
Newborn Screening for Severe Combined Immunodeficiency Using the Multiple of the Median Values of T-Cell Receptor Excision Circles

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. DNA Isolation
2.3. Real-Time PCR Assay
2.4. MoM Cutoff Establishment
3. Results
3.1. Results of Cutoff Establishment
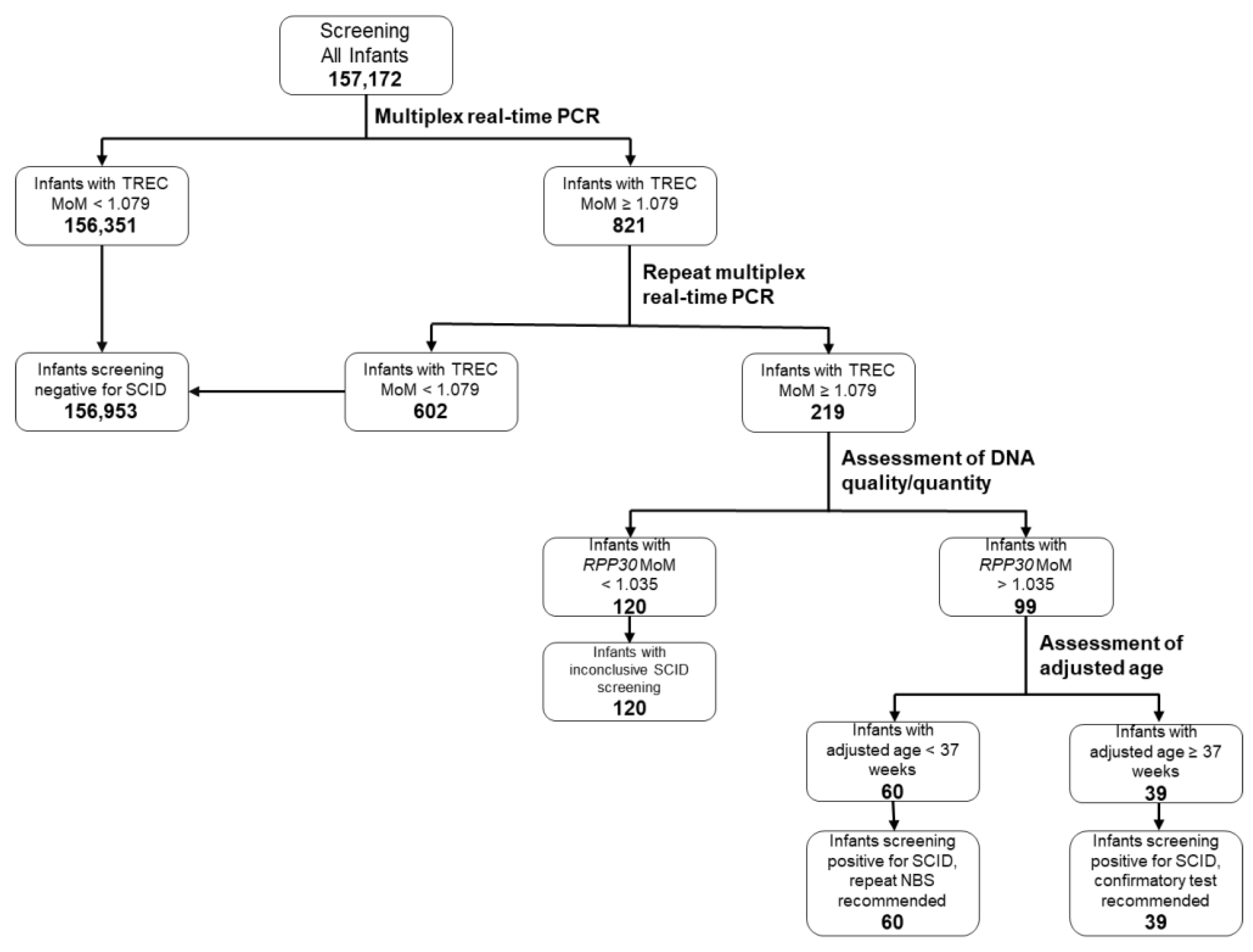
3.2. SCID Screening Algorithm and Its Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Chinn, I.K.; Shearer, W.T. Severe combined immunodeficiency disorders. Immunol. Allergy Clin. N. Am. 2015, 35, 671–694. [Google Scholar] [CrossRef] [PubMed]
- Puck, J.M. Newborn screening for severe combined immunodeficiency and T-cell lymphopenia. Immunol. Rev. 2019, 287, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Hazenberg, M.D.; Verschuren, M.C.; Hamann, D.; Miedema, F.; Dongen, J.J. T cell receptor excision circles as markers for recent thymic emigrants: Basic aspects, technical approach, and guidelines for interpretation. J. Mol. Med. 2001, 79, 631–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.W.; Grossman, W.J.; Laessig, R.H.; Hoffman, G.L.; Brokopp, C.D.; Kurtycz, D.F.; Cogley, M.F.; Litsheim, T.J.; Katcher, M.L.; Routes, J.M. Development of a routine newborn screening protocol for severe combined immunodeficiency. J. Allergy Clin. Immunol. 2009, 124, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Verbsky, J.W.; Baker, M.W.; Grossman, W.J.; Hintermeyer, M.; Dasu, T.; Bonacci, B.; Reddy, S.; Margolis, D.; Casper, J.; Gries, M.; et al. Newborn screening for severe combined immunodeficiency; The Wisconsin experience (2008–2011). J. Clin. Immunol. 2012, 32, 83–88. [Google Scholar] [CrossRef] [PubMed]
- SCID|NewSTEPs. Available online: https://www.newsteps.org/resources/disorders/scid (accessed on 25 May 2021).
- Al-Mousa, H.; Al-Dakheel, G.; Jabr, A.; Elbadaoui, F.; Abouelhoda, M.; Baig, M.; Monies, D.; Meyer, B.; Hawwari, A.; Dasouki, M. High incidence of severe combined immunodeficiency disease in Saudi Arabia detected through combined T cell receptor excision circle and next generation sequencing of newborn dried blood spots. Front. Immunol. 2018, 9, 782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argudo-Ramírez, A.; Martín-Nalda, A.; Marín-Soria, J.L.; López-Galera, R.M.; Pajares-García, S.; de Aledo-Castillo, J.M.G.; Martínez-Gallo, M.; García-Prat, M.; Colobran, R.; Riviere, J.G. First universal newborn screening program for severe combined immunodeficiency in Europe. Two-years’ experience in Catalonia (Spain). Front. Immunol. 2019, 10, 2406. [Google Scholar] [CrossRef] [PubMed]
- Audrain, M.A.; Léger, A.J.; Hémont, C.A.; Mirallié, S.M.; Cheillan, D.; Rimbert, M.G.; Le Thuaut, A.M.; Sébille-Rivain, V.A.; Prat, A.; Pinel, E.M. Newborn screening for severe combined immunodeficiency: Analytic and clinical performance of the T cell receptor excision circle assay in France (DEPISTREC study). J. Clin. Immunol. 2018, 38, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.; Ohlsson, A.; Borte, S.; Jonsson, S.; Zetterström, R.H.; King, J.; Winiarski, J.; von Döbeln, U.; Hammarström, L. Newborn screening for severe primary immunodeficiency diseases in Sweden—A 2-year pilot TREC and KREC screening study. J. Clin. Immunol. 2017, 37, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blom, M.; Bredius, R.G.; Weijman, G.; Dekkers, E.H.; Kemper, E.A.; den Akker-van Marle, V.; Elske, M.; Van der Ploeg, C.P.; Van der Burg, M.; Schielen, P.C. Introducing newborn screening for severe combined immunodeficiency (SCID) in the Dutch neonatal screening program. Int. J. Neonatal Screen. 2018, 4, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chien, Y.-H.; Yu, H.-H.; Lee, N.-C.; Ho, H.-C.; Kao, S.-M.; Lu, M.-Y.; Jaing, T.-H.; Lee, W.-I.; Chang, K.-W.; Shieh, C.-C. Newborn screening for severe combined immunodeficiency in Taiwan. Int. J. Neonatal Screen. 2017, 3, 16. [Google Scholar] [CrossRef]
- Kanegae, M.P.P.; Barreiros, L.A.; Sousa, J.L.; Brito, M.A.S.; de Oliveira, E.B. Newborn screening for severe combined immunodeficiencies using TRECs and KRECs: Second pilot study in Brazil. Rev. Paul. Pediatr. 2017, 35, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muramatsu, H.; Kojima, D.; Okuno, Y.; Kataoka, S.; Nakajima, Y.; Ito, T.; Tsuge, I.; Yoshimi, S.; Kato, T.; Kojima, S. Combination of TREC measurement and next-generation sequencing in newborn screening for severe combined immunodeficiency: A pilot program in Japan. Blood 2018, 132, 3717. [Google Scholar] [CrossRef]
- Rechavi, E.; Lev, A.; Saraf-Levy, T.; Etzioni, A.; Almashanu, S.; Somech, R. Newborn screening for severe combined immunodeficiency in Israel. Int. J. Neonatal Screen. 2017, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Berberich, S.L. Using multiples of the median (MoM) for normalization of TREC results meets the need for standardized SCID reporting. In Proceedings of the 2013 Joint Meeting of the Newborn Screening and Genetic Testing Symposium and the International Society for Neonatal Screening, Atlanta, GA, USA, 5–10 May 2013; Available online: https://www.aphl.org/conferences/proceedings/Documents/2013/Newborn-Screening-Symposium/23Berberich.pdf (accessed on 26 May 2021).
- Wald, N.J.; Cuckle, H.; Brock, J.H.; Peto, R.; Polani, P.E.; Woodford, F.P. Maternal serum-alpha-fetoprotein measurement in antenatal screening for anencephaly and spina bifida in early pregnancy. Report of U.K. collaborative study on alpha-fetoprotein in relation to neural-tube defects. Lancet 1977, 1, 1323–1332. [Google Scholar] [PubMed]
- Bishop, J.C.; Dunstan, F.D.; Nix, B.J.; Reynolds, T.M.; Swift, A. All MoMs are not equal: Some statistical properties associated with reporting results in the form of multiples of the median. Am. J. Hum. Genet. 1993, 52, 425–430. [Google Scholar] [PubMed]


{kind=link}
| Category | Number | Percentage | |
|---|---|---|---|
| Sex | Male | 80,388 | 51.1 |
| Female | 76,692 | 48.8 | |
| Unknown | 92 | ||
| Gestational age | <37 weeks | 12,971 | 8.3 |
| ≥37 weeks | 144,168 | 91.7 | |
| Unknown | 33 | ||
| Birth weight | <2500 g | 11,624 | 7.4 |
| ≥2500 g | 145,533 | 92.6 | |
| Unknown | 15 | ||
| Name | Sequence |
|---|---|
| TREC Forward Primer | 5′-CATGCTGACACCTCTGGTT-3′ |
| TREC Reverse Primer | 5′-CGGTGAATGAAGAGCAGACA-3′ |
| RPP30 Forward Primer | 5′-AGATTTGGACCTGCGAGCG-3′ |
| RPP30 Reverse Primer | 5′-GAGCGGCTGTCTCCACAAGT-3′ |
| SMN Forward Primer | 5′-CTTGTGAAACAAAATGCTTTTTAACATCCAT-3′ |
| SMN Reverse Primer | 5′-GAATGTGAGCACCTTCCTTCTTTTT-3′ |
| TREC Probe | 5′-/56-FAM/ACTCCTGTG/ZEN/CACGGTGATGCATAG/3IABkFQ/-3′ |
| RPP30 Probe | 5′-/5HEX/TTCTGACCT/ZEN/GAAGGCTCTGCGCG/3IABkFQ/-3′ |
| SMN1 Probe | 5′-/5ATTO550N/AGG + GTT + T + C + A + GAC/3IAbRQSp/-3′ |
| SMN2 Blocker | 5′-AG + G + GTT + T + T + A + GAC-3′ |
| TREC | RPP30 | |||
|---|---|---|---|---|
| Ct | MoM | Ct | MoM | |
| N | 2244 | 2244 | 2244 | 2244 |
| Mean | 30.762 | 1.002 | 24.280 | 1.002 |
| Median | 30.705 | 1.000 | 24.243 | 1.000 |
| Standard deviation | 0.794 | 0.026 | 0.643 | 0.027 |
| Category | Result of Subsequent Screen or Confirmatory Testing | Number | Percentage |
|---|---|---|---|
| First screen inconclusive | Negative screen | 105 | 87.5 |
| Infant expired | 9 | 7.5 | |
| Family declined follow-up | 2 | 1.7 | |
| Positive screen; confirmatory testing recommended (see below) | 4 | 3.3 | |
| First screen positive, age <37 weeks | Negative screen | 41 | 68.3 |
| Infant expired | 16 | 26.7 | |
| Positive screen; confirmatory testing recommended (see below) | 3 | 5.0 | |
| Positive screens referred for confirmatory testing | T-cell lymphopenia | 13 a | 28.3 |
| 22q11.2 deletion syndrome | 5 b | 10.9 | |
| Cartilage–hair hypoplasia | 2 | 4.3 | |
| CHARGE syndrome | 1 | 2.2 | |
| Ataxia telangiectasia | 1 | 2.2 | |
| SCID (homozygous RAG1,c.2974A > G) | 1 | 2.2 | |
| False positive | 23 c | 50.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cogley, M.F.; Wiberley-Bradford, A.E.; Mochal, S.T.; Dawe, S.J.; Piro, Z.D.; Baker, M.W. Newborn Screening for Severe Combined Immunodeficiency Using the Multiple of the Median Values of T-Cell Receptor Excision Circles. Int. J. Neonatal Screen. 2021, 7, 43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns7030043
Cogley MF, Wiberley-Bradford AE, Mochal ST, Dawe SJ, Piro ZD, Baker MW. Newborn Screening for Severe Combined Immunodeficiency Using the Multiple of the Median Values of T-Cell Receptor Excision Circles. International Journal of Neonatal Screening. 2021; 7(3):43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns7030043
Chicago/Turabian StyleCogley, Michael F., Amy E. Wiberley-Bradford, Sean T. Mochal, Sandra J. Dawe, Zachary D. Piro, and Mei W. Baker. 2021. "Newborn Screening for Severe Combined Immunodeficiency Using the Multiple of the Median Values of T-Cell Receptor Excision Circles" International Journal of Neonatal Screening 7, no. 3: 43. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns7030043