
Serum Concentrations of Antigen-Specific IgG4 in Patients with Japanese Cedar Pollinosis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Measurement Methods
Immunoglobulin Measurements
2.3. Assessment of Symptoms and Use of Medication
2.4. Statistical Analysis
3. Results
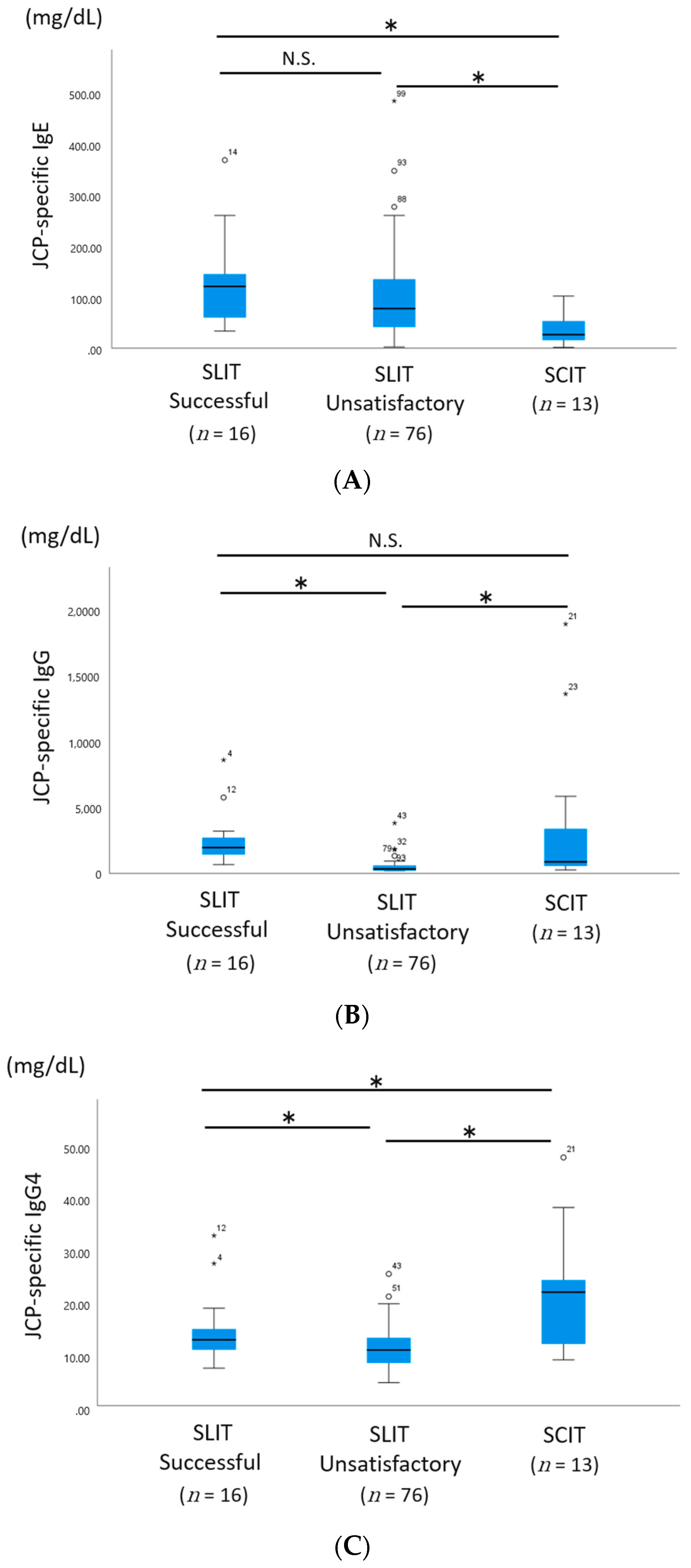
3.1. Serum JCP-Specific Levels of IgE, IgG, and IgG4
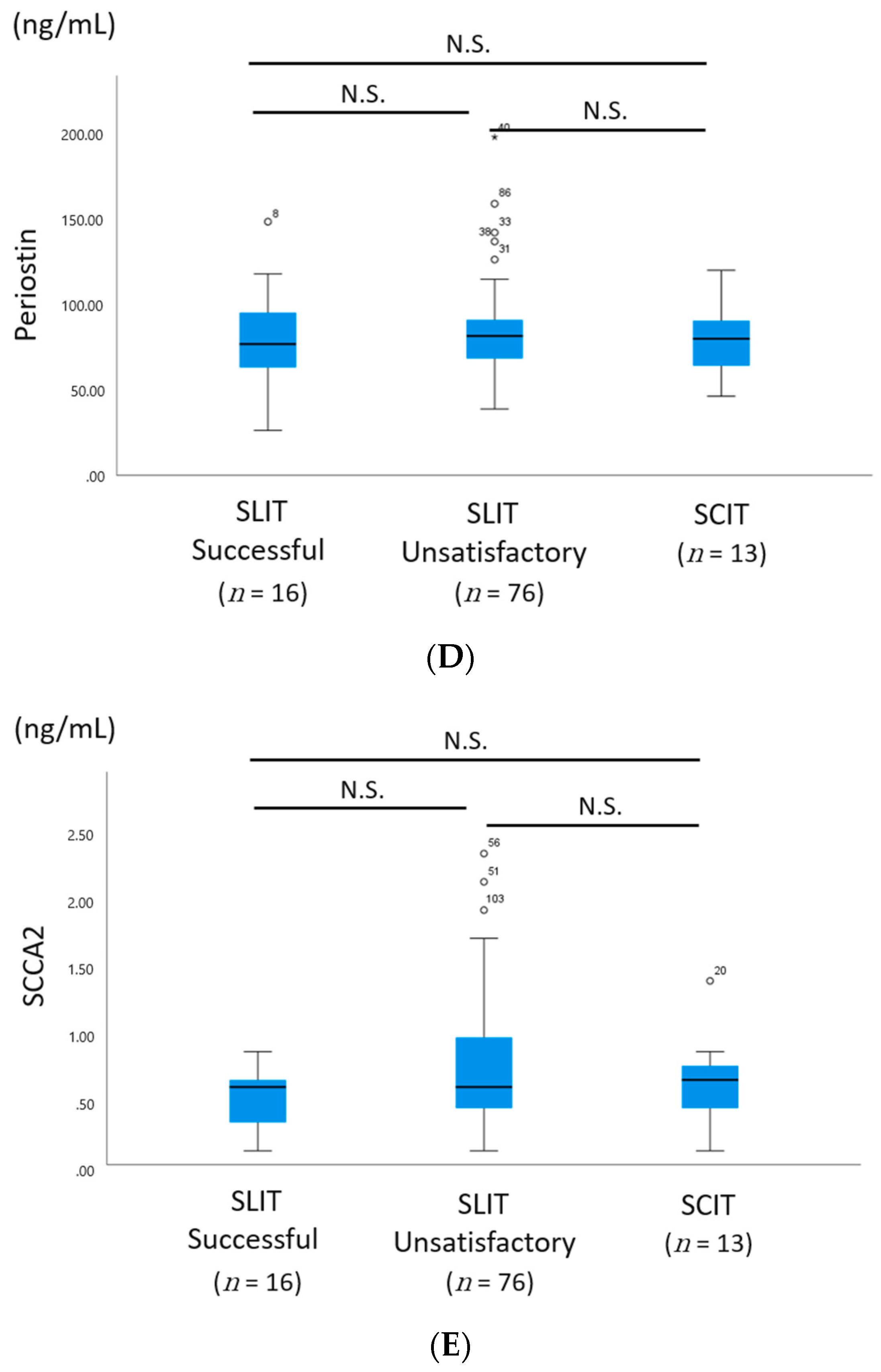
3.2. Serum Levels of Periostin and SCCA2
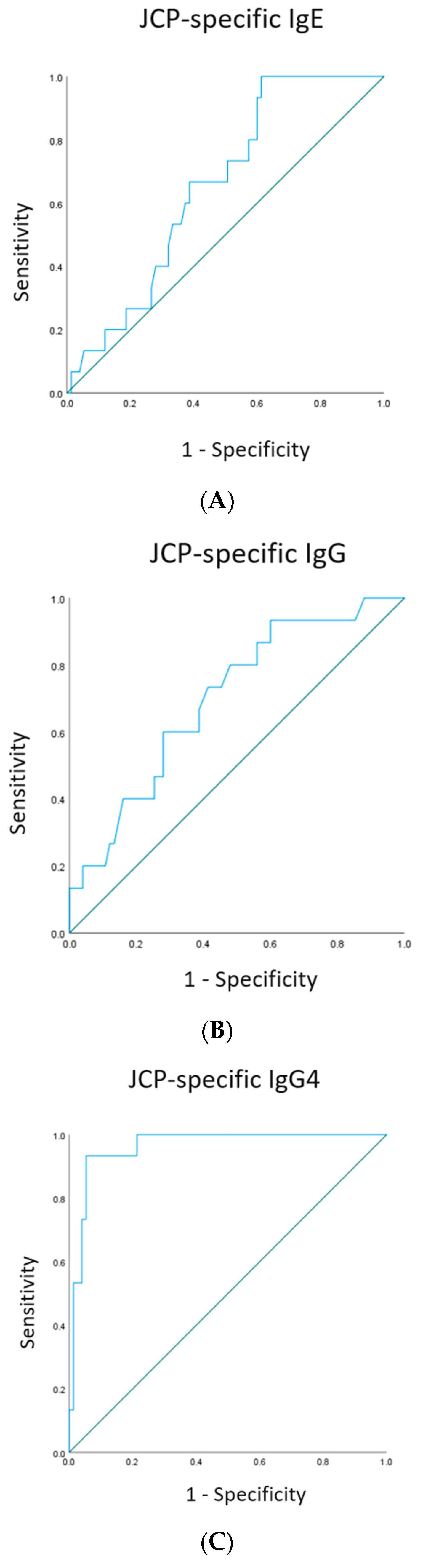
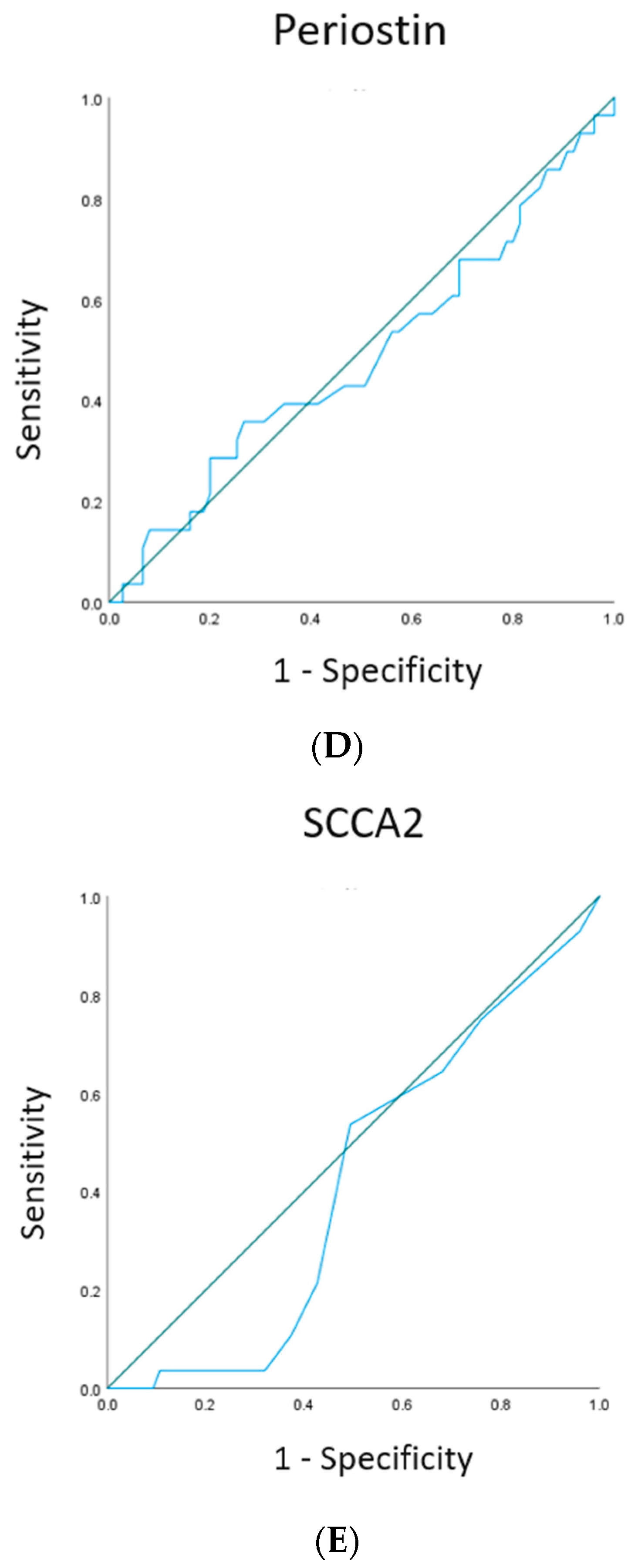
3.3. ROC Curves
4. Conclusions
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Masuyama, K.; Goto, M.; Takeno, S.; Ohta, N.; Okano, M.; Kamijo, A.; Suzuki, M.; Terada, T.; Sakurai, D.; Horiguchi, S.; et al. Guiding principles of sublingual immunotherapy for allergic rhinitis in Japanese patients. Auris Nasus Larynx 2016, 43, 1–9. [Google Scholar] [CrossRef]
- Kikuoka, H.; Kouzaki, H.; Matsumoto, K.; Arai, H.; Yamamoto, S.; Tojima, I.; Shimizu, S.; Miyashita, H.; Ogawa, Y.; Osada, T.; et al. Immunological effects of sublingual immunotherapy with Japanese cedar pollen extract in patients with combined Japanese cedar and Japanese cypress pollinosis. Clin. Immunol. 2019, 210, 108310. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, Y.; Okubo, K.; Yonekura, S.; Hashiguchi, K.; Goto, M.; Otsuka, T.; Murata, T.; Nakao, Y.; Kanazawa, C.; Nagakura, H.; et al. Efficacy and Safety of Sublingual Immunotherapy for Two Seasons in Patients with Japanese Cedar Pollinosis. Allergy Immunol. 2015, 166, 177–188. [Google Scholar] [CrossRef]
- Fujisawa, T.; Nago, M.; Hiaguchi, Y.; Hosoki, K.; Tokuda, R.; Usui, S.; Masuda, S.; Shinoda, M.; Hashiguchi, A.; Yamaguchi, M. Biomarkers for Allergen Immunotherapy in Cedar Pollinosis. Allergol. Int. 2009, 58, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Yonekura, S.; Okamoto, Y.; Sakurai, D.; Okubo, K.; Gotoh, M.; Kaneko, S.; Konno, A. An analysis of factors related to the effect of sublingual immunotherapy on Japanese cedar pollen induced allergic rhinitis. Allergol Int. 2018, 67, 201–208. [Google Scholar] [CrossRef]
- Ishida, A.; Ohta, N.; Suzuki, Y.; Kakehata, S.; Okubo, K.; Ikeda, H.; Shiraishi, H.; Izuhara, K. Expression of pendrin and periostin in allergic rhinitis and chronic rhinosinusitis. Allergol. Int. 2012, 61, 589–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagao, M.; Inagaki, S.; Kawano, T.; Azuma, Y.; Nomura, N.; Noguchi, Y.; Ohta, S.; Kawaguchi, A.; Odajima, H.; Ohya, Y.; et al. SCCA2 is a reliable biomarker for evaluating pediatric atopic dermatitis. J. Allergy Clin. Immunol. 2018, 141, 1934–1936. [Google Scholar] [CrossRef] [Green Version]
- Şahin, E.; Bafaqeeh, S.A.; Güven, S.G.; Çetinkaya, E.A.; Muluk, N.B.; Coşkun, Z.O.; Lopatin, A.; Kar, M.; Pinarbasli, M.O.; Cingi, C. Mechanism of action of allergen immunotherapy. Am. J. Rhinol. Allergy 2016, 30, 1–3. [Google Scholar] [CrossRef]
- Wachholz, P.A.; Soni, N.K.; Till, S.J.; Durham, S.R. Inhibition of allergen-IgE binding to B cells by IgG antibodies after grass pollen immunotherapy. J. Allergy Clin. Immunol. 2003, 112, 915–922. [Google Scholar] [CrossRef]
- Shamji, M.H.; Ljørring, C.; Francis, J.N.; Calderon, M.; Larche, M.; Kimber, I.; Frew, A.J.; Ipsen, H.; Lund, K.; Würtzen, P.A.; et al. Functional rather than immunoreactive levels of IgG4 correlate closely with clinical response to grass pollen immunotherapy. Allergy 2012, 67, 217–226. [Google Scholar] [CrossRef]
- Horiguchi, S.; Okamoto, Y.; Yonekura, S.; Okawa, T.; Yamamoto, H.; Kunii, N.; Sakurai, D.; Fujimura, T.; Nakazawa, K.; Yasueda, H. A randomized controlled trial of sublingual immunotherapy for Japanese cedar pollinosis. Int. Arch. Allergy Immunol. 2008, 146, 76–84. [Google Scholar] [CrossRef]
- Sakurai, S.; Yonekura, S.; Iinuma, T.; Morimoto, Y.; Mita, Y.; Arai, T.; Suzuki, S.; Okuma, Y.; Kaneko, S.; Okamoto, Y. Sublingual immunotherapy for allergic rhinitis: Subjective versus objective tools to evaluate its success. Rhinology 2016, 54, 221–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burks, A.W.; Calderon, M.A.; Casale, T.; Cox, L.; Demoly, P.; Jutel, M.; Nelson, H.; Akdis, C.A. Update on allergy immunotherapy: American Academy of Allergy, Asthma & Immunology/European Academy of Allergy and Clinical Immunology/PRACTALL consensus report. J. Allergy Clin Immunol. 2013, 131, 1288–1296. [Google Scholar] [PubMed]
- Inuo, C.; Ando, H.; Tanaka, K.; Nakajima, Y.; Tsuge, I.; Urisu, A.; Kondo, Y. Long-term immunological effects of Japanese cedar pollen-based subcutaneous immunotherapy. Allergol. Int. 2018, 67, 408–410. [Google Scholar] [CrossRef]
- Varga, E.M.; Francis, J.N.; Zach, M.S.; Klunker, S.; Aberer, W.; Durham, S.R. Time course of serum inhibitory activity for facilitated allergen-IgE binding during bee venom immunotherapy in children. Clin. Exp. Allergy 2009, 39, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Gleich, G.J.; Zimmermann, E.M.; Henderson, L.L.; Yunginger, J.W. Effect of immunotherapy on immunoglobulin E and immunoglobulin G antibodies to ragweed antigens: A six-year prospective study. J. Allergy Clin. Immunol. 1982, 70, 261–271. [Google Scholar] [CrossRef]
- Haruna, T.; Kariya, S.; Fujiwara, T.; Yuta, A.; Higaki, T.; Zhao, P.; Ogawa, Y.; Kanai, K.; Hirata, Y.; Oka, A.; et al. Role of whole saliva in the efficacy of sublingual immunotherapy in seasonal allergic rhinitis. Allergol. Int. 2019, 68, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Sakashita, M.; Yamada, T.; Imoto, Y.; Hirota, T.; Tamari, M.; Ito, Y.; Kubo, S.; Osawa, Y.; Takahashi, N.; Fujieda, S. Long-term sublingual immunotherapy for Japanese cedar pollinosis and the levels of IL-17A and complement components 3a and 5a. Cytokine 2015, 75, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Iinuma, T.; Okamoto, Y.; Morimoto, Y.; Arai, T.; Sakurai, T.; Yonekura, S.; Sakurai, D.; Hirahara, K.; Nakayama, T. Pathogenicity of memory Th2 cells is linked to stage of allergic rhinitis. Allergy 2018, 73, 479–489. [Google Scholar] [CrossRef]
- Izuhara, K.; Nunomura, S.; Nanri, Y.; Ogawa, M.; Ono, J.; Mitamura, Y.; Yoshihara, T. Periostin in inflammation and allergy. Cell Mol. Life Sci. 2017, 74, 4293–4303. [Google Scholar] [CrossRef]
- Hoshino, M.; Akitsu, K.; Kubota, K.; Ohtawa, J. Serum Periostin as a Biomarker for Predicting Clinical Response to House Dust Mite Sublingual Immunotherapy in Allergic Rhinitis. J. Allergy Clin. Immunol. Pract. 2020, 9, 1864–1870. [Google Scholar] [CrossRef] [PubMed]
- Izuhara, K.; Yamaguchi, Y.; Ohta, S.; Nunomura, S.; Nanri, Y.; Azuma, Y.; Nomura, N.; Noguchi, Y.; Aihara, M. Squamous Cell Carcinoma Antigen 2 (SCCA2, SERPINB4): An Emerging Biomarker for Skin Inflammatory Diseases. Int. J. Mol. Sci. 2018, 19, 1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nomura, Y.; Okubo, K.; Nakamura, T.; Sawaki, S.; Kitagou, H.; Idei, N.; Kaneko, S.; Kobayashi, S.; Tanaka, Y.; Okamoto, Y. Long-term treatment of Japanese cedar pollinosis with Japanese cedar pollen SLIT drops and persistence of treatment effect: A post-marketing clinical trial. Allergol. Int. 2021, 70, 96–104. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SLIT Successful (n = 16) | SLIT Unsatisfactory (n = 76) | SCIT (n = 13) | Significance | |
|---|---|---|---|---|
| Sex (male:female), n | 8:8 | 36:40 | 6:7 | ns |
| Age at onset, years, median (range) | 30.2 (12–56) | 28.9 (11–62) | 32.1 (12–55) | ns |
| Age at enrolment, years, median (range) | 42.1 (17–64) | 40.6 (18–71) | 41.9 (21–59) | ns |
| Comorbidity of CRSwNP, n (%) | 1 (6.1) | 2 (8.9) | 0 (0) | ns |
| Comorbidity of asthma, n (%) | 2 (12.5) | 10 (13.2) | 2 (15.4) | ns |
| Comorbidity of allergic conjunctivitis, n (%) | 16 (100) | 74 (97.4) | 13 (100) | ns |
| Area (eastern:western), n | 4:12 | 19:57 | 4:9 | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitaya, S.; Ohta, N.; Yuta, A.; Ogawa, Y.; Suzuki, Y.; Ichihara, S.; Ikeda, R.; Enomoto, T.; Kouzaki, H.; Shimizu, T.; et al. Serum Concentrations of Antigen-Specific IgG4 in Patients with Japanese Cedar Pollinosis. Allergies 2021, 1, 140-149. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1030013
Kitaya S, Ohta N, Yuta A, Ogawa Y, Suzuki Y, Ichihara S, Ikeda R, Enomoto T, Kouzaki H, Shimizu T, et al. Serum Concentrations of Antigen-Specific IgG4 in Patients with Japanese Cedar Pollinosis. Allergies. 2021; 1(3):140-149. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1030013
Chicago/Turabian StyleKitaya, Shiori, Nobuo Ohta, Atsushi Yuta, Yukiko Ogawa, Yusuke Suzuki, Seiya Ichihara, Ryoukichi Ikeda, Tadao Enomoto, Hideaki Kouzaki, Takeshi Shimizu, and et al. 2021. "Serum Concentrations of Antigen-Specific IgG4 in Patients with Japanese Cedar Pollinosis" Allergies 1, no. 3: 140-149. https://0-doi-org.brum.beds.ac.uk/10.3390/allergies1030013