
Towards Next-Generation Sequencing (NGS)-Based Newborn Screening: A Technical Study to Prepare for the Challenges Ahead

 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Outline of the Study
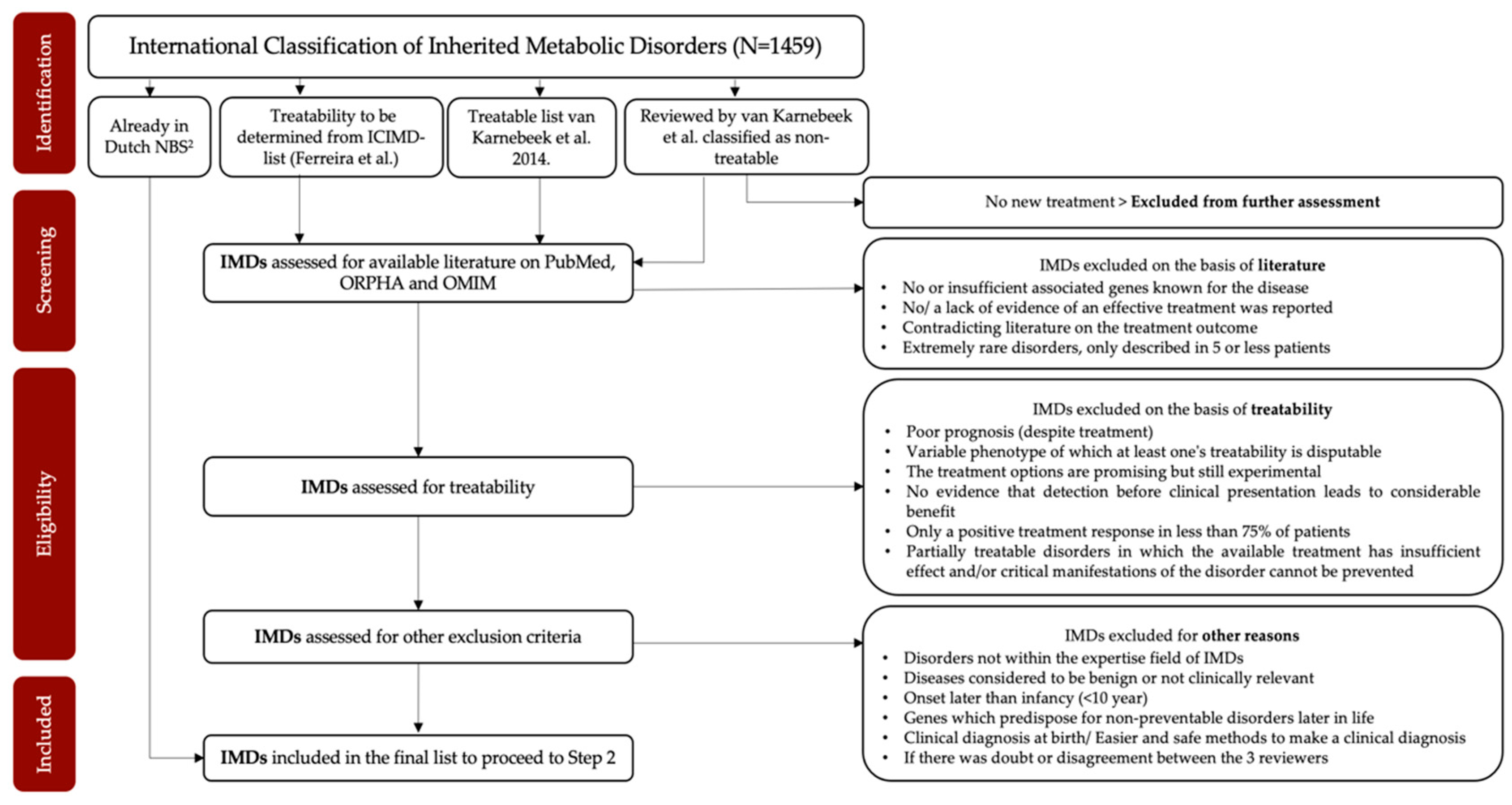
2.2. Methods to Identify Which IMDs Are Eligible for NGS-First Testing (Step 1)
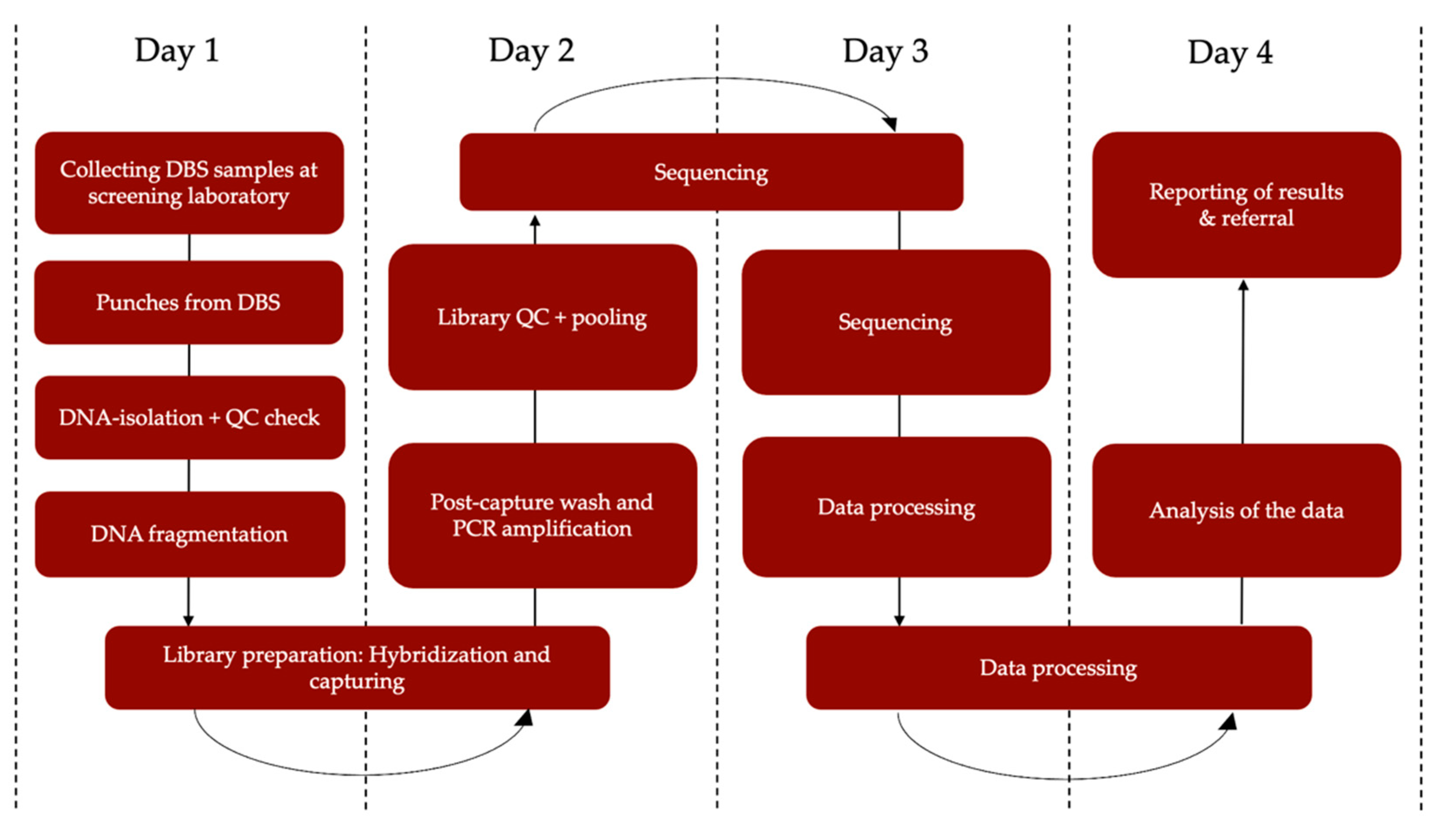
2.3. Developing a Rapid NGS-Based Workflow for NBS (Step 2)
2.3.1. Samples
2.3.2. DNA Isolation
2.3.3. NGS Methods
2.3.4. Data Analysis
2.4. Preparing for the Incorporation of the Pipeline into the Dutch NBS Program (Step 3)
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blom, M.; Bredius, R.G.; Weijman, G.; Dekkers, E.H.; Kemper, E.A.; den Akker-van Marle, V.; Elske, M.; Van der Ploeg, C.P.; Van der Burg, M.; Schielen, P.C. Introducing Newborn Screening for Severe Combined Immunodeficiency (SCID) in the Dutch Neonatal Screening Program. Int. J. Neonatal Screen. 2018, 4, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haug, U.; Coupé, V.M.H. The cumulative false-positive rate in colorectal cancer screening: A Markov analysis. Eur. J. Gastroenterol. Hepatol. 2020, 32, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Winget, M.; Yuan, Y. The impact of false positive breast cancer screening mammograms on screening retention: A retrospective population cohort study in Alberta, Canada. Can. J. Public Health 2017, 108, e539–e545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Román, M.; Hofvind, S.; Von Euler-Chelpin, M.; Castells, X. Long-term risk of screen-detected and interval breast cancer after false-positive results at mammography screening: Joint analysis of three national cohorts. Br. J. Cancer 2019, 120, 269–275. [Google Scholar] [CrossRef] [Green Version]
- van der Meij, K.R.; Sistermans, E.A.; Macville, M.V.; Stevens, S.J.; Bax, C.J.; Bekker, M.N.; Bilardo, C.M.; Boon, E.M.; Boter, M.; Diderich, K.E.; et al. TRIDENT-2: National Implementation of Genome-wide Non-invasive Prenatal Testing as a First-Tier Screening Test in the Netherlands. Am. J. Hum. Genet. 2019, 105, 1091–1101. [Google Scholar] [CrossRef]
- Welling, L.; Boelen, A.; Derks, T.G.; Schielen, P.C.; de Vries, M.; Williams, M.; Wijburg, F.A.; Bosch, A.M. Nine years of newborn screening for classical galactosemia in the Netherlands: Effectiveness of screening methods, and identification of patients with previously unreported phenotypes. Mol. Genet. Metab. 2017, 120, 223–228. [Google Scholar] [CrossRef]
- Yang, H.; Rossignol, F.; Cyr, D.; Laframboise, R.; Wang, S.P.; Soucy, J.-F.; Berthier, M.-T.; Giguère, Y.; Waters, P.J.; Mitchell, G.A.; et al. Mildly elevated succinylacetone and normal liver function in compound heterozygotes with pathogenic and pseudodeficient FAH alleles. Mol. Genet. Metab. Rep. 2018, 14, 55–58. [Google Scholar] [CrossRef]
- Tarini, B.A.; Christakis, D.A.; Welch, H.G. State Newborn Screening in the Tandem Mass Spectrometry Era: More Tests, More False-Positive Results. Pediatrics 2006, 118, 448–456. [Google Scholar] [CrossRef]
- Vasquez-Loarte, T.; Thompson, J.D.; Merritt, J.L. Considering Proximal Urea Cycle Disorders in Expanded Newborn Screening. Int. J. Neonatal Screen. 2020, 6, 77. [Google Scholar] [CrossRef]
- French, C.E.; Delon, I.; Dolling, H.; Sanchis-Juan, A.; Shamardina, O.; Mégy, K.; Abbs, S.; Austin, T.; Bowdin, S.; Branco, R.G.; et al. Whole genome sequencing reveals that genetic conditions are frequent in intensively ill children. Intensive Care Med. 2019, 45, 627–636. [Google Scholar] [CrossRef] [Green Version]
- Daoud, H.; Luco, S.M.; Li, R.; Bareke, E.; Beaulieu, C.; Jarinova, O.; Carson, N.; Nikkel, S.M.; Graham, G.E.; Richer, J.; et al. Next-generation sequencing for diagnosis of rare diseases in the neonatal intensive care unit. Can. Med. Assoc. J. 2016, 188, E254–E260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, L.; Pammi, M.; Saronwala, A.; Magoulas, P.; Ghazi, A.R.; Vetrini, F.; Zhang, J.; He, W.; Dharmadhikari, A.V.; Qu, C.; et al. Use of Exome Sequencing for Infants in Intensive Care Units. JAMA Pediatrics 2017, 171, e173438. [Google Scholar] [CrossRef] [PubMed]
- Farnaes, L.; Hildreth, A.; Sweeney, N.M.; Clark, M.M.; Chowdhury, S.; Nahas, S.; Cakici, J.A.; Benson, W.; Kaplan, R.H.; Kronick, R.; et al. Rapid whole-genome sequencing decreases infant morbidity and cost of hospitalization. NPJ Genom. Med. 2018, 3, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boemer, F.; Fasquelle, C.; d’Otreppe, S.; Josse, C.; Dideberg, V.; Segers, K.; Guissard, V.; Capraro, V.; Debray, F.G.; Bours, V. A next-generation newborn screening pilot study: NGS on dried blood spots detects causal mutations in patients with inherited metabolic diseases. Sci. Rep. 2017, 7, 17641. [Google Scholar] [CrossRef]
- Furnier, S.M.; Durkin, M.S.; Baker, M.W. Translating Molecular Technologies into Routine Newborn Screening Practice. Int. J. Neonatal Screen. 2020, 6, 80. [Google Scholar] [CrossRef]
- Adhikari, A.N.; Gallagher, R.C.; Wang, Y.; Currier, R.J.; Amatuni, G.; Bassaganyas, L.; Chen, F.; Kundu, K.; Kvale, M.; Mooney, S.D.; et al. The role of exome sequencing in newborn screening for inborn errors of metabolism. Nat. Med. 2020, 26, 1392–1397. [Google Scholar] [CrossRef]
- Sicko, R.J.; Stevens, C.F.; Hughes, E.E.; Leisner, M.; Ling, H.; Saavedra-Matiz, C.A.; Caggana, M.; Kay, D.M. Validation of a Custom Next-Generation Sequencing Assay for Cystic Fibrosis Newborn Screening. Int. J. Neonatal Screen. 2021, 7, 73. [Google Scholar] [CrossRef]
- Marsden, D.; Bedrosian, C.L.; Vockley, J. Impact of newborn screening on the reported incidence and clinical outcomes associated with medium- and long-chain fatty acid oxidation disorders. Genet. Med. 2021, 23, 816–829. [Google Scholar] [CrossRef]
- Hoytema van Konijnenburg, E.M.; Wortmann, S.B.; Koelewijn, M.J.; Tseng, L.A.; Houben, R.; Stöckler-Ipsiroglu, S.; Ferreira, C.R.; van Karnebeek, C.D. Treatable inherited metabolic disorders causing intellectual disability: 2021 review and digital app. Orphanet J. Rare Dis. 2021, 16, 170. [Google Scholar] [CrossRef]
- Zaki, O.K.; Priya Doss, C.G.; Ali, S.A.; Murad, G.G.; Elashi, S.A.; Ebnou, M.S.A.; Kumar, T.; Khalifa, O.; Gamal, R.; El Abd, H.S.A.; et al. Genotype-phenotype correlation in patients with isovaleric acidaemia: Comparative structural modelling and computational analysis of novel variants. Hum. Mol. Genet. 2017, 26, 3105–3115. [Google Scholar] [CrossRef] [Green Version]
- Holm, I.A.; Agrawal, P.B.; Ceyhan-Birsoy, O.; Christensen, K.D.; Fayer, S.; Frankel, L.A.; Genetti, C.A.; Krier, J.B.; LaMay, R.C.; Levy, H.L.; et al. The BabySeq project: Implementing genomic sequencing in newborns. BMC Pediatrics 2018, 18, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceyhan-Birsoy, O.; Murry, J.B.; Machini, K.; Lebo, M.S.; Timothy, W.Y.; Fayer, S.; Genetti, C.A.; Schwartz, T.S.; Agrawal, P.B.; Parad, R.B.; et al. Interpretation of Genomic Sequencing Results in Healthy and Ill Newborns: Results from the BabySeq Project. Am. J. Hum. Genet. 2019, 104, 76–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojcik, M.H.; Zhang, T.; Ceyhan-Birsoy, O.; Genetti, C.A.; Lebo, M.S.; Yu, T.W.; Parad, R.B.; Holm, I.A.; Rehm, H.L.; Beggs, A.H.; et al. Discordant results between conventional newborn screening and genomic sequencing in the BabySeq Project. Genet. Med. 2021, 23, 1372–1375. [Google Scholar] [CrossRef] [PubMed]
- Milko, L.V.; O’Daniel, J.M.; DeCristo, D.M.; Crowley, S.B.; Foreman, A.K.; Wallace, K.E.; Mollison, L.F.; Strande, N.T.; Girnary, Z.S.; Boshe, L.J.; et al. An Age-Based Framework for Evaluating Genome-Scale Sequencing Results in Newborn Screening. J. Pediatrics 2019, 209, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, A.N.; Currier, R.J.; Tang, H.; Turgeon, C.T.; Nussbaum, R.L.; Srinivasan, R.; Sunderam, U.; Kwok, P.Y.; Brenner, S.E.; Gavrilov, D.; et al. Genomic Analysis of Historical Cases with Positive Newborn Screens for Short-Chain Acyl-CoA Dehydrogenase Deficiency Shows That a Validated Second-Tier Biochemical Test Can Replace Future Sequencing. Int. J. Neonatal Screen. 2020, 6, 41. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.M.; Jungner, G. Principles and Practice of Screening for Disease; WHO: Geneva, Switzerland, 1968. [Google Scholar]
- Andermann, A. Revisting wilson and Jungner in the genomic age: A review of screening criteria over the past 40 years. Bull. World Health Organ. 2008, 86, 317–319. [Google Scholar] [CrossRef]
- Sturdy, S.; Miller, F.; Hogarth, S.; Armstrong, N.; Chakraborty, P.; Cressman, C.; Dobrow, M.; Flitcroft, K.; Grossman, D.; Harris, R.; et al. Half a Century of Wilson & Jungner: Reflections on the Governance of Population Screening. Wellcome Open Res. 2020, 5, 158. [Google Scholar]
- Gezondheidsraad. Advies Screenen op Niet-Behandelbare Aandoeningen Vroeg in Het Leven; Ministerie van Volksgezondheid WeS: Den Haag, The Netherlands, 2020. [Google Scholar]
- Gezondheidsraad. Neonatale Screening: Nieuwe Aanbevelingen; Ministerie van Volksgezondheid WeS: Den Haag, The Netherlands, 2015. [Google Scholar]
- Ferreira, C.R.; Rahman, S.; Keller, M.; Zschocke, J.; ICIMD Advisory Group; Abdenur, J.; Ali, H.; Artuch, R.; Ballabio, A.; Barshop, B.; et al. An international classification of inherited metabolic disorders (ICIMD). J. Inherit. Metab. Dis. 2021, 44, 164. [Google Scholar] [CrossRef]
- Van Karnebeek, C.D.M.; Shevell, M.; Zschocke, J.; Moeschler, J.B.; Stockler, S. The metabolic evaluation of the child with an intellectual developmental disorder: Diagnostic algorithm for identification of treatable causes and new digital resource. Mol. Genet. Metab. 2014, 111, 428–438. [Google Scholar] [CrossRef]
- Ghantous, A.; Saffery, R.; Cros, M.P.; Ponsonby, A.L.; Hirschfeld, S.; Kasten, C.; Dwyer, T.; Herceg, Z.; Hernandez-Vargas, H. Optimized DNA extraction from neonatal dried blood spots: Application in methylome profiling. BMC Biotechnol. 2014, 14, 60. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.H.; Lee, S.K.; Ihm, C.; Sohn, Y.H. Rapid DNA extraction from dried blood spots on filter paper: Potential applications in biobanking. Osong Public Health Res. Perspect. 2014, 5, 351–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakim, H.M.; Khan, H.O.; Ismail, S.A.; Ayob, S.; Lalung, J.; Kofi, E.A.; Chambers, G.K.; Edinur, H.A. Assessment of autosomal and male DNA extracted from casework samples using Casework Direct Kit, Custom and Maxwell 16 System DNA IQ Casework Pro Kit for autosomal-STR and Y-STR profiling. Sci. Rep. 2019, 9, 14558. [Google Scholar] [CrossRef] [PubMed]
- Mertes, F.; ElSharawy, A.; Sauer, S.; van Helvoort, J.M.; Van Der Zaag, P.J.; Franke, A.; Nilsson, M.; Lehrach, H.; Brookes, A.J. Targeted enrichment of genomic DNA regions for next-generation sequencing. Brief. Funct. Genom. 2011, 10, 374–386. [Google Scholar] [CrossRef] [PubMed]
- Haer-Wigman, L.; van Zelst-Stams, W.A.; Pfundt, R.; van den Born, L.I.; Klaver, C.C.; Verheij, J.B.; Hoyng, C.B.; Breuning, M.H.; Boon, C.J.; Kievit, A.J.; et al. Diagnostic exome sequencing in 266 Dutch patients with visual impairment. Eur. J. Hum. Genet. 2017, 25, 591–599. [Google Scholar] [CrossRef]
- Corsten-Janssen, N.; Bouman, K.; Diphoorn, J.C.; Scheper, A.J.; Kinds, R.; El Mecky, J.; Breet, H.; Verheij, J.B.; Suijkerbuijk, R.; Duin, L.K.; et al. A prospective study on rapid exome sequencing as a diagnostic test for multiple congenital anomalies on fetal ultrasound. Prenat. Diagn. 2020, 40, 1300–1309. [Google Scholar] [CrossRef]
- Alimohamed, M.Z.; Johansson, L.F.; Posafalvi, A.; Boven, L.G.; van Dijk, K.K.; Walters, L.; Vos, Y.J.; Westers, H.; Hoedemaekers, Y.M.; Sinke, R.J.; et al. Diagnostic yield of targeted next generation sequencing in 2002 Dutch cardiomyopathy patients. Int. J. Cardiol. 2021, 332, 99–104. [Google Scholar] [CrossRef]
- Kalia, S.S.; Adelman, K.; Bale, S.J.; Chung, W.K.; Eng, C.; Evans, J.P.; Herman, G.E.; Hufnagel, S.B.; Klein, T.E.; Korf, B.R.; et al. Recommendations for reporting of secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF v2.0): A policy statement of the American College of Medical Genetics and Genomics. Genet. Med. 2017, 19, 249–255. [Google Scholar] [CrossRef] [Green Version]
- van der Schoot, V.; Haer-Wigman, L.; Feenstra, I.; Tammer, F.; Oerlemans, A.J.; van Koolwijk, M.; van Agt, F.; Arens, Y.H.; Brunner, H.G.; Vissers, L.E.; et al. Lessons learned from unsolicited findings in clinical exome sequencing of 16,482 individuals. Eur. J. Hum. Genet. 2021, 30, 170–177. [Google Scholar] [CrossRef]
- Claussnitzer, M.; Cho, J.H.; Collins, R.; Cox, N.J.; Dermitzakis, E.T.; Hurles, M.E.; Kathiresan, S.; Kenny, E.E.; Lindgren, C.M.; MacArthur, D.G.; et al. A brief history of human disease genetics. Nature 2020, 577, 179–189. [Google Scholar] [CrossRef] [Green Version]
- National Human Genome Research Institute. The Cost of Sequencing a Human Genome. 2021. Available online: https://www.genome.gov/about-genomics/fact-sheets/Sequencing-Human-Genome-cost (accessed on 1 November 2021).
- Dixit, S.; Sahu, P.; Kar, S.K.; Negi, S. Identification of the hot-spot areas for sickle cell disease using cord blood screening at a district hospital: An Indian perspective. J. Community Genet. 2015, 6, 383–387. [Google Scholar] [CrossRef] [Green Version]
- Bhatia, R.; Rajwaniya, D. Congenital hypothyroidism screening in term neonates using umbilical cord blood TSH values. Indian J. Endocrinol. Metab. 2018, 22, 277. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Lincoln, S.E.; Kobayashi, Y.; Nykamp, K.; Nussbaum, R.L.; Topper, S. Sources of discordance among germ-line variant classifications in ClinVar. Genet. Med. 2017, 19, 1118–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zastrow, D.B.; Baudet, H.; Shen, W.; Thomas, A.; Si, Y.; Weaver, M.A.; Lager, A.M.; Liu, J.; Mangels, R.; Dwight, S.S.; et al. Unique aspects of sequence variant interpretation for inborn errors of metabolism (IEM): The ClinGen IEM Working Group and the Phenylalanine Hydroxylase Gene. Hum. Mutat. 2018, 39, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, S.; Wang, S.; Zeng, Q.; Chen, Y.; Fang, T.; Zhang, Y.; Zhou, Y.; Zhang, Y.; Wang, K.; et al. Cancer SIGVAR: A semiautomated interpretation tool for germline variants of hereditary cancer-related genes. Hum. Mutat. 2021, 42, 359–372. [Google Scholar] [CrossRef] [PubMed]
- TNO. The Newborn Blood Spot Screening Monitor 2019; Rijksinstituut voor Volksgezondheid en Milieu-Centrum voor Bevolkingsonderzoek: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Bienvenu, T.; Lopez, M.; Girodon, E. Molecular Diagnosis and Genetic Counseling of Cystic Fibrosis and Related Disorders: New Challenges. Genes 2020, 11, 619. [Google Scholar] [CrossRef] [PubMed]
- Farrell, P.M.; Rock, M.J.; Baker, M.W. The Impact of the CFTR Gene Discovery on Cystic Fibrosis Diagnosis, Counseling, and Preventive Therapy. Genes 2020, 11, 401. [Google Scholar] [CrossRef] [Green Version]
- Arnason, V. Coding and Consent: Moral Challenges of the Database Project in Iceland. Bioethics 2004, 18, 27–49. [Google Scholar] [CrossRef]
- Andersen, B.; Arnason, E. Iceland’s database is ethically questionable. BMJ 1999, 318, 1565. [Google Scholar] [CrossRef]
- Hauksson, P. Icelanders opt out of genetic database. Nature 1999, 400, 707–708. [Google Scholar] [CrossRef]
- Stefansdottir, V.; Thorolfsdottir, E.; Hognason, H.B.; Patch, C.; van El, C.; Hentze, S.; Cordier, C.; Mendes, Á.; Jonsson, J.J. Web-based return of BRCA2 research results: One-year genetic counselling experience in Iceland. Eur. J. Hum. Genet. 2020, 28, 1656–1661. [Google Scholar] [CrossRef]
- Loeber, J.G.; Platis, D.; Zetterström, R.H.; Almashanu, S.; Boemer, F.; Bonham, J.R.; Borde, P.; Brincat, I.; Cheillan, D.; Dekkers, E.; et al. Neonatal Screening in Europe Revisited: An ISNS Perspective on the Current State and Developments Since 2010. Int. J. Neonatal Screen. 2021, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Van Der Burg, S.; Verweij, M. Maintaining Trust in Newborn Screening. Hastings Cent. Rep. 2012, 42, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Blom, M.; Bredius, R.G.; Jansen, M.E.; Weijman, G.; Kemper, E.A.; Vermont, C.L.; Hollink, I.H.; Dik, W.A.; van Montfrans, J.M.; van Gijn, M.E.; et al. Parents’ Perspectives and Societal Acceptance of Implementation of Newborn Screening for SCID in the Netherlands. J. Clin. Immunol. 2021, 41, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Parens, E.; Appelbaum, P.S. On What We Have Learned and Still Need to Learn about the Psychosocial Impacts of Genetic Testing. Hastings Cent. Rep. 2019, 49, S2–S9. [Google Scholar] [CrossRef] [Green Version]
- Lewis, T. 23 and Baby. Nature 2019, 576, S8–S12. [Google Scholar] [CrossRef] [Green Version]
- Brenner, S. Life sentences: Detective Rummage investigates. Genome Biol. 2002, 3, 1–2. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veldman, A.; Kiewiet, M.B.G.; Heiner-Fokkema, M.R.; Nelen, M.R.; Sinke, R.J.; Sikkema-Raddatz, B.; Voorhoeve, E.; Westra, D.; Dollé, M.E.T.; Schielen, P.C.J.I.; et al. Towards Next-Generation Sequencing (NGS)-Based Newborn Screening: A Technical Study to Prepare for the Challenges Ahead. Int. J. Neonatal Screen. 2022, 8, 17. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8010017
Veldman A, Kiewiet MBG, Heiner-Fokkema MR, Nelen MR, Sinke RJ, Sikkema-Raddatz B, Voorhoeve E, Westra D, Dollé MET, Schielen PCJI, et al. Towards Next-Generation Sequencing (NGS)-Based Newborn Screening: A Technical Study to Prepare for the Challenges Ahead. International Journal of Neonatal Screening. 2022; 8(1):17. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8010017
Chicago/Turabian StyleVeldman, Abigail, Mensiena B. G. Kiewiet, Margaretha Rebecca Heiner-Fokkema, Marcel R. Nelen, Richard J. Sinke, Birgit Sikkema-Raddatz, Els Voorhoeve, Dineke Westra, Martijn E. T. Dollé, Peter C. J. I. Schielen, and et al. 2022. "Towards Next-Generation Sequencing (NGS)-Based Newborn Screening: A Technical Study to Prepare for the Challenges Ahead" International Journal of Neonatal Screening 8, no. 1: 17. https://0-doi-org.brum.beds.ac.uk/10.3390/ijns8010017