Steinmann, J.; Heinz, W.J.; Hahn, J.; Krause, S.W.; Kiehl, M.G.; et al. Diagnosis of invasive fungal infections in haematological patients by combined use of galactomannan, 1,3-beta-d-glucan, Aspergillus pcr, multifungal DNA-microarray, and Aspergillus azole resistance pcrs in blood and bronchoalveolar lavage samples: Results of a prospective multicentre study. Clin. Microbiol. Infect. 2016, 22, 862–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, R.H.; Hagen, F.; Astvad, K.M.; Tyron, A.; Meis, J.F.; Arendrup, M.C. Azole-resistant Aspergillus fumigatus in denmark: A laboratory-based study on resistance mechanisms and genotypes. Clin. Microbiol. Infect. 2016, 22, e571–e579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verweij, P.E.; Chowdhary, A.; Melchers, W.J.; Meis, J.F. Azole resistance in Aspergillus fumigatus: Can we retain the clinical use of mold-active antifungal azoles? Clin. Infect. Dis 2016, 62, 362–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendrup, M.C.; Verweij, P.E.; Mouton, J.W.; Lagrou, K.; Meletiadis, J. Multicentre validation of 4-well azole agar plates as a screening method for detection of clinically relevant azole-resistant Aspergillus fumigatus. J. Antimicrob. Chemother. 2017, 72, 3325–3333. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, J.W.; Snelders, E.; Kampinga, G.A.; Rijnders, B.J.; Mattsson, E.; Debets-Ossenkopp, Y.J.; Kuijper, E.J.; Van Tiel, F.H.; Melchers, W.J.; Verweij, P.E. Clinical implications of azole resistance in Aspergillus fumigatus, The Netherlands, 2007–2009. Emerg. Infect. Dis. 2011, 17, 1846–1854. [Google Scholar] [CrossRef]
- Chong, G.M.; van der Beek, M.T.; von dem Borne, P.A.; Boelens, J.; Steel, E.; Kampinga, G.A.; Span, L.F.; Lagrou, K.; Maertens, J.A.; Dingemans, G.J.; et al. Pcr-based detection of Aspergillus fumigatus cyp51a mutations on bronchoalveolar lavage: A multicentre validation of the aspergenius assay in 201 patients with haematological disease suspected for invasive aspergillosis. J. Antimicrob. Chemother. 2016, 71, 3528–3535. [Google Scholar] [CrossRef] [Green Version]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease from the european organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of Mics for Antifungal Agents. Version 10.0, Valid from 2020-02-04. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/AFST_BP_v10.0_200204_updatd_links_200924.pdf (accessed on 4 January 2021).
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Ruhnke, M.; Bohme, A.; Buchheidt, D.; Cornely, O.; Donhuijsen, K.; Einsele, H.; Enzensberger, R.; Hebart, H.; Heussel, C.P.; Horger, M.; et al. Diagnosis of invasive fungal infections in hematology and oncology—Guidelines from the infectious diseases working party in haematology and oncology of the german society for haematology and oncology (agiho). Ann. Oncol. 2012, 23, 823–833. [Google Scholar] [CrossRef]
- Lestrade, P.P.A.; Meis, J.F.; Melchers, W.J.G.; Verweij, P.E. Triazole resistance in Aspergillus fumigatus: Recent insights and challenges for patient management. Clin. Microbiol. Infect. 2019, 25, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Steinmann, J.; Hamprecht, A.; Vehreschild, M.J.; Cornely, O.A.; Buchheidt, D.; Spiess, B.; Koldehoff, M.; Buer, J.; Meis, J.F.; Rath, P.M. Emergence of azole-resistant invasive aspergillosis in hsct recipients in germany. J. Antimicrob. Chemother. 2015, 70, 1522–1526. [Google Scholar] [CrossRef] [Green Version]
- Mikulska, M.; Furfaro, E.; De Carolis, E.; Drago, E.; Pulzato, I.; Borghesi, M.L.; Zappulo, E.; Raiola, A.M.; Grazia, C.D.; Del Bono, V.; et al. Use of Aspergillus fumigatus real-time pcr in bronchoalveolar lavage samples (bal) for diagnosis of invasive aspergillosis, including azole-resistant cases, in high risk haematology patients: The need for a combined use with galactomannan. Med. Mycol. 2019, 57, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Denis, J.; Forouzanfar, F.; Herbrecht, R.; Toussaint, E.; Kessler, R.; Sabou, M.; Candolfi, E.; Letsher-Bru, V. Evaluation of two commercial real-time pcr kits for Aspergillus DNA detection in bronchoalveolar lavage fluid in patients with invasive pulmonary aspergillosis. J. Mol. Diagn. 2018, 20, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Dannaoui, E.; Gabriel, F.; Gaboyard, M.; Lagardere, G.; Audebert, L.; Quesne, G.; Godichaud, S.; Verweij, P.E.; Accoceberry, I.; Bougnoux, M.E. Molecular diagnosis of invasive aspergillosis and detection of azole resistance by a newly commercialized pcr kit. J. Clin. Microbiol. 2017, 55, 3210–3218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelzer, B.W.; Seufert, R.; Koldehoff, M.; Liebregts, T.; Schmidt, D.; Buer, J.; Rath, P.M.; Steinmann, J. Performance of the aspergenius pcr assay for detecting azole resistant Aspergillus fumigatus in bal fluids from allogeneic hsct recipients: A prospective cohort study from essen, west germany. Med. Mycol. 2020, 58, 268–271. [Google Scholar] [CrossRef]
- Chong, G.L.; van de Sande, W.W.; Dingemans, G.J.; Gaajetaan, G.R.; Vonk, A.G.; Hayette, M.P.; van Tegelen, D.W.; Simons, G.F.; Rijnders, B.J. Validation of a new Aspergillus real-time pcr assay for direct detection of Aspergillus and azole resistance of Aspergillus fumigatus on bronchoalveolar lavage fluid. J. Clin. Microbiol. 2015, 53, 868–874. [Google Scholar] [CrossRef] [Green Version]
- Morton, C.O.; White, P.L.; Barnes, R.A.; Klingspor, L.; Cuenca-Estrella, M.; Lagrou, K.; Bretagne, S.; Melchers, W.; Mengoli, C.; Caliendo, A.M.; et al. Determining the analytical specificity of pcr-based assays for the diagnosis of ia: What is Aspergillus? Med. Mycol. 2017, 55, 402–413. [Google Scholar] [CrossRef] [Green Version]
- Buil, J.B.; Zoll, J.; Verweij, P.E.; Melchers, W.J.G. Molecular detection of azole-resistant Aspergillus fumigatus in clinical samples. Front. Microbiol 2018, 9, 515. [Google Scholar] [CrossRef] [Green Version]
- Van der Linden, J.W.; Arendrup, M.C.; Warris, A.; Lagrou, K.; Pelloux, H.; Hauser, P.M.; Chryssanthou, E.; Mellado, E.; Kidd, S.E.; Tortorano, A.M.; et al. Prospective multicenter international surveillance of azole resistance in Aspergillus fumigatus. Emerg. Infect. Dis. 2015, 21, 1041–1044. [Google Scholar] [CrossRef] [PubMed]
- Schauwvlieghe, A.; Vonk, A.G.; Buddingh, E.P.; Hoek, R.A.S.; Dalm, V.A.; Klaassen, C.H.W.; Rijnders, B.J.A. Detection of azole-susceptible and azole-resistant Aspergillus coinfection by cyp51a pcr amplicon melting curve analysis. J. Antimicrob. Chemother. 2017, 72, 3047–3050. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Gender [n (%)] | Male | 67 (72.0) | ||
| Female | 26 (28.0) | |||
| Age [years] | Median | 61 | ||
| Min. | 18 | |||
| Max. | 92 | |||
| Underlying condition [n (%)] | ||||
| Haematological malignancy | 70 (75.3) | |||
| Acute leukemias | ||||
| • AML | 25 (26.9) | |||
| • ALL | 7 (7.5) | |||
| MDS | 8 (8.6) | |||
| Chronic leukemias | ||||
| • CLL | 1 (1.1) | |||
| • MM | 7 (7.5) | |||
| Myeloproliferative diseases | ||||
| • CML | 6 (6.5) | |||
| • MPS | 6 (6.5) | |||
| Lymphoma | ||||
| • HD | 2 (2.2) | |||
| • NHL | 6 (6.5) | |||
| Aplastic anaemia | 2 (2.2) | |||
| Allogenic stem cell transplantation [n (% of haematological malignancy)] | 41 (58.6) | |||
| Solid Cancer | 20 (21.5) | |||
| Lung (SCLC/NSCLC) | 7 (7.5) | |||
| Intestine | 5 (5.4) | |||
| Mouth | 4 (4.3) | |||
| Bladder | 1 (1.1) | |||
| Sarcoma | 1 (1.1) | |||
| Testis | 1 (1.1) | |||
| Breast | 1 (1.1) | |||
| Organ transplantation | 1 (1.1) | |||
| Kidney | 1 (1.1) | |||
| Other | 2 (2.2) | |||
| EORTC/MSG | Probable | Possible | Not categorisable | Total |
| Samples [n] | 11 | 51 | 41 | 103 |
| Patients [n] | 10 | 46 | 37 | 93 |
| Patient ID | MycoGENIE® | Fungiplex® | AsperGenius® | Culture | GM BAL | GM Serum |
|---|---|---|---|---|---|---|
| 3 | pos | pos | pos | A. fumigatus | 5.6 | 0.5 |
| 5 | inhibited | inhibited | neg | neg | 4.4 | nd |
| 11 | pos | neg | neg | neg | 3.6 | neg |
| 12 | neg | neg | neg | neg | 1.8 | 1.3 |
| 12 | pos | pos | pos | neg | 1.0 | neg |
| 19 | pos | pos | pos | neg | 4.7 | neg |
| 31 | pos | pos | pos | A. fumigatus | 4.1 | nd |
| 36 | pos | pos | pos | neg | 4.3 | neg |
| 47 | pos | neg | pos | neg | 2.1 | nd |
| 78 | neg | neg | neg | neg | 3.9 | neg |
| 82 | pos | pos | pos | neg | 3.0 | neg |
| MycoGENIE® | Fungiplex® | AsperGenius® | ||||
|---|---|---|---|---|---|---|
| Af | TR34/L98H | Aspergillus spp. | TR34/TR46 | Af/Aspergillus spp. | TR34/l98H/T289A/Y121F | |
| Probable IPA (N = 11) | 8 | 1 (TR34/L98H) | 6 | 1 (TR34) | 4/3 | 1 (TR34/L89H) |
| Inhibited PCR results | 1 | 1 | 0 | |||
| Possible IPA (N = 51) | 13 | 0 | 7 | 0 | 1/1 | 0 |
| Not categorisable IPA (N = 41) | 9 | 0 | 1 | 0 | 0/1 | 0 |
| Total (N = 103) | 30 | 1 | 14 | 1 | 5/5 | 1 |
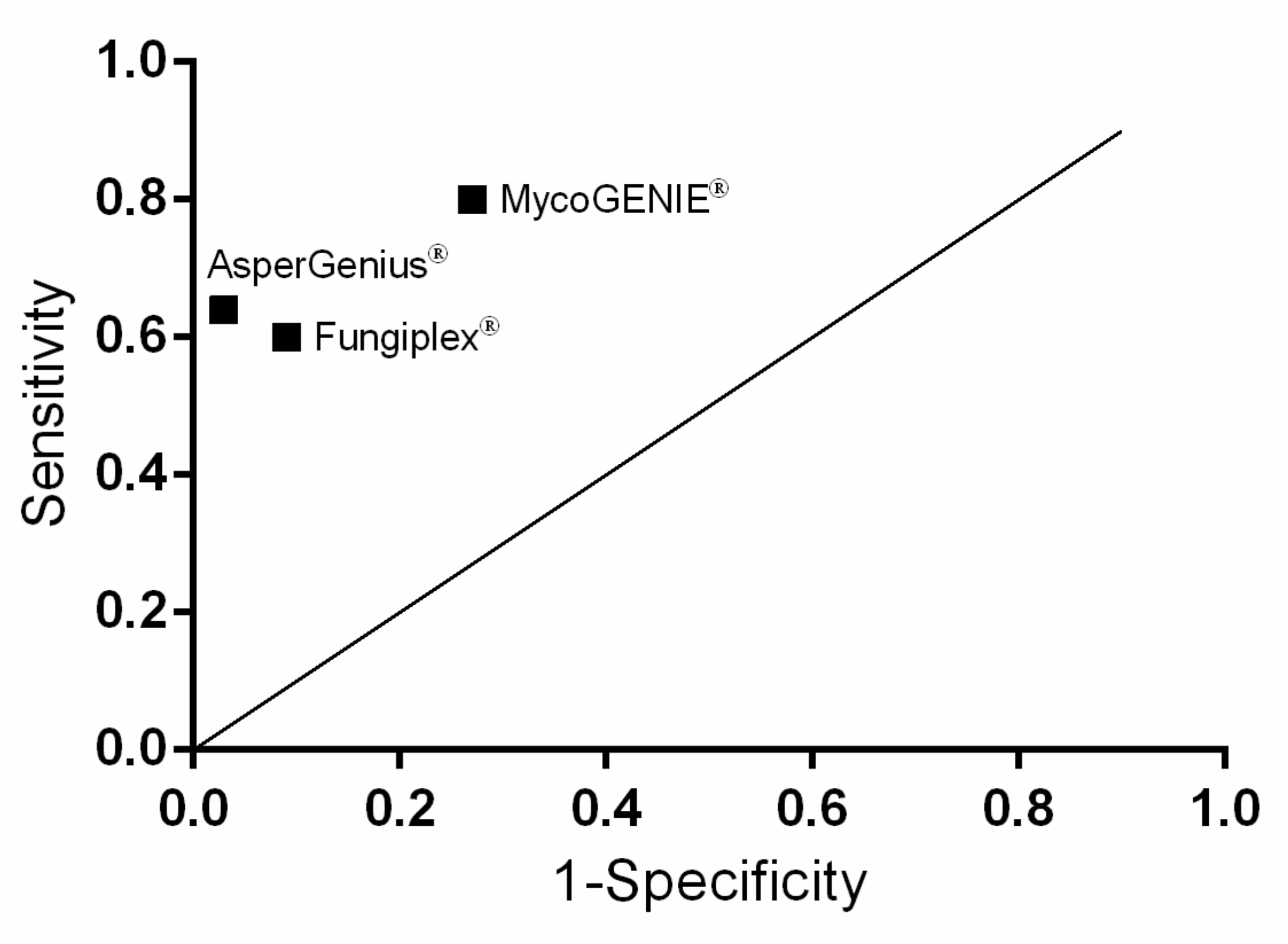
| MycoGENIE® | Fungiplex® | AsperGenius® | |
|---|---|---|---|
| PPV | 0.267 | 0.429 | 0.700 |
| NPV | 0.968 | 0.954 | 0.957 |
| Sensitivity | 0.8 | 0.6 | 0.636 |
| Specificity | 0.732 | 0.912 | 0.967 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scharmann, U.; Kirchhoff, L.; Hain, A.; Buer, J.; Koldehoff, M.; Steinmann, J.; Rath, P.-M. Evaluation of Three Commercial PCR Assays for the Detection of Azole-Resistant Aspergillus fumigatus from Respiratory Samples of Immunocompromised Patients. J. Fungi 2021, 7, 132. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7020132
Scharmann U, Kirchhoff L, Hain A, Buer J, Koldehoff M, Steinmann J, Rath P-M. Evaluation of Three Commercial PCR Assays for the Detection of Azole-Resistant Aspergillus fumigatus from Respiratory Samples of Immunocompromised Patients. Journal of Fungi. 2021; 7(2):132. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7020132
Chicago/Turabian StyleScharmann, Ulrike, Lisa Kirchhoff, Andrea Hain, Jan Buer, Michael Koldehoff, Joerg Steinmann, and Peter-Michael Rath. 2021. "Evaluation of Three Commercial PCR Assays for the Detection of Azole-Resistant Aspergillus fumigatus from Respiratory Samples of Immunocompromised Patients" Journal of Fungi 7, no. 2: 132. https://0-doi-org.brum.beds.ac.uk/10.3390/jof7020132