Novel In Vivo Mouse Cryoablation Model to Explore Unique Therapeutic Approaches for Premalignant Columnar Lesions

Abstract
:1. Introduction
2. Experimental Design
2.1. Materials
- Slip tip syringe with 26 G needle/vehicle solutions (BD, Franklin Lakes, NJ, USA; cat. no.: 309597);
- 5-0 vicryl absorbable suture/closure mouse muscle and skin (Ethicon, Somerville, NJ, USA; cat. no.: VCP303H);
- 5-0 Prolene no absorbable suture/for stomach opening exposure (Ethicon, Somerville, NJ, USA; cat. no.: 8720H);
- 8-0 Prolene no absorbable suture/closure mouse stomach (Ethicon, Somerville, NJ, USA; cat. no.: 8741H);
- TransporeTM medical tape/mouse fixation (3M, St. Paul, MN, USA; cat. no.: 70200739582);
- Castroviejo needle holder (Fine Science Tools; 12060-01);
- Mayo scissor/cut skin (Fine Science Tools, Heidelberg, DEU; cat. no.: 14010-15);
- Fine scissors/cut stomach, muscle tissue (Fine Science Tools, Heidelberg, DEU; cat. no.: 14058-09);
- Adson forceps—DeBakey serrations/grasp tissues (Fine Science Tools, Heidelberg, DEU; cat. no.: 11616-15);
- Iris forceps/grasp tissues (Fine Science Tools, Heidelberg, DEU; cat. no.: 11064-07);
- Halsted-mosquito hemostats/needle holder for stomach opening exposure (Fine Science Tools, Heidelberg, DEU; cat. no.: 13009-12);
- Feeding needle/oral gavage of treatment (Fine Science Tools, Heidelberg, DEU; cat. no.: 18065-20);
- 100 × 100 mm gauze pads (B. Braun, Melsungen, DEU; cat. no.: BRAU9031324);
- 50 × 50 mm gauze pads (B. Braun, Melsungen, DEU; cat. no.: BRAU9031308);
- Cotton swaps (Heinz Herenz Hamburg, Hamburg, DEU; cat. no.: HERE1031318);
- Betadine® solution/disinfect skin (Mylan, Canonsburg, PA, USA; cat. no.: NDC 67618-155-16);
- Sterile saline solution (NaCl 0.9%)/for injection and treatment dilutions (B. Braun, Melsungen, DEU; cat. no.: 1531131);
- Water for injection (B. Braun, Melsungen, DEU; cat. no.: 2351744);
- Baby milk powder (any commercial brand);
- Meloxicam/pain killer (Dopharma, Raamsdonksveer, NLD; cat. no.: 16A06-08C3);
- Baytril® 25 mg/mL/antibiotic for the drinking water (Bayer, Leverkusen, DEU; cat. no.: 04007221042419);
- Omeprazole/anti-acid treatment (Teva Pharmaceuticals, Petah Tikva, ISR);
- Lubruthal/eye ointment (Dechra Pharmaceuticals, Northwich, GBR; cat. No.: 570117031-3291);
- SuperFrost Plus™ adhesion slides (Thermo Fisher Scientific, Waltham, MA, USA; cat. No.: J1800AMNZ).
2.2. Equipment
- Cage heating pad (Braintree Scientific, Braintree, MA, USA; cat. no.: HP 1M);
- Rodent anesthesia circuit;
- Induction chamber;
- Bead sterilizer (Harvard Apparatus, Holiliston, MA, USA; cat. no.: 72-0125);
- 1 mm Cryo-pen + liquid nitrous oxide (N2O) cartridge (Cryoalfa LUX, Radebeu, DEU; cat. no.: CA-L);
- Weight scale;
- Histology embedding station;
- Leica DM6 fluorescent microscope (Leica, Wetzlar, DEU);
- CryoStar NX50 cryostat (Thermo Fisher Scientific, Waltham, MA, USA).
2.3. Reagents
- Phosphate-buffered saline (PBS) (Thermo Fisher Scientific, Waltham, MA, USA; cat. no.: 10010023);
- Formalin solution, neutral buffered, 10% (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: HT501128-4L);
- Ethanol (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: 51976-500ML-F);
- Xylene (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: 108298);
- Hematoxylin solution according to Mayer (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: 51275);
- Eosin Y solution 1% (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: 1170811000);
- DPX Mountant (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: 06522-100ML);
- Tissue-Plus TM O.C.T. compound (Fisher Scientific, Waltham, MA, USA; cat. no.: 23-730-571);
- DAPI (4’,6-diamidino-2-phenylindole, dihydrochloride) (Thermo Fisher Scientific, Waltham, MA, USA; cat. no.: 62247);
- Recombinant mouse noggin protein (R&D Systems, McKinley, MN, USA; cat. no.: 1967-NG);
- Tamoxifen (Sigma-Aldrich, St. Louis, MO, USA; cat. no.: T5648).
2.4. Animals
3. Procedure
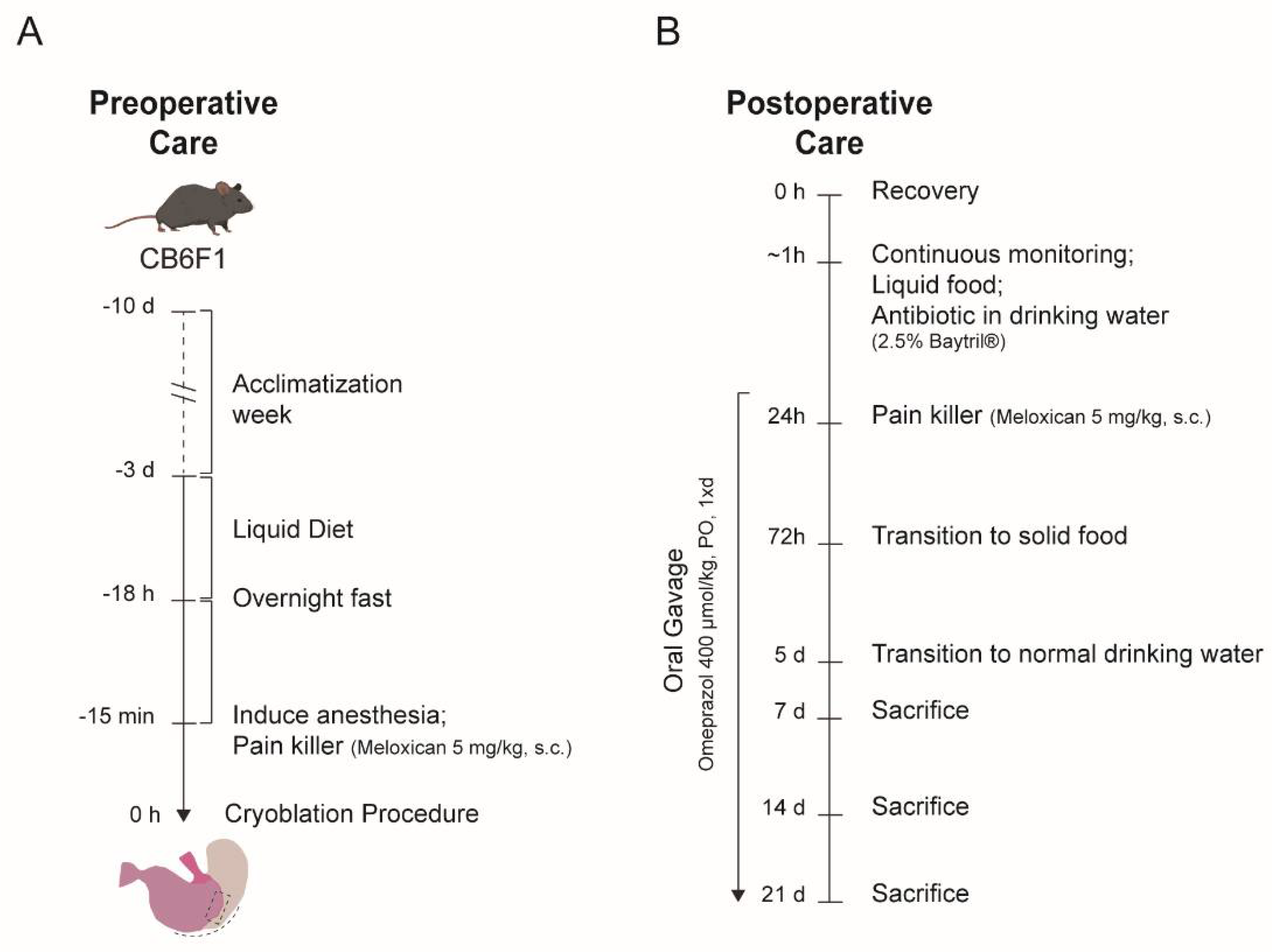
3.1. Preoperative Care. Time for Completion: 3 Days (Not Accounting Mice Acclimatation)
- Remove any solid pellet food from the +/+ IVC cages 3 days before the cryoablation procedure.
- Replace the pellet food for liquid food (commercial baby milk prepared according to the supplier in drinking water).
- Day prior to the cryoablation procedure (approximately 18 h prior), remove liquid food for overnight fasting (Figure 1A). Leave drinking water available ad libitum.
3.2. Cryoablation Procedure. Time for Completion: 30 min per Mouse
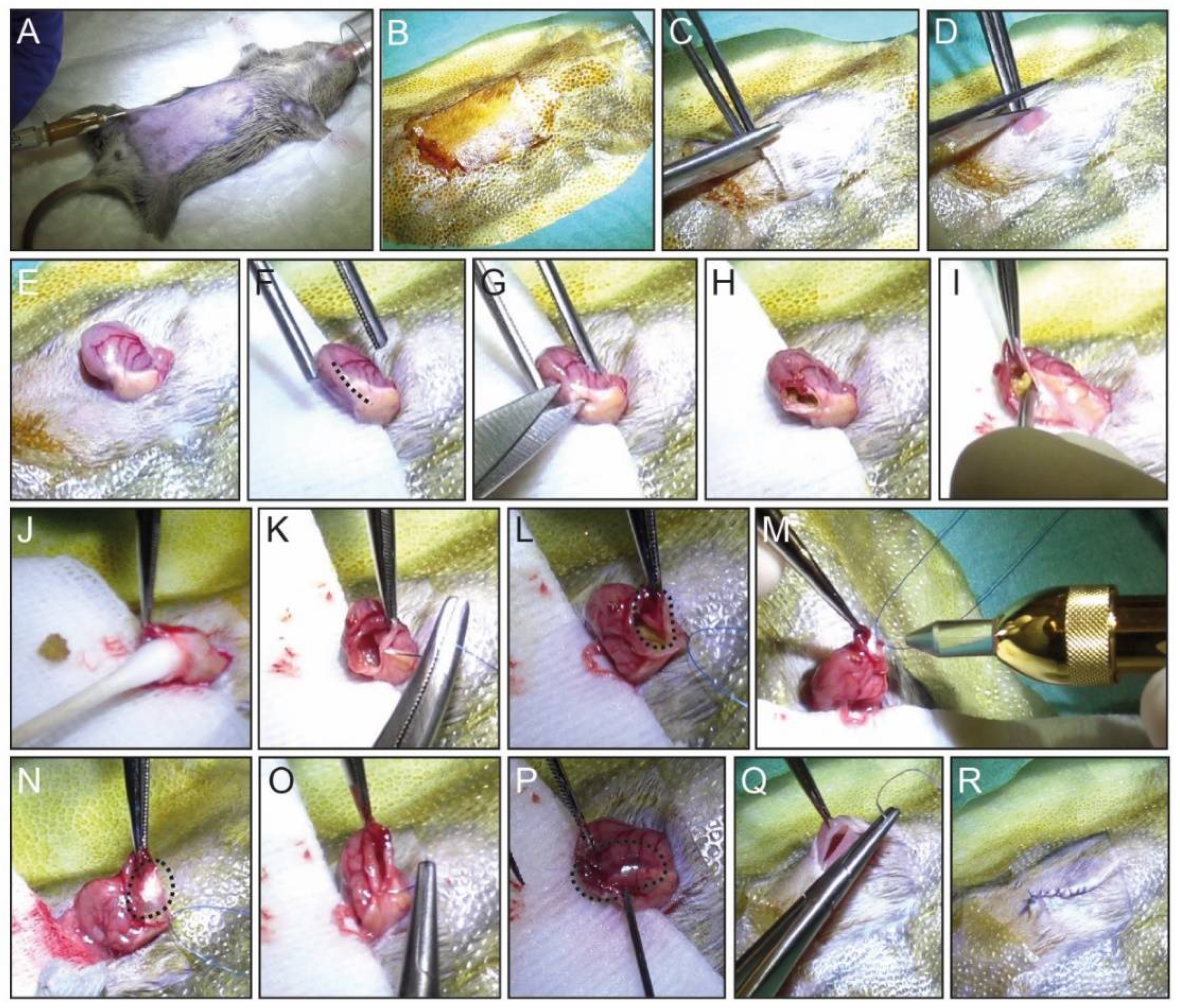
- In the non-sterile area, place the mouse in the induction chamber with 2% isoflurane. Under anesthesia, weigh the mouse and register his weight. Shave the abdominal area and transfer the mouse to the sterile field.
- Mobilize the mouse in the sterile field with medical tape, place the anesthesia cone on the mouse nose, and apply eye ointment to prevent corneal damage (Figure 2A).
-
![Mps 04 00006 i001]()
- CRITICAL STEP: It is important to prepare the sterile field onto a heating pad (37 °C) to be able to maintain the mouse body temperature throughout the procedure.
-
- Administer pain killer (Meloxicam, 5 mg/kg body weight) with a single subcutaneous (s.c.) injection with a 26 G needle syringe (Figure 2A).
- Clean the skin with betadine solution (Figure 2B).
- Start the surgical procedure by lifting the mouse skin with forceps and making a midline vertical incision on the abdomen, of about 2 cm (Figure 2C,D).
- Use the round atraumatic forceps to reach the stomach inside the intraperitoneal cavity.
- Pull the stomach out from the intraperitoneal cavity for better visibility and performance (Figure 2E).
- Embed a sterile medical gauze pad with warm PBS and place it between the stomach and the mouse skin (Figure 2F).
-
![Mps 04 00006 i001]()
- CRITICAL STEP: The use of sterile gauze pad is important to avoid direct contact between the two distinguish surfaces, stomach and skin. In addition, it is essential when removing the stomach content in step 10. This step will minimize possible infection post-surgery.
-
- Using a fine scissor, make an incision of 0.75 to 1 cm long in the middle of the greater curvature of the mouse stomach including the SCJ as shown in Figure 2F,G.
- Once opened, remove the stomach content with the help of round-tip forceps and cotton swaps until the area at the SCJ for the ablation is clean (Figure 2H–J).
- For better visualization of the stomach interior, make a stich with a 5/0 non-absorbable suture and hold it with a needle holder and set it aside (Figure 2K).
- Apply liquid N2O twice in the same area for 5 to 10 s each time, waiting for the tissue to thaw in between applications.
-
![Mps 04 00006 i001]()
- CRITICAL STEP: The time of each liquid N2O application depends on how stretched the mouse stomach is, i.e., how thin the stomach wall is. It is important not to exceed the duration of 10 s and pause briefly between applications to assess the damage and avoid perforation of the stomach wall.
-
![Mps 04 00006 i001]()
- WARNING: Cryoalpha pen allows for precise and accurate applications of liquid N2O, which can produce temperatures of −89 °C. Cryoalpha pen is a safe instrument and should be held like a pencil when in use, only aiming the applicator to the area of interest.
-
- Close the stomach using an 8/0 non-absorbable suture with continuous stiches (Figure 2O). The ablated area can be observed on the exterior of stomach by a darker red color of the wall (Figure 2P, dotted line).
-
![Mps 04 00006 i001]()
- CRITICAL STEP: Carefully inspect if the stomach is completely closed. Small openings in the mouse stomach can lead to leakage of the stomach content into the peritoneal cavity.
-
- Place the ablated stomach back inside the intraperitoneal cavity and close the abdominal wall and skin separately by using and a 5/0 vicryl absorbable suture (Figure 2Q,R).

3.3. Postoperative Care. Time for Completion: Up to 21 Days
- Remove the mouse from the sterile field and place the mouse back to the +/+IVC cage in the ventilated rack onto a warm pad for the first 24 h postoperative hours.
- Add liquid food (baby milk) in the +/+ IVC cage and antibiotic (Baytril®, 25 mg/mL) in the drinking water
- Observe the mouse recovery from the anesthesia and register any signs of discomfort.
- 4.
- NOTE: Animals need to be euthanized immediately if a humane endpoint is reached after surgery or during the follow up period. In our institution, humane endpoints include severe weight loss (>15% body weight loss compared to the initial weight, an extended period of weight loss without improvement after 48 h) or severe dehydration for more than 72 h without improvement after s.c. saline injections.
- 5.
- From day 1 post-cryoablation and throughout the experiment, give daily oral gavage of anti-acid (Omeprazole, 400 µmol/kg).
- 6.
- On day 3 post-cryoablation, replace liquid food by normal pellet food ad libitum.
- 7.
- On day 5 post-cryoablation replace antibiotic water by tap water ad libitum.
3.4. End of the Experiment. Time for Completion: Approximatly 30 min per Mouse
- Cull the mice at the pre-determined experimental endpoints (t = 7, 14, and 21 days) by placing the mice in a CO2 chamber.
- Immediately after culling, remove mice from the CO2 chamber, shave the abdominal area, and open using a round tips scissor by making an upper-midline vertical incision of the abdomen.
- Dissect and isolate the stomach.
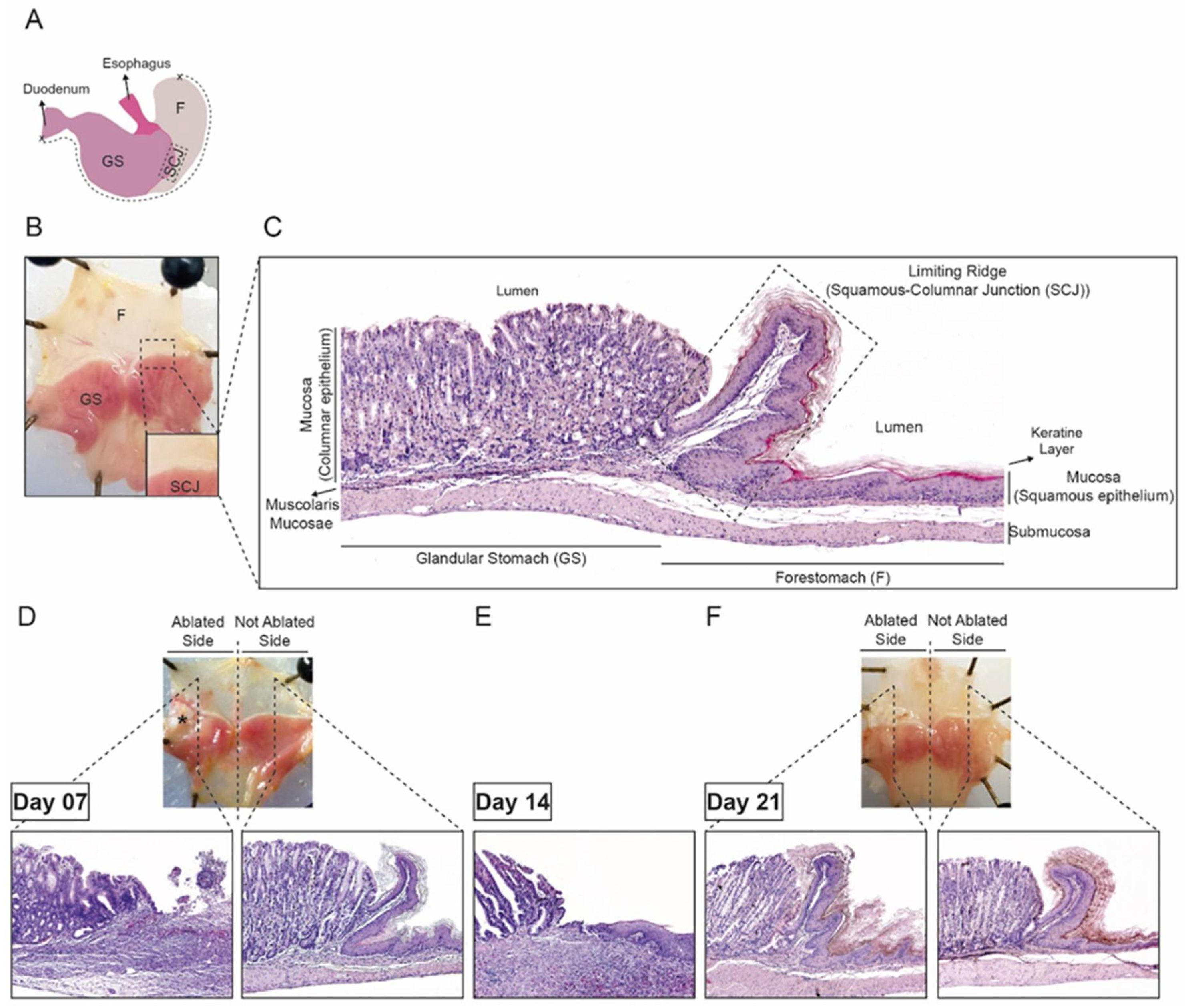
- Holding the isolated stomach, with the stomach curvature upwards, open the stomach from the duodenum opening to the forestomach part along the greater curvature (Figure 3A).
- Remove the stomach content and clean with PBS.
- Pin the open stomach to a paraffin block to flatten the stomach for histological preparation.
3.5. Histological Preparation
3.5.1. Tissue Fixation and Slide Preparation. Time for Completion: 3 Days
- Fix the pinned stomach into 10% neutral buffered formalin solution for 24 h.
- Transfer the tissues to labeled histology cassettes and dehydrate the tissues in a series of increasing ethanol percentage solution (70%, 80%, 90%, and 96% ethanol) until 100% ethanol, during 1 h for each ethanol grade.
- Clean tissue cassettes in 100% xylene for 1 h.
- Place the cleaned tissue cassettes in a high-temperature paraffin bath (60 °C) overnight.
- Transfer the cassettes to an embedding station and cut the fixed tissue in four pieces as represented in Figure 3D,F.
- Place tissue pieces in a mold and embed it in paraffin.
- Cut the tissue paraffin blocks as 5 µm sections and place onto a slide.
- Dry the tissue slides at 37 °C for at least 16 h.
3.5.2. Hematoxylin and Eosin Staining. Time of Completion: 2 h and 30 min
- Deparaffinize the tissue slides in 100% xylene for 10 min.
- Rehydrate the slides in a graded series of decreasing ethanol percentage solutions (100%, 96%, 90%, 80%, and 70%) for 10 min each grade.
- Place the slides in hematoxylin staining solution for 10 min at room temperature.
- Wash slides in running water for 5 min.
- Counter stain with 1% eosin solution for 5 min.
- Dehydrate the tissue slides with increase grade of ethanol percentage (70%, 80%, 90%, 96%, and 100%) for 10 min each grade.
- Clean the slides with 2× xylene for 2 min each.
- Let the slides dry in the flow cabinet and mount with DPX mounting medium and a coverslip.
3.5.3. Tissue Cryopreservation. Time of Completion: 10 min per Mouse Stomach
- Cut the pinned stomach from K5-GFP mice into 4 pieces (<5 mm) as represented in Figure 3D,F.
- Place the tissue pieces flat inside a tinned-metal sample container or a cryovial.
- Snap frozen in liquid nitrogen and store the samples at −80 °C until further analysis.
3.5.4. Cryo Slide Preparation and Fluorescence Microscopy: Time of Completion: 30 min per Sample
- In a CryoStat station, remove the cryopreserved tissue and place it onto a cold base.
- Cover the tissue with cryo-embedding media (OTC).
- Place the mold in the Peltier fast-freezing platform of the cryostat to ensure the tissue is frozen before sectioning.
- Cut the frozen tissue block into 6 µm sections and place onto a Superfrost Plus adhesion glass slide.
- Dry the slides at room temperature and store them in a slide box at −20 °C for later use.
- Stain the slides with DAPI (1:1000) for nuclear staining and visualize under a fluorescent microscope.
4. Expected Results
4.1. Establishment of the Cryoablation Mouse Model
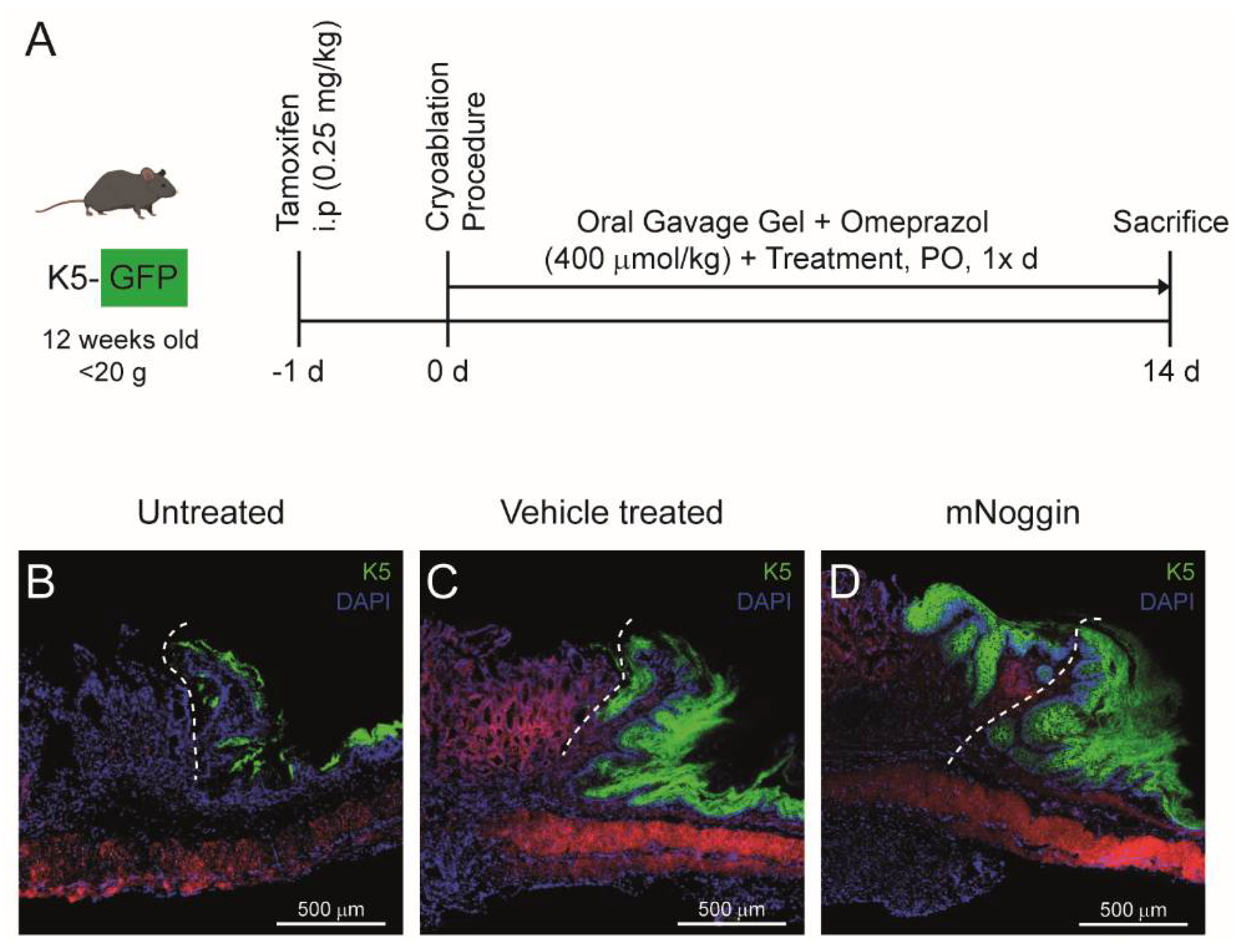
4.2. Intervening with the Regenerative Process of the Neo-Columnar Epithelium at the SCJ
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Giroux, V.; Rustgi, A.K. Metaplasia: Tissue injury adaptation and a precursor to the dysplasia-cancer sequence. Nat. Rev. Cancer 2017, 17, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Milano, F.; Van Baal, J.W.; Buttar, N.S.; Rygiel, A.M.; De Kort, F.; DeMars, C.J.; Rosmolen, W.D.; Bergman, J.J.; Van Marle, J.; Wang, K.K.; et al. Bone morphogenetic protein 4 expressed in esophagitis induces a columnar phenotype in esophageal squamous cells. Gastroenterology 2007, 132, 2412–2421. [Google Scholar] [CrossRef] [PubMed]
- Mari, L.; Milano, F.; Parikh, K.; Straub, D.; Everts, V.; Hoeben, K.K.; Fockens, P.; Buttar, N.S.; Krishnadath, K.K. A pSMAD/CDX2 complex is essential for the intestinalization of epithelial metaplasia. Cell Rep. 2014, 7, 1197–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, Y.; Al-Kaabi, A.; Shaheen, N.J.; Chak, A.; Blum, A.; Souza, R.F.; Di Pietro, M.; Iyer, P.G.; Pech, O.; Fitzgerald, R.C.; et al. Barrett oesophagus. Nat. Rev. Dis. Primers 2019, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Quinlan, J.M.; Colleypriest, B.J.; Farrant, M.; Tosh, D. Epithelial metaplasia and the development of cancer. Biochim. Biophys. Acta 2007, 1776, 10–21. [Google Scholar] [CrossRef]
- Jencks, D.S.; Adam, J.D.; Borum, M.L.; Koh, J.M.; Stephen, S.; Doman, D.B. Overview of Current Concepts in Gastric Intestinal Metaplasia and Gastric Cancer. Gastroenterol. Hepatol. (N. Y.) 2018, 14, 92–101. [Google Scholar]
- Chandrasoma, P.T. Histologic definition of gastro-esophageal reflux disease. Curr. Opin. Gastroenterol. 2013, 29, 460–467. [Google Scholar] [CrossRef]
- Munoz-Largacha, J.A.; Litle, V.R. Endoscopic mucosal ablation and resection of Barrett’s esophagus and related diseases. J. Vis. Surg. 2017, 3, 128. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.N.; Green, J.; Wang, Z.; Deng, Y.; Qiao, M.; Peabody, M.; Zhang, Q.; Ye, J.; Yan, Z.; Denduluri, S.; et al. Bone Morphogenetic Protein (BMP) signaling in development and human diseases. Genes Dis. 2014, 1, 87–105. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.J.; Choi, A.Y.; Truong, C.D.; Yeh, M.M.; Hwang, J.H. Diagnosis and Management of Gastric Intestinal Metaplasia: Current Status and Future Directions. Gut Liver 2019, 13, 596–603. [Google Scholar] [CrossRef]
- Sharma, P.; Shaheen, N.J.; Katzka, D.; Bergman, J.J. AGA Clinical Practice Update on Endoscopic Treatment of Barrett’s Esophagus With Dysplasia and/or Early Cancer: Expert Review. Gastroenterology 2020, 158, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banks, M.; Graham, D.; Jansen, M.; Gotoda, T.; Coda, S.; Di Pietro, M.; Uedo, N.; Bhandari, P.; Pritchard, D.M.; Kuipers, E.J.; et al. British Society of Gastroenterology guidelines on the diagnosis and management of patients at risk of gastric adenocarcinoma. Gut 2019, 68, 1545–1575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinis-Ribeiro, M.; Areia, M.; De Vries, A.C.; Marcos-Pinto, R.; Monteiro-Soares, M.; O’connor, A.; Pereira, C.; Pimentel-Nunes, P.; Correia, R.; Ensari, A.; et al. Management of precancerous conditions and lesions in the stomach (MAPS): Guideline from the European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter Study Group (EHSG), European Society of Pathology (ESP), and the Sociedade Portuguesa de Endoscopia Digestiva (SPED). Endoscopy 2012, 44, 74–94. [Google Scholar] [PubMed] [Green Version]
- Liu, K.S.; Wong, I.O.; Leung, W.K. Helicobacter pylori associated gastric intestinal metaplasia: Treatment and surveillance. World J. Gastroenterol. 2016, 22, 1311–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, W.K.; Tong, D.K.; Leung, S.Y.; Chan, F.S.; Tong, T.S.; Ho, R.S.; Chu, K.M.; Law, S.Y. Treatment of Gastric Metaplasia or Dysplasia by Endoscopic Radiofrequency Ablation: A Pilot Study. Hepatogastroenterology 2015, 62, 748–751. [Google Scholar]
- Scott, D.R.; Sachs, G.; Marcus, E.A. The role of acid inhibition in Helicobacter pylori eradication. F1000Research 2016, 5. [Google Scholar] [CrossRef] [Green Version]
- Ierardi, E.; Losurdo, G.; La Fortezza, R.F.; Principi, M.; Barone, M.; Di Leo, A. Optimizing proton pump inhibitors in Helicobacter pylori treatment: Old and new tricks to improve effectiveness. World J. Gastroenterol. 2019, 25, 5097–5104. [Google Scholar] [CrossRef]
- Eluri, S.; Shaheen, N.J. Barrett’s esophagus: Diagnosis and management. Gastrointest. Endosc. 2017, 85, 889–903. [Google Scholar] [CrossRef] [Green Version]
- Read, M.D.; Krishnadath, K.K.; Clemons, N.J.; Phillips, W.A. Preclinical models for the study of Barrett’s carcinogenesis. Ann. N. Y. Acad. Sci. 2018, 1434, 139–148. [Google Scholar] [CrossRef]
- Di Pietro, M.; Alzoubaidi, D.; Fitzgerald, R.C. Barrett’s esophagus and cancer risk: How research advances can impact clinical practice. Gut Liver 2014, 8, 356–370. [Google Scholar] [CrossRef] [Green Version]
- Singh, T.; Sanaka, M.R.; Thota, P.N. Endoscopic therapy for Barrett’s esophagus and early esophageal cancer: Where do we go from here? World J. Gastrointest. Endosc. 2018, 10, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Bragdon, B.; Moseychuk, O.; Saldanha, S.; King, D.; Julian, J.; Nohe, A. Bone morphogenetic proteins: A critical review. Cell. Signal. 2011, 23, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Que, J.; Garman, K.S.; Souza, R.F.; Spechler, S.J. Pathogenesis and Cells of Origin of Barrett’s Esophagus. Gastroenterology 2019, 157, 349.e1–364.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, M.; Li, H.; Zhang, Y.; Yang, Y.; Lu, R.; Liu, K.; Lin, S.; Lan, X.; Wang, H.; Wu, H.; et al. Transitional basal cells at the squamous-columnar junction generate Barrett’s oesophagus. Nature 2017, 550, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Krishnadath, K.K.; Wang, K.K. Molecular pathogenesis of Barrett esophagus: Current evidence. Gastroenterol. Clin. N. Am. 2015, 44, 233–247. [Google Scholar] [CrossRef]
- Liang, C.C.; You, L.R.; Chang, J.L.; Tsai, T.F.; Chen, C.M. Transgenic mice exhibiting inducible and spontaneous Cre activities driven by a bovine keratin 5 promoter that can be used for the conditional analysis of basal epithelial cells in multiple organs. J. Biomed. Sci. 2009, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Krause, C.; Guzman, A.; Knaus, P. Noggin. Int. J. Biochem. Cell Biol. 2011, 43, 478–481. [Google Scholar] [CrossRef]
- Que, J.; Choi, M.; Ziel, J.W.; Klingensmith, J.; Hogan, B.L. Morphogenesis of the trachea and esophagus: Current players and new roles for noggin and Bmps. Differentiation 2006, 74, 422–437. [Google Scholar] [CrossRef]
- Calpe, S.; Wagner, K.; El Khattabi, M.; Rutten, L.; Zimberlin, C.; Dolk, E.; Verrips, C.T.; Medema, J.P.; Spits, H.; Krishnadath, K.K. Effective Inhibition of Bone Morphogenetic Protein Function by Highly Specific Llama-Derived Antibodies. Mol. Cancer Ther. 2015, 14, 2527–2540. [Google Scholar] [CrossRef] [Green Version]
- Calpe, S.; Correia, A.C.; Sancho-Serra, M.D.; Krishnadath, K.K. Comparison of newly developed anti-bone morphogenetic protein 4 llama-derived antibodies with commercially available BMP4 inhibitors. MAbs 2016, 8, 678–688. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Problem | Procedure Step | Possible Reason | Solution |
|---|---|---|---|
| Stomach perforation | Figure 2M | Extensive exposure to liquid N2O | This step needs to be adjusted depending on the animal model used. K5-GFP mice are more fragile than CB6F1, therefore the time of exposure needs to be slightly less than with the CB6F1 mice (2× 5 to 8 s for K5-GFP and 2 × 8 to 10 s for CB6F1 mice). Make sure that the stomach is outside the abdominal cavity to avoid exposure of other vital organs to liquid N2O. |
| Bleeding from the stomach | Figure 2O | Cryoablation of the stomach | It is normal to observe some minimal bleeding after cryoablation. |
| Bleeding from the stomach | Figure 2G | Damage of the stomach vasculature | Make sure to open the stomach at the greater curvature, where there is less vasculature. Apply pressure using a cotton swab for approximately 1 min on the bleeding spot or blood vessel. |
| Bleeding from the stomach | Figure 2I–O | Forced grabbing of the stomach wall during ablation | Use appropriate forceps to hold the stomach wall during cryoablation. Holding too tight will damage the stomach wall. |
| Leakage from the stomach incision | Figure 2P | The stomach is not sutured properly | Additional stitches are required. |
| Not drinking liquid food | Postoperative care (day 0–2) | It is not unusual that some animals dislike liquid food | Provide small amounts of solid food after day 2 or soften the pellet food with water. |
| Not eating solid food and low mobility | Postoperative care | High discomfort | Extreme weight loss can be an indication of infection due to perforation of the stomach and exposure of stomach content to the abdominal cavity. Endpoint rule applies and the animal should be euthanized. |
| Dehydration | Postoperative care | Not drinking water due to discomfort | s.c. injection of saline solution. |
| Opening of the skin wound | Postoperative care | Animals can reach and eat the stitches | Additional stitches or other means are required to close the skin incision/wound. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia, A.C.P.; Straub, D.; Calpe, S.; Krishnadath, K.K. Novel In Vivo Mouse Cryoablation Model to Explore Unique Therapeutic Approaches for Premalignant Columnar Lesions. Methods Protoc. 2021, 4, 6. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010006
Correia ACP, Straub D, Calpe S, Krishnadath KK. Novel In Vivo Mouse Cryoablation Model to Explore Unique Therapeutic Approaches for Premalignant Columnar Lesions. Methods and Protocols. 2021; 4(1):6. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010006
Chicago/Turabian StyleCorreia, Ana C. P., Danielle Straub, Silvia Calpe, and Kausilia K. Krishnadath. 2021. "Novel In Vivo Mouse Cryoablation Model to Explore Unique Therapeutic Approaches for Premalignant Columnar Lesions" Methods and Protocols 4, no. 1: 6. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4010006