
POIS-10 Māori: Outcomes and Experiences in the Decade Following Injury

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. The Burden of Injury for Māori in New Zealand
1.2. The Need for POIS-10 Māori: Evidence from our Existing Mixed-Methods Research
1.2.1. Whānau Flourishing as a Protective Factor to Injury
1.2.2. A Kaupapa Māori Approach to Understanding Outcomes of Injury
1.3. POIS-10 Māori Aims and Objectives
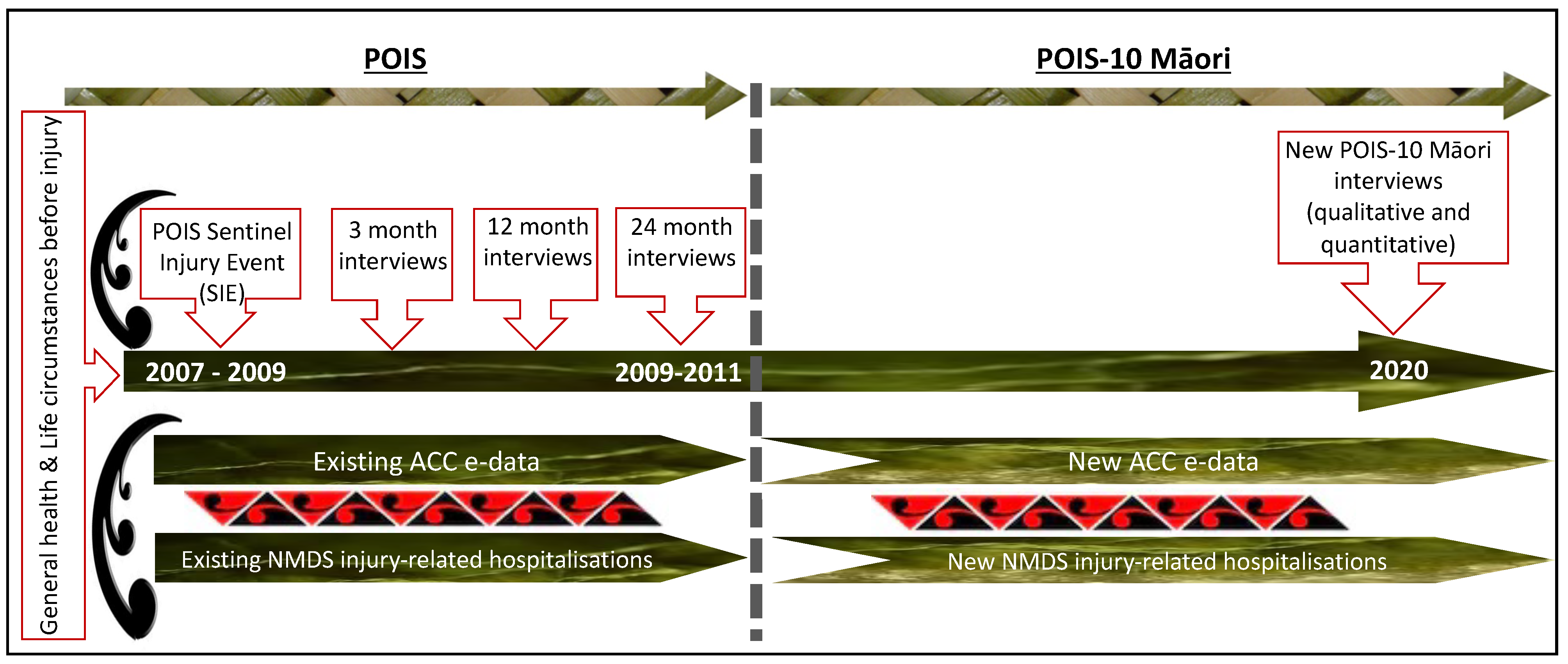
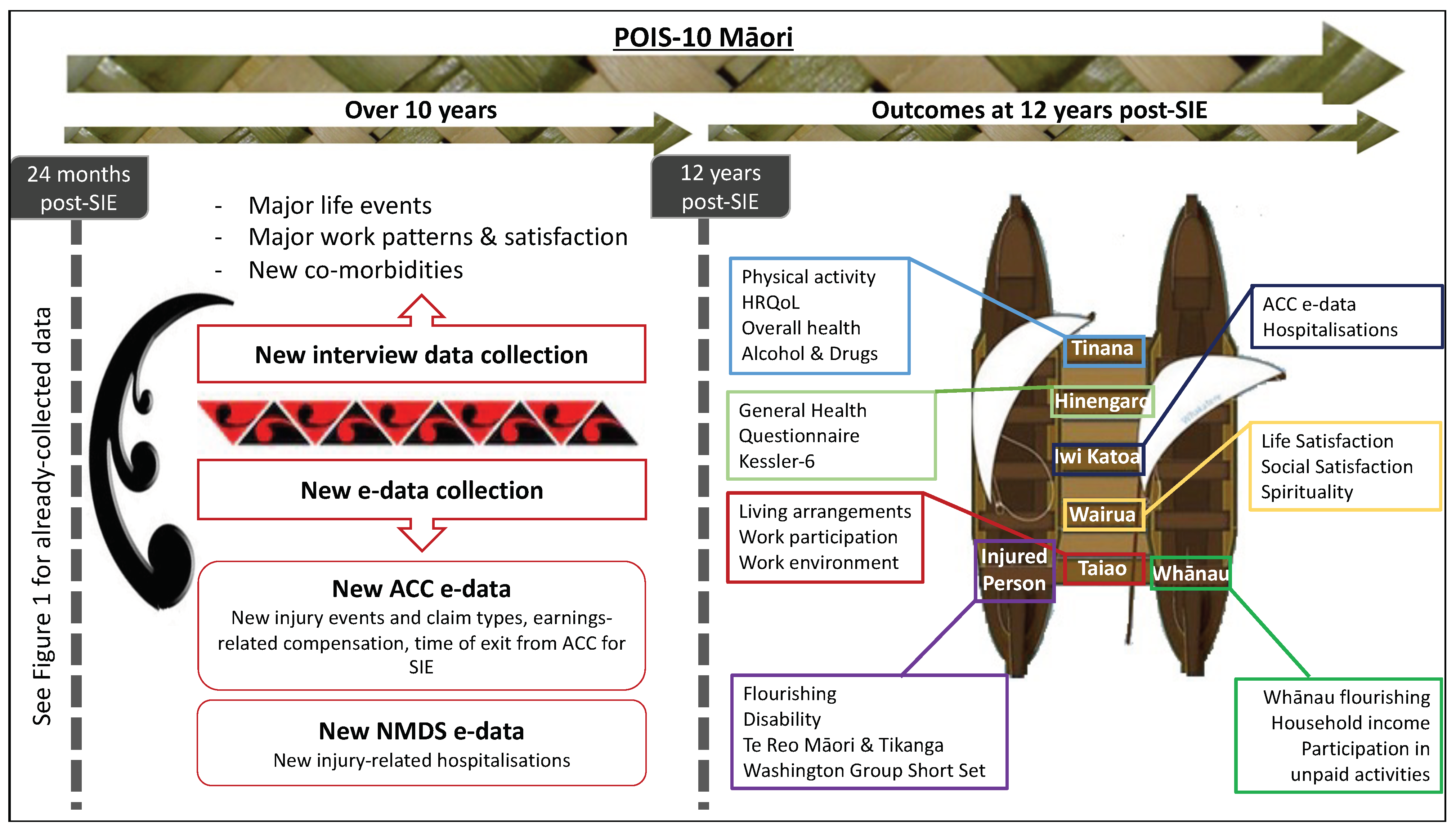
- Quantitatively describe significant life events, employment variations, comorbidities, new injury events and injury-related health service utilisation over the past 10 years (i.e., since the last interview at 24 months post-SIE);
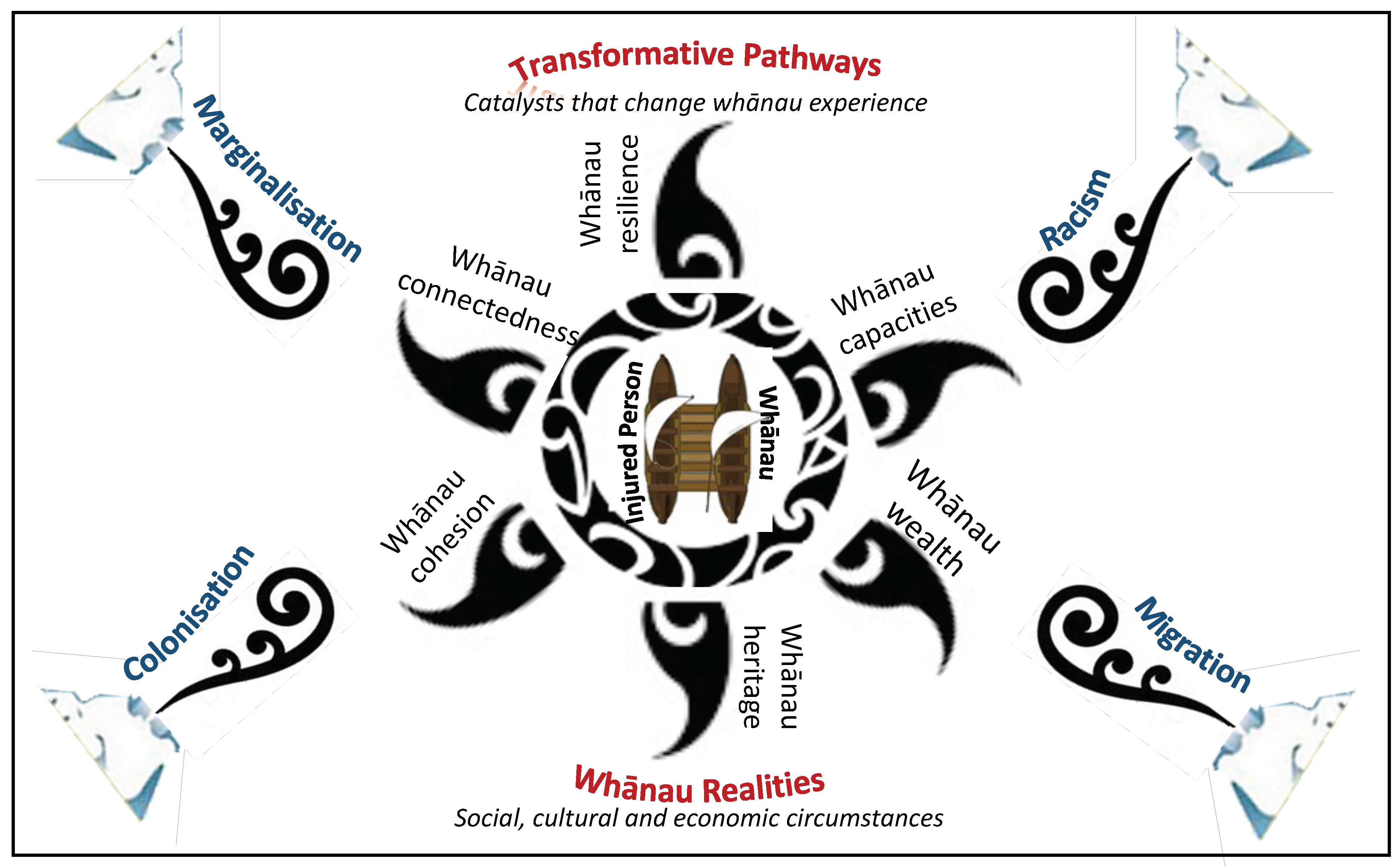
- Quantitatively investigate 12-year post-SIE outcomes, as informed by the Meihana Model [38];
- Quantitatively determine which characteristics (including baseline socio-demographic and health-related, SIE-related and post-SIE-related) predict outcomes at 12 years post-SIE;
- Qualitatively explore long-term experiences of, and barriers and facilitators of access to, health and rehabilitation services, ACC and whānau flourishing, for injured Māori and their whānau;
- Work with key advisors and organisations to meaningfully interpret findings and identify appropriate opportunities for future interventions to improve experiences and outcomes for injured Māori and their whānau.
2. Experimental Design
3. Procedure
3.1. Participants
3.2. Quantitative Data
3.2.1. POIS-10 Interviews at 12-Year Follow up
3.2.2. E-Data between 24-Months and 12-Year Follow up
3.3. Qualitative Data
3.4. Ethical Approval
4. Expected Results
Analyses
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics New Zealand. He Hauā Māori Findings from the 2013 Disability Survey; Statistics New Zealand: Wellington, New Zealand, 2015. [Google Scholar]
- Wilson, R.; Derrett, S.; Hansen, P.; Langley, J.D. Costs of injury in New Zealand: Accident Compensation Corporation spending, personal spending and quality-adjusted life years lost. Inj. Prev. 2012, 19, 124–129. [Google Scholar] [CrossRef]
- Ministry of Health and Accident Compensation Corporation. Injury-Related Health Loss: A Report from the New Zealand Burden of Diseases, Injuries and Risk Factors Study 2006–2016; Ministry of Health: Wellington, New Zealand, 2013. [Google Scholar]
- Ministry of Health. Tatau Kahukura: Māori Health Chart Book 2015, 3rd ed.; Ministry of Health: Wellington, New Zealand, 2015. [Google Scholar]
- Ratima, K.; Ratima, M. Māori Experience of Disability and Disability Support Services. In Hauora: Māori Standards of Health IV. A study of the Years 2000–2005; Robson, B., Harris, R., Eds.; Te Rōpū Rangahau Hauora a Eru Pōmare: Wellington, New Zealand, 2007; pp. 189–208. [Google Scholar]
- Wren, J. Barriers to Māori Utilisation of ACC Funded Services, and Evidence for Effective Interventions: Māori Responsiveness Report 2; ACC Research: Wellington, New Zealand, 2015. [Google Scholar]
- Wren, J. Evidence for Māori under-Utilisation of ACC Injury Treatment and Rehabilitation Support Services: Māori Responsiveness Report 1; ACC Research: Wellington, New Zealand, 2015. [Google Scholar]
- Abdalla, S.; Kelleher, C.C.; Quirke, B.; Daly, L.; l-Ireland Traveller Health Study Team. Disparities in fatal and non-fatal injuries between Irish travellers and the Irish general population are similar to those of other indigenous minorities: A cross-sectional population-based comparative study. BMJ Open 2013, 3, e002296. [Google Scholar] [CrossRef] [Green Version]
- Karmali, S.; Laupland, K.; Harrop, A.R.; Findlay, C.; Kirkpatrick, A.W.; Winston, B.; Kortbeek, J.; Crowshoe, L.; Hameed, M. Epidemiology of severe trauma among status Aboriginal Canadians: A population-based study. Can. Med. Assoc. J. 2005, 172, 1007–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassler, S.; Johansson, R.; Sjölander, P.; Grönberg, H.; Damber, L. Causes of death in the Sami population of Sweden, 1961–2000. Int. J. Epidemiol. 2005, 34, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Soininen, L.; Pukkala, E. Mortality of the Sami in northern Finland 1979–2005. Int. J. Circumpolar Health 2008, 67, 45–57. [Google Scholar] [CrossRef]
- Kohler, I.V.; Preston, S.H. Ethnic and religious differentials in Bulgarian mortality, 1993–1998. Popul. Stud. 2011, 65, 91–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, T.; Barker, B.; Begg, S.; Stanley, L.; Lopez, A.D. Burden of disease and injury in Aboriginal and Torres Strait Islander Peoples: The Indigenous health gap. Int. J. Epidemiol. 2008, 38, 470–477. [Google Scholar] [CrossRef] [Green Version]
- Ajwani, S.; Blakely, T.; Robson, B.; Tobias, M.; Bonne, M. Decades of Disparity: Ethnic Mortality Trends in New Zealand 1980–1999; Ministry of Health: Wellington, New Zealand, 2003. [Google Scholar]
- Reid, P.; Robson, B. Understanding Health Inequities. In Hauora: Maori Standards of Health IV. A Study of the Years 2000–2005; Robson, B., Harris, R., Eds.; Te Rōpū Rangahau Hauora a Eru Pōmare: Wellington, New Zealand, 2007; pp. 3–10. [Google Scholar]
- Office for Disability Issues, Statistics New Zealand. Disability and Māori in New Zealand in 2006: Results from the New Zealand Disability Survey; Statistics New Zealand: Wellington, New Zealand, 2010. [Google Scholar]
- Reid, J.; Cormack, D.; Crowe, M. The significance of socially-assigned ethnicity for self-identified Māori accessing and engaging with primary healthcare in New Zealand. Health 2016, 20, 143–160. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.; Kydd, R.; Shield, K.; Rehm, J. The burden of disease and injury attributable to alcohol in New Zealanders under 80 years of age: Marked disparities by ethnicity and sex. N. Z. Med. J. 2015, 128, 3. [Google Scholar]
- Accident Compensation Corporation. Annual Report 2009; Accident Compensation Corporation: Wellington, New Zealand, 2009. [Google Scholar]
- Derrett, S.; Langley, J.; Hokowhitu, B.; Ameratunga, S.; Hansen, P.; Davie, G.; Wyeth, E.; Lilley, R. Prospective Outcomes of Injury Study. Inj. Prev. 2009, 15, e3. [Google Scholar] [CrossRef]
- Derrett, S.; Davie, G.; Ameratunga, S.; Wyeth, E.; Colhoun, S.; Wilson, S.; Samaranayaka, A.; Lilley, R.; Hokowhitu, B.; Hansen, P.; et al. Prospective Outcomes of Injury Study: Recruitment, and participant characteristics, health and disability status. Inj. Prev. 2011, 17, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Maclennan, B.; Wyeth, E.; Hokowhitu, B.; Wilson, S.; Derrett, S. Injury Severity and 3-Month Outcomes Among Māori: Results from a New Zealand Prospective Cohort Study. N. Z. J. Med. 2013, 126, 39–49. [Google Scholar]
- Wyeth, E.H.; MacLennan, B.; Lambert, M.; Davie, G.; Lilley, R.; Derrett, S. Predictors of work participation for Māori 3 months after injury. Arch. Environ. Occup. Health 2017, 73, 79–89. [Google Scholar] [CrossRef]
- Wyeth, E.; Samaranayaka, A.; Lambert, M.; Tapsell, M.; Anselm, D.; Ellison, P.; Harwood, M.; Metzger, B.; Wright-Tawha, T.; Derrett, S. Understanding longer-term disability outcomes for Māori and non-Māori after hospitalisation for injury: Results from a longitudinal cohort study. Public Health 2019, 176, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Derrett, S.; Wilson, S.; Samaranayaka, A.; Langley, J.; Wyeth, E.; Ameratunga, S.; Lilley, R.; Davie, G.; Mauiliu, M. Prevalence and Predictors of Disability 24-Months After Injury for Hospitalised and Non-Hospitalised Groups: Results from a Longitudinal Cohort Study in New Zealand. PLoS ONE 2013, 8, e80194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyeth, E.; Samaranayaka, A.; Davie, G.; Derrett, S. Prevalence and predictors of disability for Māori 24 months after injury. Aust. N. Z. J. Public Health 2017, 41, 262–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLennan, B.; Wyeth, E.; Davie, G.; Wilson, S.; Derrett, S. Twelve-month post-injury outcomes for Māori and non-Māori: Findings from a New Zealand cohort study. Aust. N. Z. J. Public Health 2014, 38, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Wyeth, E.H.; Derrett, S.; Hokowhitu, B.; Samaranayaka, A. Indigenous injury outcomes: Life satisfaction among injured Maori in New Zealand three months after injury. Health Qual. Life Outcomes 2013, 11, 120. [Google Scholar] [CrossRef] [Green Version]
- Verhaeghe, S.; Defloor, T.; Grypdonck, M. Stress and coping among families of patients with traumatic brain injury: A review of the literature. J. Clin. Nurs. 2005, 14, 1004–1012. [Google Scholar] [CrossRef]
- Dew, K.; Signal, L.; Davies, C.; Tavite, H.; Hooper, C.; Sarfati, D.; Stairmand, J.; Cunningham, C. Dissonant roles: The experience of Māori in cancer care. Soc. Sci. Med. 2015, 138, 144–151. [Google Scholar] [CrossRef]
- Auckland District Health Board. Auckland District Health Board Outpatient Experience Report 10; Auckland District Health Board: Auckland, New Zealand, 2016. [Google Scholar]
- Lambert, M.; Wyeth, E.H.; Brausch, S.; Harwood, M.L.; Anselm, D.; Wright-Tawha, T.; Metzger, B.; Ellison, P.; Derrett, S. “I couldn’t even do normal chores”: A qualitative study of the impacts of injury for Māori. J. Disabil. Rehabil. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kingi, T.; Durie, M.; Cunningham, C.; Borman, B.; Ellison-Loschmann, L. Te Puawaitanga o Ngā Whānau: Six Markers of Flourishing Whānau; Māori and Pasifika Massey University: Wellington, New Zealand, 2014. [Google Scholar]
- Durie, M. Ngā Tini Whetū: Navigating Māori futures; Huia Publishers: Wellington, New Zealand, 2011. [Google Scholar]
- Cram, F. Rangahau Māori: Tona tika, tona pono—The Validity and Integrity of Māori Research. In Research Ethics in Aotearoa New Zealand; Tolich, M., Ed.; Pearson Education New Zealand Limited: Auckland, New Zealand, 2001; pp. 35–52. [Google Scholar]
- Te Mana Raraunga. Principles of Māori Data Sovereignty. Available online: https://static1.squarespace.com/static/58e9b10f9de4bb8d1fb5ebbc/t/5bda208b4ae237cd89ee16e9/1541021836126/TMR+Ma%CC%84ori+Data+Sovereignty+Principles+Oct+2018.pdf (accessed on 1 November 2018).
- Wyeth, E.H.; Derrett, S.; Hokowhitu, B.; Hall, C.; Langley, J. Rangatiratanga and Ōritetanga: Responses to the Treaty of Waitangi in a New Zealand study. Ethn. Health 2010, 15, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Pitama, S.; Huria, T.; Lacey, C. Improving Māori health through clinical assessment: Waikare o te Waka o Meihana. N. Z. Med. J. 2014, 127, 107–119. [Google Scholar]
- Research Electronic Data Capture. Project: REDCap. Available online: https://www.project-redcap.org/ (accessed on 1 November 2018).
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.W.; Oishi, S.; Biswas-Diener, R. New Well-being Measures: Short Scales to Assess Flourishing and Positive and Negative Feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Üstün, T.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0); WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- Fugl-Meyer, A.R.; Bränholm, I.B.; Fugl-Meyer, K.S. Happiness and Domain-specific Life Satisfcation in Adult Northern Swedes. Clin. Rehabil. 1991, 5, 25–33. [Google Scholar] [CrossRef]
- Statistics New Zealand. New Zealand Census of Population and Dwellings—Individual Form; Statistics New Zealand: Wellington, New Zealand, 2006. [Google Scholar]
- Wilson, S.J.; Davie, G.; Harcombe, H.; Wyeth, E.H.; Cameron, I.D.; Derrett, S. Impact of further injury on participation in work and activities among those previously injured: Results from a New Zealand prospective cohort study. Qual. Life Res. 2018, 27, 3167–3178. [Google Scholar] [CrossRef]
- Harcombe, H.; Langley, J.; Davie, G.; Derrett, S. Functional status following injury: What recovery pathways do people follow? J. Inj. 2015, 46, 1275–1280. [Google Scholar] [CrossRef]
- Langley, J.; Derrett, S.; Davie, G.; Ameratunga, S.; Wyeth, E. A cohort study of short-term functional outcomes following injury: The role of pre-injury socio-demographic and health characteristics, injury and injury-related healthcare. Heal. Qual. Life Outcomes 2011, 9, 68–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT Alcohol Consumption Questions (AUDIT-C) An Effective Brief Screening Test for Problem Drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [Green Version]
- Sports and Recreation New Zealand. The New Zealand Physical Activity Questionnaires; Sports and Recreation New Zealand: Wellington, New Zealand, 2004. [Google Scholar]
- Goldberg, D. General Health Questionnaire (GHQ-12); NFER-Nelson: Windsor, UK, 1992. [Google Scholar]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for Serious Mental Illness in the General Population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- FACIT.org. FACIT. Available online: http://www.facit.org/facitorg/questionnaires (accessed on 1 November 2018).
- Lilley, R.; Davie, G.; Langley, J.; Ameratunga, S.; Derrett, S. Do outcomes differ between work and non-work-related injury in a universal injury compensation system? Findings from the New Zealand Prospective Outcomes of Injury Study. BMC Public Health 2013, 13, 995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lilley, R.; Davie, G.; Derrett, S. Are the early predictors of long-term work absence following injury time dependent? Results from the Prospective Outcomes of Injury Study. BMJ Open 2017, 7, e017390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health. Content Guide 2016/17: New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2017. [Google Scholar]
- Holmes, T.H.R.R. The social readjustment rating scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Durie, M. Tirohanga Māori—Maori Health Perspectives. In Whaiora—Māori Health Development, 2nd ed.; Durie, M., Ed.; Oxford University Press: Melbourne, Australia, 1994; pp. 66–80. [Google Scholar]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Davie, G.; Samaranayaka, A.; Derrett, S. The role of pre-existing comorbidity on the rate of recovery following injury: A longitudinal cohort study. PLoS ONE 2018, 13, e0193019. [Google Scholar] [CrossRef]
- Smith, J.A.; Flowers, P.; Larkin, M. Interpretive Phenomenological Analysis: Theory, Method and Research; Sage Publications: London, UK, 2009. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.; Ingham, T.R.; Cram, F.; Dean, S.; Davies, C. An indigenous approach to explore health-related experiences among Māori parents: The Pukapuka Hauora asthma study. BMC Public Health 2013, 13, 228. [Google Scholar] [CrossRef] [Green Version]
- Jones, B.; Ingham, T.; Davies, C.; Cram, F. Whānau Tuatahi: Māori community partnership research using a Kaupapa Māori methodology. MAI Rev. 2010, 3, 1–14. [Google Scholar]
- Mark, G.T.; Lyons, A.C. Maori healers’ views on wellbeing: The importance of mind, body, spirit, family and land. Soc. Sci. Med. 2010, 70, 1756–1764. [Google Scholar] [CrossRef]
- Bevington, G.; Wolcott, H.F. Transforming Qualitative Data: Description, Analysis, and Interpretation. Mod. Lang. J. 1996, 80, 405. [Google Scholar] [CrossRef]
- Bergin, M. NVivo 8 and consistency in data analysis: Reflecting on the use of a qualitative data analysis program. Nurse Res. 2011, 18, 6–12. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wyeth, E.H.; Derrett, S.; Nelson, V.; Bourke, J.; Crengle, S.; Davie, G.; Harcombe, H. POIS-10 Māori: Outcomes and Experiences in the Decade Following Injury. Methods Protoc. 2021, 4, 37. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020037
Wyeth EH, Derrett S, Nelson V, Bourke J, Crengle S, Davie G, Harcombe H. POIS-10 Māori: Outcomes and Experiences in the Decade Following Injury. Methods and Protocols. 2021; 4(2):37. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020037
Chicago/Turabian StyleWyeth, Emma H., Sarah Derrett, Vicky Nelson, John Bourke, Sue Crengle, Gabrielle Davie, and Helen Harcombe. 2021. "POIS-10 Māori: Outcomes and Experiences in the Decade Following Injury" Methods and Protocols 4, no. 2: 37. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4020037