The Global Rise and the Complexity of Sesame Allergy: Prime Time to Regulate Sesame in the United States of America?

Food Allergy and Immunology Laboratory, Department of Food Science and Human Nutrition, Michigan State University, East Lansing, MI 48824, USA
*
Author to whom correspondence should be addressed.
Allergies 2021, 1(1), 1-21; https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1010001
Submission received: 24 July 2020
/
Revised: 13 September 2020
/
Accepted: 15 September 2020
/
Published: 21 September 2020
Abstract
:Sesame allergy is a life-threatening disease that has been growing globally with poorly understood mechanisms. To protect sensitive consumers, sesame is regulated in many countries. There were four research goals for this work on sesame allergy: (i) to map the timeline, and the extent of its global rise; (ii) to dissect the complexity of the disease, and its mechanisms; (iii) to analyze the global regulation of sesame; and (iv) to map the directions for future research and regulation. We performed a literature search on PubMed and Google Scholar, using combinations of key words and analyzed the output. Regulatory information was obtained from the government agencies. Information relevant to the above goals was used to make interpretations. We found that: (i) the reports appeared first in 1950s, and then rapidly rose globally from 1990s; (ii) sesame contains protein and lipid allergens, a unique feature not found in other allergenic foods; (iii) it is linked to five types of diseases with understudied mechanisms; and (iv) it is a regulated allergen in 32 advanced countries excluding the USA. We also provide directions for filling gaps in the research and identify implications of possible regulation of sesame in the USA.
1. Introduction
There is sound evidence that the Western world is in the midst of an ongoing widespread food allergy, and that some of the Eastern world is noticing its rise as well [1,2,3,4]. For example, recent reports show that the prevalence of food allergies in the United States of America (USA) have increased to 8% in children and 10.8% among adults from their respective prevalence rates of 6% and 3.7% just 15 years ago [5,6]. This data translate to an increase of 33% among children, and a staggering 191.8% rise among adults during this short historical period. A similar rise in food allergy prevalence has been noted in Canada, Australia, European countries, New Zealand, and Israel [4]. Furthermore, in the Eastern world, once thought to be free from food allergies, increasingly evidence shows their rise in Japan, Singapore, South Korea, and India [1,7,8]. A few African countries have recently reported cases of food allergies as well [9,10]. Thus, food allergies are on the rise in multiple continents, and therefore warrant serious considerations for further research and food safety regulation.
Since avoidance of food allergens is critical in protecting allergic consumers, the USA, Canada, European Union (EU) countries, the United Kingdom (UK), Australia, New Zealand, and Japan have developed their own lists of priority/major allergenic foods for regulatory purposes [11,12,13,14,15,16] (Table 1). There are many allergic foods that are commonly regulated across all these countries. However, some foods are not. For example, in the USA, sesame, mustard, lupine, celery, mollusks, and sulfites are not presently regulated as food allergens. During the past two years, sesame allergy has been increasingly discussed in the USA, and the United States Food and Drug Agency (US FDA) has been considering whether or not to include sesame into the list of major allergens for regulation [2,11].
Sesame is a major global agricultural crop whose production has increased from 2.3 million tons in 1994 to more than 5.5 million tons in 2017 [17]. Interestingly, sesame allergies are not reported from the top ten sesame-producing countries in the world, including India and China, which are the top two largest sesame producers [17]. Sesame seeds are available in three different colors—black, white, and brown (Figure 1). They contain 50% to 60% oil. Both seeds and oils are commonly used in food preparations. For example, sesame seeds are added to foods (such as bread, bagels, buns, pizza, etc.) or used directly in making food items (such as tahini, hummus, dry food powder, and confectionaries) [18]. Sesame oil is used in salad dressings and for the deep-frying of foods. Sesame oil has long been regarded as safe and inert [18,19]. Therefore, it is used very commonly in pharmaceutical and cosmetic industries. For example, oil is used in ointments, in intramuscular injections to deliver hormones and drugs, in lipsticks, body oils, and in moisturizing creams [18]. Furthermore, sesame oil is widely used in ancient medical practices of Indian (Ayurveda) and Chinese systems for pain disorders [18,20,21]. Furthermore, exposure to sesame also occurs in occupational settings (e.g., bakeries and oil industry) where it is dealt with as an occupational hazard for workers [22,23,24]. Thus, environmental exposure of humans to sesame and sesame containing products has been increasing globally.
There were four research goals for this article: (i) to map the timeline, and the extent of the global rise of sesame allergy; (ii) to dissect the complexity of sesame allergy, and identify the gaps in the mechanisms of the disease; (iii) to compare and contrast the global regulation of sesame and to identify the challenges; and (iv) to map the directions for future research and regulation.
We performed a literature search on PubMed and Google Scholar using the key words. We retried 265 documents from the PubMed using the key words ‘Sesame AND allergy’. Other combination of key words retrieved 212 to 215 documents from the PubMed. We retrieved 4490 articles from Google Scholar search using the combination of key words ‘Sesame AND allergy AND hypersensitivity AND human’. We analyzed the output, removed the duplications and identified the relevant articles in English language for further analysis. All used articles have been cited in the references. The relevant information pertaining to the study goals was then used to produce collective data and make interpretations to accomplish the goals. Published information by food safety regulatory agencies on their respective webpages was used to collect, analyze, and interpret the information on the regulation of sesame.
Results from this work has provided the concise and an up to date information on the published evidence related to the timeline of the global rise of sesame allergy, the natural history of sesame allergy, the diverse nature of the sesame allergens, the complexity of diseases with largely unknown underlying mechanisms, the gaps in the scientific knowledge, and the challenges and implications for potentially regulating sesame as a major allergenic food in the USA. We think that this timely article will stimulate advances in sesame allergy research, as well as provide the scientific background and a context to the ongoing discussions on whether or not to regulate sesame as a major food allergen in the USA, and perhaps in other countries as well.
2. Mapping the Origin and the Global Rise of Sesame Allergy: The 1950s to the Present
Sesame has been used by humans since the ancient times as a food, as well as a medicine. Earliest records of use dates back to 2450 BC [25]. We have tabulated the origin and the major milestones of the global rise of sesame allergies [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] (Table 2). Reports of adverse reactions to sesame started appearing from the 1950s and then rose dramatically during the past thirty years. Ironically, although sesame is not currently regulated in the USA, the very first report on sesame seed and oil allergy and anaphylaxis came from this country [26]. The first report describes a sudden, multi-organ onset of symptoms in a subject by 30 min of consumption of food containing sesame seed and sesame oil. Reactions included gut and skin symptoms, as well as anaphylaxis. Skin testing was positive with sesame seed extract. The author raised safety concerns for sesame for the first time in the modern medical history. A year later, a second case with symptoms of asthma, as well as food allergic reaction caused by sesame seed was also reported from the USA [27].
The first report of an allergic reaction to sesame oil was also from the USA [28]. These authors surprisingly found that sesame oil, which had been used as a control oil for gold therapy in rheumatoid arthritis patients, had triggered generalized urticaria and pruritus in 25% of control subjects (5/25) when intramuscularly injected. They warned that, in contrast to the popular medical notion that sesame oil was inert and safe, serious adverse reactions to sesame oil must be considered.
Since then, the number of reports on sesame allergy from multiple countries have steadily grown in the literature. However, estimation of the prevalence of sesame allergy did not begin until the later part of the 1990s. Although the first estimation of population prevalence of sesame allergy in the UK showed it a low level, later studies reported significantly increased prevalence. For example, based on perception, a prevalence rate of 0.6% among children >15 years old was reported subsequently [49]. Later studies, based on skin prick testing, estimated a prevalence of 0.2–0.9% among the children of the UK [50,51,52]. However, based on oral challenge confirmations, the prevalence was at the rate of 0.1% [52]. Similarly, in Australia also, increased prevalence among infants (0.8%) has been reported since the first prevalence study [53,54].
In light of the extensive use of sesame in the Middle Eastern diet, there is a growing interest in studying sesame allergy in those countries with the report from Israel. The sesame allergy was the third most common food allergy amongst Israeli children after egg and milk; and sesame was the second most common trigger of anaphylaxis after milk [33]. A recent study showed that the prevalence of sesame allergy in Israel among young adults (17–18 years) was at 0.09% [55]. In Lebanon, sensitization (i.e., IgE, and skin prick testing positivity) to sesame among infants, children, and adults was at 3.9%, 2.65% and 1.9%, respectively; and anaphylaxis was the only clinical symptom [37]. Later studies have identified that the sesame allergy and anaphylaxis are also a growing problem in Saudi Arabia, Iran, Kuwait, and Turkey [39,41,42,48]. Thus, the extensive use of sesame in the food and the increased reporting of sesame allergy among the Middle Eastern population suggests a strong correlation of disease with widespread exposure to sesame via the food.
Although the first US prevalence study on sesame allergy, based on self-reporting, found a rate of 0.1% among the general population, a very recent report and the largest study to date (78,851 subjects), showed that 0.49% of the US population reported sesame allergy [2]. Based on at least one stringent symptom, they found that 0.23% of the population had confirmed sesame allergy. These two studies, conducted about a decade apart, suggest substantial increase (230–490%) in the prevalence of sesame allergy during the past decade in the USA [2]. Sesame allergies have also become a significant public health problem in Canada and Mexico [36,40].
In Asian countries, sesame allergies appear to be not very common, with the exception of Singapore, where nearly 3.7% of food allergic children had sensitization to sesame as measured by skin prick testing [56]. Interestingly, there are no reports on sesame allergy from India, China, or other countries where it is commonly grown and used. It is unclear whether or not this is due to absence of actual disease, or simply a lack of reporting due to inadequate diagnosis and testing. Nevertheless, as discussed above, there is now growing evidence that the burden of sesame allergy appears to be increasing in European countries, the Americas, Australia, and Middle Eastern countries with a high risk of life-threatening anaphylaxis (Table 2).
3. The Natural History of Sesame Allergy vs. Other Major Food Allergies
Most food allergies start early in infancy or childhood (during the first three years of life after birth), and so do most sesame allergies [3,5,57,58]. However, adult-onset food allergies are also fairly common [3]. A recent study shows that 1 in 4 sesame allergies are indeed adult-onset types [2]. A similar frequency of adult-onset food allergy has been previously reported for shellfish, milk, wheat, tree nuts, and soy [58].
Some food allergies are outgrown more commonly than others. For example, even though children develop allergies to egg, milk, soy, and wheat early on in life, most of them outgrow their food allergies before becoming adults [3,4,58]. In contrast, most (70–80%) children with allergies to peanut, tree nut, fish, shellfish, and sesame do not outgrow their food allergies [2,3,49,58,59,60]. In general, there is no evidence for a major gender-bias for either sesame allergies or for other major food allergies [2,3,18].
Thus, similar to other major food allergies, sesame allergies also tend to be life-long health problems for both children and adults. All must avoid the offending allergenic foods for the rest of their lives until they outgrow their food allergies as verified by their doctors. Therefore, sesame allergy subjects face the same set of challenges of avoiding the allergen as do subjects with other major types of food allergies.
4. Sesame Allergy: A Complex Spectrum of Clinical Presentations
Sesame allergy does not appear as just one type of disease. Rather, current evidence from the literature shows that it includes at least five types of distinct clinical entities based on the nature of clinical presentations as summarized below and illustrated in Figure 1.
In the first type, clinical symptoms appear immediately within minutes to 3 h after exposure to sesame seeds. Symptoms include angioedema, vomiting, diarrhea, urticaria (hives), conjunctivitis, systemic anaphylaxis, and airways allergic reactions including asthma [1,2,3,4,5,18,58]. This reaction is potentially deadly.
The second type of reaction is of immediate nature, however, it is triggered by sesame oil, where systemic anaphylaxis, including generalized pruritus, erythema, vomiting, and dizziness occurs within minutes to hours after eating the sesame oil containing foods [18,61,62]. This reaction is also potentially deadly.
The third type of reaction includes mainly skin symptoms (i.e., allergic contact dermatitis) a day or two after exposure to the sesame oil [29,63,64,65]. This is not a life-threatening reaction. However, without the prompt diagnosis and avoidance of exposure to the sesame oil, it can become a chronic inflammatory skin condition.
The fourth type involves acute reactions with colic and diarrhea within 1–4 h upon eating sesame. This condition is known as acute food protein-induced enterocolitis syndrome (AFPIES) with explosive (or projectile) vomiting as the most common symptom [66,67]. This reaction can be potentially fatal in infants and children.
Finally, the fifth type includes chronic inflammation of the esophagus leading to dysphagia and is associated with excessive number of eosinophils in the esophagus—a condition known as eosinophilic esophagitis (EOE) [2,5,68,69]. Without diagnosis and elimination of sesame from the diet, this can become a chronic, debilitating condition. However, it is not a life-threatening reaction.
5. The Biochemical Diversity of Sesame Allergens: Proteins and Lipids
Current evidence shows that sesame produces at least two distinct groups of allergens—protein allergens present in the sesame seeds and lipid allergens present in the sesame oil. There are eight protein allergens identified in sesame to date—Ses i 1 to Ses i 8, with molecular weights ranging from 7 to 57 kDa (Table 3). There is the possibility that additional protein allergens may be present in the sesame seed that remain to be characterized [70,71,72,73,74].
Six of the sesame protein allergens (Ses i 1, Ses i 2, Ses i 3, Ses i 6, Ses i 7, and Ses i 8) are hydrophilic in nature and therefore are soluble in aqueous solutions. They belong to 4 different protein families that function as seed storage proteins—2S albumin, 11S globulin, 7S vicilin, and profilin [70,71,72,73,74]. Seed storage proteins are an important source of nutrients during seed germination. Allergy to seed storage protein is easily detected by conventional skin testing with aqueous extracts.
Two sesame protein allergens, Ses i 4 and Ses i 5, are hydrophobic in nature, and are associated with oil. These are known as oleosins [75,76]. They function as structural proteins present in the oil bodies and stabilize the oil droplets. They are linked to severe anaphylaxis. However, allergy to oleosins is not detectable by conventional skin testing done with aqueous extracts because of their insolubility. They are major allergens in France and minor allergens in the Netherlands [75,77].
Sesame oil contains at least three lipid allergens. Previous studies have identified these lipid allergens as unsaponifiable lignan molecules with a small ring structure—Sesamin, Sesamol, and Sesamolin [29,65]. These investigators used purified lipid allergens and confirmed their ability to cause allergic contact dermatitis by conducting skin patch testing in sensitized subjects. There is no current evidence that other major allergenic foods, including peanut oil, contain any lipid allergens [3,4,78]. There are reports on local and systemic contact dermatitis in cashew nut industry workers. There is also report of such a reaction upon eating pesto sauce contaminated with cashew nutshell oil, which contains lipid allergens similar to urushiol present in poison ivy [79,80,81].
6. Pathogenesis of Sesame Allergy: Gaps in the Cellular and Molecular Mechanisms
The mechanisms of the pathogenesis of sesame allergy are largely understudied. It is simply assumed to be similar to other food allergies. Most food allergies manifest in two general forms based on the time of appearance of clinical symptoms after exposure and the underlying immune mechanisms involved in eliciting them [3,4,82]. They are: (i) immediate (or Type I or IgE antibody-mediated) hypersensitivity reactions, where symptoms appear within minutes to 3 h; and (ii) delayed (or Type IV or cell mediated) hypersensitivity reactions, where symptoms of reaction appear after 48–72 h of exposure to the food allergens [83,84]. Most food allergies are of the Type I nature. However, some food allergies such as milk allergies can involve both Type I and Type IV reactions [84].
Mechanisms underlying these two distinct types of reactions are completely different. However, both involve two essential steps: (i) sensitization phase; and (ii) disease elicitation phase [3,4,82]. Although specific mechanisms of these phases for sesame allergy have not been widely studied, they are thought to be similar to other allergies. Therefore, using general mechanisms of food allergy development, these phases are described below for sesame allergy.
6.1. Sesame Seed Protein Allergens Cause Type I Hypersensitivity Reactions: Mechanisms
Mechanisms through which sesame seed proteins specifically trigger sensitization in humans are largely unknown. However, based on mechanisms in a mouse model of sesame allergy, and based on the general mechanisms of other food allergies, the following model is proposed (Figure 2) [3,4,82,85,86].
6.1.1. Phase One: Mechanism of Sensitization upon Initial Exposure to Protein Allergens
Exposure of a genetically susceptible subject to sesame protein allergens via the oral and/or skin routes results in capture of the allergenic proteins by the professional antigen presenting cells (APCs) (e.g., Langerhans cells in the skin, dendritic cells, macrophages/monocytes in the gut) [3,4,82] (Figure 2). These APCs process the allergen and present its fragments as peptides in association with the Major Histocompatibility Complex (MHC) class-II molecule to allergen specific naïve T helper (Th) lymphocytes. In association with costimulatory cell surface molecules and secreted cytokines, these naïve Th lymphocytes differentiate to become sesame-specific Th-2 lymphocytes. These Th2 lymphocytes in turn help sesame-specific B lymphocytes to produce sesame-specific IgE antibodies. These sesame specific IgE bodies are secreted and released into the blood stream and distributed throughout the body. These IgE antibodies are captured by the high affinity IgE receptors expressed on the mast cells present in the connective tissues and the basophils in the blood. Once an individual has reached this state, this person is regarded as ‘sensitized to sesame protein’ and the process of sensitization to sesame protein is complete. It is noteworthy that at this time, this person has not expressed any clinical symptoms of the disease, but the entire immune process has occurred in the body of the susceptible subject because of exposure to sesame protein allergens [3,4].
6.1.2. Phase Two: Mechanism of Elicitation of Allergic Reaction upon Re-Exposure to Protein Allergens
Re-exposure of a previously sensitized subject to the sesame allergens via the skin, oral, nasal, or other routes of exposure, results in the entry of the allergenic protein into the local tissues where mast cells loaded with sesame-specific IgE antibodies are located, and into the blood where basophils loaded with sesame-specific IgE antibodies are located [3,4,82] (Figure 2). Direct cross-linking of IgE-IgE receptor molecules by the allergenic proteins results in cellular activation and the release of histamine and other powerful mediators of allergic inflammation. It only takes a few minutes to 3 h for these processes to be triggered. Consequently, clinical symptoms of Type I reactions appear immediately after exposure to the sesame allergen. Entry of significant amounts of the allergen into the blood triggers systemic anaphylaxis that can be life-threatening [3,4,82].
6.2. Sesame Seed Oil Lipid Allergens Cause Type IV Hypersensitivity Reaction: Mechanisms
Sesame oil causes a delayed hypersensitivity reaction known as allergic contact dermatitis [29,63,64,65]. No other major allergenic food-derived oils, with the exception of cashew nutshell oil, appear to have this capacity [3,4,78,79,80,81]. Sesame oil allergens that trigger these reactions have been identified as Sesamin, Sesamol, and Sesamolin [29]. These are small ring-structured lipid allergens known as lignans [18,29]. The mechanisms through which they cause sensitization and elicitation of reactions are unknown.
Lipid allergens in general are small hydrophobic chemicals present in plant oils (sesame oil, cashew nutshell oil, poison ivy, poison oak, poison sumac) and cosmetics such as fragrance, toothpaste, and hair dyes (e.g., balsam of Peru, urushiol of poison ivy, farnesol, benzyl benzoate, benzyl cinnamate) [86,87,88,89,90,91]. The mechanisms through which they trigger allergic reactions have been deciphered for some of the lipid allergens, but not for sesame lipid allergens [86,87,88,89,90,91]. Furthermore, some of these lipid allergens show structures similar to that of sesame lipid allergens. Therefore, here we have discussed mechanisms about how lipid allergens are known to trigger allergic contact dermatitis (or contact hypersensitivity) reactions in humans or in animal models, and have illustrated this in Figure 3.
6.2.1. Phase One: Mechanisms of Sensitization to Lipid Allergens
Entry of lipid allergens into the body of susceptible subjects leads to their uptake by the APCs, such as Langerhans cells and presentation to specific naïve T cells to initiate their proliferation and differentiation into effector and memory T cells [86,87,88,89,90,91] (Figure 3). There are two models to explain specifics on how APCs are able to do this. The first model suggests that lipid allergens, which are considered as haptens because of their very small sizes of <500 Daltons, form covalent bonds to host proteins, resulting in an immunogenic hapten-carrier complex molecule that is then presented by the APCs in the context of MHC class II molecules to T cells that get activated [86]. The second, and most recent, model suggests that lipids allergens can also directly bind to CD1a molecule, a non-classical MHC molecule expressed by the Langerhans cells (a type of APC) in the skin, by displaying the self-lipids normally bound to the CD1a inside its molecular cleft or hole [87,88,89,90,91]. This results in the presentation of lipid allergens to which T cell reactions are initiated, resulting in the formation of specific effector and memory T cells. Once an individual has reached this state, this person is regarded as ‘sensitized to the lipid allergen’ and the process of sensitization to the lipid allergen is complete. At this time, however, no disease symptoms are expressed; only the entire immune process has occurred in the body of the susceptible subject because of the exposure to the lipid allergen.
6.2.2. Phase Two: Mechanisms of Elicitation of Allergic Reaction to Lipid Allergens
Re-exposure of a previously sensitized subject to the same lipid allergens results in their entry and presentation of by the APCs to the pre-formed allergen specific effector and memory T cells [86,87,88,89,90,91] (Figure 3). This results in their activation, proliferation, and release of cytokines and chemokines into the local tissues and eventually into the blood. These inflammatory molecules recruit more immune cells (including T helper subsets, eosinophils, monocytes, macrophages) to the tissue that further cause damage. Consequently, this tissue damage is expressed clinically as swelling, erythema, itching, and urticaria as in allergic contact dermatitis. It takes 48–72 h for these cellular and molecular responses to reach the peak. Consequently, this type of allergic disease is known as delayed hypersensitivity.
6.3. Does Sesame Use Additional Immune Mechanisms to Trigger Allergic Reactions?
Interestingly, there are two reports of sesame oil causing anaphylactic reaction without the need of IgE antibodies [61,62] (Figure 1). In the first study, authors investigated a case of recurrent anaphylactic attacks from sesame oil consumption [61]. They found 2-fold stronger skin test positivity to commercial sesame oil (4+) vs. commercial sesame seed protein (2+) and strong histamine release from sesame oil (40%) vs. the sesame seed protein (6%). Specific IgE (Radio Allergo Sorbent Test) results were negative. Therefore, they concluded that the mechanism of anaphylaxis to sesame oil was unknown. In the second study, authors investigated a case of anaphylaxis upon eating foods containing sesame oil but not the sesame seed [62]. They found the blood test negative for IgE to sesame protein (ImmunoCap-FEIA). They optimized a basophil activation test and found that sesame oil activated basophils to a higher level (51%) than the sesame seed (44%). They concluded that anaphylaxis to sesame oil can occur in the absence of IgE antibodies. The mechanism was not explained.
Sesame is also increasingly linked to two other less understood types of allergic reactions: acute food-protein induced enterocolitis syndrome (AFPIES) and eosinophilic esophagitis (EOE) [66,67,68,69]. Both of these are non-IgE allergic reactions mediated by unknown mechanisms.
The AFPIES is characterized by vomiting, lethargy, and diarrhea in infants and children within 1–4 h after feeding. This requires immediate medical help because it can be life-threatening due to dehydration and shock [66]. Many major allergenic foods (milk, egg etc.), can trigger this, and so also can sesame. However, authors note that there is lack of awareness on this issue as this is a relatively newly identified immune disorder [67]. Furthermore, another recent study found that compared to subjects with other food allergies, subjects with sesame allergy had 2.5-fold higher rates of AFPIES [2]. Although these allergic reactions are linked to sesame, the biochemical nature of the allergens mediating them are unknown (Figure 1).
The food induced EOE is a non-IgE mediated reaction. It is caused by the reaction of eosinophils to the food components. Several major allergenic foods (e.g., wheat, milk, egg, soy) can trigger this reaction. Recent studies have identified sesame also as a suspected food trigger of EOE [2,68,69]. One study showed that compared to subjects with other major food allergies, sesame allergy subjects have seven times higher rates of EOE [2]. However, the components of sesame (i.e., the allergen) responsible for causing EOE are unknown. The molecular mechanism of EOE pathogenesis is a subject of intense research at present and readers are referred to an excellent recent review [92] (Figure 1).
Thus, there is growing evidence that allergic reactions caused by sesame are diverse and complex. Cellular and molecular mechanisms underlying these reactions are largely understudied. Therefore, future research is warranted in this area.
7. How to Advance the Basic, Preclinical, and Clinical Research in Sesame Allergy? An Urgent Need
As opposed to several other major allergenic foods (e.g., peanut, milk, egg etc.), research on sesame allergy remains very basic. Published papers typically report the sesame allergy prevalence, characterization of the allergens, and description of the cases illustrating clinical presentation, diagnosis, and treatment. We have illustrated eight specific directions where advancement of research is needed, rather urgently, in view of the ongoing global rise of sesame allergies and their ability to trigger life-threatening anaphylaxis (Figure 4).
Food allergies are complex genetic disorders where unknown environmental factors trigger the disease onset only in genetically susceptible subjects [93,94,95,96]. The role of genetics in resistance vs. susceptibility to develop sesame allergies needs to be determined. Knowledge about what kind of environmental factors favor development of sesame allergy are largely unknown [97,98,99,100,101,102,103,104,105].
Several exposure conditions (e.g., environmental toxicants, triclosan, parabens, food preservatives, misuse of antibiotics, Vitamin D deficiency, sunlight exposure, dog ownership, excess use of antacids etc.,) that are currently being explored for other food allergies should provide the starting points of research [97,98,99,100,101,102,103,104,105].
Host microbiome plays a critical role in the development of multiple diseases including food allergies [106,107]. Their role in prevention as well as causing sesame allergies remains unknown in humans or in animal models. Therefore, this represents a fascinating area of research to undertake in the future.
Effective clinical interventions (e.g., vaccines, immunotherapy) are underway for peanut allergies and other food allergies with variable success [3,4]. Therefore, development of vaccines and effective immunotherapy protocols (e.g., oral, sublingual, and epicutaneous immunotherapy) for sesame allergies are urgently needed.
Food processing has been shown to influence food protein allergenicity [108,109,110,111,112,113,114]. For example, boiling vs. roasting of peanuts reduces vs. increases allergenicity, respectively [107,110,111,114]; and extrusion processing appears to reduce hazelnut allergenicity [112]. Therefore, effect of thermal and nonthermal food processing methods on sesame allergenicity must be evaluated in future research.
The last, but not the least, important area is the development of hypoallergenic sesame products. There are hypoallergenic food products available for milk and egg allergic subjects [115,116]. Hypoallergenic wheat lines and peanuts are being developed using genetic engineering methods [117,118]. Similar approaches could be used to develop hypoallergenic and potentially nonallergenic sesame products. Previous studies show that different wheat genotypes may naturally differ in allergenicity [119]. Whether or not sesame varieties naturally differ in allergenicity in vivo is largely unexplored at present. Therefore, evaluating differences in allergencity among existing sesame varieties and efforts to produce novel potentially hypo/nonallergenic varieties using conventional cross-hybridization and plant breeding methods may be undertaken in the future.
Animal models of sesame allergy would be of immense value in all these areas of research [82,120]. However, only one mouse model of sesame allergy and anaphylaxis to proteins has been reported so far [34]. Therefore, more emphasis needs to be placed on developing both primate and nonprimate animal models and their use to conduct the basic, preclinical translational research on sesame allergy.
In essence, there is conspicuous absence of significant basic, preclinical, and clinical research on sesame allergies at present. The current rapid rise in sesame allergies warrants that the food industry, the government agencies, and the private research enterprise needs to take note of this gap in science and devote funds to address these research challenges so that the future generations are empowered to prevent and manage sesame allergies.
8. The Global Regulation of Sesame for Food Safety: Does Sesame Need to Be Regulated in the United States of America?
Since exposure to sesame allergens is required to trigger allergic reactions including life-threatening anaphylaxis, preventing exposure is an effective method to protect sensitive consumers. It is not easy to avoid sesame, as opposed to other major allergens, because it is often added in small amounts as a garnishing item to many foods, dressings, condiments, and as a ‘natural flavor’ [121]. Despite labeling, accidental exposures are common [122,123,124]. It is noted that both initial and accidental reactions to sesame are inadequately managed for children at present [125]. Thus, the challenges faced by sesame allergic subjects and their families are very similar to that faced by other food allergic subjects. Consequently, food safety regulatory authorizes in Canada, the EU countries, the UK, Australia, New Zealand, and Japan currently regulate sesame as a major or priority food allergen [18,126]. Appropriate labeling on the food products is an effective method of prevention by informing sensitive consumers to avoid the food product.
The Food Allergen Labeling and Consumer Protection Act (FALCPA) of the USA came into effect from January 2006 to improve the regulation of major food allergens [11]. However, it did not include sesame into the list of major allergens. The FALCPA regulates specifics on the labeling of allergenic foods on food packages. Absence of such labeling is a leading cause of class I food recalls—the highest state of alert issued in the USA [11]. However, sesame is not federally regulated by FALCPA. A new federal bill, the Food Allergy Safety, Treatment, Education, and Research (FASTER) act, has been introduced recently in the US Congress that proposes to add sesame to the list of major allergenic foods, although the final decision on regulation has not been made as yet [44].
The lack of the federal regulation of sesame, but the growing prevalence of the disease at an alarming rate in the USA as discussed earlier, resulted in the creation of a new state law in Illinois, USA [45]. On 26 July 2019, the Illinois Governor signed HB2123, which requires any packaged food containing sesame to identify it on the label. This action amended the Illinois Food, Drug, and Cosmetic Act by changing the Section 11 of the law. Per this change, “a food is considered misbranded: _ (s) if it contains sesame, is offered for sale in package form but not for immediate consumption, and the label does not include sesame” (lines 19–21) [45].
A zero-tolerance policy is in place for the regulation of major allergenic foods in all countries where they are regulated [126]. This applies to sesame also in those countries where it is regulated (Table 1). The zero-tolerance policy is based on the fact that threshold oral elicitation doses for food allergens have not been universally standardized and are not well accepted at present. Oral provocation tests show that there is a large variability in the oral threshold elicitation doses amongst food allergic subjects, with some reacting to lower milligram quantities of allergenic food extracts [126]. A similar variability has been noted for sesame allergy patients in oral challenge studies [127,128,129]. Latest studies show that the minimal reaction elicitation dose (ED) in 5% of the sensitized population (ED05) for sesame vs. peanut is as follows: 4.2 mg (95% CI, 0.6–57.7 mg) for sesame vs. 3.9 mg (95% CI, 2.8–7.1 mg) for peanut [130]. Thus, oral disease elicitation potency of sesame appears to be similar to that of the other currently regulated major allergenic foods. These facts suggest that a zero-tolerance policy might be necessary for the regulation of sesame, similar to other major allergenic foods, if it were to be regulated in the USA.
Currently, food safety regulations apply only to protein allergens. Regulation of oils from major allergenic foods is complicated. In the USA, highly refined oils derived from the major allergenic foods are exempt from FALCPA labeling requirements as long as there is evidence that the method used to produce that oil establishes absence of protein contaminants [11]. In Canada, all unrefined oils are subjected to enhanced food allergen labeling requirements [14]. However, highly refined oils, except peanut oil, are not subjected to enhanced food allergen labeling requirements, but declaration as ingredient is required [14]. In the EU countries, Australia, and New Zealand, fully refined soy oil is exempt from labeling and no information is available for sesame oil or oils derived from other major allergenic foods in those countries [12,13,15].
Sometimes, oil-induced reactions could result from trace amounts of proteins present in them due to inadequate processing, and that are falsely attributed to oils. Furthermore, some hydrophobic protein allergens, known as oleosins, can also be present in oils. Nevertheless, as discussed earlier, sesame oil has been implicated in causing true allergic reactions—both immediate as well as delayed types of reactions (Figure 1). Furthermore, an oral challenge test using oil in sesame allergy subjects also shows that immediate allergic reactions do occur upon oil feeding in controlled studies: some react to 3 mL while others at 15 mL of sesame oil in oral provocation testing [127,128,129]. In addition, a variety of adverse reactions to sesame oil have been reported in the literature: lipoid pneumonia from sesame oil pulling, pneumonitis, eosinophilia, and eosinophilic pneumonia after in vitro fertilization treatments that had exposed subjects to the sesame oil, and subcutaneous granuloma formation due to intramuscular injection of sesame oil [131,132,133,134,135,136]. Thus, there is considerable evidence that the sesame oil is immunologically active in vivo and that it can elicit immune mediated adverse reactions in a variety of exposure situations.
Thus, together these lines of evidence show that the mechanisms of action of sesame oil on the immune system needs to be further elucidated. Furthermore, they also raise the question: should sesame oil be regulated for food safety in addition to the sesame protein?
The current food allergen regulation model is based on the ability of foods to trigger IgE-mediated reactions that tend to be life-threatening. There is growing evidence that non-IgE mechanisms to sesame and to other foods/drugs also can mediate life-threatening reactions in humans [137,138]. Therefore, should non-IgE mediated mechanisms also dictate food safety regulation?
Mandatory food allergen labelling has significantly advanced food safety for food allergy consumers. A related issue is the precautionary labelling of allergens, which are increasingly noticed on packaged foods. Occasionally, sesame is identified on the food labels in the USA, under the precautionary allergen labelling concept, which is not legally required in the USA. It is a voluntary decision made by the food industry. However, a recent outstanding study showed that consumers misunderstand such precautionary allergen labelling and that up to 40% of consumers purchased the products with precautionary labels [139]. Therefore, to enable enhanced food safety for sesame allergic consumers in the USA, mandatory labelling may be of more benefit than the voluntary precautionary allergen labels.
9. Conclusions
There is substantial evidence that the prevalence and the severity of sesame allergy has been rising at the global level, including in the USA. There is scientific evidence that sesame contains both protein as well as lipid allergens that can trigger distinct types of allergic reactions. However, the specific mechanisms underlying the pathogenesis of sesame allergy remains to be determined. There is a major gap in animal models development and their application in basic and preclinical research studies. The human clinical research on sesame allergy is urgently needed to develop effective therapeutic and preventive methods for both IgE as well as non-IgE mediated reactions. Currently, 32 countries regulate sesame as a major or priority allergen. However, sesame is not federally regulated as yet in the USA. Nevertheless, the state of Illinois recently enacted a state law to regulate sesame in that one state in the USA. This situation, along with the recent research showing an alarming rise in the prevalence during the past decade, has placed more pressure on regulating sesame as a major allergen in the USA. This review is expected to provide the background and the context to stimulate further discussions on whether or not to regulate sesame in the USA and in other countries where it is not currently regulated.
Author Contributions
Conceptualization, V.G. and H.G.A.; methodology, V.G. and H.G.A.; validation, V.G. and H.G.A.; formal analysis, V.G. and H.G.A.; investigation, V.G. and H.G.A.; resources, V.G.; data curation, V.G. and H.G.A.; writing—original draft preparation, V.G.; writing—review and editing, V.G. and H.G.A.; visualization, V.G. and H.G.A.; supervision, V.G.; project administration, V.G.; funding acquisition, Not Applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This project was conducted without any funding.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- De Martinis, M.; Sirufo, M.M.; Suppa, M.; Ginaldi, L. New Perspectives in Food Allergy. Int. J. Mol. Sci. 2020, 21, 1474. [Google Scholar] [CrossRef] [Green Version]
- Warren, C.M.; Chadha, A.S.; Sicherer, S.H.; Jiang, J.; Gupta, R.S. Prevalence and Severity of Sesame Allergy in the United States. JAMA Netw. Open 2019, 2, e199144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renz, H.; Allen, K.J.; Sicherer, S.H.; Sampson, H.A.; Lack, G.; Beyer, K.; Oettgen, H.C. Food allergy. Nat. Rev. Dis. Primers 2018, 4, 17098. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.S.; Warren, C.M.; Smith, B.M.; Jiang, J.; Blumenstock, J.A.; Davis, M.M.; Schleimer, R.P.; Nadeau, K.C. Prevalence and Severity of Food Allergies Among US Adults. JAMA Netw. Open 2019, 2, e185630. [Google Scholar] [CrossRef]
- Sampson, H.A. Update on food allergy. J. Allergy Clin. Immunol. 2004, 113, 805–819. [Google Scholar] [CrossRef]
- Lee, A.J.; Shek, L.P. Food allergy in Singapore: Opening a new chapter. Singapore Med. J. 2014, 55, 244–247. [Google Scholar] [CrossRef]
- Loh, W.; Tang, M.L.K. The Epidemiology of Food Allergy in the Global Context. Int. J. Environ. Res. Public Health 2018, 15, 2043. [Google Scholar] [CrossRef] [Green Version]
- Kung, S.J.; Steenhoff, A.P.; Gray, C. Food allergy in Africa: Myth or reality? Clin. Rev. Allergy Immunol. 2014, 46, 241–249. [Google Scholar] [CrossRef]
- Levin, M.E.; Botha, M.; Basera, W.; Facey-Thomas, H.E.; Gaunt, B.; Gray, C.L.; Kiragu, W.; Ramjith, J.; Watkins, A.; Genuneit, J. Environmental factors associated with allergy in urban and rural children from the South African Food Allergy (SAFFA) cohort. J. Allergy Clin. Immunol. 2020, 145, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Guidance & Regulation Food and Dietary Supplements. Available online: https://www.fda.gov/Food/GuidanceRegulation (accessed on 20 May 2020).
- EFSA Provides Scientific Basis for Labelling of Food Allergens: Current Evidence does not Allow Determination of Intake Thresholds. Available online: https://www.efsa.europa.eu/it/press/news/nda040325 (accessed on 21 June 2020).
- Allergy and Intolerance. Available online: https://www.food.gov.uk/science/allergy-intolerance (accessed on 22 January 2020).
- Food Labelling. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-labelling/ (accessed on 22 January 2020).
- Australia 2020. Available online: http://www.foodstandards.gov.au/consumer/foodallergies/allergies (accessed on 12 June 2020).
- Japan 2020. Available online: http://expatsguide.jp/features/everyday-life/food-allergy-labeling/ (accessed on 12 February 2020).
- FAO 2020. Available online: http://www.fao.org/faostat/en/#data/QD/visualize (accessed on 24 June 2020).
- Gangur, V.; Kelly, C.; Navuluri, L. Sesame allergy: A growing food allergy of global proportions? Ann. Allergy Asthma Immunol. 2005, 95, 4–11. [Google Scholar] [CrossRef]
- Johnson, W., Jr.; Bergfeld, W.F.; Belsito, D.V.; Hill, R.A.; Klaassen, C.D.; Liebler, D.C.; Marks, J.G., Jr.; Shank, R.C.; Slaga, T.J.; Snyder, P.W.; et al. Amended safety assessment of Sesamum indicum (sesame) seed oil, hydrogenated sesame seed oil, Sesamum indicum (sesame) oil unsaponifiables, and sodium sesameseedate. Int. J. Toxicol. 2011, 30 (Suppl. 3), 40S–53S. [Google Scholar] [CrossRef] [PubMed]
- Askari, A.; Ravansalar, S.A.; Naghizadeh, M.M.; Mosavat, S.H.; Khodadoost, M.; Jazani, A.M.; Hashempur, M.H. The efficacy of topical sesame oil in patients with knee osteoarthritis: A randomized double-blinded active-controlled non-inferiority clinical trial. Complement. Ther. Med. 2019, 47, 102183. [Google Scholar] [CrossRef] [PubMed]
- Afroz, M.; Zihad, S.M.N.K.; Uddin, S.J.; Rouf, R.; Rahman, M.S.; Islam, M.T.; Khan, I.N.; Ali, E.S.; Aziz, S.; Shilpi, J.A.; et al. A systematic review on antioxidant and antiinflammatory activity of Sesame (Sesamum indicum L.) oil and further confirmation of antiinflammatory activity by chemical profiling and molecular docking. Phytother. Res. 2019, 33, 2585–2608. [Google Scholar] [CrossRef]
- Alday, E.; Curiel, G.; Lopez-Gil, M.J.; Carreño, D.; Moneo, I. Occupational hypersensitivity to sesame seeds. Allergy 1996, 51, 69–70. [Google Scholar] [CrossRef]
- Keskinen, H.; Ostman, P.; Vaheri, E.; Tarvainen, K.; Grenquist-Norden, B.; Karppinen, O.; Nordman, H. A case of occupational asthma, rhinitis and urticaria due to sesame seed. Clin. Exp. Allergy 1991, 21, 623–624. [Google Scholar] [CrossRef]
- Caimmi, S.; Marseglia, A.; Caimmi, D.; Marseglia, G.L. Friday asthma crisis in the daughter of two bakers. Int. J. Immunopathol. Pharmacol. 2011, 24, 517–518. [Google Scholar] [CrossRef]
- Kägi, M.K.; Wüthrich, B. Falafel burger anaphylaxis due to sesame seed allergy. Ann. Allergy 1993, 71, 127–129. [Google Scholar] [CrossRef]
- Rubenstein, L. Sensitivity to sesame seed and sesame oil. N. Y. State J. Med. 1950, 50, 343. [Google Scholar]
- Uvitsky, I.H. Sensitivity to sesame seed. J. Allergy 1951, 22, 377–378. [Google Scholar] [CrossRef]
- Batterman, R.C.; Grossman, A.J.; Leifer, P. Skin eruptions with gold therapy; influence of sesame oil. Arthritis Rheum. 1958, 1, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Neering, H.; Vitányi, B.E.; Malten, K.E.; van Ketel, W.G.; van Dijk, E. Allergens in sesame oil contact dermatitis. Acta Derm.-Venereol. 1975, 55, 31–34. [Google Scholar] [PubMed]
- Malish, D.; Glovsky, M.M.; Hoffman, D.R.; Ghekiere, L.; Hawkins, J.M. Anaphylaxis after sesame seed ingestion. J. Allergy Clin. Immunol. 1981, 67, 35–38. [Google Scholar] [CrossRef]
- United Kingdom Ministry of Agriculture Fisheries and Food. Sesame Seed Allergy Food Safety Information Bulletin; UK Ministry of Agriculture Fisheries and Food: London, UK, 1996.
- Hill, D.J.; Hosking, C.S.; Zhie, C.Y.; Leung, R.; Baratwidjaja, K.; Iikura, Y.; Iyngkaran, N.; Gonzalez-Andaya, A.; Wah, L.B.; Hsieh, K.H. The frequency of food allergy in Australia and Asia. Environ. Toxicol. Pharmacol. 1997, 4, 101–110. [Google Scholar] [CrossRef]
- Dalal, I.; Binson, I.; Reifen, R.; Amitai, Z.; Shohat, T.; Rahmani, S.; Levine, A.; Ballin, A.; Somekh, E. Food allergy is a matter of geography after all: Sesame as a major cause of severe IgE-mediated food allergic reactions among infants and young children in Israel. Allergy 2002, 57, 362–365. [Google Scholar] [CrossRef]
- Navuluri, L.; Parvataneni, S.; Hassan, H.; Birmingham, N.P.; Kelly, C.; Gangur, V. Allergic and anaphylactic response to sesame seeds in mice: Identification of Ses i 3 and basic subunit of 11s globulins as allergens. Int. Arch. Allergy Immunol. 2006, 140, 270–276. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Muñoz-Furlong, A.; Godbold, J.H.; Sampson, H.A. US prevalence of self-reported peanut, tree nut, and sesame allergy: 11-year follow-up. J. Allergy Clin. Immunol. 2010, 125, 1322–1326. [Google Scholar] [CrossRef]
- Ben-Shoshan, M.; Harrington, D.W.; Soller, L.; Fragapane, J.; Joseph, L.; St Pierre, Y.; Godefroy, S.B.; Elliott, S.J.; Clarke, A.E. A population-based study on peanut, tree nut, fish, shellfish, and sesame allergy prevalence in Canada. J. Allergy Clin. Immunol. 2010, 125, 1327–1335. [Google Scholar] [CrossRef] [Green Version]
- Irani, C.; Maalouly, G.; Germanos, M.; Kazma, H. Food allergy in Lebanon: Is sesame seed the “middle eastern” peanut. World Allergy Organ J. 2011, 4, 1–3. [Google Scholar] [CrossRef] [Green Version]
- CSPI. Available online: https://cspinet.org/new/201411181.html (accessed on 20 June 2020).
- Sheikh, F.; Amin, R.; Rehan Khaliq, A.M.; Al Otaibi, T.; Al Hashim, S.; Al Gazlan, S. First study of pattern of anaphylaxis in a large tertiary care hospital in Saudi Arabia. Asia Pac. Allergy 2015, 5, 216–221. [Google Scholar] [CrossRef]
- Bedolla-Barajas, M.; Bedolla-Pulido, T.R.; Macriz-Romero, N.; Morales-Romero, J.; Robles-Figueroa, M. Prevalence of Peanut, Tree Nut, Sesame, and Seafood Allergy in Mexican Adults. Rev. Invest. Clin. 2015, 67, 379–386. [Google Scholar]
- Nabavi, M.; Lavavpour, M.; Arshi, S.; Bemanian, M.H.; Esmaeilzadeh, H.; Molatefi, R.; Rekabi, M.; Ahmadian, J.; Eslami, N.; Shokri, S.; et al. Characteristics, Etiology and Treatment of Pediatric and Adult Anaphylaxis in Iran. Iran J. Allergy Asthma Immunol. 2017, 16, 480–487. [Google Scholar] [PubMed]
- Ali, F. A Survey of Self-Reported Food Allergy and Food-Related Anaphylaxis among Young Adult Students at Kuwait University, Kuwait. Med. Princ. Pract. 2017, 26, 229–234. [Google Scholar] [CrossRef] [PubMed]
- US FDA. Available online: https://www.fda.gov/news-events/press-announcements/statement-fda-commissioner-scott-gottlieb-md-fdas-new-consideration-labeling-sesame-allergies (accessed on 20 June 2020).
- All Information (Except Text) for H.R.2117—FASTER Act of 2019. Available online: https://www.congress.gov/bill/116th-congress/house-bill/2117/all-info (accessed on 10 June 2020).
- Illinois Requires Food Manufacturers to Label Sesame Allergens. Available online: https://will.illinois.edu/news/story/illinois-requires-food-manufacturers-to-label-sesame-allergen (accessed on 15 June 2020).
- Sokol, K.; Rasooly, M.; Dempsey, C.; Lassiter, S.; Gu, W.; Lumbard, K.; Frischmeyer-Guerrerio, P.A. Prevalence and diagnosis of sesame allergy in children with IgE-mediated food allergy. Pediatric Allergy Immunol. 2020, 31, 214–218. [Google Scholar] [CrossRef] [PubMed]
- NIH. Available online: https://www.nih.gov/news-events/nih-research-matters/sesame-allergy-common-among-children-food-allergies (accessed on 13 July 2020).
- Kahveci, M.; Koken, G.; Şahiner, Ü.M.; Soyer, Ö.; Şekerel, B.E. Immunoglobulin E-Mediated Food Allergies Differ in East Mediterranean Children Aged 0-2 Years. Int. Arch. Allergy Immunol. 2020, 181, 365–374. [Google Scholar] [CrossRef]
- Emmett, S.E.; Angus, F.J.; Fry, J.S.; Lee, P.N. Perceived prevalence of peanut allergy in Great Britain and its association with other atopic conditions and with peanut allergy in other household members. Allergy 1999, 54, 380–385, Erratum in 1999, 54, 891. [Google Scholar] [CrossRef] [PubMed]
- Roberts, G.; Peckitt, C.; Northstone, K.; Strachan, D.; Lack, G.; Henderson, J.; Golding, J. ALSPAC Study Team. Relationship between aeroallergen and food allergen sensitization in childhood. Clin. Exp. Allergy 2005, 35, 933–940. [Google Scholar] [CrossRef]
- Pereira, B.; Venter, C.; Grundy, J.; Clayton, C.B.; Arshad, S.H.; Dean, T. Prevalence of sensitization to food allergens, reported adverse reaction to foods, food avoidance, and food hypersensitivity among teenagers. J. Allergy Clin. Immunol. 2005, 116, 884–892. [Google Scholar] [CrossRef]
- Venter, C.; Pereira, B.; Grundy, J.; Clayton, C.B.; Arshad, S.H.; Dean, T. Prevalence of sensitization reported and objectively assessed food hypersensitivity amongst six-year-old children: A population-based study. Pediatric Allergy Immunol. 2006, 17, 356–363. [Google Scholar] [CrossRef]
- Osborne, N.J.; Koplin, J.J.; Martin, P.E.; Gurrin, L.C.; Lowe, A.J.; Matheson, M.C.; Ponsonby, A.L.; Wake, M.; Tang, M.L.; Dharmage, S.C.; et al. HealthNuts Investigators. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J. Allergy Clin. Immunol. 2011, 127, 668–676.e2. [Google Scholar] [CrossRef]
- Peters, R.L.; Koplin, J.J.; Gurrin, L.C.; Dharmage, S.C.; Wake, M.; Ponsonby, A.L.; Tang, M.L.K.; Lowe, A.J.; Matheson, M.; Dwyer, T.; et al. HealthNuts Study. The prevalence of food allergy and other allergic diseases in early childhood in a population-basedstudy: HealthNuts age 4-year follow-up. J. Allergy Clin. Immunol. 2017, 140, 145–153.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nachshon, L.; Schwartz, N.; Elizur, A.; Schon, Y.; Cheryomukhin, M.; Katz, Y.; Goldberg, M.R. The Prevalence of Food Allergy in Young Israeli Adults. J. Allergy Clin. Immunol. Pract. 2019, 7, 2782–2789.e4. [Google Scholar] [CrossRef] [PubMed]
- Chiang, W.C.; Kidon, M.I.; Liew, W.K.; Goh, A.; Tang, J.P.; Chay, O.M. The changing face of food hypersensitivity in an Asian community. Clin. Exp. Allergy 2007, 37, 1055–1061. [Google Scholar] [CrossRef]
- Cohen, A.; Goldberg, M.; Levy, B.; Leshno, M.; Katz, Y. Sesame food allergy and sensitization in children: The natural history and long-term follow-up. Pediatric Allergy Immunol. 2007, 18, 217–223. [Google Scholar] [CrossRef]
- Warren, C.M.; Jiang, J.; Gupta, R.S. Epidemiology and Burden of Food Allergy. Curr. Allergy Asthma Rep. 2020, 20, 6. [Google Scholar] [CrossRef]
- Permaul, P.; Stutius, L.M.; Sheehan, W.J.; Rangsithienchai, P.; Walter, J.E.; Twarog, F.J.; Young, M.C.; Scott, J.E.; Schneider, L.C.; Phipatanakul, W. Sesame allergy: Role of specific IgE and skin-prick testing in predicting food challenge results. Allergy Asthma Proc. 2009, 30, 643–648. [Google Scholar] [CrossRef]
- Aaronov, D.; Tasher, D.; Levine, A.; Somekh, E.; Serour, F.; Dalal, I. Natural history of food allergy in infants and children in Israel. Ann. Allergy Asthma Immunol. 2008, 101, 637–640. [Google Scholar] [CrossRef]
- Chiu, J.T.; Haydik, I.B. Sesame seed oil anaphylaxis. J. Allergy Clin. Immunol. 1991, 88 (3 Pt 1), 414–415. [Google Scholar] [CrossRef]
- Stevens, W.J.; Ebo, D.G.; Bridts, C.H.; De Clerck, L.S. Anaphylaxis tos sesame (Sesamum indicum) seed and sesame oil. J. Allergy Clin. Immunol. 2002, 109, 650. [Google Scholar] [CrossRef]
- Van Dijk, E.; Dijk, E.; Neering, H.; Vitányi, B.E. Contact hypersensitivity to sesame oil in patients with leg ulcers and eczema. Acta Derm. Venereol. 1973, 53, 133–135. [Google Scholar]
- Kubo, Y.; Nonaka, S.; Yoshida, H. Contact sensitivity to unsaponifiable substances in sesame oil. Contact Dermat. 1986, 15, 215–217. [Google Scholar] [CrossRef]
- Oiso, N.; Yamadori, Y.; Higashimori, N.; Kawara, S.; Kawada, A. Allergic contact dermatitis caused by sesame oil in a topical Chinese medicine, shi-un-ko. Contact Dermat. 2008, 58, 109. [Google Scholar] [CrossRef]
- Nowak-Wegrzyn, A.; Warren, C.M.; Brown-Whitehorn, T.; Cianferoni, A.; Schultz-Matney, F.; Gupta, R.S. Food protein-induced enterocolitis syndrome in the US population-based study. J. Allergy Clin. Immunol. 2019, 144, 1128–1130. [Google Scholar] [CrossRef] [Green Version]
- Ovadia, A.; Nahum, A.; Tasher, D.; Abiri, S.; Epov, L.; Kessel, A.; Dalal, I. Sesame: An unrecognized trigger of food protein-induced enterocolitis syndrome. J. Allergy Clin. Immunol. Pract. 2019, 7, 305–306. [Google Scholar] [CrossRef]
- Momen, T.; Saneian, H.; Amini, N. Demographic, Clinical, and Allergic Characteristics of Children with Eosinophilic Esophagitis in Isfahan, Iran. Iran J. Allergy Asthma Immunol. 2018, 17, 533–539. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Choi, S.S.; Gupta, S.K. Eosinophilic esophagitis: Current status and future directions. Pediatr. Res. 2020, in press. [Google Scholar] [CrossRef] [Green Version]
- Van Ree, R.; Voitenko, V.; van Leeuwen, W.A.; Aalberse, R.C. Profilin is a cross-reactive allergen in pollen and vegetable foods. Int. Arch. Allergy Immunol. 1992, 98, 97–104. [Google Scholar] [CrossRef]
- Beyer, K.; Bardina, L.; Grishina, G.; Sampson, H.A. Identification of sesame seed allergens by 2 dimensional proteomics and Edmansequencing: Seed storage proteins as common food allergens. J. Allergy Clin. Immunol. 2002, 110, 154–159. [Google Scholar] [CrossRef]
- Beyer, K.; Grishina, G.; Bardina, L.; Sampson, H.A. Identification of 2 new sesame seed allergens: Ses i 6 and Ses i 7. J. Allergy Clin. Immunol. 2007, 119, 1554–1556. [Google Scholar] [CrossRef]
- Magni, C.; Ballabio, C.; Restani, P.; Fuggetta, D.; Alessandri, C.; Mari, A. Molecular insight into IgE mediated reactions to sesame (Sesamum indicumL.) seed proteins. Ann. Allergy Asthma Immunol. 2010, 105, 458–464. [Google Scholar] [CrossRef]
- Teodorowicz, M.; Terlouw, R.J.; Jansen, A.; Savelkoul, H.F.; Ruinemans-Koerts, J. Immunological Characterization of Dutch Sesame Seed-Allergic Patients. Int. Arch. Allergy Immunol. 2016, 169, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Leduc, V.; Moneret-Vautrin, D.A.; Tzen, J.T.C.; Morisset, M.; Guerin, L.; Kanny, G. Identification of oleosins as major allergens in sesame seed allergic patients. Allergy 2006, 61, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Jappe, U.; Schwager, C. Relevance of Lipophilic Allergens in Food Allergy Diagnosis. Curr. Allergy Asthma Rep. 2017, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, A.M.; Rossnagel, M.; Brix, B.; Blankestijn, M.A.; Le, T.M.; Suer, W.; Otten, H.G.; Knulst, A.C. Sesame oleosins are minor allergens. Clin. Transl. Allergy 2019, 9, 32. [Google Scholar] [CrossRef]
- Taylor, S.L.; Busse, W.W.; Sachs, M.I. Peanut oil is not allergenic to peanut-sensitive individuals. J. Allergy Clin. Immunol. 1981, 68, 372–375. [Google Scholar] [CrossRef]
- Kadlubowska, D.; Bargman, H.; Sasseville, D. Systemic contact dermatitis caused by inhaled cashew oil smoke. Contact Dermat. 2016, 75, 248–250. [Google Scholar] [CrossRef]
- Hirao, A.; Oiso, N.; Matsuda, H.; Kawara, S.; Kawada, A. Occupational allergic contact dermatitis due to cashew nut oil. Contact Dermat. 2008, 59, 131–132. [Google Scholar] [CrossRef]
- Hamilton, T.K.; Zug, K.A. Systemic contact dermatitis to raw cashew nuts in a pesto sauce. Am. J. Contact Dermat. 1998, 9, 51–54. [Google Scholar]
- Jin, Y.; Acharya, H.G.; Acharya, D.; Jorgensen, R.; Gao, H.; Secord, J.; Ng, P.K.W.; Gangur, V. Advances in Molecular Mechanisms of Wheat Allergenicity in Animal Models: A Comprehensive Review. Molecules 2019, 24, 1142. [Google Scholar] [CrossRef] [Green Version]
- Cartledge, N.; Chan, S. Atopic Dermatitis and Food Allergy: A Paediatric Approach. Curr. Pediatric Rev. 2018, 14, 171–179. [Google Scholar] [CrossRef]
- Wąsik, M.; Nazimek, K.; Nowak, B.; Askenase, P.W.; Bryniarski, K. Delayed-Type Hypersensitivity Underlying Casein Allergy Is Suppressed by Extracellular Vesicles Carrying miRNA-150. Nutrients 2019, 11, 907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, H.A.; O’Mahony, L.; Burks, A.W.; Plaut, M.; Lack, G.; Akdis, C.A. Mechanisms of food allergy. J. Allergy Clin. Immunol. 2018, 141, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, D.H.; Igyártó, B.Z.; Gaspari, A.A. Early immune events in the induction of allergic contact dermatitis. Nat. Rev. Immunol. 2012, 12, 114–124. [Google Scholar] [CrossRef]
- Kim, J.H.; Hu, Y.; Yongqing, T.; Kim, J.; Hughes, V.A.; Le Nours, J.; Marquez, E.A.; Purcell, A.W.; Wan, Q.; Sugita, M.; et al. CD1a on Langerhans cells controls inflammatory skin disease. Nat. Immunol. 2016, 17, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Casorati, G.; Dellabona, P. Of self-lipids, CD1-restricted T cells, and contact sensitization. Eur. J. Immunol. 2017, 47, 1119–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betts, R.J.; Perkovic, A.; Mahapatra, S.; Del Bufalo, A.; Camara, K.; Howell, A.R.; Martinozzi Teissier, S.; De Libero, G.; Mori, L. Contact sensitizers trigger human CD1-autoreactive T-cell responses. Eur. J. Immunol. 2017, 47, 1171–1180. [Google Scholar] [CrossRef] [Green Version]
- Nicolai, S.; Wegrecki, M.; Cheng, T.Y.; Bourgeois, E.A.; Cotton, R.N.; Mayfield, J.A.; Monnot, G.C.; Le Nours, J.; van Rhijn, I.; Rossjohn, J.; et al. Human T cell response to CD1a and contact dermatitis allergens in botanical extracts and commercial skin care products. Sci. Immunol. 2020, 5, eaax5430. [Google Scholar] [CrossRef]
- Nguyen, H.L.; Yiannias, J.A. Contact Dermatitis to Medications and Skin Products. Clin. Rev. Allergy Immunol. 2019, 56, 41–59. [Google Scholar] [CrossRef]
- Arias, Á.; Lucendo, A.J. Molecular basis and cellular mechanisms of eosinophilic esophagitis for the clinical practice. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 99–117. [Google Scholar] [CrossRef]
- Noguchi, E.; Akiyama, M.; Yagami, A.; Hirota, T.; Okada, Y.; Kato, Z.; Kishikawa, R.; Fukutomi, Y.; Hide, M.; Morita, E.; et al. HLA-DQ and RBFOX1 as susceptibility genes for an outbreak of hydrolyzed wheat allergy. J. Allergy Clin. Immunol. 2019, 144, 1354–1363. [Google Scholar] [CrossRef] [Green Version]
- Carter, C.A.; Frischmeyer-Guerrerio, P.A. The Genetics of Food Allergy. Curr. Allergy Asthma Rep. 2018, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Asai, Y.; Eslami, A.; van Ginkel, C.D.; Akhabir, L.; Wan, M.; Ellis, G.; Ben-Shoshan, M.; Martino, D.; Ferreira, M.A.; Allen, K.; et al. Genome-wide association study and meta-analysis in multiple populations identifies new loci for peanut allergy and establishes C11orf30/EMSY as a genetic risk factor for food allergy. J. Allergy Clin. Immunol. 2018, 141, 991–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashley, S.E.; Tan, H.T.; Peters, R.; Allen, K.J.; Vuillermin, P.; Dharmage, S.C.; Tang, M.L.K.; Koplin, J.; Lowe, A.; Ponsonby, A.L.; et al. Genetic variation at the Th2 immune gene IL13 is associated with IgE-mediated paediatric food allergy. Clin. Exp. Allergy 2017, 47, 1032–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.H.; Song, Y.; Wu, W.; Yu, K.; Zhang, G. The gut microbiota, environmental factors, and links to the development of food allergy. Clin. Mol. Allergy 2020, 18, 5. [Google Scholar] [CrossRef]
- Marrs, T.; Logan, K.; Craven, J.; Radulovic, S.; McLean, W.H.A.I.; Lack, G.; Flohr, C.; Perkin, M.R. EAT Study Team. Dog ownership at three months of age is associated with protection against food allergy. Allergy 2019, 74, 2212. [Google Scholar] [CrossRef] [PubMed]
- Metzler, S.; Frei, R.; Schmaußer-Hechfellner, E.; von Mutius, E.; Pekkanen, J.; Karvonen, A.M.; Kirjavainen, P.V.; Dalphin, J.C.; Divaret-Chauveau, A.; Riedler, J.; et al. PASTURE/EFRAIM study group. Association between antibiotic treatment during pregnancy and infancy and the development of allergic diseases. Pediatric Allergy Immunol. 2019, 30, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, M.; Peters, R.L.; Koplin, J.J.; Field, M.J.; McWilliam, V.; Sawyer, S.M.; Vuillermin, P.J.; Pezic, A.; Gurrin, L.C.; Douglass, J.A.; et al. Risk Factors for Food Allergy in Early Adolescence: The SchoolNuts Study. J. Allergy Clin. Immunol. Pract. 2018, 6, 496–505. [Google Scholar] [CrossRef]
- Mitselou, N.; Hallberg, J.; Stephansson, O.; Almqvist, C.; Melén, E.; Ludvigsson, J.F. Cesarean delivery, preterm birth, and risk of food allergy: Nationwide Swedish cohort study of more than 1 million children. J. Allergy Clin. Immunol. 2018, 142, 1510–1514.e2. [Google Scholar] [CrossRef] [Green Version]
- Hennessy, Á.; Hourihane, J.O.; Malvisi, L.; Irvine, A.D.; Kenny, L.C.; Murray, D.M.; Kiely, M.E. Antenatal vitamin D exposure and childhood eczema, food allergy, asthma and allergic rhinitis at 2 and 5 years of age in the atopic disease-specific Cork BASELINE Birth Cohort Study. Allergy 2018, 73, 2182–2191. [Google Scholar] [CrossRef]
- DeMuth, K.; Stecenko, A.; Sullivan, K.; Fitzpatrick, A. Relationship between treatment with antacid medication and the prevalence of food allergy in children. Allergy Asthma Proc. 2013, 34, 227–232. [Google Scholar] [CrossRef]
- Silva, C.M.; Silva, S.A.D.; Antunes, M.M.C.; Silva, G.A.P.D.; Sarinho, E.S.C.; Brandt, K.G. Do infants with cow’s milk protein allergy have inadequate levels of vitamin D? J. Pediatr. 2017, 93, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.H.; Matsui, E.C.; Wood, R.A.; Keet, C.A. Urinary levels of triclosan and parabens are associated with aeroallergen and food sensitization. J. Allergy Clin. Immunol. 2012, 130, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Shu, S.A.; Yuen, A.W.T.; Woo, E.; Chu, K.H.; Kwan, H.S.; Yang, G.X.; Yang, Y.; Leung, P.S.C. Microbiota and Food Allergy. Clin. Rev. Allergy Immunol. 2019, 57, 83–97. [Google Scholar] [CrossRef] [PubMed]
- Feehley, T.; Plunkett, C.H.; Bao, R.; Choi Hong, S.M.; Culleen, E.; Belda-Ferre, P.; Campbell, E.; Aitoro, R.; Nocerino, R.; Paparo, L.; et al. Healthy infants harbor intestinal bacteria that protect against food allergy. Nat. Med. 2019, 25, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, B.; Novak, N. Effects of daily food processing on allergenicity. Crit. Rev. Food Sci. Nutr. 2019, 59, 31–42. [Google Scholar] [CrossRef]
- Meng, S.; Li, J.; Chang, S.; Maleki, S.J. Quantitative and kinetic analyses of peanut allergens as affected by food processing. Food Chem. X 2019, 1, 100004. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, Z.; Li, K.; Li, X.; Yang, A.; Tong, P.; Chen, H. Allergenicity assessment on thermally processed peanut influenced by extraction and assessment methods. Food Chem. 2019, 281, 130–139. [Google Scholar] [CrossRef]
- Zhang, T.; Shi, Y.; Zhao, Y.; Tang, G.; Niu, B.; Chen, Q. Boiling and roasting treatment affecting the peanut allergenicity. Ann. Transl. Med. 2018, 6, 357. [Google Scholar] [CrossRef]
- Ortiz, T.; Para, R.; Gonipeta, B.; Reitmeyer, M.; He, Y.; Srkalovic, I.; Ng, P.K.; Gangur, V. Effect of extrusion processing on immune activation properties of hazelnut protein in a mouse model. Int. J. Food Sci. Nutr. 2016, 67, 660–669. [Google Scholar] [CrossRef]
- Verhoeckx, K.C.M.; Vissers, Y.M.; Baumert, J.L.; Faludi, R.; Feys, M.; Flanagan, S.; Herouet-Guicheney, C.; Holzhauser, T.; Shimojo, R.; van der Bolt, N.; et al. Food processing and allergenicity. Food Chem. Toxicol. 2015, 80, 223–240. [Google Scholar] [CrossRef]
- Blanc, F.; Vissers, Y.M.; Adel-Patient, K.; Rigby, N.M.; Mackie, A.R.; Gunning, A.P.; Wellner, N.K.; Skov, P.S.; Przybylski-Nicaise, L.; Ballmer-Weber, B.; et al. Boiling peanut Ara h 1 results in the formation of aggregates with reduced allergenicity. Mol. Nutr. Food Res. 2011, 55, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Kulis, M. Hypoallergenic Proteins for the Treatment of Food Allergy. Curr. Allergy Asthma Rep. 2019, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Maslin, K.; Fox, A.T.; Chambault, M.; Meyer, R. Palatability of hypoallergenic formulas for cow’s milk allergy and healthcare professional recommendation. Pediatr. Allergy Immunol. 2018, 29, 857–862. [Google Scholar] [CrossRef]
- Palladino, C.; Breiteneder, H. Peanut allergens. Mol. Immunol. 2018, 100, 58–70. [Google Scholar] [CrossRef] [PubMed]
- Kohno, K.; Takahashi, H.; Endo, T.R.; Matsuo, H.; Shiwaku, K.; Morita, E. Characterization of a hypoallergenic wheat line lacking ω-5 gliadin. Allergol. Int. 2016, 65, 400–405. [Google Scholar] [CrossRef] [Green Version]
- Gao, H.; Jin, Y.; Jian, D.I.; Olson, E.; Ng, P.K.W.; Gangur, V. Development and validation of a mouse-based primary screening method for testing relative allergenicity of proteins from different wheat genotypes. J. Immunol. Methods 2019, 464, 95–104. [Google Scholar] [CrossRef]
- Gonipeta, B.; Kim, E.; Gangur, V. Mouse models of food allergy: How well do they simulate the human disorder? Crit. Rev. Food Sci. Nutr. 2015, 55, 437–452. [Google Scholar] [CrossRef]
- Shaker, D. An Analysis of “Natural” Food Litigation to Build a Sesame Allergy Consumer Class Action. Food Drug Law J. 2017, 72, 103–140. [Google Scholar]
- Blom, W.M.; Michelsen-Huisman, A.D.; van Os-Medendorp, H.; van Duijn, G.; de Zeeuw-Brouwer, M.L.; Versluis, A.; Castenmiller, J.J.M.; Noteborn, H.P.J.M.; Kruizinga, A.G.; Knulst, A.C.; et al. Accidental food allergy reactions: Products and undeclared ingredients. J. Allergy Clin. Immunol. 2018, 142, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Caminiti, L.; Vita, D.; Passalacqua, G.; Arrigo, T.; Barberi, S.; Lombardo, F.; Pajno, G.B. Tahini, a little known sesame-containing food, as an unexpected cause of severe allergic reaction. J. Investig. Allergol. Clin. Immunol. 2006, 16, 308–310. [Google Scholar]
- Reese, I.; Holzhauser, T.; Schnadt, S.; Dölle, S.; Kleine-Tebbe, J.; Raithel, M.; Worm, M.; Zuberbier, T.; Vieths, S. Allergen and allergy risk assessment, allergen management, and gaps in the European Food Information Regulation (FIR): Are allergic consumers adequately protected by current statutory food safety and labeling regulations? Allergo J. Int. 2015, 24, 180–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segal, L.; Ben-Shoshan, M.; Alizadehfar, R.; Primeau, M.N.; Asai, Y.; Killorn, K.R.; Chan, E.; Cheuk, S.; Shand, G.; St-Pierre, Y.; et al. Initial and accidental reactions are managed inadequately in children with sesame allergy. J. Allergy Clin. Immunol. Pract. 2017, 5, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L.; Baumert, J.L. Worldwide food allergy labeling and detection of allergens in processed foods. Chem. Immunol. Allergy 2015, 101, 227–234. [Google Scholar] [PubMed]
- Eberlein-König, B.; Rueff, F.; Przybilla, B. Generalized urticaria caused by sesame seeds with negative prick test results and without demonstrable specific IgE antibodies. J. Allergy Clin. Immunol. 1995, 96, 560–561. [Google Scholar] [CrossRef]
- Kanny, G.; De Hauteclocque, C.; Moneret-Vautrin, D.A. Sesame seed and sesame seed oil contain masked allergens of growing importance. Allergy 1996, 51, 952–957. [Google Scholar] [CrossRef] [PubMed]
- Kolopp-Sarda, M.N.; Moneret-Vautrin, D.A.; Gobert, B.; Kanny, G.; Brodschii, M.; Bene, M.C.; Faure, G.C. Specific humoral immune responses in 12 cases of food sensitization to sesame seed. Clin. Exp. Allergy 1997, 27, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- Remington, B.C.; Westerhout, J.; Meima, M.Y.; Blom, W.M.; Kruizinga, A.G.; Wheeler, M.W.; Taylor, S.L.; Houben, G.F.; Baumert, J.L. Updated population minimal eliciting dose distributions for use in risk assessment of 14 priority food allergens. Food Chem. Toxicol. 2020, 139, 111259. [Google Scholar] [CrossRef]
- Kuroyama, M.; Kagawa, H.; Kitada, S.; Maekura, R.; Mori, M.; Hirano, H. Exogenous lipoid pneumonia caused by repeated sesame oil pulling: A report of two cases. BMC Pulm. Med. 2015, 15, 135. [Google Scholar] [CrossRef] [Green Version]
- Veysman, B.; Vlahos, I.; Oshva, L. Pneumonitis and eosinophilia after in vitro fertilization treatment. Ann. Emerg. Med. 2006, 47, 472–475. [Google Scholar] [CrossRef]
- Phy, J.L.; Weiss, W.T.; Weiler, C.R.; Damario, M.A. Hypersensitivity to progesterone-in-oil after in vitro fertilization and embryo transfer. Fertil. Steril. 2003, 80, 1272–1275. [Google Scholar] [CrossRef]
- Bouckaert, Y.; Robert, F.; Englert, Y.; De Backer, D.; De Vuyst, P.; Delbaere, A. Acute eosinophilic pneumonia associated with intramuscular administration of progesterone as luteal phase support after IVF: Case report. Hum. Reprod. 2004, 19, 1806–1810. [Google Scholar] [CrossRef] [PubMed]
- Darsow, U.; Bruckbauer, H.; Worret, W.I.; Hofmann, H.; Ring, J. Subcutaneous oleomas induced by self-injection of sesame seed oil for muscle augmentation. J. Am. Acad. Dermatol. 2000, 42 Pt 1, 292–294. [Google Scholar] [CrossRef]
- Khankhanian, N.K.; Hammers, Y.A.; Kowalski, P. Exuberant local tissue reaction to intramuscular injection of nandrolone decanoate (Deca-Durabolin)—A steroid compound in a sesame seed oil base--mimicking soft tissue malignant tumors: A case report and review of the literature. Mil. Med. 1992, 157, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.; Wüthrich, B. Non-IgE-mediated anaphylaxis to sesame. Allergy 1998, 53, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Cano, R.; Picado, C.; Valero, A.; Bartra, J. Mechanisms of Anaphylaxis Beyond IgE. J. Investig. Allergol. Clin. Immunol. 2016, 26, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Marchisotto, M.J.; Harada, L.; Kamdar, O.; Smith, B.M.; Waserman, S.; Sicherer, S.; Allen, K.; Muraro, A.; Taylor, S.; Gupta, R.S. Food Allergen Labeling and Purchasing Habits in the United States and Canada. J. Allergy Clin. Immunol. Pract. 2017, 5, 345–351.e2. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sesame allergy: diversity of the allergens and the complex disease spectrum. The brown, white, and black sesame seeds contain protein allergens, lipid allergens, and allergens of unknown nature. Current evidence shows that sesame is linked to at least five types of clinical presentation of diseases (from left to right): non-IgE immediate hypersensitivity to oil, delayed hypersensitivity to lipid allergens, IgE mediated immediate hypersensitivity to protein allergens, and acute food protein-induced enterocolitis syndrome, and eosinophilic esophagitis caused by unknown allergens.
Figure 1.
Sesame allergy: diversity of the allergens and the complex disease spectrum. The brown, white, and black sesame seeds contain protein allergens, lipid allergens, and allergens of unknown nature. Current evidence shows that sesame is linked to at least five types of clinical presentation of diseases (from left to right): non-IgE immediate hypersensitivity to oil, delayed hypersensitivity to lipid allergens, IgE mediated immediate hypersensitivity to protein allergens, and acute food protein-induced enterocolitis syndrome, and eosinophilic esophagitis caused by unknown allergens.

Figure 2.
Mechanism of IgE mediated immediate hypersensitivity reaction elicited by sesame seed protein allergens: Type I Hypersensitivity. This happens in two phases. (1) the sensitization phase: exposure to sesame protein allergens results in their uptake by the antigen presenting cells (APCs). The APCs process and present the allergen peptide fragments along with the Major Histocompatibility Complex (MHC) class II molecules to the allergen specific naïve T cells. With the help of the costimulatory molecules and the local cytokines (e.g., IL-4), they differentiate to become T helper (Th)-2 cells. These cells help the allergen specific B cells to produce IgE antibodies. The B cells become plasma cells and secrete large amounts of IgE antibodies that are distributed systemically and picked up by the mast cells and the basophils, which express high affinity receptor for IgE. At this stage, the subject is considered ‘sensitized to sesame’ but has no apparent clinical symptoms of the disease; and (2) the disease elicitation phase: re-exposure of the sensitized subject to the sesame allergen results in direct binding of the allergen fragments to the IgE present on mast cells and basophils. Cross-linking of the surface IgE receptor results in cellular activation, degranulation, and release of mediators resulting in the clinical expression of the disease within minutes to 3 h after exposure to the protein allergens. Therefore, this disease is known as immediate hypersensitivity reaction.
Figure 2.
Mechanism of IgE mediated immediate hypersensitivity reaction elicited by sesame seed protein allergens: Type I Hypersensitivity. This happens in two phases. (1) the sensitization phase: exposure to sesame protein allergens results in their uptake by the antigen presenting cells (APCs). The APCs process and present the allergen peptide fragments along with the Major Histocompatibility Complex (MHC) class II molecules to the allergen specific naïve T cells. With the help of the costimulatory molecules and the local cytokines (e.g., IL-4), they differentiate to become T helper (Th)-2 cells. These cells help the allergen specific B cells to produce IgE antibodies. The B cells become plasma cells and secrete large amounts of IgE antibodies that are distributed systemically and picked up by the mast cells and the basophils, which express high affinity receptor for IgE. At this stage, the subject is considered ‘sensitized to sesame’ but has no apparent clinical symptoms of the disease; and (2) the disease elicitation phase: re-exposure of the sensitized subject to the sesame allergen results in direct binding of the allergen fragments to the IgE present on mast cells and basophils. Cross-linking of the surface IgE receptor results in cellular activation, degranulation, and release of mediators resulting in the clinical expression of the disease within minutes to 3 h after exposure to the protein allergens. Therefore, this disease is known as immediate hypersensitivity reaction.
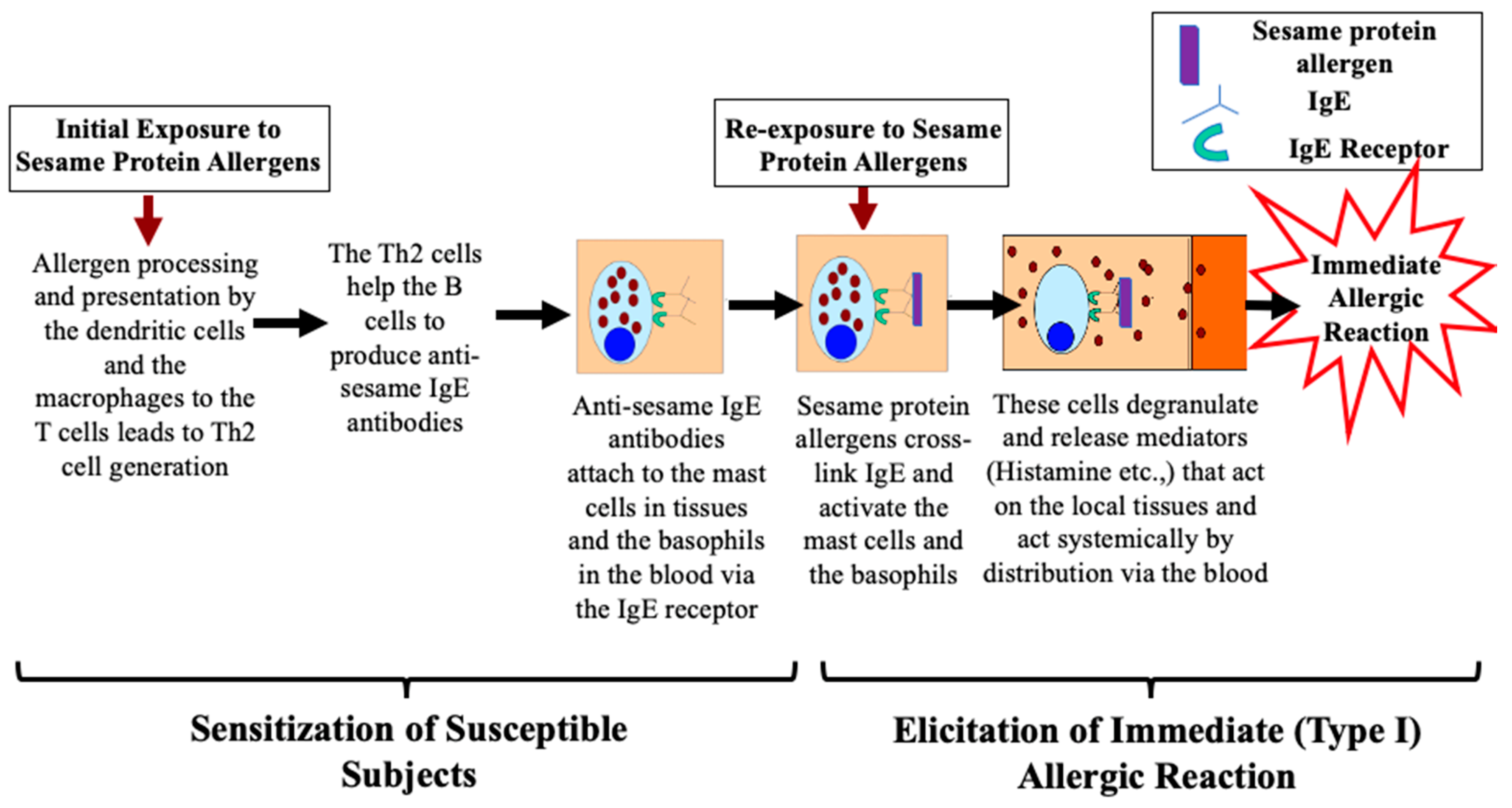
Figure 3.
Mechanism of delayed hypersensitivity reactions elicited by sesame lipid allergens: a plausible model. This happens in two phases. (1) the sensitization phase: exposure to sesame lipid allergens results in their uptake by the antigen presenting cells (APCs). They present the lipid allergen along with the non-classical MHC molecule, CD1a, to the allergen specific naïve T cells that differentiate to become the effector T (ET) cells and memory T (MT) cells. There are no disease symptoms at this phase; and (2) the disease elicitation phase: re-exposure of the sensitized subjects to the sesame lipid allergen results in their uptake and presentation by the APCs (along with the CD1a?) to the ET and MT cells resulting in their activation. The MT cells differentiate to become ET cells. Activated ET cells release cytokines and chemokines that cause recruitment of additional immune cells to the local tissue. The consequent tissue damage from all these processes occurs in about 48–72 h after exposure to the lipid allergen and, therefore, it is known as the delayed hypersensitivity reaction.
Figure 3.
Mechanism of delayed hypersensitivity reactions elicited by sesame lipid allergens: a plausible model. This happens in two phases. (1) the sensitization phase: exposure to sesame lipid allergens results in their uptake by the antigen presenting cells (APCs). They present the lipid allergen along with the non-classical MHC molecule, CD1a, to the allergen specific naïve T cells that differentiate to become the effector T (ET) cells and memory T (MT) cells. There are no disease symptoms at this phase; and (2) the disease elicitation phase: re-exposure of the sensitized subjects to the sesame lipid allergen results in their uptake and presentation by the APCs (along with the CD1a?) to the ET and MT cells resulting in their activation. The MT cells differentiate to become ET cells. Activated ET cells release cytokines and chemokines that cause recruitment of additional immune cells to the local tissue. The consequent tissue damage from all these processes occurs in about 48–72 h after exposure to the lipid allergen and, therefore, it is known as the delayed hypersensitivity reaction.

Figure 4.
Directions for the future basic and translational research on sesame allergy. Advances in basic and translational (preclinical and clinical) research on sesame allergies are urgently needed because the prevalence and the severity of sesame allergies are growing at an alarming rate globally. This figure shows major directions for conducting future studies using both human and nonhuman (animal, cell line, plant) systems as illustrated.
Figure 4.
Directions for the future basic and translational research on sesame allergy. Advances in basic and translational (preclinical and clinical) research on sesame allergies are urgently needed because the prevalence and the severity of sesame allergies are growing at an alarming rate globally. This figure shows major directions for conducting future studies using both human and nonhuman (animal, cell line, plant) systems as illustrated.
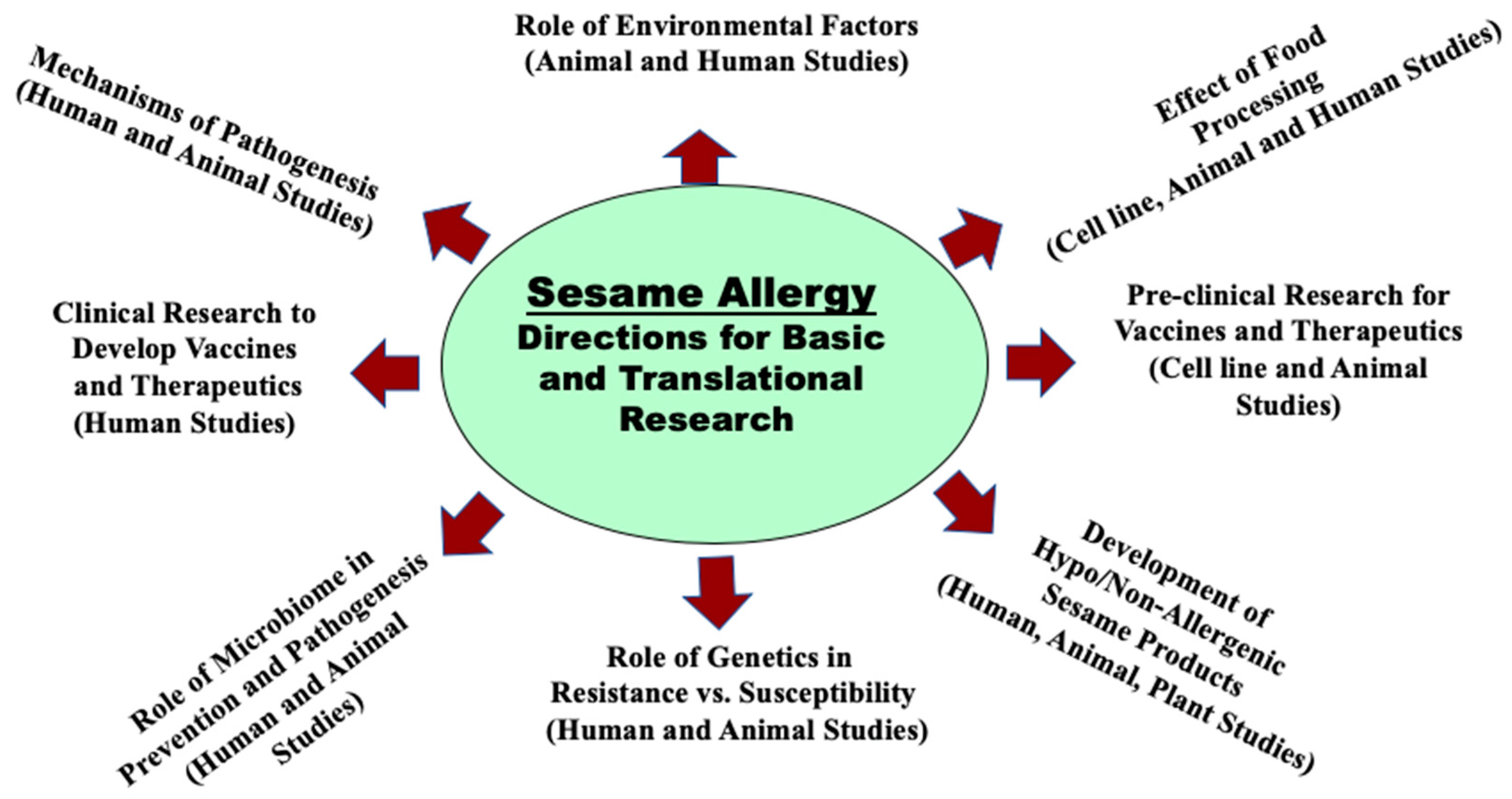

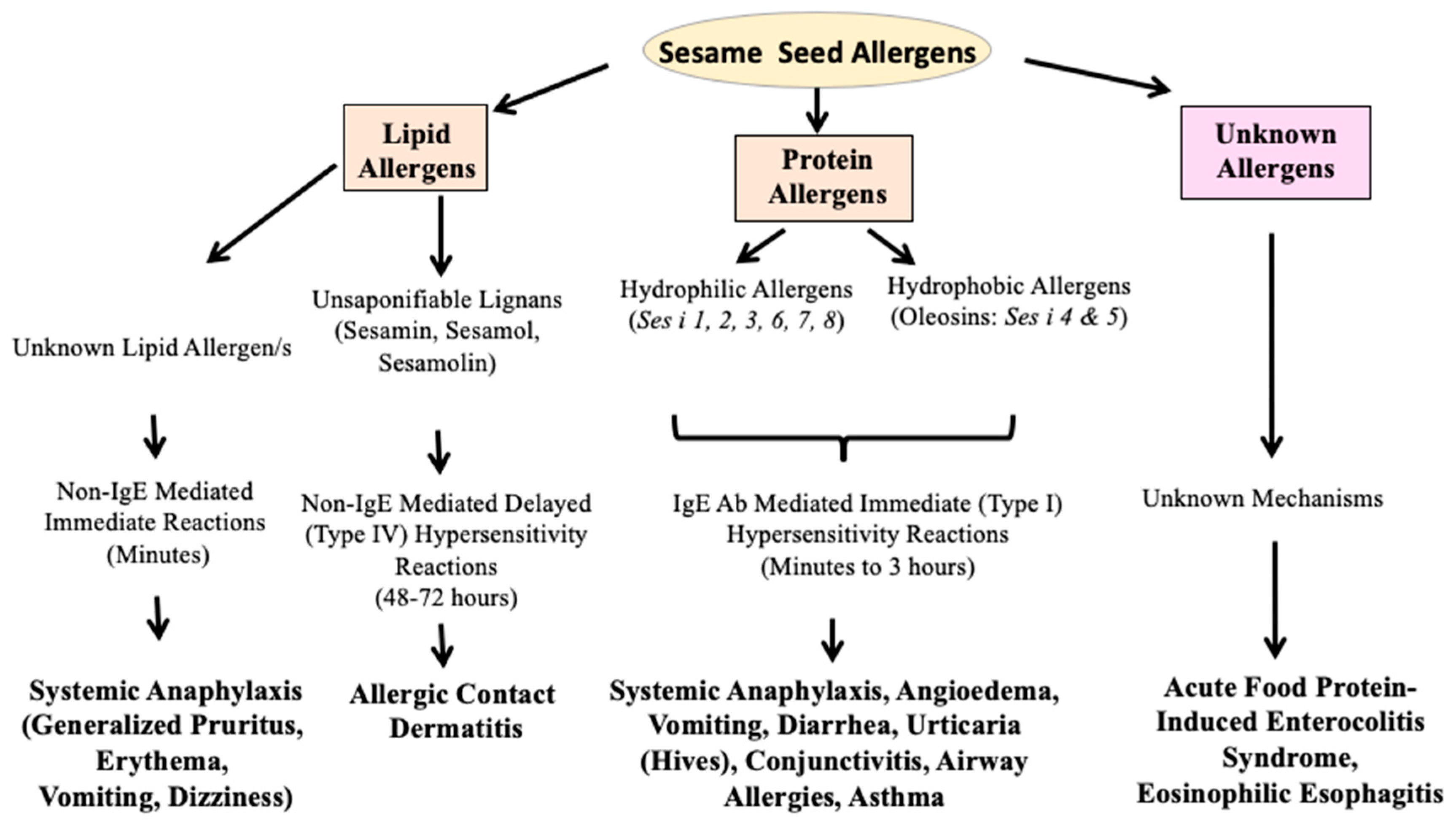{kind=link}
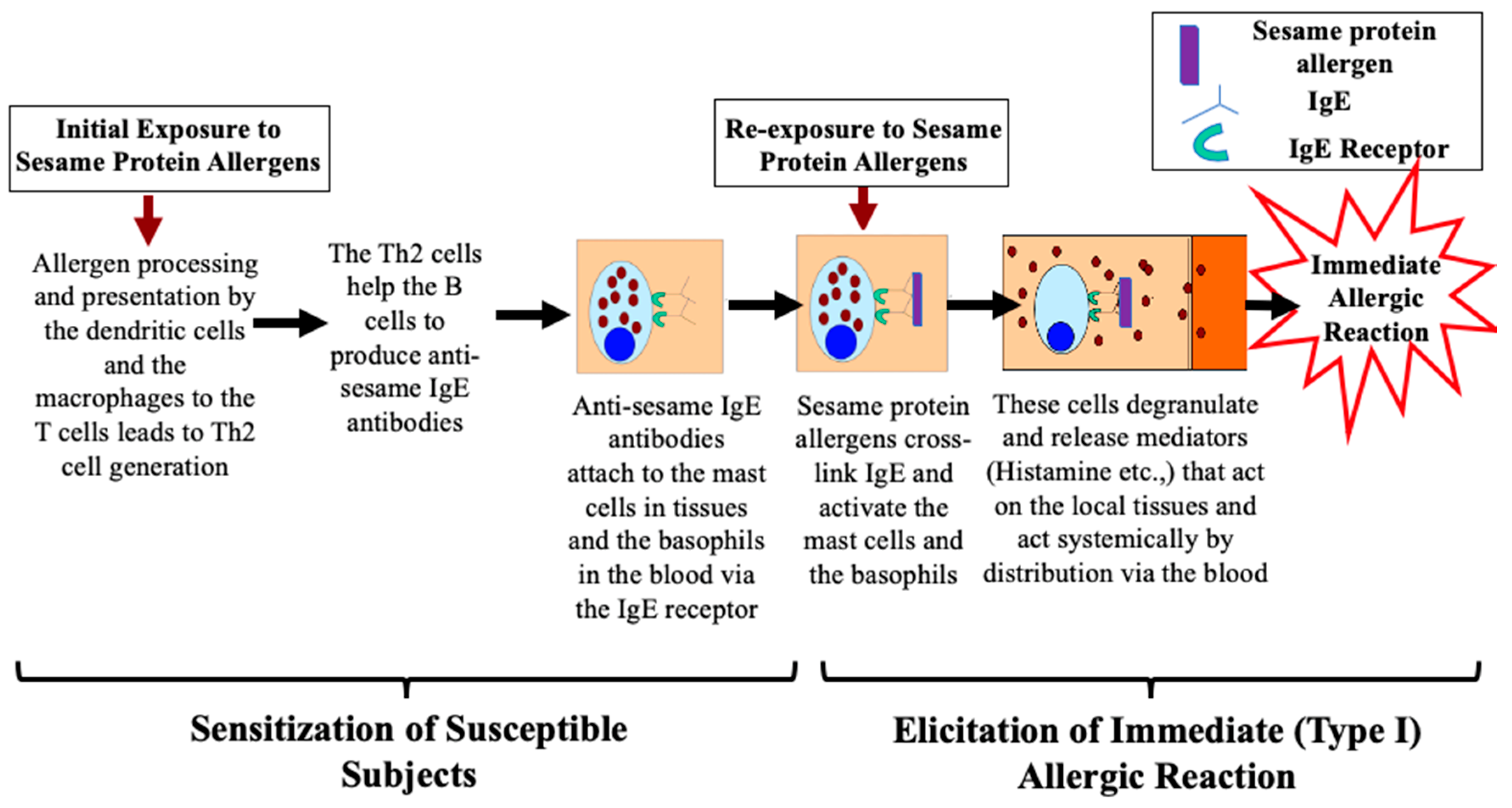{kind=link}
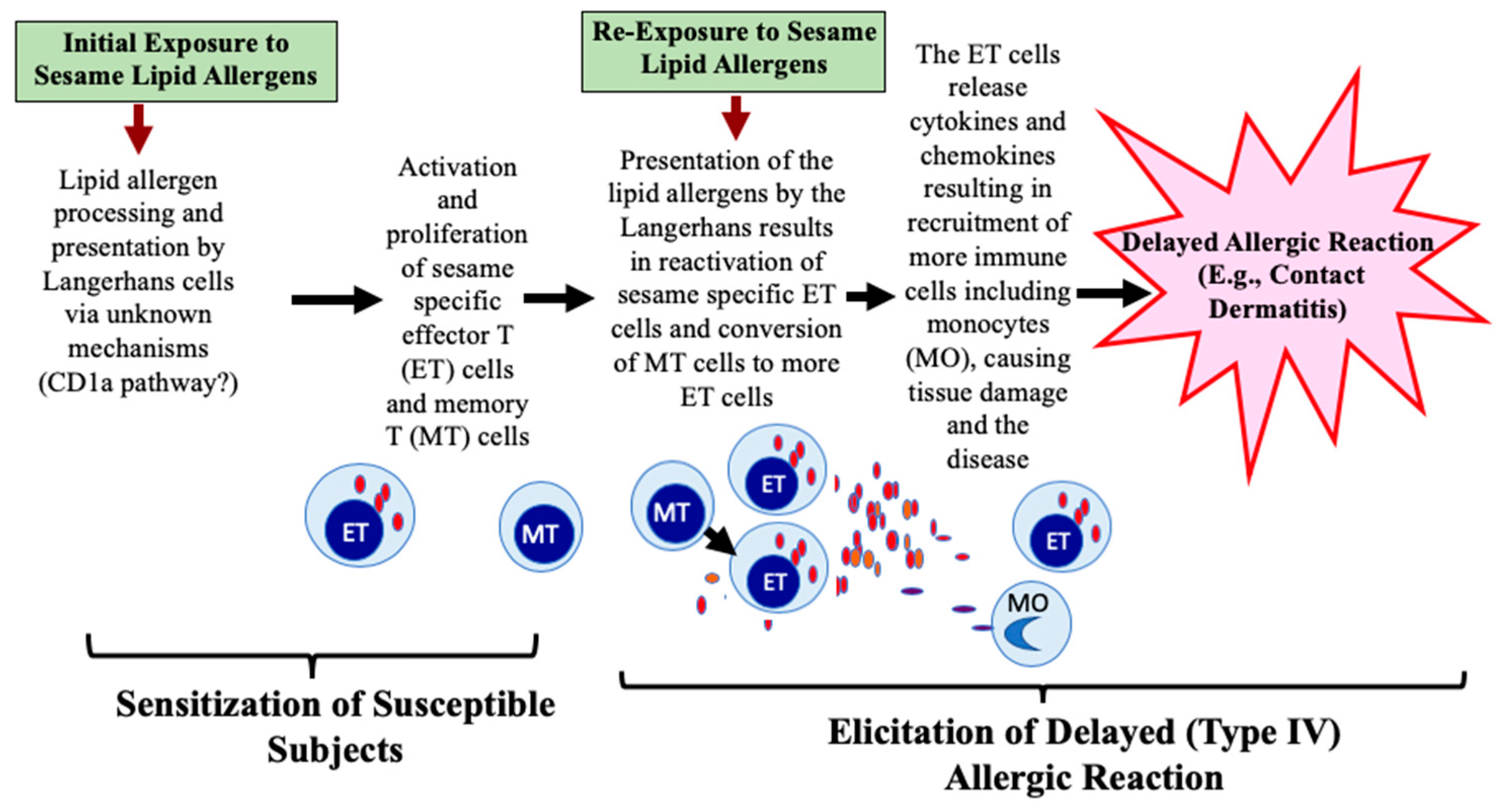{kind=link}
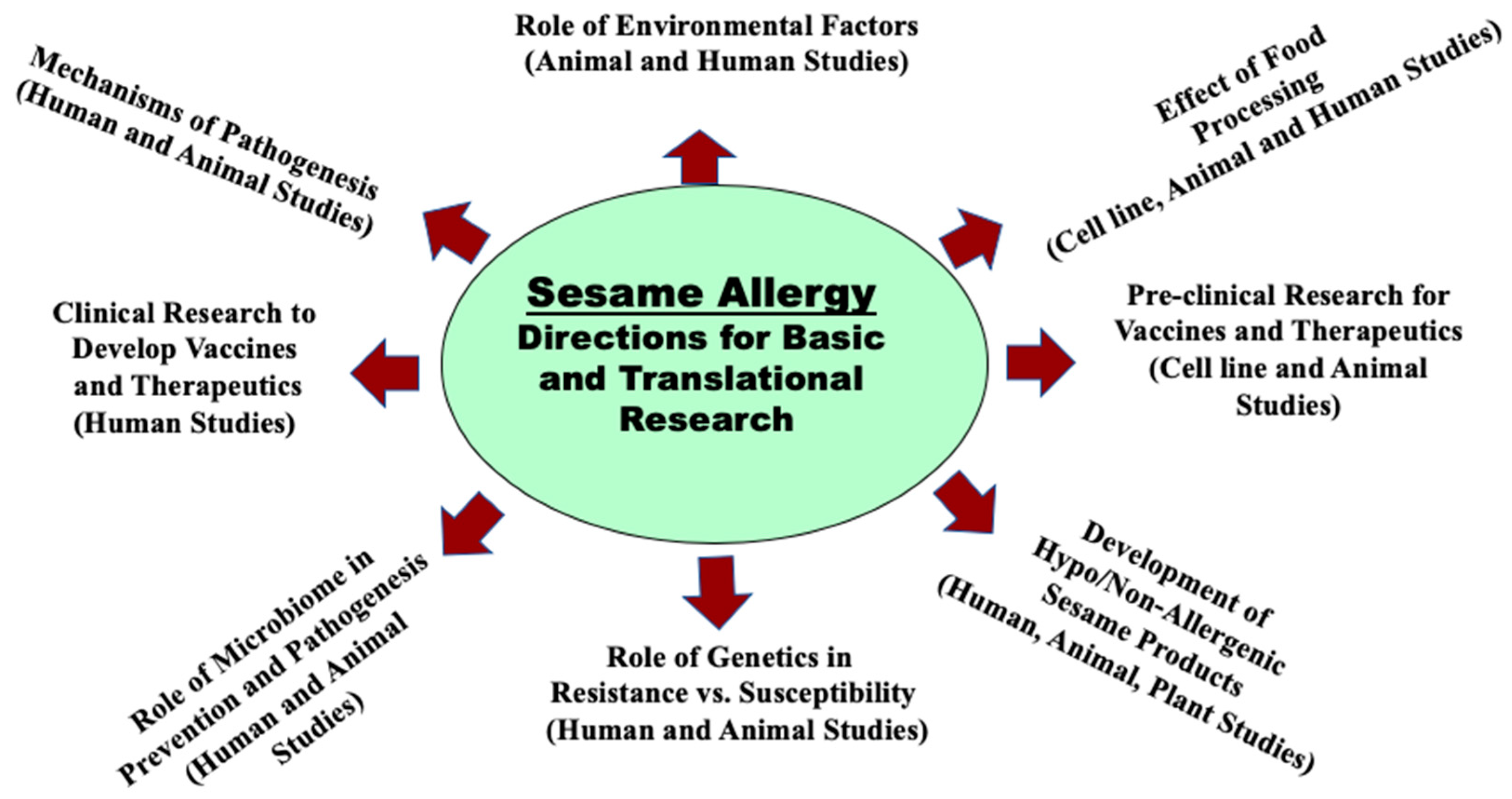{kind=link}
Table 1.
Food safety regulation of sesame and other allergenic foods.
| Country | List of Federally Regulated Allergenic Foods |
|---|---|
| USA | 8 foods: wheat, milk, soybean, egg, peanut, tree nuts, fish, and crustacean shellfish # (sesame is not federally regulated). |
| Canada | 12 foods: wheat and triticale (hybrid of wheat and rye grains), milk, soy, egg, peanut, tree nuts, fish, shellfish (crustaceans, mollusks *), sesame, mustard, sulfites. |
| European Union ** & UK | 14 foods: Cereals that contain gluten including wheat, rye, barley and oats, milk, soy, egg, fish, shellfish (crustaceans including prawns, crabs, and lobsters, mollusks including mussels and oysters), peanut, tree nuts, sesame seed, mustard, sulfur dioxide, and sulfites, celery, lupine. |
| Australia & New Zealand | 10 foods: wheat, milk, soybean, egg, peanut, tree nuts, fish, shellfish (crustacean and mollusks), sesame, and lupine. |
| Japan | 7 foods: wheat, buckwheat, milk, egg, peanut, shrimp, and crab; Recommends manufacturers to display 20 additional foods: abalone, squid, salmon roe, orange, cashew nut, kiwi, beef, walnut, sesame, salmon, mackerel, soybean, chicken, banana, pork, matsutake mushroom, peach, yam, apple, and gelatin. |
# Examples of crustaceans: shrimp, crayfish, crab, and lobster. * Examples of mollusks: white clams, scallops, oysters, and mussels. ** European Union includes these 27 countries: Austria, Belgium, Bulgaria, Croatia, Republic of Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, Netherlands, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, and Sweden.
Table 2.
Global rise of sesame allergies: the origin and the milestones.
| Year | Milestone |
|---|---|
| 1950 | The first report, sesame seed allergy and anaphylaxis, USA [26]. |
| 1951 | The first report of asthma due to sesame, USA [27]. |
| 1958 | The first report, sesame oil allergic dermatitis (urticaria and rash upon injection), USA [28]. |
| 1975 | The first identification of sesamin, sesamol, and sesamolin as lipid allergens in contact dermatitis [29]. |
| 1981 | The first identification of sesame seed proteins of 8–62 kDa as protein allergens [30]. |
| 1991 | The first report of occupational (baker) allergy (dermatitis, asthma, rhinitis) to sesame seed [23]. |
| 1996 | The first prevalence study of sesame allergy in the UK general population, 0.05% [31]. |
| 1997 | The first prevalence study of sesame allergy in the pediatric population in Australia, 0.42% [32]. |
| 1999 | Sesame regulated by the European Union, Canada, Australia, and New Zealand [12,13,14,15]. |
| 2002 | The first report showing that the sesame allergy is more prevalent in Israel (0.18%) than peanut allergy (0.04%) [33]. |
| 2005 | The first report asking whether sesame allergy might be growing globally; concern on the absence of sesame regulation in the USA [18]. |
| 2006 | FALCPA 2004 Act implemented in USA; did not include sesame as a major allergen [11]. |
| 2006 | The first and the only animal model of sesame allergy and anaphylaxis [34]. |
| 2010 | The first report to show the population prevalence of sesame allergy in USA at 0.1% [35]. |
| 2011 | The first prevalence study of sesame allergy in Canada (children, 0.23%, adults, 0.05%) [36]. |
| 2011 | The first prevalence of sesame allergy in Lebanon (children, 2.6–3.9%, adults, 1.9%) [37]. |
| 2014 | 18 November, Citizen Petition by Center for Science in Public Interest asking the US FDA to regulate sesame as an allergen [38]. |
| 2015 | The first report that in Saudi Arabia, sesame was the third most common cause of anaphylaxis (22.7% of all anaphylaxis cases) [39]. |
| 2015 | The first study to show the prevalence of sesame allergy in Mexican adults (0.1%) [40] |
| 2017 | The first report that sesame anaphylaxis in Iran is common (children, 1.3%, adults, 9.3% of all anaphylaxis cases) [41]. |
| 2017 | The first study to show the prevalence of sesame allergy in Kuwait (young adults, 0.46%) [42]. |
| 2018 | 29 October, US FDA requests for public information on sesame allergy in the US [43]. |
| 2019 | A second study shows prevalence of sesame allergy in the USA at 0.23–0.49% [2]. |
| 2019 | 8 April, FASTER Act introduced in USA; it proposes to regulate sesame as an allergen [44]. |
| 2019 | Illinois (USA) enacts a new state law mandating sesame labeling on food packages [45]. |
| 2019 | NIH/USA study: 17% of food allergic children have sesame allergy [46]. |
| 2019 | NIH (USA) news release on the above story; highlights rising concerns on lack of sesame regulation in the USA [47]. |
| 2020 | The first report from Turkey: 20.2% of food allergic children have sesame allergy [48]. |
FASTER = Food Allergy Safety, Treatment, Education and Research; CFIA = Canadian Food Inspection Agency; NIH = National Institutes of Health; FALCPA = food allergen labeling and consumer protection act.
Table 3.
Protein and lipid allergens present in sesame seed: biochemical nature, diversity, and functions.
Table 3.
Protein and lipid allergens present in sesame seed: biochemical nature, diversity, and functions.
| Name | Biochemical Nature | Size (Da) | Solubility | Function |
|---|---|---|---|---|
| Ses i 1 | 2S Albumin | 9000 | Hydrophilic | Seed storage |
| Ses i 2 | 2S Albumin | 7000 | Hydrophilic | Seed storage |
| Ses i 3 | 7S Vicilin-like globulin | 45,000 | Hydrophilic | Seed storage |
| Ses i 4 | Oleosin | 17,000 | Hydrophobic | Oil-body structure |
| Ses i 5 | Oleosin | 15,000 | Hydrophobic | Oil-body structure |
| Ses i 6 | 11S Globulin | 52,000 | Hydrophilic | Seed storage |
| Ses i 7 | 11S Globulin | 57,000 | Hydrophilic | Seed storage |
| Ses i 8 * | Profilin | 14,000 | Hydrophilic | Actin-binding |
| Sesamin | Lipid allergen, lignan | 354 | Hydrophobic | Pro-antioxidant |
| Sesamol ** | Lipid allergen, lignan | 134 | Hydrophobic | Antioxidant |
| Sesamolin | Lipid allergen, lignan | 370 | Hydrophobic | Antioxidant |
* Not an official allergen of the International Union of Immunological Societies (IUIS) as yet. ** Sesamol is a thermally degraded product of Sesamolin.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gangur, V.; Acharya, H.G. The Global Rise and the Complexity of Sesame Allergy: Prime Time to Regulate Sesame in the United States of America? Allergies 2021, 1, 1-21. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1010001
AMA Style
Gangur V, Acharya HG. The Global Rise and the Complexity of Sesame Allergy: Prime Time to Regulate Sesame in the United States of America? Allergies. 2021; 1(1):1-21. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1010001
Chicago/Turabian StyleGangur, Venugopal, and Harini G. Acharya. 2021. "The Global Rise and the Complexity of Sesame Allergy: Prime Time to Regulate Sesame in the United States of America?" Allergies 1, no. 1: 1-21. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1010001