Pulse Oximetry and Congenital Heart Disease Screening: Results of the First Pilot Study in Morocco

 , , ,
, , ,
Abstract
:1. Introduction
- To study the feasibility of CCHD screening in our context.
- To improve the early detection of CCHD for better management.
- To improve the timely detection of neonates with other causes of hypoxemia.
2. Material and Methods
3. Results
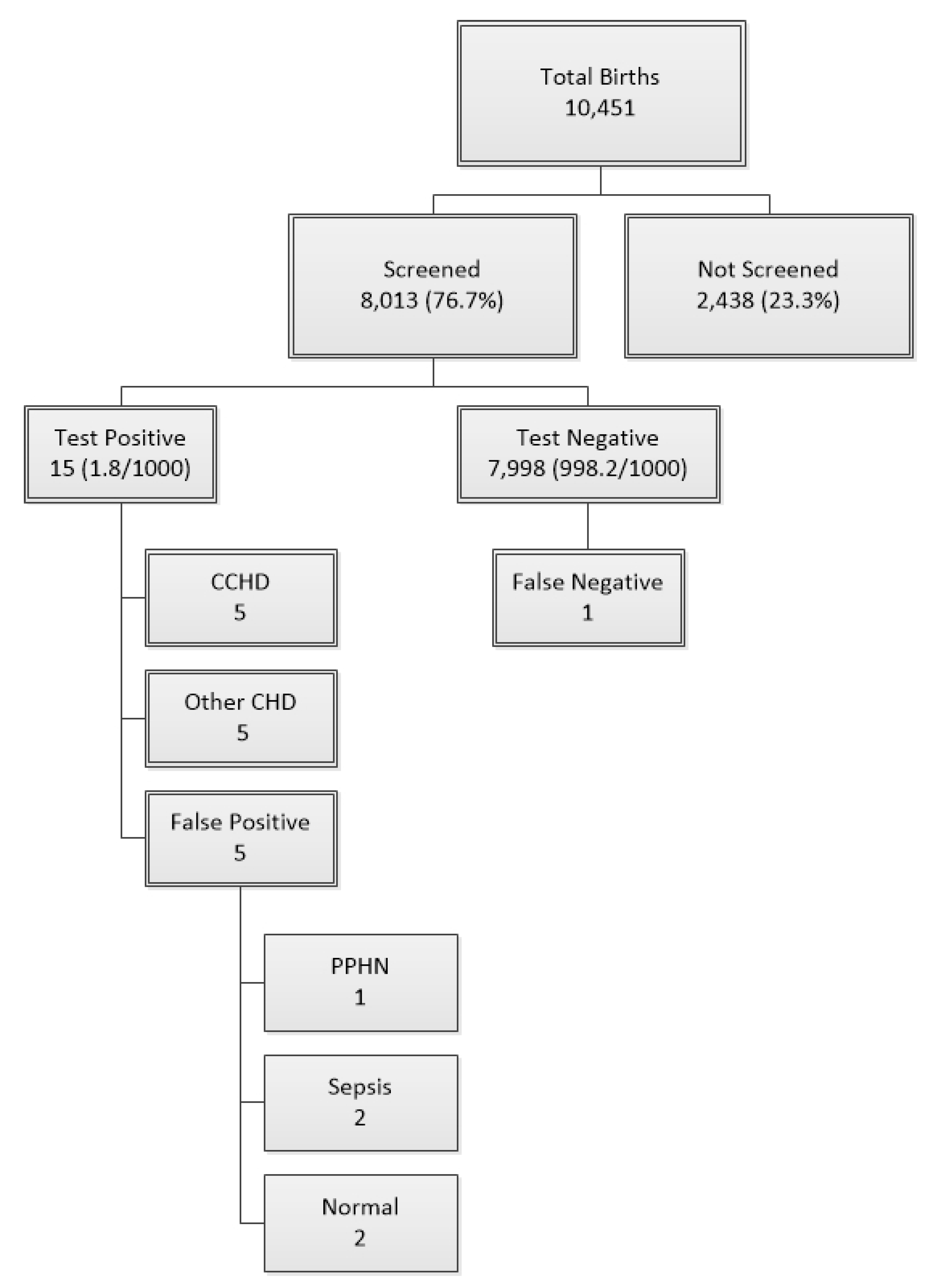
- 5 CCHD: 1 case of D-transposition of great arteries, 1 case of double outlet right ventricle (DORV), transposition of great arteries, and pulmonary stenosis, 1 case of coarctation, and 2 cases of hypoplastic left heart syndrome (HLHS).
- 5 with other heart diseases: 1 case of AV canal, 1 case of large ASD, 2 cases of hypertrophic cardiomyopathy, and 1 case of single atrium.
- 5 false positives: 1 persistent pulmonary hypertension (PPHN), 2 sepsis, and 2 normal heart.
- 1 false negative: coarctation of aorta at 2 months of age.
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Plana, M.N.; Zamora, J.; Suresh, G.; Fernandez-Pineda, L.; Thangaratinam, S.; Ewer, A.K. Pulse oximetry screening for critical congenital heart defects. Cochrane Database Syst. Rev. 2018, 3, CD011912. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.-K.R.; Gurvitz, M.; Rodriguez, S. Missed Diagnosis of Critical Congenital Heart Disease. Arch. Pediatr. Adolesc. Med. 2008, 162, 969–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilçıkan, Ş.; Can, E. Critical congenital heart disease screening with a pulse oximetry in neonates. J. Perinat. Med. 2018, 46, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Kemper, A.R.; Mahle, W.T.; Martin, G.R.; Cooley, W.C.; Kumar, P.; Morrow, W.R.; Kelm, K.; Pearson, G.D.; Glidewell, J.; Grosse, S.D.; et al. Strategies for implementing screening for critical congenital heart disease. Pediatrics 2011, 128, e1259–e1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahle, W.T.; Martin, G.R.; Beekman, R.H.; Morrow, W.R. Section on Cardiology and Cardiac Surgery Executive Committee. Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Pediatrics 2012, 129, 190–192. [Google Scholar] [PubMed] [Green Version]
- Zhao, Q.; Ma, X.; Ge, X.; Liu, F.; Yan, W.; Wu, L.; Ye, M.; Liang, X.; Zhang, J.; Gao, Y.; et al. Pulse oximetry with clinical assessment to screen for congenital heart disease in neonates in China: A prospective study. Lancet 2014, 384, 747–754. [Google Scholar] [CrossRef]
- Arlettaz, R.; Bauschatz, A.; Mönkhoff, M.; Essers, B. The contribution of pulse oximetry to the early detection of congenital heart disease in newborns. Eur. J. Pediatr. 2006, 165, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Ewer, A.K.; Middleton, L.J.; Furmston, A.T.; Bhoyar, A.; Daniels, J.P.; Thangaratinam, S.; Deeks, J.J.; Khan, K.S.; On Behalf of the PulseOx Study Group. Pulse oximetry screening for congenital heart defects in newborn infants: A test accuracy study. Lancet 2011, 378, 785–794. [Google Scholar] [CrossRef]
- Ramegowda, S.; Ramachandra, N.B. Parental consanguinity increases congenital heart diseases in South India. Ann. Hum. Biol. 2006, 33, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Thangaratinam, S.; Brown, K.; Zamora, J.; Khan, K.S.; Ewer, A.K. Pulse oxymetry screening for critical congenital heart defects (CCHD) in asymptomatic newborn babies: A systematic review and meta-analysis. Lancet 2012, 379, 2459–2464. [Google Scholar] [CrossRef]
- De-Wahl Granelli, A.; Wennergren, M.; Sandberg, K.; Mellander, M.; Bejlum, C.; Inganäs, L.; Eriksson, M.; Segerdahl, N.; Agren, A.; Ekman-Joelsson, B.M.; et al. Impact of pulse oxymetry screening on the detection of duct dependent congenital heart disease: A Swedish prospective screening study in 39,821 newborns. BMJ 2009, 338, a3037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riede, F.T.; Paech, C.; Orlikowsky, T. Pulse Oximetry Screening in Germany—Historical Aspects and Future Perspectives. Int. J. Neonatal Screen. 2018, 4, 15. [Google Scholar] [CrossRef] [Green Version]
- Al Mazrouei, S.K.; Moore, J.; Ahmed, F.; Mikula, E.B.; Martin, G.R. Regional implementation of newborn screening for critical congenital heart disease screening in Abu Dhabi. Pediatr. Cardiol. 2013, 34, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Methlouthi, J.; Mahdhaoui, N.; Bellaleh, M.; Guith, A.; Zouari, D.; Ayech, H.; Nouri, S.; Séboui, H. Incidence of congenital heart disease in newborns after pulse oximetry screening introduction. Tunis Med. 2016, 94, 231–234. [Google Scholar] [PubMed]
- Thangaratinam, S.; Daniels, J.; Ewer, A.K.; Zamora, J.; Khan, K.S. Accuracy of pulse oxymetry in screening for congenital heart disease in asymptomatic newborns: A systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F176–F180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sola, A.; Rodríguez, S.; Young, A.; Lemus, L.; Villamayor, R.M.; Cardetti, M.; Navarrete, J.P.; Favareto, V.; Lima, V.; Baquero, H.; et al. CCHD Screening Implementation Efforts in Latin American Countries by the Ibero American Society of Neonatology (SIBEN). Int. J. Neonatal Screen. 2020, 6, 21. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Diagnosis | Number of Cases | Outcome |
|---|---|---|
| Critical Congenital Heart Disease | ||
| D-Transposition of great arteries | 1 | Operated with good results |
| Double outlet right ventricle, transposition of great arteries, and pulmonary stenosis | 1 | Stable, waiting for surgery |
| Coarctation and Persistent ductus arteriosus | 1 | Waiting for surgery |
| Hypoplastic left heart syndrome | 2 | Died |
| Non-Critical Congenital Heart Diseases | ||
| Single atrium. | 1 | Stable, waiting for surgery |
| Hypertrophic myocardium | 2 | Normal heart |
| Large atrial septal defect | 1 | Stable, waiting for surgery |
| Atrio ventricular canal defect | 1 | Stable, waiting for surgery |
| False positive | ||
| Persistent pulmonary hypertension of the newborn | 1 | Normal |
| Sepsis | 2 | Recovered |
| Normal | 2 | Normal |
| False negative | ||
| Coarctation of aorta | 1 | Stable, waiting for surgery |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Idrissi Slitine, N.; Bennaoui, F.; Sable, C.A.; Martin, G.R.; Hom, L.A.; Fadel, A.; Moussaoui, S.; Inajjarne, N.; Boumzebra, D.; Mouaffak, Y.; et al. Pulse Oximetry and Congenital Heart Disease Screening: Results of the First Pilot Study in Morocco. Int. J. Neonatal Screen. 2020, 6, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6030053
El Idrissi Slitine N, Bennaoui F, Sable CA, Martin GR, Hom LA, Fadel A, Moussaoui S, Inajjarne N, Boumzebra D, Mouaffak Y, et al. Pulse Oximetry and Congenital Heart Disease Screening: Results of the First Pilot Study in Morocco. International Journal of Neonatal Screening. 2020; 6(3):53. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6030053
Chicago/Turabian StyleEl Idrissi Slitine, Nadia, Fatiha Bennaoui, Craig A. Sable, Gerard R. Martin, Lisa A. Hom, Amal Fadel, Soufiane Moussaoui, Nadir Inajjarne, Drissi Boumzebra, Youssef Mouaffak, and et al. 2020. "Pulse Oximetry and Congenital Heart Disease Screening: Results of the First Pilot Study in Morocco" International Journal of Neonatal Screening 6, no. 3: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns6030053