Measuring Industrial Health Using a Diminished Quality of Life Instrument


Department of Mechanical Engineering, University of Canterbury, Christchurch 8140, Canterbury, New Zealand
*
Author to whom correspondence should be addressed.
Safety 2018, 4(4), 55; https://0-doi-org.brum.beds.ac.uk/10.3390/safety4040055
Submission received: 15 October 2018
/
Revised: 20 November 2018
/
Accepted: 23 November 2018
/
Published: 27 November 2018
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Historically, the focus of industrial health and safety (H&S) has been on safety and accident avoidance with relatively less attention to long-term occupational health other than via health monitoring and surveillance. The difficulty is the multiple overlapping health consequences that are difficult to separate, measure, and attribute to a source. Furthermore, many health problems occur later, not immediately on exposure, and may be cumulative. Consequently, it is difficult to conclusively identify the cause. Workers may lack knowledge of long-term consequences, and thus not use protective systems effectively. Compounding this is the lack of instruments and methodologies to measure exposure to harm. Historically, the existing risk methodologies for calculating safety risk are based on the construct of consequence and likelihood. However, this may not be appropriate for health, especially for the long-term harm, as both the consequence and likelihood may be indeterminate. This paper develops an instrument to measure the health component of workplace H&S. This is achieved by adapting the established World Health Organization Disability Assessment Schedule (WHODAS) quality of life score to workplace health. Specifically, the method is to identify the likelihood of an exposure incident arising (as estimated by engineering technologists and H&S officers), followed by evaluation of the biological harm consequences. Those consequences are then scored by using the WHODAS 12-item inventory. The result is an assessment of the Diminished Quality of Life (DQL) associated with a workplace hazard. This may then be used to manage the minimization of harm, exposure monitoring, and the design of safe systems of work.
1. Introduction
Health and safety (H&S) in industries has now become important in most countries. However, the focus is generally on the safety component, i.e., avoiding accidents [1], rather than long-term health [2]. Existing methodologies for improving safety are primarily based on the risk methodologies [3], normally by reducing the consequence of harm and likelihood of the occurrence. This is widely applied in risk management and related areas [4]. There has been relatively less attention to long-term occupational health, other than via health monitoring and surveillance. The difficulty is the multiple overlapping health consequences that are difficult to separate, measure, and attribute to a source. Furthermore, many health problems are chronic; they may take a period to occur due to cumulative exposure, hence increasing the detection difficulty [5]. Consequently, it is often difficult to conclusively identify the cause of health issues, and too late to change the work practices for that worker. At the time of exposure, workers may lack knowledge of long-term consequences, and thus not use protective systems effectively. Hence, there is a need for instruments and methodologies to measure the risk of harm, especially in the long-term H&S risk in the workplace, before it occurs. Examples of existing methods are the International Organization for Standardization (ISO) 31000 risk management standard [6] with its many derivatives, and a variety of checklists and scoring methods (reviewed below). This paper explores a new way of looking at the subject, and proposes the concept of Diminished Quality of Life (DQL) as a measure of occupational health. An instrument is developed to embody this concept. This may then be used to manage the minimization of harm, exposure monitoring, and the design of safe systems of work. The specific area under examination is the manufacturing industry, and the instrument was developed with this audience in mind. This was selected as representative of a variety of health risks, and employs many people.
2. Literature Review
2.1. Health and Safety in the Manufacturing Industry
Hazards in health and safety are “a source or a situation with a potential for harm in terms of human injury or ill-health, damage to property, damage to the environment, or a combination of these” [7]. Individuals have the right to work in a place with a healthy and safe environment, and this is especially so for people working in manufacturing. Workers in manufacturing are exposed to relatively high risks, such as breathing dust [8,9], contacting toxic or poison products [10], and participating in repetitive activities [11,12]. These hazards can result in injuries and illness [13].
Many health problems are not immediately evident in the response of the human body. Some health problems are affected by the environment [14], e.g., chemical [15,16], light [17], temperature [18], fire [19], and noise [20]. Other health issues are related to physical [11,12] and psychological effects [21]. Some research has focused on ergonomics [22,23] and suggests that poor ergonomic design can have a negative result on a worker’s musculoskeletal system, resulting in muscle fatigue [24], and may even progress into musculoskeletal disease [25]. All these health issues take time to develop.
In contrast, safety accidents normally cause immediate harm to the human body. Safety hazards in manufacturing typically occur when working with tools, machines [26], materials, and transport vehicles in factories [27]. Some research addresses the typical machinery hazards, for example, cutting, crushing, and squashing [28], electrical shock [29], and radiation [30]. Some other safety accidents are caused by environmental hazards, such as trips and falls [31].
Many prevention and recovery methods for health and safety have been designed in the industry [32]. For example, personal protective equipment (PPE) is one of the most popular protection measures in the workplace and has been described as the last means of defense to a hazard [14]. Other research has been focused on developing new methods and designs in protection equipment [33,34], regulations in safety [35], and traffic management in factories [36].
2.2. Risk Management in Health and Safety
Historically, the general focus has been on safety accidents, e.g., machinery accidents [8], and human error [37]. Existing approaches to reduce health and safety risk are primarily focused on risk management methodology [7]. ISO 31000:2009 presents a systemic workflow process for general risk assessment [38], which finds application in many industries [39,40]. Many countries are focused on establishing general principles for protection of individual health and safety at work, for example, the European Union Directive 89/391/EEC [41] and New Zealand Health and Safety Work Act [42]. Research on health risk management is focused on work policy [43], the working environment [44,45], risk prevention [46,47], and risk estimation [48,49]. Some research has been focused on design aids to identify hazards, e.g., inspection checklists [50,51]. Some other approaches are focused exclusively on the risk management methodology [6], such as the continual improvement circle [13], fault tree [52], and safety matrix [53]. Other important developments in health and safety research have been to better address the mental health component of work, e.g., psychosocial risk management [54,55] and mental health [56], and provide means for these factors to be included in the design of safe systems of work. Another area where psychology intersects with health and safety is in the perverse agency concept [57], which seeks to explain why workers take safety risks that may lead to adverse long-term health.
The area of health is weakly handled by the standard approach to risk management. The level of harm associated with health issues is difficult to determine. The actual cause of harm is often difficult to determine and, consequently, this results in a weak estimate in the level of harm [58] and corresponding treatments. Many risk methodologies are based on estimates with consequences [59,60,61], and this is difficult to determine in a chronic health case, as the biological consequences are seldom immediately apparent after exposure.
Quality of Life Scales (QOLS) have been developed in the medical area and used to quantify the effects of disability, age, and health impairment [62]. Several scales and instruments have been developed based on this methodology, e.g., World Health Organization Disability Assessment Schedule (WHODAS) [63], World Health Organization Quality of Life (WHOQOL-BREF) [64] and RAND-36 [65]. These ask questions about the ability of individuals to undertake tasks of daily living [66]. These instruments have also been applied to mental, neurological, and addictive disorders [67].
2.3. Contemporary Issues in Health and Safety Research
The research literature is sparse on methodologies for assessing health risk in the industry. The majority of safety research is focused on risk reduction and accident prevention, rather than biological consequences. Methods to evaluate long-term health effects are especially absent. Self-prevention is difficult because of the challenge of identifying harm associated with the work, see also the concept of perverse agency [57]. The relationship between hazards and consequences are often poorly developed. There has been little emphasis on health in the workplace and, consequently, prevention and treatment are poorly addressed. There are considerable difficulties in associating the source of injuries with a specific workplace because of worker mobility. This is problematic because no one specific employer acts to identify and prevent the injury, especially long term health effects.
3. Methodology
3.1. Purpose
The purpose of this research was to develop an instrument to measure long term health, suitable to be used as a method to manage the risks in the industry.
3.2. Approach
Our approach was to identify the typical hazards in a manufacturing situation. Then, we determined the range of biological consequences for these, with a particular focus on the health issues. An initial hazards list was generated based on the literature [68,69] and health and safety legislation [32]. The specific area under examination for developing the hazards list was based on lathe work in a workshop. This list included items, such as ‘Chemical Exposure’.
The literature concerning the potential biological consequences in the manufacturing industry was also examined from sources, such as the international classification of disease in occupational health (ICD) [69]. A list of biological consequences was developed together with the level of harm. This analysis was related to the particular type of machine operation under examination. Examples of items on this list are ‘Skin Disease, Respiratory System Compromised, Blood Pressure Compromised, etc.’
The next challenge was to link the hazards with the biological consequences. This is a many-to-many correspondence. This link was demonstrated using an ontology, using the “Protégé” software. This expressed the multiple biological consequences associated with the hazards.
Subsequently, we needed a measurement of harm. For this, we adopted the established WHODAS quality of life score. We applied the WHODAS questionnaire to each of the biological consequences to determine the quality of life consequences of such a biological event.
Finally, we needed a framework to link these components into a coherent system that might be used to manage health in the workplace. We found that the conventional risk assessment methodology, with its strict demarcation between consequence and likelihood of the consequence, was unhelpful. Instead, we devised a new framework, which inverts the conventional process. It starts with the likelihood of an exposure incident arising (as estimated by engineering technologists and H&S officers), followed by evaluation of the likelihood of biological harm consequences in the situation (as evaluated by an occupational hygienist). The rest of the process is then mostly automatic, since it uses the previously established WHODAS scores. It results in a quantitative measure of the adverse effects of the work activities on the quality of life of the worker.
We call this the Diminished Quality of Life (DQL) metric. It is not the same as the conventional risk assessment method, and the results must be interpreted differently. See Section 5 for a discussion comparing the methods. We propose a set of thresholds and associated preventative mechanisms.
The DQL method is then applied to a case study.
4. Results
4.1. The Conceptual Model
The dominant paradigm for risk assessment is per the ISO 31000 process that partitions risk into consequence and the likelihood of that consequence. If we are to find better ways of incorporating the long-term health component into the assessment, then it will be necessary to re-conceptualise harm. Consequently, we developed a new conceptual framework, by starting with the biological consequences and working backwards to connect those causally to the hazards that might cause them, and how to represent them.
The hazards were classified by following a review of existing research. The objective was to address hazards for both health and safety, and with a special focus on the hazards that may result in long-term effects. Health and safety incident descriptions were identified for each hazard along with the corresponding biological consequences. The three steps in designing this conceptual model are shown in Figure 1.
The literature review showed that each hazard has potentially multiple effects on a person’s health. For example, chemical exposure can have negative effects on a person’s body not only due to long-term exposure, but also by short term exposure, such as accidental contact. Chemical exposure can cause potential harm to a person’s health by cumulative exposure, for example, skin disease, respiratory system harm, and high or low blood pressure. It also can cause harm to the body by accidental contact, and, consequently, result in damage, such as acid burn.
Health needs to be treated differently to safety. This is because of their unique characteristics. Safety problems are related to accidents, and they can affect a person’s body immediately. By contrast, health problems are more likely to occur after a period of time, or by cumulative exposure with an associated accumulation/incubation period. Furthermore, compared to safety, some health problems can be hard to cure, or cannot be cured, and thus result in chronic issues. Therefore, we propose to classify hazards as either health or safety.
4.2. Health and Safety Hazards List
Based on the existing literature, manufacturing industry hazards are of two types: Environmental hazards and machinery hazards. A list of such health and safety hazards was aggregated from multiple sources, e.g., Health and Safety Executive (HSE), UK [70], WorkSafe NZ [71], and Occupational Safety and Health Administration US (OSHA), US [68].
The environmental hazards in the manufacturing industry are grouped as chemical exposure, dust environment, light, noise, trips and falls, and temperature.
- Light: Activities, such as cutting and welding, can have light issues associated with them. The consequence can be eye strain and short sightedness [79]. The light in welding activities can be very strong, and lack of eye protection can result in blindness.
- Slips, trips, and falls: Slips can be caused by inadequate cleaning, e.g., uncleaned and undried water on surfaces [31]. Trips can be caused by unsecured equipment, e.g., cables [82]. Falls from a height can be caused by loss of function of PPE, e.g., improper footwear [83,84]. The biological consequence of slips, trips, and falls can be bruises, abrasions, sprains, fracture, and even death [85].
- Temperature: Temperature can be uncomfortable in the manufacturing industry, as some products are created by using high or low temperature, e.g., tyres. High temperatures in the work environment can cause circulatory system diseases, e.g., blood pressure problems. Low temperatures can result in muscle fatigue [86].
Machinery hazards in the manufacturing industry include cutting, crushing and squashing, electrical damage, heat and radiation, impact damage, wearing loose cloth, manual heavy loads, doing repetitive work, ventilation, vibration at work, and working in an uncomfortable position.
- Cutting, crushing, and squashing: Manufacturing industry activities can result in cutting and squashing, for example, by operating machines (e.g., a lathe) and using hand tools (e.g., a hammer). The consequence of the associated hazards can be abrasion, small cuts, fracture, amputation [87], and even death [84].
- Entrapment: Loose clothes and working with machines can result in machines jamming or clothing touching hot surfaces (resulting in burns), and slips and falls [85]. This may then result in squashing, amputation, burns, and fractures.
- Impact: Impact damage to a worker can be caused by machines and moving vehicles, such as forklifts [95]. The biological outcome can be bruises, abrasions, sprains, fracture, paralysis, and even death.
- Manual heavy loads: Manual heavy loads in the manufacturing industry can be caused by moving heavy products, and operating machines. A person who suddenly moves a heavy object can get muscle injury, resulting, for example, in back pain [85]. Heavy manual work can result in musculoskeletal damage, such as tendinitis and fibromyalgia.
- Repetitive work: Manufacturing work can be characterised by repetitive activities, such as packaging. Long term exposure to this hazard can result musculoskeletal damage [12].
- Ventilation: Fresh air provides a healthy working environment for workers, and this can be contributed by ventilation [96]. Poor ventilation may result from lack of oxygen, and this can lead to dizziness; it may also lead to an uncomfortable temperature [97,98]. It may contribute to a lack of attention, and hence exposure to other hazards. Welding in confined spaces can be particularly dangerous.
- Uncomfortable working position: Work in an uncomfortable and awkward position may happen when the height of the work surface is not appropriate for someone [12]. It can happen when workers are asked to hold an object at an overhead height [100]. This is an ergonomic issue and may result in muscle strain and musculoskeletal damage [101].
A hazards list was created, combining both environmental hazards and machinery hazards. The various hazards were sorted alphabetically, and are shown in Figure 2. This hazard list is considered to be comprehensive, but can be customised.
4.3. Biological Consequences
Health related biological outcomes in the manufacturing industry were identified based on the international classification of disease in occupational health (ICD) [69] and the international classification of functioning, disability, and health (ICF). These are infectious diseases [69], malignant diseases [102], blood disease [103,104], mental and behavioral disorders [105,106], nervous system disease [107], eye disease [108,109], ear disease [110,111], circulatory system disease [112], respiratory system disease [9], and musculoskeletal system disease [12]. The incubation period can be very long, or may occur by cumulative exposure, hence they can be difficult to detect [113]. Additionally, because of individual physique, the consequence of harm may be different. The consequences of health harm can be influenced by a number of factors, such as gender [114] and age [34,115].
In contrast with health, safety accidents usually cause immediate personal harm to the human body. Transportation equipment, such as conveyors, forklifts, and trucks, may also result in impact damage to workers [27]. The biological outcome of machinery accidents may result in amputation [116], laceration [117], fracture [118], and even death [119]. Other possible harms are cuts and bruises [26]. Some other harms are caused by environmental accidents, such as trips and falls, chemicals [120], and electrical discharges [121]. Some of the environment accidents, like fire, can cause significant damage, even death [122].
Once all potential biological consequences in the manufacturing industry were identified, a health consequences list was generated based on the literature, and this is presented in Figure 3. We propose the consequence is different for different body parts. Hence, for example, amputation was divided into five categories: Arms, fingers, foots, hands, and legs. The various consequences list is presented by level. The application of the framework is limited to the second level. This is because further work is necessary to establish the lower level consequences with confidence.
4.4. Linking the Hazards to the Biological Consequences
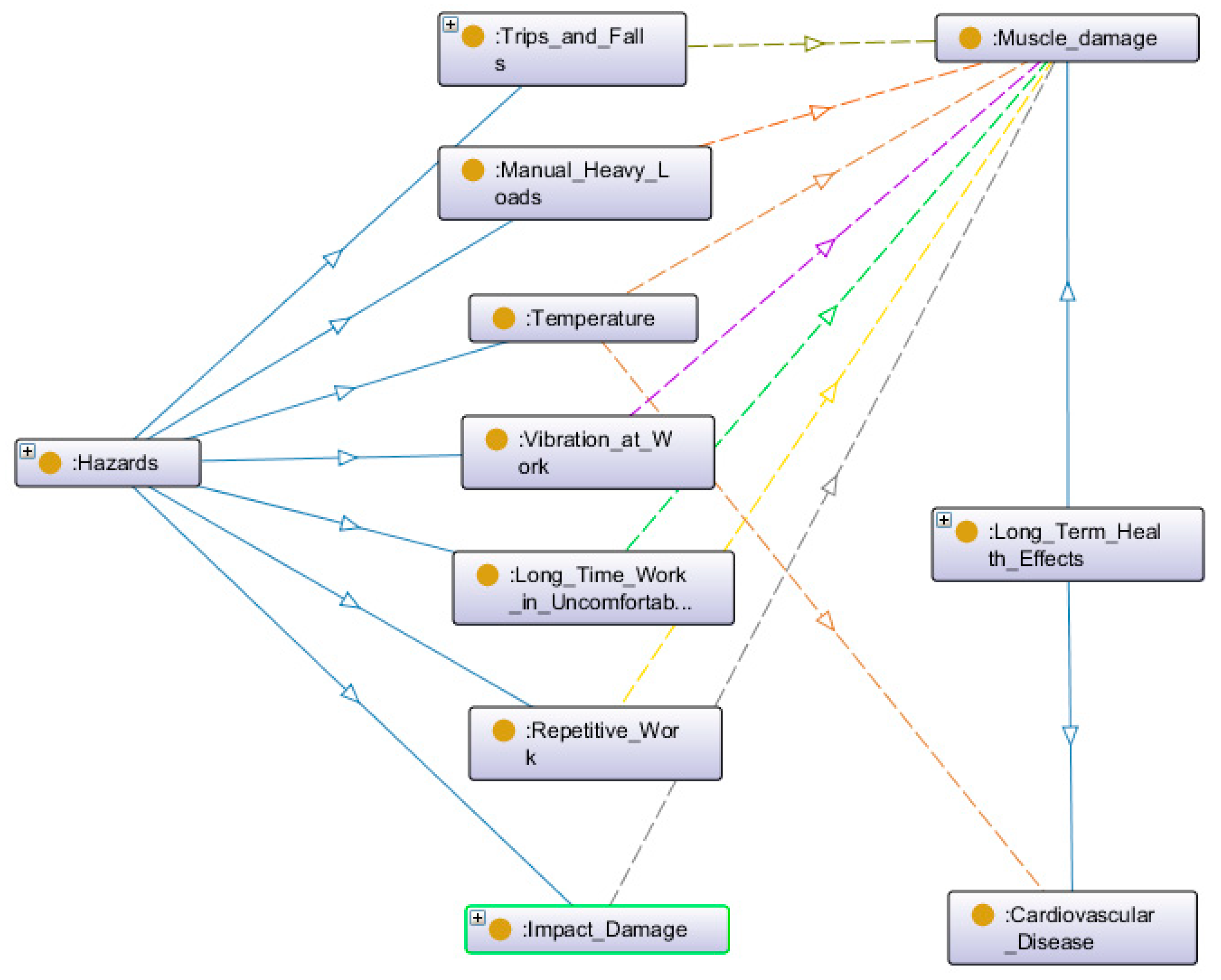
The relationships between hazards and biological consequence were then identified. The relationships are complex. A hazard can result in multiple consequences; a consequence can also be caused by different hazards. Therefore, an information methodology was adopted using an ontology. An ontology describes the relationship and hierarchy between each hazard and the corresponding biological consequence. Additionally, the ontology also focuses on processing and grouping similar consequences into categories. We applied Protégé software to map the lists of hazards and biological consequences. The relationship was then expressed by using mapping analysis. See Figure 4 for an example of the relationship between safety hazards and muscle damage, and cardiovascular disease.
The benefit of using the ontology is that it imposes a systematic process for ensuring the coherence of the model. We found this helped ensure that biological consequences were less likely to be overlooked.
In practice, the way the ontology is expected to work is that the hazards would be identified in the workplace (e.g., ‘chemical exposure’), and the ontology would then automatically identify the associated biological consequences (e.g., skin disease, respiratory system problem, blood pressure problem, eye injury, skin damage). An occupational hygienist would identify the frequency of these consequences arising in the situation. Possibly, the ontology could also support decision-making at this latter step by providing default estimates. In the present work, the ontology is not fully automated in the software, instead the process requires manual input of data via a spreadsheet. Nonetheless, we believe that the overall architecture shown here should be feasible to deploy in the software.
Based on the result of the relationship map, we then developed a register to express the casualty of hazards and biological consequences, see Figure 5 (H: Health; S: Safety.). The casualty was developed based on the existing literature.
4.5. Adoption of a Quality of Life Scale
Level of harm is a key factor in illustrating the negative effects to the human body. However, it is very hard for people to measure the level of harm. The first reason is that some health problems are chronic and this then results in uncertain consequences. Secondly, some health problems may have a long incubation period or affect the human body slowly, hence attribution to a specific time or event may be difficult. Hence, this may then result in uncertain consequences, weak protections, and late treatments. Thirdly, the level of harm is also dependent on a person’s physical ability. Therefore, we propose to use the Quality of Life (QOL) methodology to address the level of harm.
QOL was defined by the World Health Organisation (WHO) in 1948 as “a state of complete physical, mental, and social well-being, and not merely the absence of disease” [123]. There are many QOL measuring instruments developed by different researchers, e.g., the Karnofsky Performance Scale, Sickness Impact Profile, and linear analogue self-assessment (LASA) methods [123]. However, these are focused on medical aspects, and QOL in the manufacturing industry are weakly applied and developed. The WHO also have a quality of life score, the WHO Disability Assessment Schedule (WHODAS 2.0) [63]. We assessed this as more relevant to the situation of industrial harm. There are three different instruments developed by WHODAS, and we decided to use WHODAS 12-item instrument [63]. This is more focused on physical effects than the other two instruments. It was developed to identify how much difficulty a person has in completing the tasks of daily living. The WHODAS questions are shown in Appendix B. Each WHODAS 12-item has a 0 to 4 scale, see Figure 6. The results are percentages, and are used to express the level of physical ability. A higher score indicates higher disability.
4.6. WHODAS Scores for Manufacturing
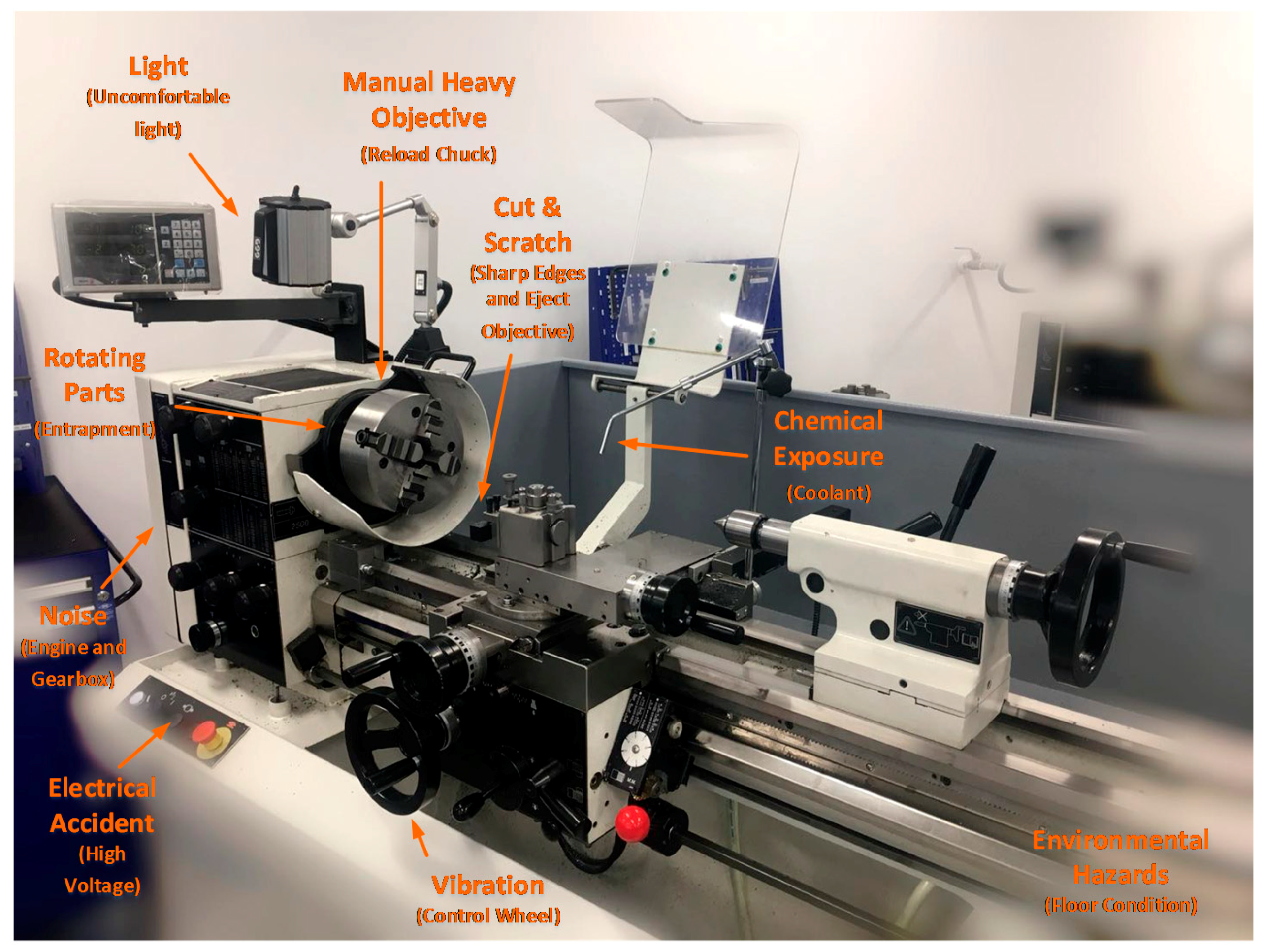
We then applied the WHODAS to a lathe work process, as representative of a common manufacturing industry activity. Potential hazards in operating a lathe were identified, see Figure 7.
In this type of work, workers are exposed to both environmental hazards and machinery hazards. A typical environmental hazard here is hearing loss. Some other typical machinery hazards are cuts by the machine and contact with chemical products (e.g., coolant). The biological consequence for a cut may result in laceration and in extreme cases amputation; and the chemical exposure may potentially result in skin disease. We classified all potential hazards and their biological outcomes, and for each, we determined the WHODAS score. Representative data were used to demonstrate the principle. In this way, we determined the diminished long-term quality of life due to the exposure to say coolant. The WHODAS results for the lathe work are shown in Figure 8, (see also Appendix B).
4.7. Likelihood of an Incident Arising
Probability and frequency can be used to express the likelihood of an incident. Sherman Kent in 1964 presented the idea of Words to Estimate Probability (WEP) [124]. This is widely used in likelihood descriptions. Some popular WEP words are ‘certain’, ‘possible’, and ‘impossible’. This has been applied to risk research, and the likelihood scales were developed using qualitative words [60]. Sherman Kent also proposed that there are differences between “poets” (people preferring to use wordy descriptions in probability) and “mathematicians” (people preferring to use quantitative methods) [125].
We propose to use a quantitative number to express the probability and frequency, instead of qualitative words. This is because we intend to get a numerical result in health and safety risk. A likelihood diagram was developed by the Central Intelligence Agency (CIA) in 2007 [126], see Figure 9. We adapted this, as further described below.
We developed and adopted a scale for the estimated frequency and likelihood by modifying the CIA scale in discussion with engineering technicians. The results are shown in Figure 10.
4.8. Proposed Instrument for Diminished Quality of Life (DQL)
We now present a new concept that integrates all the above. We propose that health effects of industrial activities be measured as ‘diminished quality of life’ (DQL). DQL refers to the extent to which a hazard has a biological consequence that adversely affects a person’s quality of life much later in life. The DQL measurement is quantitative, ranging from 0 to 100. 0 refers to no negative effects on a person’s life, and 100 refers to a very bad outcome, like death.
DQL can be calculated in a four-step process. First is identifying the likelihood of incidents, see Section 4.5.1. Second is identifying the likelihood of a biological consequence. Third is identifying the level of harm: This is done through WHODAS, see Section 4.3.2. Finally, DQL can be calculated using Equation (1):
- ;
- ;
- ;
- ;
- ; and
- .
We propose that DQL can be used for both long term health effects and short term safety accidents. It can potentially also be used in H&S management across other industries, such as construction. However, this paper is focused on DQL in the manufacturing industry. The DQL result of lathe operating has been addressed in Appendix A.
4.9. Evaluation of Severity of Consequences for Quality of Life
After collecting the result of DQL, a method is proposed for workers to determine the overall outcome in health and safety. There is a need to determine thresholds for action, i.e., DQL scores that warrant treatment of the hazard. This is a difficult problem because the long-term biological consequences are poorly understood. Nonetheless, there is a need to develop guidelines for practitioners, so that they can target their finite resources towards appropriate interventions.
To determine the thresholds for action, we analysed the DQL result of lathe operating as representative of a typical material removing (cutting) process in manufacturing. It was noted that 51% of results were between 0-1. We inferred this as an acceptable score, on the basis that the lathe technology is widely used, and this level of residual risk appears to be accepted by industry: there appears to be an acceptance or assumption of risk at this level. We propose that items scoring 1 or lower are low level and may be inconsequential. They are indistinguishable from background risk factors in society generally. This category includes, for the lathe case, e.g., ‘Blood Pressure Problem’, and ‘Respiratory System Problem’. (In different situations, these may be more important.)
It was noted that 29% of DQL results were between 1-3 for the lathe. We propose that a DQL result between 1-3 is a moderate level. This applies in the lathe case where the current safety preventions are considered good. Some of the ‘Musculoskeletal Injury’ risks appear to be in this category for lathe work.
A further 20% of results were between 3-8. We propose a DQL result between 3-8 be considered a high level, and more attention should be given to implementation of treatments. For the lathe work, these were identified as hearing loss and eye injury.
Additionally, the DQL result can, in principle, be over 8, though no such levels were evident for the lathe process. Hence, we propose that a DQL result over 8 is at the extreme high level, and has an unacceptable risk, requiring urgent treatment.
It is acknowledged that these thresholds are subjective. The above strategy is summarized in Figure 11, along with the recommended preventative mechanisms.
There are several advantages in adopting a DQL instrument. Firstly, through analysing the result of DQL, workers can get a better understanding of safety hazards and biological consequences, especially of the long-term health effects. Workers can also identify the DQL level and determine reasonable preventative mechanisms. This results in better recognition of health and safety at work, hence improving prevention and recovery treatments.
4.10. Health and Safety Measuring Instrument- DQL Instrument
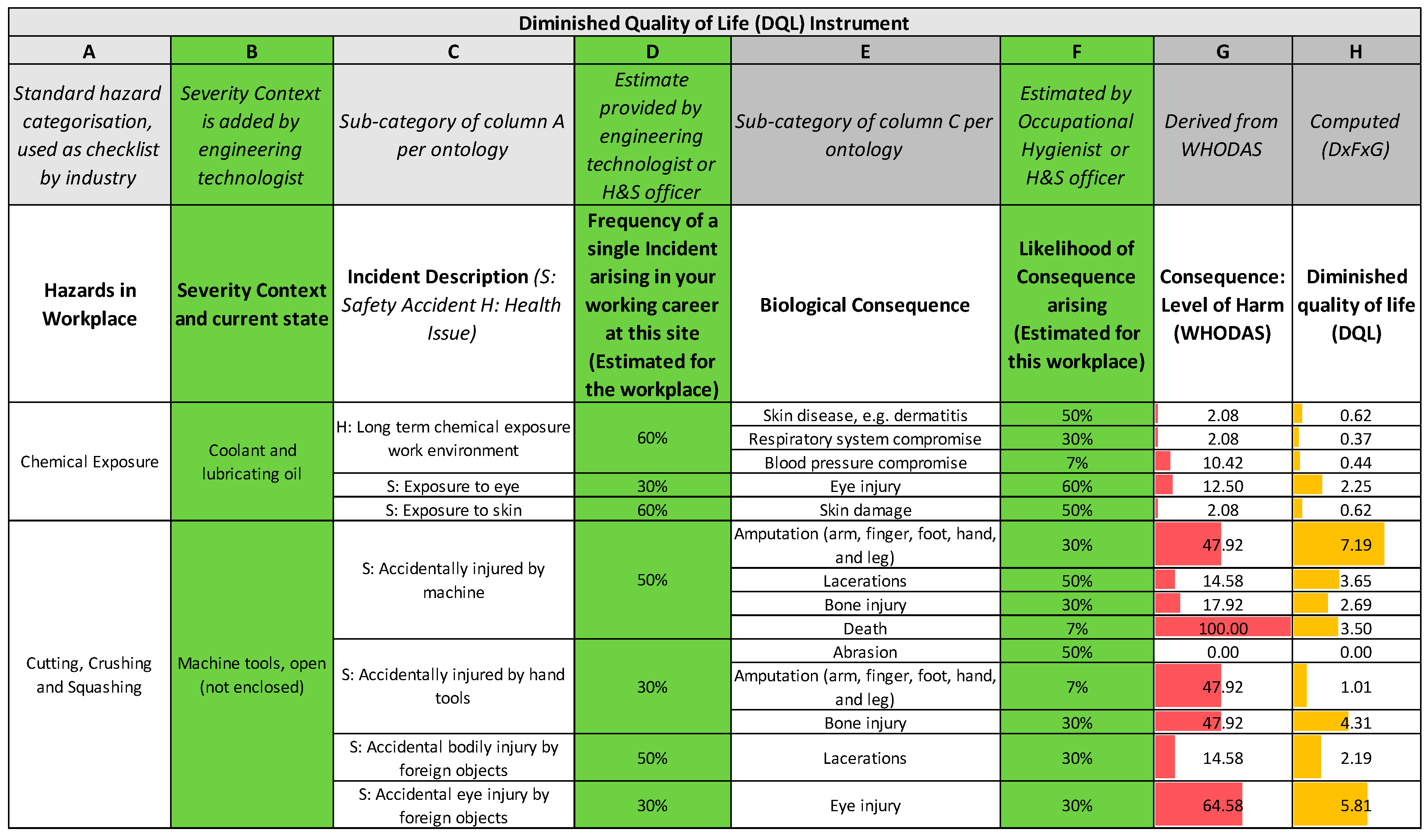
The practical implementation of the DQL instrument may be achieved in a spreadsheet or table, see Figure 12. The instrument consists of eight columns (A to H). Column A describes hazards in the workplace. Columns B is a description of the severity context and the current state. Column C is designed for a specific description of each hazard and relates to how someone could be harmed. Column D is for estimated frequency at work. Column E illustrates the corresponding biological consequence. Column F is the likelihood of the consequence. Column G is the corresponding WHODAS score. Column H is for calculating the DQL result, which is the product of columns D, F, and G.
This instrument is designed to be completed by engineering technologists, H&S officers, and occupational hygienists. Column B and Column D are designed for an engineering technologist to fill in. We assume that engineering technologists have a clear understanding of hazard identification and the frequency thereof. Column F is designed for H&S officers or occupational hygienists to fill in, as they are expected to have a good knowledge of occupational health and safety and also have the ability to present a reasonable likelihood based on analysing the incident reports.
For the full edition of the instrument with an application in lathe work, see Appendix A. An extract is shown in Figure 12. According to results of the application in lathe work, 51% of results were between 0-1 (Low Level), 29% of results were between 1-3 (Moderate Level), 20% of results were between 3-7 (High Level), and 0% of the results were over 8 (Extreme High level). We then found that the high level DQL results were associated with amputation, laceration, eye injury, hearing loss, and death. Clearly, these need to have preventative treatments applied, hence it would be recommended for inclusion in a safe-work plan. Note that some of these outcomes (such as hearing loss) are in the long-term harm category, while others (such as amputation) are in the immediate accident category.
5. Discussion
5.1. Summary
5.1.1. Health Consequences
In summary, the DQL measuring instrument presents a new way to manage health and safety in manufacturing industries, especially the health component. This is achieved by adapting the established WHODAS quality of life score to workplace health. Specifically, the method is to identify the likelihood of an exposure incident arising (as estimated by engineering technologists and H&S officers), followed by evaluation of the biological harm consequences. Those consequences are then scored by using the WHODAS 12-item inventory. The result is an assessment of the Diminished Quality of Life associated with a workplace hazard. This may then be used to manage the minimization of harm, exposure monitoring, and the design of safe systems of work.
In doing this, our premise is that the ‘health’ component of H&S does not always have immediate consequences, but rather effects occur at some indeterminate point in the future. Once the harm does occur, it can often be too late for full cure. We propose that for these hazards, the lack of any immediate harm and the indeterminateness of the consequences contributes to a worker inadvertently assuming a degree of personal risk. Hence, self-prevention is undermined by the worker’s perverse agency [57].
5.1.2. Comparison between Risk Management and DQL Methods
We propose that the existing risk management methodology [6], with its focus on consequence and likelihood, is adequate for safety accidents that have an immediate and tangible consequence, but less so for the long-term harm hazards. The conventional risk assessment process per ISO 31000 encapsulates the concept that the assessment first identifies the consequences, and then the likelihood of those consequences, and then combines them with a product relationship. It is the indeterminate nature of both the consequences and likelihood that limits the risk assessment method in these cases. The product of two uncertain variables further increases the uncertainty in the outcome. We propose that it is intrinsically difficult for industrial risk assessors to make these evaluations reliably. It is difficult for people to anticipate the consequences of the present exposure on their health at some remote point in the future.
Hence, we make the somewhat radical proposal that the risk management methodology is intrinsically unsuited for the harm category of hazards. Instead, we propose that it could be more useful to get people to think about how the hazard might decrease their future quality of life. In doing so, we have borrowed and adapted a validated quality of life instrument used in medicine and rehabilitation. In the DQL methodology, the outcome is measured as a diminished quality of life and is the product of the frequency of exposure, the likelihood of long and short term biological consequences arising, and the WHODAS score for those consequences. While these frequencies and likelihoods are also subjective, the use of the WHODAS provides a measure of consistency, and frames the cognition process in the hazard assessment to be future-focused.
We propose that the two methods are complementary—they achieve different things. In both cases, the results of applying the methodologies are numerical outcomes, which can usefully contribute to health and safety management. The conventional risk management methodology may be ideal for risks that can be reliably quantified, e.g., financial, insurance, technical systems. It is also a simple and useful, even if imprecise, method for assessing accident risk when using simple scales for the two axes. We propose that risk assessment is an important first analysis tool: It causes people to be mindful of the hazards in a situation, and encourages the deployment of preventative treatments. It also provides a means to do due diligence to legal requirements, such as [42]. We suggest that methods based on quality of life, such as the DQL developed here, should be applied as a second stage of evaluation, as part of the continuous improvement process.
5.2. Original Contributions
This work makes several novel contributions. Firstly, it offers a systematic categorisation of health and safety hazards, and specifically addresses long-term health effects, including biological outcomes and their cause. This could potentially help workers better understand occupational health, and help managers provide safer work places.
Secondly, a conceptual framework has been developed around diminished quality of life to present health in a different way to the conventional risk management methodology. This has the potential to enrich the safety field, since health risks are otherwise difficult to analyse and manage. Thirdly, a methodology has been developed to provide a means to quantify DQL in an industrial setting. The DQL instrument not only addresses the accidental harm (environmental and physical) in the manufacturing industry, but also has a special focus on long-term health effects. The biological outcome and its cause are also addressed. The method relies on estimates that are feasible to obtain in the industry, hence it is not difficult to apply.
5.3. Implications for Practitioners
Health issues are under-represented in the safety literature compared to accidents, hence there is a need to develop an instrument to manage both health and safety. It is much easier for industry people to manage safety because an accident tends to have immediate consequences. By contrast, health problems are difficult to identify in the workplace, and some of the health problems require a period to occur or cumulative exposure. The DQL instrument presented here is focused on hazards and their biological consequences in the manufacturing industry. For its implementation, the methodology requires input from a number of industry professionals, such as an engineering technologist, H&S, and occupational hygienist/therapist. In principle, the methodology is applicable to other areas, such as construction, chemical and process engineering, agriculture, etc.
5.4. Limitations of the Work
The work has a number of limitations. One of these is the need for frequency and likelihood data, which is subjective. This is, similar to the subjective estimates needed for consequence and likelihood in the conventional risk assessment method. A second limitation is that we have used representative data to evaluate WHODAS scores. It could be interesting to see the variability between workers (and possibly across different cultures) to the WHODAS scores. A third limitation is that loops of causality have not been included in the work. Some factors (such as lighting and noise) cause fatigue, which may reduce concentration and increase the risk of accidents. A fourth limitation is that determination of an unacceptable threshold for the DQL score was set at >1, but this was our subjective evaluation. It is difficult to see how this score might be objectively determined.
The work was developed with industrial workers in mind, specifically manufacturing engineering. How well the method might apply to other areas has not been determined. Since the WHODAS is a not a sector-specific measure, it is possible that the DQL may be applicable more widely, but this would need to be verified.
5.5. Implications for Further Research
WHODAS scores for different stakeholders could be identified. This could involve developing a survey wherein respondents record the impact on their quality of life for each of the biological consequences identified. It may be necessary to simplify the list of biological consequences to avoid survey fatigue. It would be interesting to see if different groups, e.g., categorized by experience, appraised the consequences differently. A statistical approach may be useful here. A possible concurrent project could be to use qualitative research methods to determine why people made the responses they did. This might involve semi-structured interviews or semantic analysis. The DQL method could also be applied to other industries, such as construction.
Additionally, methodologies for control consequences at work need to be improved, especially in health aspects. Some potential barriers could be, for example, sound isolation (noise), ergonomics work station (manual work activity), and good quality PPE (chemical exposure). Hence, a potential research on efficient treatments for controlling health consequences at work may be valuable. However, some health consequences arise not only from the workplace, but rather individuals’ lifestyle choices (exercise, diet) and existing health conditions that occur outside of their workplace. Mental health needs to be considered as part of risk assessment too. Thus, we suggest there may be other potentially fruitful research to be undertaken on developing methods to provide a more holistic assessment of worker well-being.
6. Conclusions
We have developed a methodology to measure occupational health harm in the workplace. The principles are based on identifying the likelihood of an exposure, and evaluation of the biological consequences using the WHODAS 12-item inventory. This results in an overall metric of risk for the activity, which is called the Diminished Quality of Life score. This may then be included in risk prevention treatments. In this way, a method has been devised to evaluate long-latency harm, cumulative effects, and chronic injuries.
Author Contributions
Z.J. and D.P. created the conceptual model and devised the methodology and categorisations. All authors contributed to the refinement of the model and the writing of the paper. Z.J. and J.P. developed the noise/hearing subsets of the model. D.P. and J.P. provided project direction and supervision.
Funding
This research received no external funding.
Acknowledgments
We thank our colleague, Garry Cotton from University of Canterbury, who provided insight into hazards in the lathe case. In this section you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g. materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A: Application of DQL Instrument in Lathe Work

Appendix B: WHODAS II Application in Lathe Work- Biological Consequences


References
- Tugnoli, A.; Khan, F.; Amyotte, P.; Cozzani, V. Safety assessment in plant layout design using indexing approach: Implementing inherent safety perspective. Part 2-domino hazard index and case study. J. Hazard. Mater. 2008, 160, 110–121. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, R.C. Changing the Workplace Safety Culture; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Rigas, F.; Konstandinidou, M.; Centola, P.; Reggio, G.T. Safety analysis and risk assessment in a new pesticide production line. J. Loss Prev. Process Ind. 2003, 16, 103–109. [Google Scholar] [CrossRef]
- Siu, N. Risk assessment for dynamic systems: An overview. Reliab. Eng. Syst. Saf. 1994, 43, 43–73. [Google Scholar] [CrossRef]
- Whittaker, J.D.; Robinson, T.; Acharya, A.; Singh, D.; Smith, M. Noise-induced hearing loss in small-scale metal industry in Nepal. J. Laryngol. Otol. 2014, 128, 871–880. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. ISO 31000 Risk Management—Principles and Guidelines; International Organization for Standardization: Geneva, Switzerland, 2009. [Google Scholar]
- Standards Australia International Limited; Standards New Zealand. Occupational Health and Safety Management Systems: Specification with Guidance for Use; Standards Australia International: Sydney, Australia, 2001. [Google Scholar]
- Murray, J.; Davies, T.; Rees, D. Occupational lung disease in the South African mining industry: Research and policy implementation. J. Public Health Policy 2011, 32, S65–S79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borton, C. Industrial Dust Diseases. Available online: www.patient.info/doctor/industrial-dust-diseases (accessed on 26 August 2018).
- Li, Y.; Wang, H. Quantitative area risk assessment and safety planning on chemical industry parks. In Proceedings of the 2013 International Conference on Quality, Reliability, Risk, Maintenance, and Safety Engineering, QR2MSE 2013, Emeishan, China, 15–18 July 2013; IEEE Computer Society: Emeishan, China, 2013; pp. 413–418. [Google Scholar]
- National Research Council and the Institute of Medicine. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Bazzini, G.; Capodaglio, E.M.; Mancin, D. The shoe industry and the musculoskeletal system. G. Ital. Med. Lav. Ergon. 2012, 34, 24–28. [Google Scholar] [PubMed]
- Worksafe. Worksafe New Zealand: How to Manage Work Risks. Available online: https://worksafe.govt.nz/managing-health-and-safety/managing-risks/how-to-manage-work-risks/ (accessed on 4 April 2018).
- Chohan, J.S.; Bilga, P.S. Occupational health hazards in small scale steel manufacturing industries: A case study. Int. J. Manuf. Technol. Manag. 2011, 24, 182–192. [Google Scholar] [CrossRef]
- Takriff, M.S.; Bahnuddin, N.N. Integration of inherent safety assessment into process simulation. In Proceedings of the CISAP4—4th International Conference on Safety and Environment in Process Industry, Florence, Italy, 14–17 March 2010; Italian Association of Chemical Engineering—AIDIC: Milan, Italy, 2010; pp. 397–402. [Google Scholar]
- Spellman, F.R.; Bieber, R.M. Occupational Safety and Health Simplified for the Chemical Industry; Government Institutes/Scarecrow Press: Lanham, MD, USA, 2009. [Google Scholar]
- Stave, G.M.; Wald, P.H. Physical and Biological Hazards of the Workplace, 3rd ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2017. [Google Scholar]
- Smith, K. Environmental Hazards: Assessing Risk and Reducing Disaster, 3rd ed.; Routledge: London, UK; New York, NY, USA, 2001. [Google Scholar]
- Spellman, F.R.; Bieber, R.M. Physical Hazard Control: Preventing Injuries in the Workplace; Government Institutes: Lanham, MD, USA, 2011. [Google Scholar]
- Mohammadi, G. Occupational noise pollution and hearing protection in selected industries. Iran. J. Health 2014, 1, 30–35. [Google Scholar]
- Westgaard, R.H.; Winkel, J. Occupational musculoskeletal and mental health: Significance of rationalization and opportunities to create sustainable production systems—A systematic review. Appl. Ergon. 2011, 42, 261–296. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Grant, K.A.; Habes, D.J.; Bertsche, P.K. Ergonomics: Lifting hazards at a cabinet manufacturing company: Evaluation and recommended controls. Appl. Occup. Environ. Hyg. 1997, 12, 253–258. [Google Scholar] [CrossRef]
- Malkin, R.; Hudock, S.D.; Hayden, C.; Lentz, T.J.; Topmiller, J.; Niemeier, R.W. Ergonomics: An assessment of occupational safety and health hazards in selected small businesses manufacturing wood pallets-part 1. Noise and physical hazards. J. Appl. Occup. Environ. Hyg. 2005, 2, D18–D21. [Google Scholar] [CrossRef] [PubMed]
- Thain, P.K.; Hughes, G.T.G.; Mitchell, A.C.S. The effect of repetitive ankle perturbations on muscle reaction time and muscle activity. J. Electromyogr. Kinesiol. 2016, 30, 184–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahram, T.Z.; Karwowski, W. Advances in Physical Ergonomics and Safety; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Worksafe. Worksafe New Zealand: Why Be Safe. Available online: http://manufacturing.worksafe.govt.nz/ (accessed on 14 December 2018).
- Kasahara, M.; Mori, Y. The proposal of the forklift fall accidents prevention method using sliding mode control. In Proceedings of the Society of Instrument and Control Engineers—SICE 2015, Hangzhou, China, 28–30 July 2015; pp. 1326–1331. [Google Scholar]
- Shendell, D.G.; Mizan, S.S.; Marshall, E.G.; Kelly, S.W.; Therkorn, J.H.; Campbell, J.K.; Miller, A.E. Cut-laceration injuries and related career groups in new jersey career, vocational, and technical education courses and programs. Workplace Health Saf. 2012, 60, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Floyd, H.L. A practical guide for applying the hierarchy of controls to electrical hazards. IEEE Trans. Ind. Appl. 2015, 51, 4263–4266. [Google Scholar] [CrossRef]
- Domenech, H. Radiation Safety: Management and Programs; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Amandus, H.; Bell, J.; Tiesman, H.; Biddle, E. The epidemiology of slips, trips, and falls in a helicopter manufacturing plant. Hum. Factors 2012, 54, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-McCleave, R.; Shortall, S. Health and Safety at Work in New Zealand: Know the Law; Thomson Reuters: Wellington, DC, USA, 2016. [Google Scholar]
- Heydaryan, S.; Suaza Bedolla, J.; Belingardi, G. Safety design and development of a human-robot collaboration assembly process in the automotive industry. Appl. Sci. 2018, 8, 344. [Google Scholar] [CrossRef]
- Borowsky, A.; Shinar, D.; Oron-Gilad, T. Age, skill, and hazard perception in driving. Accid. Anal. Prev. 2010, 42, 1240–1249. [Google Scholar] [CrossRef] [PubMed]
- Schröder, I.; Gibson, J.H.; Wayne, N.L. Proceedings of the 2014 university of California center for laboratory safety workshop. J. Chem. Health Saf. 2016, 23, 35–45. [Google Scholar] [CrossRef]
- Worksafe. Worksafe New Zealand: Traffic Management in Manufacturing. Available online: https://worksafe.govt.nz/topic-and-industry/manufacturing/traffic-management-manufacturing/ (accessed on 1 May 2018).
- Reyes, R.M.; de la Riva, J.; Maldonado, A.; Woocay, A. Association between human error and occupational accidents’ contributing factors for hand injuries in the automotive manufacturing industry. Procedia Manuf. 2015, 3, 6498–6504. [Google Scholar] [CrossRef]
- Flaus, J.M. The Risk Management Process (iso31000); John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 53–69. [Google Scholar]
- Oehmen, J.; Ben-Daya, M.; Seering, W.; Al-Salamah, M. Risk management in product design: Current state, conceptual model and future research. In Proceedings of the ASME 2010 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Montreal, QC, Canada, 15–18 August 2010. [Google Scholar]
- Porananond, D.; Thawesaengskulthai, N. Risk management for new product development projects in food industry. J. Eng. 2014, 4, 99–113. [Google Scholar] [CrossRef]
- European Health and Safety Law. Council directive 89/391/EEC of 12 June 1989 on the introduction of measures to encourage improvements in the safety and health of workers at work. Off. J. L 1989, 183, 06. [Google Scholar]
- New Zealand Legislation. Health and Safety at Work Act 2015; Ministry of Business, Innovation and Employment: Wellington, New Zealand, 2015.
- Sato, H.M.D. Management of Health Risks from Environment and Food: Policy and Politics of Health Risk Management in Five Countries: Asbestos and BSE; Springer: New York, NY, USA; Dordrecht, The Netherlands, 2010; Volume 16. [Google Scholar]
- Institute for Work & Health. OHS Vulnerability Measure. Available online: https://www.iwh.on.ca/tools-and-guides/ohs-vulnerability-measure (accessed on 14 September 2018).
- Glas, J.J.P.; Kjaer, E. Draugen HSE-case—Occupational health risk management. In Proceedings of the 1996 3rd International Conference on Health, Safety and Environment in Oil and Gas Exploration and Production. Part 2 (of 2), New Orleans, LA, USA, 9–12 June 1996; Society of Petroleum Engineers (SPE): New Orleans, LA, USA, 1996; pp. 307–313. [Google Scholar]
- Geldart, S. Health and Safety in Today’s Manufacturing Industry; Elsevier Ltd: Amsterdam, The Netherlands, 2014; Volume 8, pp. 177–197. [Google Scholar]
- Foo, S.H.; Wong, K.Y. Occupational safety and health improvement in a cutting tools manufacturing company. In Proceedings of the 26th International Business Information Management Association Conference—Innovation Management and Sustainable Economic Competitive Advantage: From Regional Development to Global Growth, IBIMA 2015, Madrid, Spain, 11–12 November 2015; International Business Information Management Association, IBIMA: Madrid, Spain, 2015; pp. 446–462. [Google Scholar]
- Moatari-Kazerouni, A.; Chinniah, Y.; Agard, B. A proposed occupational health and safety risk estimation tool for manufacturing systems. Int. J. Prod. Res. 2015, 53, 4459–4475. [Google Scholar] [CrossRef]
- Kungwani, P. Risk management-an analytical study. IOSR J. Bus. Manag. 2014, 16, 83–89. [Google Scholar] [CrossRef]
- Canadian Centre for Occupational Health and Safety. Inspection Checklists—Sample Checklist for Manufacturing Facilities. Available online: http://www.ccohs.ca/oshanswers/hsprograms/list_mft.html (accessed on 13 June 2018).
- Lin, Y.H.; Chen, C.Y.; Pan, Y.T. The suitability for the work-related musculoskeletal disorders checklist assessment in the semiconductor industry: A case study. Hum. Factors Ergon. Manuf. Serv. Ind. 2013, 23, 222–229. [Google Scholar] [CrossRef]
- Song, W.; Shi, H.; Li, Q. Application of fault tree knowledge in reasoning of safety risk assessment expert system in petrochemical industry. In Proceedings of the 2009 Pacific-Asia Conference on Knowledge Engineering and Software Engineering, KESE 2009, Shenzhen, China, 19–20 December 2009; IEEE Computer Society: Shenzhen, China, 2009; pp. 167–170. [Google Scholar]
- Inyang, E.; Oyinlola, S. Security matrix in the Niger delta operations. In Proceedings of the 8th SPE International Conference on Health, Safety and Environment in Oil and Gas Exploration and Production 2006, Abu Dhabi, UAE, 2–4 April 2006; Society of Petroleum Engineers: Abu Dhabi, UAE, 2006; pp. 152–161. [Google Scholar]
- Leka, S.; Jain, A.; Widerszal-Bazyl, M.; Żołnierczyk-Zreda, D.; Zwetsloot, G. Developing a standard for psychosocial risk management: Pas 1010. Saf. Sci. 2011, 49, 1047–1057. [Google Scholar] [CrossRef]
- Paul Jimenez, A.D. Assessment of psychosocial risks and mental stress at work: The development of the instrument OrgFit. J. Ergon. 2017, 7, 2. [Google Scholar] [CrossRef]
- Leka, S.; Jain, A.; Iavicoli, S.; Di Tecco, C. An Evaluation of the Policy Context on Psychosocial Risks and Mental Health in the Workplace in the European Union: Achievements, Challenges, and the Future. BioMed Res. Int. 2015, 2015, 213089. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Pons, D.; Pearse, J. Why do workers take safety risks?—A conceptual model for the motivation underpinning perverse agency. Safety 2018, 4, 24. [Google Scholar] [CrossRef]
- Flanagan, J.C. A research approach to improving our quality of life. Am. Psychol. 1978, 33, 138. [Google Scholar] [CrossRef]
- Ruan, X.; Yin, Z.; Chen, A. A review on risk matrix method and its engineering application. J. Tongji Univ. 2013, 41, 381–385. [Google Scholar]
- Zhang, F.-Y.; Li, D.-Y.; Geng, B.; Liu, Z.-L. Risk assessment of contractor support based on improved risk matrix method. J. Shanghai Jiaotong Univ. 2015, 20, 464–467. [Google Scholar] [CrossRef]
- Garg, A.; Murray, S.L. Managing project risks: A generic risk matrix. In Proceedings of the 27th Annual National Conference of the American Society for Engineering Management 2006—Managing Change: Managing People and Technology in a Rapidly Changing World, ASEM 2006, Huntsville, AL, USA, 25–28 October 2006; American Society for Engineering Management: Huntsville, AL, USA, 2006; pp. 176–181. [Google Scholar]
- Burckhardt, C.S.; Anderson, K.L. The quality of life scale (QOLS): Reliability, validity, and utilization. Health Qual. Life Outcomes 2003, 1, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Üstün, T.B. Measuring Health and Disability: Manual for Who Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Costa, C.; Freitas, E.; Mendonca, L.; Alem, M.; Coury, H. Work ability and quality of life of Brazilian industrial workers. Cienc. Saude Coletiva 2012, 17, 1635–1642. [Google Scholar] [CrossRef]
- Salo, P.; Ylönen-Käyrä, N.; Häkkinen, A.; Kautiainen, H.; Mälkiä, E.; Ylinen, J. Effects of long-term home-based exercise on health-related quality of life in patients with chronic neck pain: A randomized study with a 1-year follow-up. Disabil. Rehabil. 2012, 34, 1971–1977. [Google Scholar] [CrossRef] [PubMed]
- Roja, Z.; Kalkis, V.; Roja, I.; Kalkis, H. The effects of a medical hypnotherapy on clothing industry employees suffering from chronic pain. J. Occup. Med. Toxicol. 2013, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, T.-Y.; Yen, C.-F.; Chou, C.-H.; Lin, J.-D.; Hwang, A.-W.; Liao, H.-F.; Chi, W.-C. Development of traditional Chinese version of world health organization disability assessment schedule 2.0 36—item (WHODAS 2.0) in Taiwan: Validity and reliability analyses. Res. Dev. Disabil. 2014, 35, 2812–2820. [Google Scholar] [CrossRef] [PubMed]
- Occupational Safety and Health Administration. United States Department of Labor: Hazard Circle Chart. Available online: https://www.osha.gov/dte/grant_materials/fy10/sh-20839-10.html (accessed on 26 June 2018).
- World Health Organization. Strengthening of health surveillance of working populations: The use of international statistical classification of diseases (ICD-10) in occupational health. In Proceedings of the WHO Meeting, Geneva, Switzerland, 8–10 July 1998. [Google Scholar]
- Health and Safety Executive. Health and Safety in Engineering Workshops; Health and Safety Executive: Bootle, UK, 1999.
- Worksafe. Worksafe New Zealand: Safe Use of Machinery. Available online: https://worksafe.govt.nz/topic-and-industry/manufacturing/safe-use-of-machinery/ (accessed on 13 June 2018).
- Chou, T.-C.; Wang, P.-C.; Wu, J.-D.; Sheu, S.-C. Chromium-induced skin damage among Taiwanese cement workers. Toxicol. Ind. Health 2016, 32, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Janicijevic-Petrovic, M.A.; Sarenac-Vulovic, T.S.; Janicijevic, K.M.; Vujic, D.I.; Vulovic, D.D. Chemical eye injuries. Acta Medica Salin. 2013, 42, 27. [Google Scholar] [CrossRef]
- Gube, M.; Ebel, J.; Brand, P.; Göen, T.; Holzinger, K.; Reisgen, U.; Kraus, T. Biological effect markers in exhaled breath condensate and biomonitoring in welders: Impact of smoking and protection equipment. Int. Arch. Occup. Environ. Health 2010, 83, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Jensen, O.C.; Sørensen, J.F.L.; Canals, M.L.; Hu, Y.P.; Nikolic, N.; Bloor, M. Subjective assessments of safety, exposure to chemicals and use of personal protection equipment in seafaring. Occup. Med. 2005, 55, 454–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cummings, K.J.; Boylstein, R.J.; Stanton, M.L.; Piacitelli, C.A.; Edwards, N.T.; LeBouf, R.F.; Kreiss, K. Respiratory symptoms and lung function abnormalities related to work at a flavouring manufacturing facility. Occup. Environ. Med. 2014, 71, 549–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Materna, B.; Quint, J.; Prudhomme, J.; Payne, S.; Harrison, R.; Welsh, L.; Kochie, M.; Howard, K.; Kreiss, K.; Kanwal, R.; et al. Prevention. Fixed obstructive lung disease among workers in the flavor-manufacturing industry—California, 2004–2007. Morb. Mortal. Wkly. Rep. 2007, 56, 389–393. [Google Scholar]
- Wade, J. Breath of Fresh Air in Dust Control; Reed Business Information Ltd.: South Melbourne, Australia, 2006; p. 20. [Google Scholar]
- Walls, H.L.; Walls, K.L.; Benke, G. Eye disease resulting from increased use of fluorescent lighting as a climate change mitigation strategy. Am. J. Public Health 2011, 101, 2222–2225. [Google Scholar] [CrossRef] [PubMed]
- Tahir, N.; Aljunid, S.M.; Hashim, J.H. Occupational noise exposure in manufacturing industries in Malaysia. BMC Public Health 2014, 14 (Suppl. 1), O17. [Google Scholar] [CrossRef]
- Wang, Z.; Liang, J.; Rong, X.; Zhou, H.; Duan, C.; Du, W.; Liu, Y. Noise hazard and hearing loss in workers in automotive component manufacturing industry in Guangzhou, china. Chin. J. Ind. Hyg. Occup. Dis. 2015, 33, 906–909. [Google Scholar]
- Swaen, G.; Burns, C.J.; Collins, J.J.; Bodner, K.M.; Dizor, J.F.; Craun, B.A.; Bonner, E.M. Slips, trips and falls at a chemical manufacturing company. Occup. Med. 2014, 64, 120–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, S.K.; Lombardi, D.A.; Chang, W.-R.; Courtney, T.K.; Brennan, M.J. A matched case-control study of circumstances of occupational same-level falls and risk of wrist, ankle and hip fracture in women over 45 years of age. Ergonomics 2008, 51, 1960–1972. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.; Kumar, S. Occupational injuries and illnesses in the plywood manufacturing industry group 1997–2002: A descriptive study of workers compensation board claims. Int. J. Ind. Ergon. 2005, 35, 183–196. [Google Scholar] [CrossRef]
- Koepp, G.A.; Snedden, B.J.; Levine, J.A. Workplace slip, trip and fall injuries and obesity. Ergonomics 2015, 58, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N.; Elovainio, M.; de Nardis, I.; Heponiemi, T.; Bergamaschi, A. Environmental discomfort and musculoskeletal disorders. Occup. Med. 2011, 61, 196–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Largo, T.W.; Rosenman, K.D. Surveillance of work-related amputations in Michigan using multiple data sources: Results for 2006–2012. Occup. Environ. Med. 2015, 72, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Kadavil, H.P.; Palmer, J. Electrical hazards: Causes and prevention. Anaesth. Intensiv. Care Med. 2013, 14, 428–430. [Google Scholar] [CrossRef]
- Stokes, A.D.; Sweeting, D.K. Electric arcing burn hazards. IEEE Trans. Ind. Appl. 2006, 42, 134–141. [Google Scholar] [CrossRef]
- Hisey, D.A.S. Welding electrical hazards: An update. Weld. World 2014, 58, 171–191. [Google Scholar] [CrossRef]
- Cheremisinoff, N.P. Dust Explosion and Fire Prevention Handbook: A Guide to Good Industry Practices; Scrivener Publishing/Wiley: Hoboken, NJ, USA, 2014. [Google Scholar]
- International Organization for Standardization. Fire Safety Engineering—Requirements Governing Algebraic Equations—Part 7: Radiation Heat Flux Received from an Open Pool Fire; International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- Atlas, R.M.; Maloy, S.R. One Health: People, Animals, and the Environment, 1st ed.; ASM Press: Washington, DC, USA, 2014. [Google Scholar]
- McCaughey, C. Q fever: A tough zoonosis. Vet. Rec. 2014, 175, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S. Traffic accidents during work and work commuting. Int. J. Ind. Ergon. 2000, 26, 75–85. [Google Scholar] [CrossRef]
- Burgess, W.A.; Ellenbecker, M.J.; Treitman, R.D.; Ebrary, I. Ventilation for Control of the Work Environment, 2nd ed.; Wiley-Interscience: Hoboken, NJ, USA, 2004. [Google Scholar]
- Health and Safety Executive. General Ventilation in the Workplace: Guidance for Employers; Health and Safety Executive: Bootle, UK, 2000. [Google Scholar]
- Occupational Safety & Health Administration. Ventilation of welding work areas. Weld. J. 2013, 92, 94. [Google Scholar]
- Mansfield, N.J. Human Response to Vibration; CRC Press: Boca Raton, FL, USA, 2005. [Google Scholar]
- Gomes De Lima, J.F.; Colaço, G.; Da Silva, R.; Masculo, F. Members of the human body prone to musculoskeletal damages: A comparison between the sector of transportation and footwears production. Work 2012, 41, 1582–1587. [Google Scholar] [PubMed]
- Hadler, N.M. Occupational Musculoskeletal Disorders, 3rd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- World Health Organization. Environmental and Occupational Cancers. Available online: http://www.who.int/mediacentre/factsheets/fs350/en/ (accessed on 27 November 2018).
- Zhang, M.; Jian, L.; Bin, P.; Xing, M.; Lou, J.; Cong, L.; Zou, H. Workplace exposure to nanoparticles from gas metal arc welding process. J. Nanopart. Res. 2013, 15, 2016. [Google Scholar] [CrossRef]
- World Health Organization. Ionizing Radiation, Health Effects and Protective Measures. Available online: http://www.who.int/mediacentre/factsheets/fs371/en/ (accessed on 27 November 2018).
- World Health Organization. Mental Health: Strengthening Our Response. Available online: http://www.who.int/mediacentre/factsheets/fs220/en/ (accessed on 27 November 2018).
- Dutta, S.; Kar, N.; Thirthalli, J.; Nair, S. Prevalence and risk factors of psychiatric disorders in an industrial population in India. Indian J. Psychiatry 2007, 49, 103. [Google Scholar] [PubMed] [Green Version]
- Donaghy, M. Brain’s Diseases of the Nervous System, 12th ed.; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Centers for Disease Control and Prevention. Eye Safety. Available online: http://www.cdc.gov/niosh/topics/eye/ (accessed on 25 July 2018).
- Schulte, P.A.; Ahlers, H.W.; Jackson, L.L.; Malit, B.D. Current Intelligence Bulletin 59: Contact Lens Use in a Chemical Environment; Department of Health and Human Services: Washington, DC, USA, 2005.
- Nanda, S.K.; Tripathy, D.P.; Patra, S.K. A sugeno fuzzy model for noise induced hearing loss in the mining industry. Noise Vib. Worldw. 2008, 39, 25–36. [Google Scholar] [CrossRef]
- Kovalchik, P.G.; Matetic, R.J.; Smith, A.K.; Bealko, S.B. Application of prevention through design for hearing loss in the mining industry. J. Saf. Res. 2008, 39, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Sinkiewicz, W.; Dziedziczko, A.; Hoffmann, A. Evaluation of the circulatory system in workers in the cellulose-paper industry. Med. Pr. 1998, 49, 147–156. [Google Scholar] [PubMed]
- Cherrie, J.W.; Howie, R.; Semple, S.; Ashton, I. Monitoring for Health Hazards at Work, 4th ed.; Wiley-Blackwell: Malden, MA, USA, 2010. [Google Scholar]
- Cottini, E. Is your job bad for your health? Explaining differences in health at work across gender. Int. J. Manpow. 2012, 33, 301–321. [Google Scholar] [CrossRef]
- Park, J.; Kim, S.G.; Park, J.-S.; Han, B.; Kim, K.B.; Kim, Y. Hazards and health problems in occupations dominated by aged workers in south Korea. Ann. Occup. Environ. Med. 2017, 29, 27. [Google Scholar] [CrossRef] [PubMed]
- Safety Management Clinic. Protecting workers from amputations. Saf. Compliance Lett. 2012, 7. [Google Scholar]
- Lander, L.; Sorock, G.S.; Stentz, T.L.; Eisen, E.A.; Mittleman, M.; Hauser, R.; Perry, M.J. A case-crossover study of occupational laceration injuries in pork processing: Methods and preliminary findings. Occup. Environ. Med. 2010, 67, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.S.; Biswas, R.S.; Nambiar, A.M.; Syamlal, G.; Velilla, A.M.; Ducatman, A.M.; Doyle, E.J. Incidence and risk of work-related fracture injuries: Experience of a state-managed workers’ compensation system. J. Occup. Environ. Med. 2001, 43, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Jeong, B.Y. Occupational injuries and deaths in domestic waste collecting process. Hum. Factors Ergon. Manuf. Serv. Ind. 2016, 26, 608–614. [Google Scholar] [CrossRef]
- Ratnasingam, J.; Natthondan, V.; Ioras, F.; McNulty, T. Dust, noise and chemical solvents exposure of workers in the wooden furniture industry in south East Asia. J. Appl. Sci. 2010, 10, 1413–1420. [Google Scholar]
- El-Sharkawi, M.A. Electric Safety: Practice and Standards; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Tamoli, M. Tazreen factory fire: An accident or sheer negligence? Prabandhan 2016, 9, 28–44. [Google Scholar] [CrossRef]
- Fayers, P.M.; Machin, D. Quality of Life: The Assessment, Analysis, and Reporting of Patient-Reported Outcomes, 3rd ed.; John Wiley & Sons Inc.: Chichester, UK; Hoboken, NJ, USA, 2016. [Google Scholar]
- Kent, S.; Project, M. Strategic Intelligence for American World Policy; Princeton University Press: Princeton, NJ, USA, 1966. [Google Scholar]
- Davis, J. Sherman Kent and the Profession of Intelligence Analysis. Available online: https://www.cia.gov/library/kent-center-occasional-papers/vol1no5.htm (accessed on 12 June 2018).
- Center for Intelligence Analysis. Words of Estimative Probability. Available online: https://www.cia.gov/library/center-for-the-study-of-intelligence/csi-publications/books-and-monographs/sherman-kent-and-the-board-of-national-estimates-collected-essays/6words.html (accessed on 12 June 2018).
Figure 1.
The three steps in designing the conceptualization model.

Figure 2.
Manufacturing industry hazards list. Applicable hazards are identified as illustrated in Figure 5, see Section 4.3.1. This part of the analysis can be addressed by using a conventional risk management process.
Figure 2.
Manufacturing industry hazards list. Applicable hazards are identified as illustrated in Figure 5, see Section 4.3.1. This part of the analysis can be addressed by using a conventional risk management process.
| Manufacturing Industry Hazards List: |
|---|
| 1. Chemical Exposure |
| 2. Cutting, Crushing, and Squashing |
| 3. Dust |
| 4. Electrical Damage |
| 5. Entrapment |
| 6. Heat and Radiation |
| 7. Impact Damage |
| 8. Infection |
| 9. Lighting |
| 10. Manual Heavy Loads |
| 11. Noise |
| 12. Repetitive Work |
| 13. Slips, Trips, and Falls |
| 14. Temperature |
| 15. Uncomfortable Work Position |
| 16. Ventilation |
| 17. Vibration at Work |
Figure 3.
Biological consequences.
| Biological Consequences: |
|---|
| 1. Abrasions and Lacerations |
| a. Abrasions |
| i. Minor Abrasion |
| ii. Extensive or Deep Lacerations Leading to Scarring |
| b. Lacerations |
| i. Minor Laceration |
| ii. Soft Tissue Damage (Surgical Intervention) |
| iii. De-gloving Accident |
| 2. Amputation |
| a. Amputation of Arm |
| b. Amputation of Finger |
| c. Amputation of Foot |
| d. Amputation of Hand |
| e. Amputation of Leg |
| 3. Blood Pressure Compromised |
| a. High Blood Pressure |
| b. Low Blood Pressure |
| 4. Cardiovascular Disease |
| a. Heart Disease |
| b. Blood Vessels Disease |
| 5. Death |
| 6. Eye injury |
| a. Foreign Object in Eye |
| b. Damage to Cornea |
| c. Partial Loss of Sight |
| d. Loss of One Eye |
| e. Loss of Both Eyes |
| f. Eye Fatigue |
| 7. Hearing Loss |
| a. Auditory Processing Disorders |
| b. Conductive Hearing Loss |
| c. Sensorineural Hearing Loss |
| d. Mixed Hearing Loss |
| 8. Infections |
| a. Wound Infection |
| b. Animal Infectious Diseases |
| 9. Musculoskeletal Injury |
| a. Bruise to Soft Tissue |
| i. Localised - Minor |
| ii. Severe |
| iii. Organ Bruising |
| b. Muscle Damage |
| i. Temporary Fatigue |
| ii. Muscle Micro Tear |
| c. Tendon and Ligament Injury |
| i. Sprain |
| ii. Dislocation |
| iii. Tearing |
| iv. Detachment |
| d. Bone Injury |
| i. Incomplete Crack |
| ii. Fracture of Digits |
| iii. Fracture Requiring Splinting |
| iv. Fracture Requiring Cast |
| v. Fracture Requiring Surgical Setting |
| vi. Fracture Requiring Surgical Fixation (Metal Plates) |
| e. Head Injury |
| i. Concussion |
| ii. Bone Damage |
| iii. Neurological Damage |
| f. Musculoskeletal Disease |
| 10. Paralysis |
| a. Monoplegia |
| b. Hemiplegia |
| c. Paraplegia |
| d. Quadriplegia |
| 11. Respiratory System Compromised |
| 12. Skin Harm |
| a. Skin Damage |
| i. Acid Burn |
| ii. Physical Wound |
| b. Skin Disease |
| i. Dermatitis |
| ii. Acne |
Figure 4.
Relationship between safety hazards and biological consequences in Protégé.
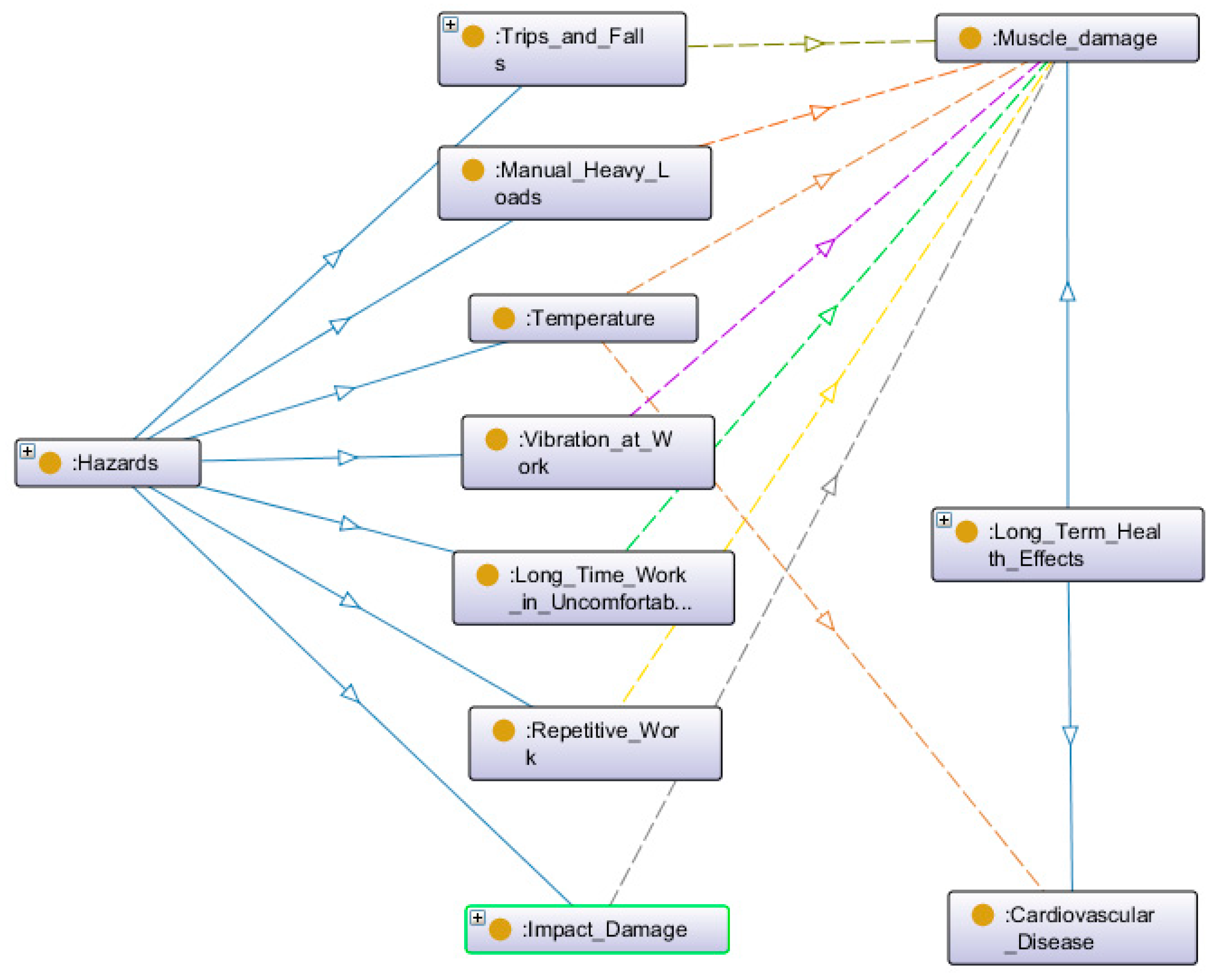
Figure 5.
Hazards and biological consequences.
| Hazards in Workplace | Incident Description(S: Safety Accident H: Health Issue) | Biological Consequence |
| Chemical Exposure | H: Long term chemical exposure in work environment | Skin disease, e.g., dermatitis |
| Respiratory system compromised | ||
| Blood pressure compromised | ||
| S: Exposure to eye | Eye injury | |
| S: Exposure to skin | Skin damage | |
| Cutting, Crushing, and Squashing | S: Accidentally injured by machine | Amputation (arm, finger, foot, hand, and leg) |
| Lacerations | ||
| Bone injury | ||
| Death | ||
| S: Accidentally injured by hand tools | Abrasion | |
| Amputation (arm, finger, foot, hand, and leg) | ||
| Bone injury | ||
| S: Accidental bodily injury by foreign objects | Lacerations | |
| S: Accidental eye injury by foreign objects | Eye injury | |
| Dust | H: Dust in lungs | Respiratory system compromise |
| Electrical Accident | S: Electrical burn | Skin damage |
| H: Electrical shock | Skin damage | |
| Paralysis | ||
| Death | ||
| Heat and Radiation | S: Burn via fire, hot object, hot liquid, hot vapour | Eye injury |
| Skin damage | ||
| Impact Damage | S: Workers hit by machine, forklift, and other objects | Musculoskeletal injury |
| Abrasion | ||
| Bone injury | ||
| Lacerations | ||
| Skin damage | ||
| Paralysis | ||
| Death | ||
| Lighting | H: Uncomfortable or strange light in workplace | Eye fatigue |
| Entrapment | S: Get caught by machine | Amputation (arm, finger, foot, hand, and leg) |
| S: Touch hot surface | Skin damage | |
| S: Trips, slips and falls | Abrasion | |
| Musculoskeletal injury | ||
| Lacerations | ||
| Eye Injury | ||
| Bone injury | ||
| Paralysis | ||
| Death | ||
| Manual Heavy Loads and Repetitive Work | H: Moving heavy tools, machines, and other objectives; or long-time repetitive work, e.g., packaging | Muscle damage, tendon, and ligament injury |
| Noise | H: Caused by machine operating | Hearing loss |
| Temperature | H: Uncomfortable temperature Environment | Circulatory system diseases |
| Musculoskeletal injury | ||
| Ventilation | H: Uncirculated air | Respiratory system compromise |
| Vibration | H: Long term vibration exposure | Muscle damage, tendon, and ligament injury |
| Uncomfortable Working Position | H: Long term work in uncomfortable position | Muscle damage, tendon, and ligament injury |
Figure 6.
WHODAS scales.
| When using WHODAS the following numbers are assigned to the response |
| 0 = No Difficulty |
| 1 = Mild Difficulty |
| 2 = Moderate Difficulty |
| 3 = Severe Difficulty |
| 4 = Extreme Difficulty or Cannot Do |
Figure 7.
Lathe machine hazards.
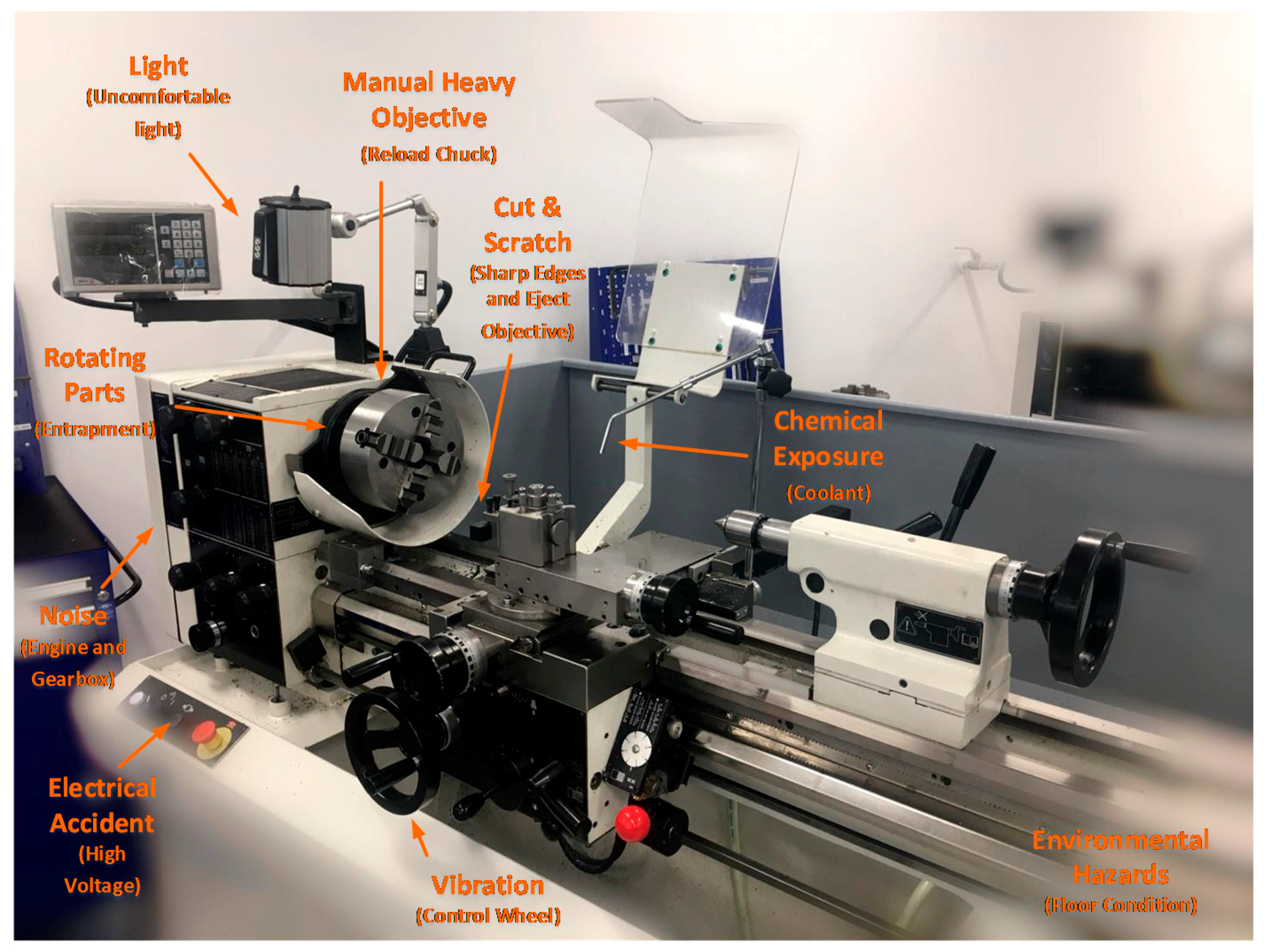
Figure 8.
WHODAS score for lathe work.
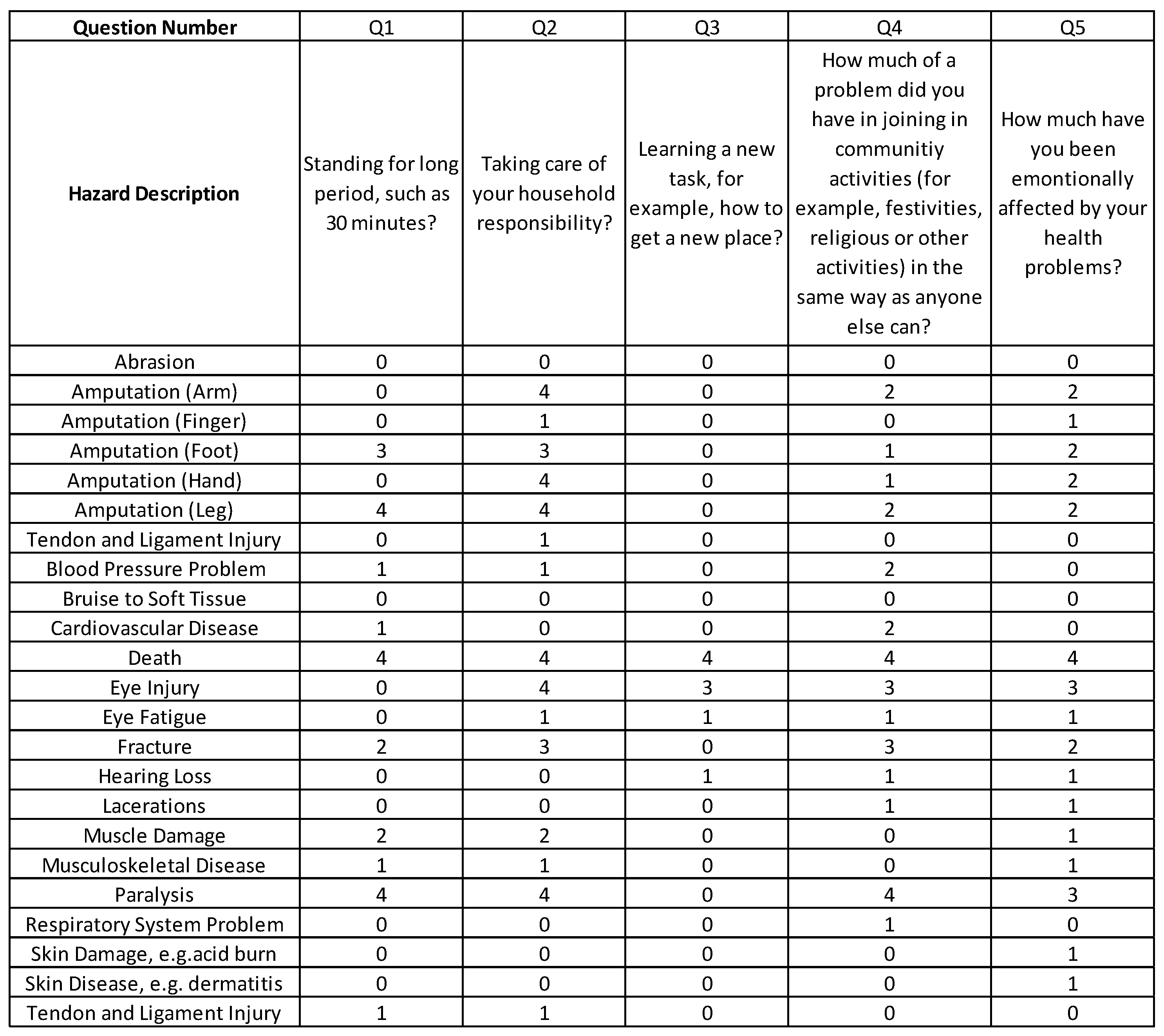
Figure 9.
Likelihood scale (adapted from CIA, US).
| Qualitative Description | Numerical Probability |
| Certain | 100% |
| Almost Certain | 93% (Give or Take About 6%) |
| Probable | 75% (Give or Take About 12%) |
| Chances About Even | 50% (Give or Take About 10%) |
| Probably Not | 30% (Give or Take About 10%) |
| Almost Certainly Not | 7% (Give or Take About 5%) |
| Impossible | 0% |
Figure 10.
WEP-likelihood scale diagram.
| Descriptor | Description of frequency | Probability |
| Almost Certain | Annual occurrence in the situation | 90% |
| Likely | Has Occurrence several times in a person’s career life | 60% |
| Possible | Might occur once somewhere from time to time | 50% |
| Unlikely | Event does occur somewhere from time | 30% |
| Rare | Heard of something like this happened | 7% |
| Almost Incredible | Theoretically possible but not expected to occur | 1% |
Figure 11.
DQL result.
| DQL Result | DQL Level | Preventative Mechanisms |
| 0-1 | Low | No further treatments required. |
| 1-3 | Moderate | Implement treatment in a reasonable time period. |
| 3-8 | High | Implementation of treatment required. |
| Over 8 | Extreme High | Unacceptable risk. Need urgent treatment. |
Figure 12.
DQL health and safety measuring instrument applied to lathe work.

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ji, Z.; Pons, D.; Pearse, J. Measuring Industrial Health Using a Diminished Quality of Life Instrument. Safety 2018, 4, 55. https://0-doi-org.brum.beds.ac.uk/10.3390/safety4040055
AMA Style
Ji Z, Pons D, Pearse J. Measuring Industrial Health Using a Diminished Quality of Life Instrument. Safety. 2018; 4(4):55. https://0-doi-org.brum.beds.ac.uk/10.3390/safety4040055
Chicago/Turabian StyleJi, Zuzhen, Dirk Pons, and John Pearse. 2018. "Measuring Industrial Health Using a Diminished Quality of Life Instrument" Safety 4, no. 4: 55. https://0-doi-org.brum.beds.ac.uk/10.3390/safety4040055
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.