Ultrasonic Navigation for the Treatment of Medication-Related Jaw Osteonecrosis Involving the Inferior Alveolar Nerve: A Case Report and Protocol Review

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Experimental Design
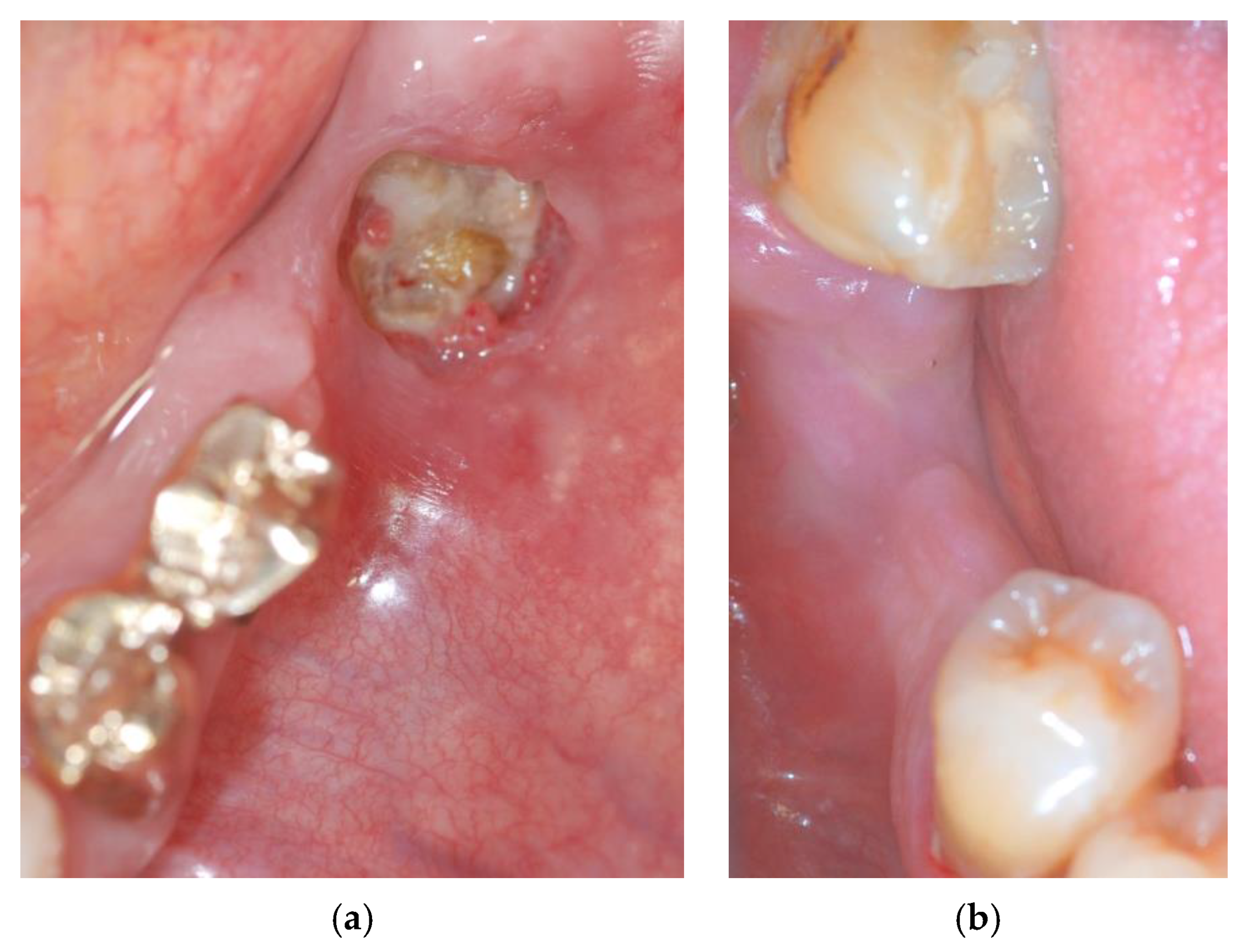
2.1. Case Presentation
2.2. Materials
- ImplaNav (BresMedical, Sydney, Australia) navigation system.
- Esacrom, (Imola, Italy) piezo-surgical instruments.
3. Procedure
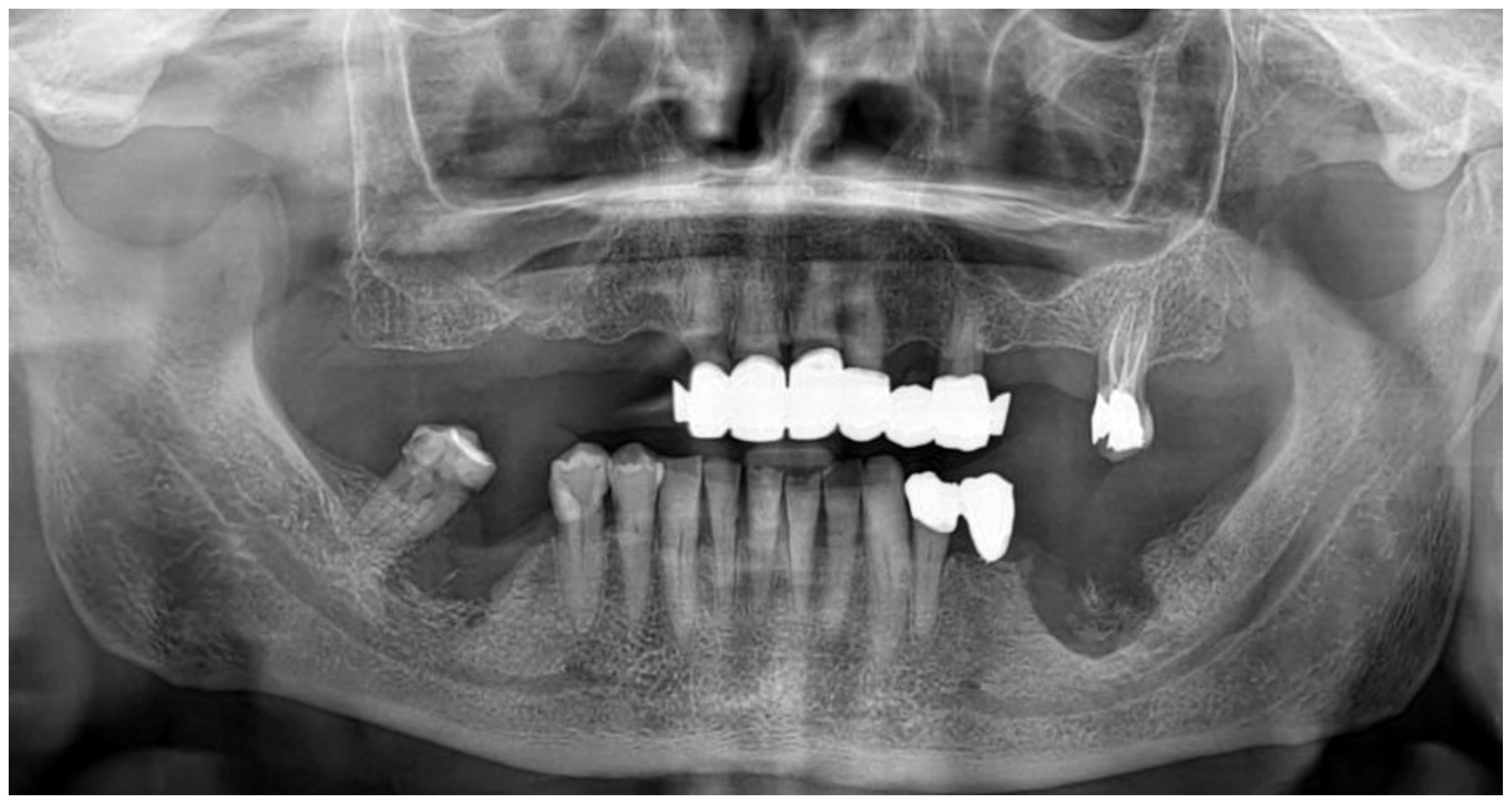
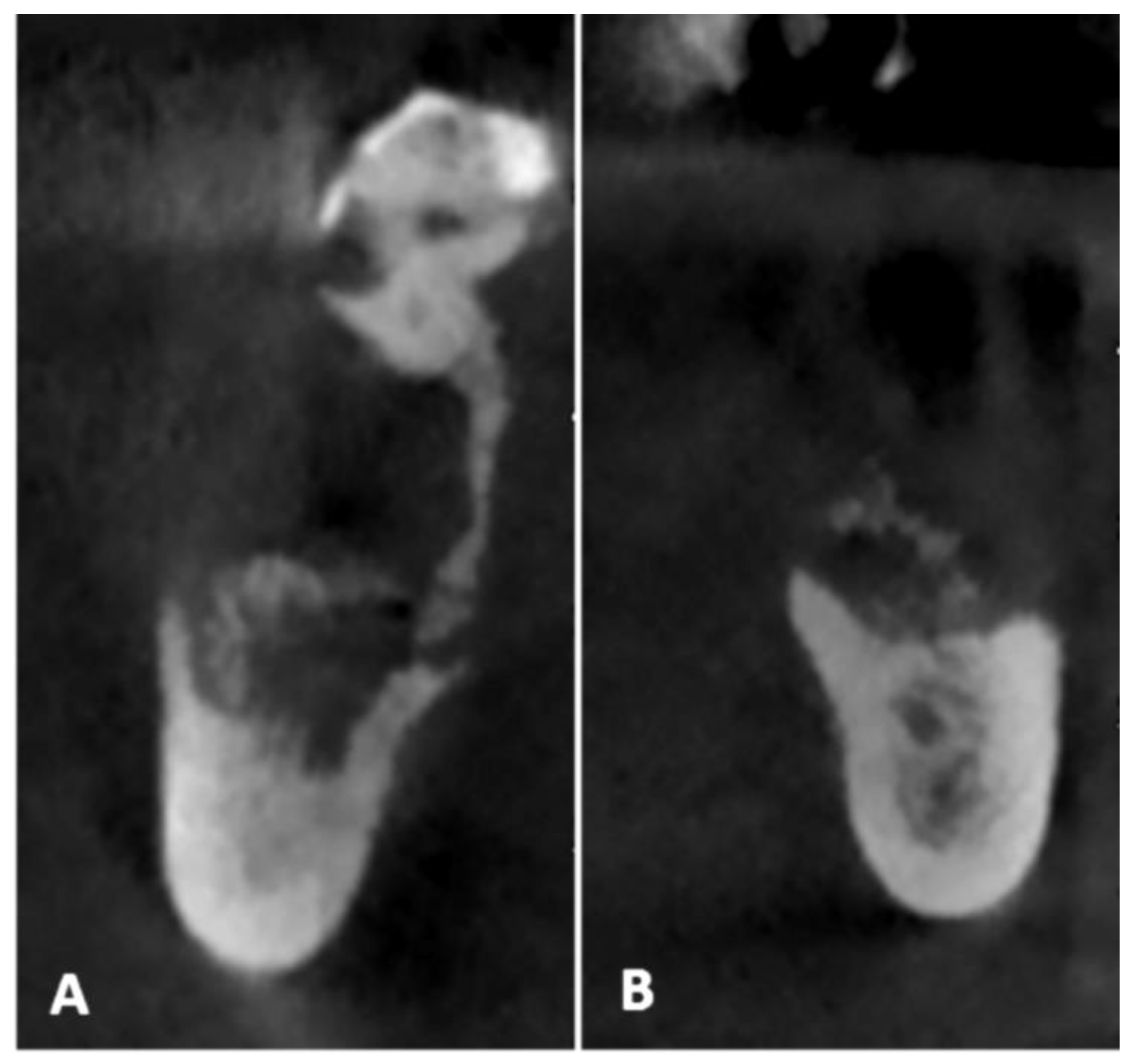
- Pre-operative evaluation. The patient undergoes a cone-beam CT exam with a reference plate containing the fiducial markers, fixed on his inferior teeth. The Digital Imaging and Communications in Medicine (DICOM) were imported into the navigation software.
- Just before surgery, the patient wears the reference plate with the patient reference tool attached onto it and the handle reference tool on the piezoelectric handpiece. The calibration of the navigator system, accomplished in this phase, is performed through a connection reproducing the universal joint for the drills embedded into the calibration tool, allowing the navigation system software to identify the drill position and axis in relation to the patient position and to the CT imaging data.
- Surgery timing. The surgeon can follow in real time the ultrasonic tip position onto the system screen displaying the CBCT images and safely identify and remove the necrotic bone surrounding the inferior alveolar nerve on the right side.
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Voss, P.J.; Poxleitner, P.; Schmelzeisen, R.; Stricker, A.; Semper-Hogg, W. Update MRONJ and perspectives of its treatment. J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Beth-Tasdogan, N.H.; Mayer, B.; Hussein, H.; Zolk, O. Interventions for managing medication-related osteonecrosis of the jaw. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- El-Rabbany, M.; Lam, D.K.; Shah, P.S.; Azarpazhooh, A. Surgical Management of Medication-Related Osteonecrosis of the Jaw Is Associated with Improved Disease Resolution: A Retrospective Cohort Study. J. Oral Maxillofac. Surg. 2019, 77, 1816–1822. [Google Scholar] [CrossRef]
- Kagami, H.; Inoue, M.; Kobayashi, A.; Taguchi, A.; Li, X.; Yoshizawa, M. Issues with the surgical treatment of antiresorptive agent-related osteonecrosis of the jaws. Oral Dis. 2018, 24, 52–56. [Google Scholar] [CrossRef]
- Blus, C.; Giannelli, G.; Szmukler-Moncler, S.; Orru, G. Treatment of medication-related osteonecrosis of the jaws (MRONJ) with ultrasonic piezoelectric bone surgery. A case series of 20 treated sites. Oral Maxillofac. Surg. 2017, 21, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, A.; Badiali, G.; Piersanti, L.; Marchetti, C. Computer-assisted piezoelectric surgery: A navigated approach toward performance of craniomaxillofacial osteotomies. J. Craniofac. Surg. 2015, 26, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.C.S.; Batista, F.R.S.; Jacob, R.G.M.; Nogueira, L.M.; Carvalho, A.C.G.S.; Gealh, W.C.; Garcia-Júnior, I.R.; Okamoto, R. Comparative Evaluation of Cell Viability Immediately After Osteotomy for Implants with Drills and Piezosurgery: Immunohistochemistry Analysis. J. Craniofac. Surg. 2018, 29, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Cullum, D.R.; Sheikh, A. Implant Placement Is More Accurate Using Dynamic Navigation. J. Oral Maxillofac. Surg. 2017, 75, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Taraschi, V.; Andrea, Z.; Ferri, A.; Marchetti, C. Dynamic navigation: A prospective clinical trial to evaluate the accuracy of implant placement. Int. J. Comput. Dent. 2019, 22, 139–147. [Google Scholar] [PubMed]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Taraschi, V.; Vercellotti, T.; Ben-Nissan, B.; Marchetti, C. Three-Dimensional Implant Positioning with a Piezosurgery Implant Site Preparation Technique and an Intraoral Surgical Navigation System: Case Report. Int. J. Oral Maxillofac. Implants 2017, 32, e163–e165. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef] [PubMed]
- Mauceri, R.; Panzarella, V.; Morreale, I.; Campisi, G. Medication-related osteonecrosis of the jaw in a cancer patient receiving lenvatinib. Int. J. Oral Maxillofac. Surg. 2019, 48, 1530–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blus, C.; Szmukler-Moncler, S.; Orru, G.; Denotti, G.; Piras, A.; Piras, V. Bactericide effect of vibrating ultra-sonic (piezo-surgery) tips. An in vitro study. Clin. Oral Implants Res. 2009, 20, 905. [Google Scholar]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellegrino, G.; Pavanelli, F.; Ferri, A.; Lizio, G.; Parrulli, R.; Marchetti, C. Ultrasonic Navigation for the Treatment of Medication-Related Jaw Osteonecrosis Involving the Inferior Alveolar Nerve: A Case Report and Protocol Review. Methods Protoc. 2020, 3, 70. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3040070
Pellegrino G, Pavanelli F, Ferri A, Lizio G, Parrulli R, Marchetti C. Ultrasonic Navigation for the Treatment of Medication-Related Jaw Osteonecrosis Involving the Inferior Alveolar Nerve: A Case Report and Protocol Review. Methods and Protocols. 2020; 3(4):70. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3040070
Chicago/Turabian StylePellegrino, Gerardo, Francesca Pavanelli, Agnese Ferri, Giuseppe Lizio, Roberto Parrulli, and Claudio Marchetti. 2020. "Ultrasonic Navigation for the Treatment of Medication-Related Jaw Osteonecrosis Involving the Inferior Alveolar Nerve: A Case Report and Protocol Review" Methods and Protocols 3, no. 4: 70. https://0-doi-org.brum.beds.ac.uk/10.3390/mps3040070