
Perilla Oil and Bifidobacterium for Alleviating Fear of Cancer Recurrence in Breast Cancer Survivors: Study Protocol for a Three-Arm Phase II Randomized Controlled Study (POB Study)

 , , and
, , and
Abstract
:1. Introduction
2. Methods and Analysis
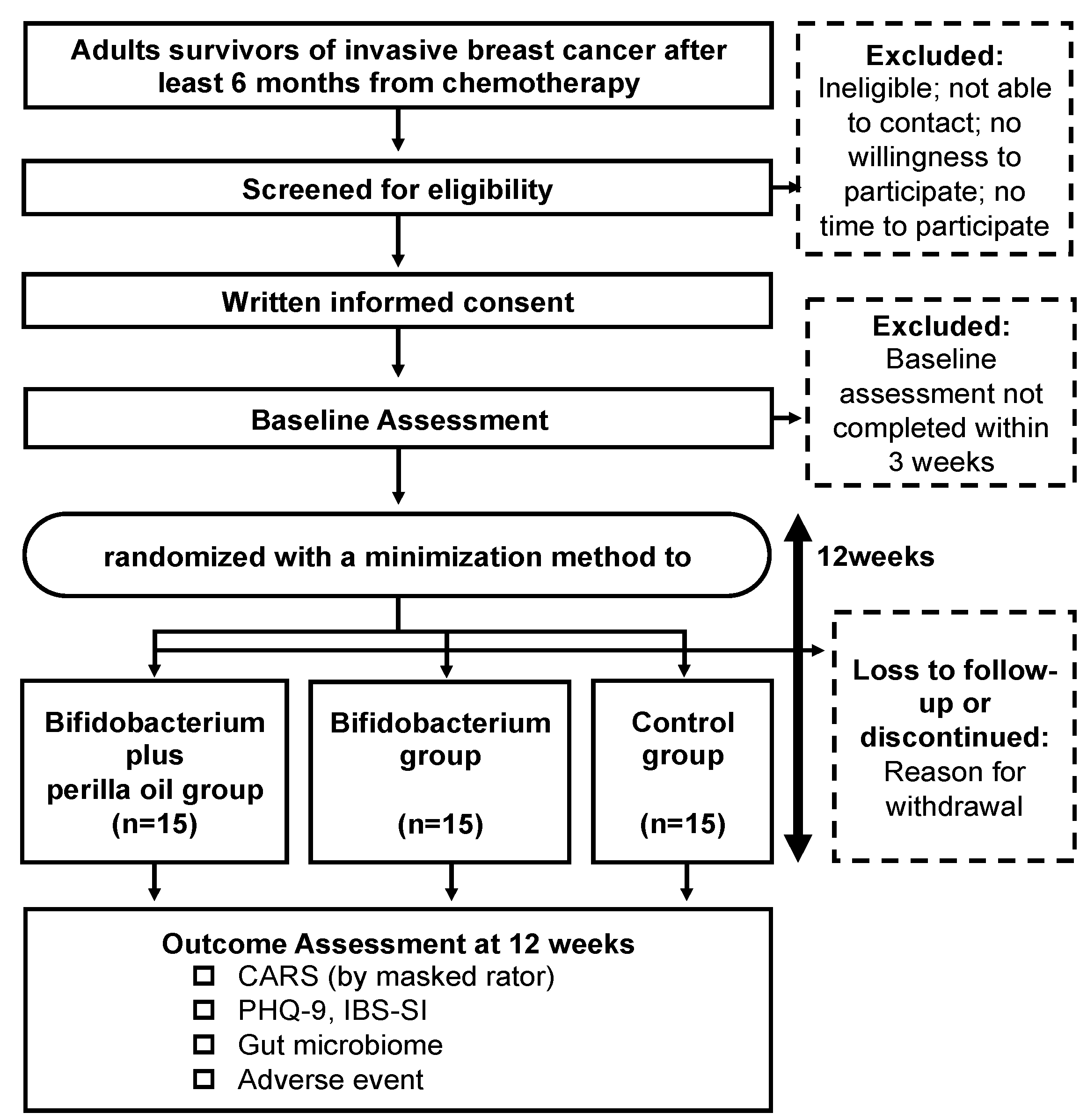
2.1. Study Design
2.2. Inclusion Criteria
- Aged 20 years or older at the time of providing informed consent;
- Outpatient at the National Center of Neurology and Psychiatry hospital or the National Hospital Organization Tokyo Medical Center;
- Histologically or cytologically confirmed invasive breast cancer without cancer recurrence. The criteria is limited to invasive breast cancers because they are more likely to recur than non-invasive breast cancers and tend to be associated with a higher level of (more severe) FCR;
- Chemotherapy completed at least 6 months before registration. Hormone therapy may be ongoing. Patients who have only just completed chemotherapy will not be included because their diets tend to change due to stomatitis, and their gut environment can be unstable due to acute intestinal inflammation from the chemotherapy;
- Recognition of cancer diagnosis. This criterion is set because a small number of people do not recognize themselves as having cancer, but the patients in the present study must recognize themselves as cancer survivors.
2.3. Exclusion Criteria
- Severe cognitive impairment due to delirium, dementia, or other problems. Patients with severe cognitive impairment are excluded since they might be unable to properly consume the test food or respond to questions independently;
- No Japanese literacy;
- Ongoing non-hormonal anticancer therapy for breast or other cancers;
- Need for immediate psychiatric intervention for suicidal ideation or other severe psychiatric symptoms at study entry;
- No antianxiety or antidepressant medication added or discontinued in the preceding month;
- Daily habit of consuming any ALA-containing food (e.g., perilla or linseed oil). That is, we will exclude patients who are intentionally consuming ALA-containing food daily;
- Daily habit of consuming Bifidobacterium-containing food. These patients are excluded to prevent over- or underestimation of the effect of the intervention. That is, we will exclude patients who are intentionally consuming Bifidobacterium-containing food daily;
- Deemed by the attending physician to be unfit for inclusion in the study for any other reasons. For this criterion, it is necessary to consider the possibility of extreme bias in the patients to be excluded due to the personal opinion of individual physicians. Therefore, the reason for exclusion should be documented whenever this criterion is met.
2.4. Participant Timeline and Recruitment
2.5. Randomization and Masking
2.6. Intervention Groups
2.7. Criteria for Discontinuing Allocated Interventions
2.8. Control Group
2.9. Data Collection Methods
2.10. Primary Outcome Measures
2.11. Secondary Outcome Measures
2.12. Harm
2.13. Sample Size Calculation
2.14. Statistical Methods
2.15. Data Management and Monitoring and Auditing
3. Ethics and Dissemination
3.1. Ethical Considerations
3.2. Declaration of Interests and Access to Data
3.3. Availability of Data and Materials
3.4. Patient and Public Involvement
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ARs | adverse reactions |
| ALA | alpha-linolenic acid |
| CRC | clinical research coordinator |
| CRF | case report form |
| CARS | Concerns about Recurrence Scale |
| EDC | electronic data capture system |
| FCR | fear of cancer recurrence |
| FFQ | Food Frequency Questionnaire |
| IAP | intestinal alkaline phosphatase |
| ITT | intention-to-treat |
| ICMJE | International Committee of Medical Journal Editors |
| IBS | irritable bowel syndrome |
| IBS-SI | Irritable bowel syndrome severity index |
| JRCT | Japan Registry of Clinical Trials |
| NCNP | National Center for Neurology and Psychiatry Hospital |
| NHO | National Hospital Organization |
| PHQ-9 | Patient Health Questionnaire-9 |
| PPS | per protocol set |
| PRO | patient-reported outcomes |
| PUFA | polyunsaturated fatty acid |
References
- Okubo, R.; Chen, C.; Sekiguchi, M.; Hamazaki, K.; Matsuoka, Y.J. Mechanisms underlying the effects of n-3 polyunsaturated fatty acids on fear memory processing and their hypothetical effects on fear of cancer recurrence in cancer survivors. Prostaglandins Leukot. Essent. Fat. Acids 2018, 131, 14–23. [Google Scholar] [CrossRef]
- Armes, J.; Crowe, M.; Colbourne, L.; Morgan, H.; Murrells, T.; Oakley, C.; Palmer, N.; Ream, E.; Young, A.; Richardson, A. Patients’ supportive care needs beyond the end of cancer treatment: A prospective, longitudinal survey. J. Clin. Oncol. 2009, 27, 6172–6179. [Google Scholar] [CrossRef]
- Akechi, T.; Okuyama, T.; Endo, C.; Sagawa, R.; Uchida, M.; Nakaguchi, T.; Akazawa, T.; Yamashita, H.; Toyama, T.; Furukawa, T.A. Patient’s perceived need and psychological distress and/or quality of life in ambulatory breast cancer patients in Japan. Psycho-Oncology 2011, 20, 497–505. [Google Scholar] [CrossRef]
- Simonelli, L.E.; Siegel, S.D.; Duffy, N.M. Fear of cancer recurrence: A theoretical review and its relevance for clinical presentation and management. Psycho-Oncology 2016, 26, 1444–1454. [Google Scholar] [CrossRef] [PubMed]
- Fardell, J.E.; Thewes, B.; Turner, J.; Gilchrist, J.; Sharpe, L.; Smith, A.; Girgis, A.; Butow, P. Fear of cancer recurrence: A theoretical review and novel cognitive processing formulation. J. Cancer Surviv. 2016, 10, 663–673. [Google Scholar] [CrossRef]
- Butow, P.N.; Bell, M.L.; Smith, A.B.; Fardell, J.E.; Thewes, B.; Turner, J.; Gilchrist, J.; Beith, J.; Girgis, A.; Sharpe, L. Conquer fear: Protocol of a randomised controlled trial of a psychological intervention to reduce fear of cancer recurrence. BMC Cancer 2013, 13, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McHale, C.T.; Cruickshank, S.; Torrens, C.; Armes, J.; Fenlon, D.; Banks, E.; Kelsey, T.; Humphris, G.M. A controlled pilot trial of a nurse-led intervention (Mini-AFTERc) to manage fear of cancer recurrence in patients affected by breast cancer. Pilot Feasibility Stud. 2020, 6, 1–10. [Google Scholar] [CrossRef]
- Van Beusekom, M.; Cameron, J.; Bedi, C.; Banks, E.; Kelsey, T.; Humphris, G. Development, acceptability and feasibility of a communication skills training package for therapeutic radiographers to reduce fear of recurrence development in breast cancer patients (FORECAST2). Pilot Feasibility Stud. 2018, 4, 148. [Google Scholar] [CrossRef]
- Simard, S.; Thewes, B.; Humphris, G.; Dixon, M.; Hayden, C.; Mireskandari, S.; Ozakinci, G. Fear of cancer recurrence in adult cancer survivors: A systematic review of quantitative studies. J. Cancer Surviv. 2013, 7, 300–322. [Google Scholar] [CrossRef]
- White, R.G.; Gumley, A.I. Postpsychotic posttraumatic stress disorder: Associations with fear of recurrence and intolerance of uncertainty. J. Nerv. Ment. Dis. 2009, 197, 841–849. [Google Scholar] [CrossRef]
- LeDoux, J.E. Emotion circuits in the brain. Annu. Rev. Neurosci. 2000, 23, 155–184. [Google Scholar] [CrossRef]
- Rauch, S.L.; Shin, L.M.; Phelps, E.A. Neurocircuitry models of posttraumatic stress disorder and extinction: Human neuroimaging research—Past, present, and future. Biol. Psychiatry 2006, 60, 376–382. [Google Scholar] [CrossRef]
- McNamara, R.K.; Carlson, S.E. Role of omega-3 fatty acids in brain development and function: Potential implications for the pathogenesis and prevention of psychopathology. Prostaglandins Leukot. Essent. Fat. Acids 2006, 75, 329–349. [Google Scholar] [CrossRef]
- Mathieu, G.; Oualian, C.; Denis, I.; Lavialle, M.; Gisquet-Verrier, P.; Vancassel, S. Dietary n-3 polyunsaturated fatty acid deprivation together with early maternal separation increases anxiety and vulnerability to stress in adult rats. Prostaglandins Leukot. Essent. Fat. Acids 2011, 85, 129–136. [Google Scholar] [CrossRef]
- Noguchi, H.; Okubo, R.; Hamazaki, K.; Yamashita, A.; Narisawa, T.; Matsuoka, Y.J. Serum polyunsaturated fatty acids and risk of psychiatric disorder at 6 months after acute coronary syndrome: A prospective cohort study. Prostaglandins Leukot. Essent. Fat. Acids 2019, 149, 18–23. [Google Scholar] [CrossRef]
- Arentsen, T.; Raith, H.; Qian, Y.; Forssberg, H.; Diaz Heijtz, R. Host microbiota modulates development of social preference in mice. Microb. Ecol. Health Dis. 2015, 26, 29719. [Google Scholar] [CrossRef] [PubMed]
- Hoban, A.E.; Stilling, R.M.; Moloney, G.; Shanahan, F.; Dinan, T.G.; Clarke, G.; Cryan, J.F. The microbiome regulates amygdala-dependent fear recall. Mol. Psychiatry 2017, 23, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Noguchi, H.; Hamazaki, K.; Sekiguchi, M.; Kinoshita, T.; Katsumata, N.; Narisawa, T.; Uezono, Y.; Xiao, J.; Matsuoka, Y.J. Fear of cancer recurrence among breast cancer survivors could be controlled by prudent dietary modification with polyunsaturated fatty acids. J. Affect. Disord. 2019, 245, 1114–1118. [Google Scholar] [CrossRef]
- Okubo, R.; Kinoshita, T.; Katsumata, N.; Uezono, Y.; Xiao, J.; Matsuoka, Y.J. Impact of chemotherapy on the association between fear of cancer recurrence and the gut microbiota in breast cancer survivors. Brain Behav. Immun. 2019, 85, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Romijn, A.R.; Rucklidge, J.J. Systematic review of evidence to support the theory of psychobiotics. Nutr. Rev. 2015, 73, 675–693. [Google Scholar] [CrossRef] [Green Version]
- Pirbaglou, M.; Katz, J.; de Souza, R.J.; Stearns, J.C.; Motamed, M.; Ritvo, P. Probiotic supplementation can positively affect anxiety and depressive symptoms: A systematic review of randomized controlled trials. Nutr. Res. 2016, 36, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Lee, I.S.; Braun, C.; Enck, P. Effect of Probiotics on Central Nervous System Functions in Animals and Humans: A Systematic Review. J. Neurogastroenterol. Motil. 2016, 22, 589–605. [Google Scholar] [CrossRef]
- Nishimura, M.; Ohkawara, T.; Tetsuka, K.; Kawasaki, Y.; Nakagawa, R.; Satoh, H.; Sato, Y.; Nishihira, J. Effects of yogurt containing Lactobacillus plantarum HOKKAIDO on immune function and stress markers. J. Tradit. Complement. Med. 2016, 6, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Yadav, V.; Chatterjee, S.S.; Majeed, M.; Kumar, V. Preventive potentials of piperlongumine and a Piper longum extract against stress responses and pain. J. Tradit. Complement. Med. 2016, 6, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Koga, M.; Katsumata, N.; Odamaki, T.; Matsuyama, S.; Oka, M.; Narita, H.; Hashimoto, N.; Kusumi, I.; Xiao, J.; et al. Effect of Bifidobacterium breve A-1 on anxiety and depressive symptoms in schizophrenia: A proof-of-concept study. J. Affect. Disord. 2019, 245, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Patterson, E.; O’Dohery, R.M.; Murphy, E.F.; Wall, R.; O’Sullivan, O.; Nilaweera, K.; Fitzgerald, G.F.; Cotter, P.D.; Ross, R.P.; Stanton, C. Impact of dietary fatty acids on metabolic activity and host intestinal microbiota composition in C57BL/6J mice. Br. J. Nutr. 2014, 111, 1905–1917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, T.M.; Wall, R.; O’Sullivan, O.; Fitzgerald, G.F.; Shanahan, F.; Quigley, E.M.; Cotter, P.D.; Cryan, J.F.; Dinan, T.G.; Ross, R.P.; et al. Dietary trans-10, cis-12-conjugated linoleic acid alters fatty acid metabolism and microbiota composition in mice. Br. J. Nutr. 2015, 113, 728–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.N.; Zhu, J.; Pan, W.S.; Shen, S.R.; Shan, W.G.; Das, U.N. Effects of fish oil with a high content of n-3 polyunsaturated fatty acids on mouse gut microbiota. Arch. Med. Res. 2014, 45, 195–202. [Google Scholar] [CrossRef]
- Horigome, A.; Okubo, R.; Hamazaki, K.; Kinoshita, T.; Katsumata, N.; Uezono, Y.; Xiao, J.Z.; Matsuoka, Y.J. Association between blood omega-3 polyunsaturated fatty acids and the gut microbiota among breast cancer survivors. Benef. Microbes 2019, 10, 751–758. [Google Scholar] [CrossRef]
- Kuda, T.; Enomoto, T.; Yano, T.; Fujii, T. Cecal environment and TBARS level in mice fed corn oil, beef tallow and menhaden fish oil. J. Nutr. Sci. Vitaminol. 2000, 46, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Kaliannan, K.; Wang, B.; Li, X.Y.; Kim, K.J.; Kang, J.X. A host-microbiome interaction mediates the opposing effects of omega-6 and omega-3 fatty acids on metabolic endotoxemia. Sci. Rep. 2015, 5, 11276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lichtenthal, W.G.; Corner, G.W.; Slivjak, E.T.; Roberts, K.E.; Li, Y.; Breitbart, W.; Lacey, S.; Tuman, M.; DuHamel, K.N.; Blinder, V.S.; et al. A pilot randomized controlled trial of cognitive bias modification to reduce fear of breast cancer recurrence. Cancer 2017, 123, 1424–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vickberg, S.M. The Concerns About Recurrence Scale (CARS): A systematic measure of women’s fears about the possibility of breast cancer recurrence. Ann. Behav. Med. 2003, 25, 16–24. [Google Scholar] [CrossRef]
- Kato, T.; Furukawa, T.A.; Mantani, A.; Kurata, K.; Kubouchi, H.; Hirota, S.; Sato, H.; Sugishita, K.; Chino, B.; Itoh, K.; et al. Optimising first- and second-line treatment strategies for untreated major depressive disorder—The SUND study: A pragmatic, multi-centre, assessor-blinded randomised controlled trial. BMC Med. 2018, 16, 103. [Google Scholar] [CrossRef]
- Watanabe, N.; Furukawa, T.A.; Horikoshi, M.; Katsuki, F.; Narisawa, T.; Kumachi, M.; Oe, Y.; Shinmei, I.; Noguchi, H.; Hamazaki, K.; et al. A mindfulness-based stress management program and treatment with omega-3 fatty acids to maintain a healthy mental state in hospital nurses (Happy Nurse Project): Study protocol for a randomized controlled trial. Trials 2015, 16, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, N.; Hashimoto, A.; Takemoto, Y.; Okuyama, H.; Nomura, M.; Kitajima, R.; Togashi, T.; Tamai, Y. Effect of the dietary alpha-linolenate/linoleate balance on lipid compositions and learning ability of rats. II. Discrimination process, extinction process, and glycolipid compositions. J. Lipid Res. 1988, 29, 1013–1021. [Google Scholar] [CrossRef]
- Miller, H.C.; Struyf, D.; Baptist, P.; Dalile, B.; Van Oudenhove, L.; Van Diest, I. A mind cleared by walnut oil: The effects of polyunsaturated and saturated fat on extinction learning. Appetite 2018, 126, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Tsubono, Y.; Takamori, S.; Kobayashi, M.; Takahashi, T.; Iwase, Y.; Iitoi, Y.; Akabane, M.; Yamaguchi, M.; Tsugane, S. A data-based approach for designing a semiquantitative food frequency questionnaire for a population-based prospective study in Japan. J. Epidemiol. 1996, 6, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsugane, S.; Sasaki, S.; Kobayashi, M.; Tsubono, Y.; Akabane, M. Validity and reproducibility of the self-administered food frequency questionnaire in the JPHC Study Cohort I: Study design, conduct and participant profiles. J. Epidemiol. 2003, 13, S2–S12. [Google Scholar] [CrossRef] [Green Version]
- Momino, K.; Akechi, T.; Yamashita, T.; Fujita, T.; Hayahi, H.; Tsunoda, N.; Miyashita, M.; Iwata, H. Psychometric properties of the Japanese version of the Concerns About Recurrence Scale (CARS-J). Jpn. J. Clin. Oncol. 2014, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Muramatsu, K.; Miyaoka, H.; Kamijima, K.; Muramatsu, Y.; Yoshida, M.; Otsubo, T.; Gejyo, F. The patient health questionnaire, Japanese version: Validity according to the mini-international neuropsychiatric interview-plus. Psychol. Rep. 2007, 101, 952–960. [Google Scholar] [CrossRef]
- Shinozaki, M.; Kanazawa, M.; Sagami, Y.; Endo, Y.; Hongo, M.; Drossman, D.A.; Whitehead, W.E.; Fukudo, S. Validation of the Japanese version of the Rome II modular questionnaire and irritable bowel syndrome severity index. J. Gastroenterol. 2006, 41, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Pharmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotwal, S.; Jun, M.; Sullivan, D.; Perkovic, V.; Neal, B. Omega 3 Fatty acids and cardiovascular outcomes: Systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 808–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and probiotics for depression and anxiety: A systematic review and meta-analysis of controlled clinical trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef]
- Taichman, D.B.; Sahni, P.; Pinborg, A.; Peiperl, L.; Laine, C.; James, A.; Hong, S.T.; Haileamlak, A.; Gollogly, L.; Godlee, F.; et al. Data Sharing Statements for Clinical Trials—A Requirement of the International Committee of Medical Journal Editors. N. Engl. J. Med. 2017, 376, 2277–2279. [Google Scholar] [CrossRef]
- Okubo, R.; Wada, S.; Shimizu, Y.; Tsuji, K.; Hanai, A.; Imai, K.; Uchitomi, Y.; Fujiwara, Y.; Tsugane, S.; Matsuoka, Y.J. Expectations of and recommendations for a cancer survivorship guideline in Japan: A literature review of guidelines for cancer survivorship. Jpn. J. Clin. Oncol. 2019, 49, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Noguchi, H.; Hamazaki, K.; Sekiguchi, M.; Kinoshita, T.; Katsumata, N.; Narisawa, T.; Uezono, Y.; Xiao, J.; Matsuoka, Y.J. Association between blood polyunsaturated fatty acid levels and depressive symptoms in breast cancer survivors. Prostaglandins Leukot. Essent. Fat. Acids 2018, 139, 9–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Screening Period | Treatment Period | ||||
|---|---|---|---|---|---|
| Rater | Pre-Entry Screening | Baseline Assessment 1 | Random Allocation 1 | Outcome Assessment 2 | |
| Enrolment | |||||
| Screening for eligibility | Physician | × | |||
| Informed consent | CRC/Physician | × | |||
| Registration to EDC | CRC | × | |||
| Assessment | |||||
| Baseline characteristics of participants | CRC | × | |||
| Blood fatty acid test | CRC | × | |||
| Interstitial flora | CRC | × | × | ||
| CARS assessed via interview | CRC/masked rater | ×(CRC) | ×(masked raters) | ||
| PHQ-9 | PRO questionnaires | × | × | ||
| IBS-SI | PRO questionnaires | × | × | ||
| Information about allocated groups | CRC | × | |||
| Adverse reactions | CRC/PRO questionnaires | × | |||
| ← As needed throughout protocol → | |||||
| Data Sharing Policy | |
|---|---|
| Is IPD available? | Yes |
| What types of data will be shared? | All anonymized IPD reported in the paper (body text, tables, and figures) |
| Are there any other documents available? | Protocol paper |
| How long will the data be available for? | For 5 years after publication of the paper |
| Who will use the data? | Researchers who have presented plans with appropriate methodologies |
| What types of analysis will this be used for? | For meta-analyses using IPD |
| How can the data be accessed? | Interested researchers should send a request for data sharing, along with a synopsis of the secondary analysis plan, to the Principal Investigator (RO) by email ([email protected]). The study administrative office will examine the request and, if approved, send a letter of approval for data sharing to the requesting researcher. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sasaki, Y.; Honyashiki, M.; Kinoshita, T.; Matsui, A.; Nakashoji, A.; Inagawa, T.; Ikezawa, S.; Yoshimura, N.; Yamamura, R.; Amano, M.; et al. Perilla Oil and Bifidobacterium for Alleviating Fear of Cancer Recurrence in Breast Cancer Survivors: Study Protocol for a Three-Arm Phase II Randomized Controlled Study (POB Study). Methods Protoc. 2021, 4, 46. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030046
Sasaki Y, Honyashiki M, Kinoshita T, Matsui A, Nakashoji A, Inagawa T, Ikezawa S, Yoshimura N, Yamamura R, Amano M, et al. Perilla Oil and Bifidobacterium for Alleviating Fear of Cancer Recurrence in Breast Cancer Survivors: Study Protocol for a Three-Arm Phase II Randomized Controlled Study (POB Study). Methods and Protocols. 2021; 4(3):46. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030046
Chicago/Turabian StyleSasaki, Yohei, Mina Honyashiki, Takayuki Kinoshita, Akira Matsui, Ayako Nakashoji, Takuma Inagawa, Satoru Ikezawa, Naoki Yoshimura, Ryodai Yamamura, Mizuki Amano, and et al. 2021. "Perilla Oil and Bifidobacterium for Alleviating Fear of Cancer Recurrence in Breast Cancer Survivors: Study Protocol for a Three-Arm Phase II Randomized Controlled Study (POB Study)" Methods and Protocols 4, no. 3: 46. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030046