
Experimental Protocol to Assess Neuromuscular Plasticity Induced by an Exoskeleton Training Session

 ,
,  , ,
, ,  ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
- Neurophysiological signals as biomarkers of brain plasticity induced by exoskeleton training. EEG and/or electromyographic (EMG) pattern modifications induced by robotic training may be markers to quantify and track neuromuscular plasticity [6,9]. Since commonly used clinical scales rely mainly on subjective functional assessments and are not able to provide a complete description of patients’ neuro-biomechanical status, current clinical tests should be integrated with specific physiological measurements to obtain a deeper understanding of the effect of the rehabilitative intervention [16].
- Robotic training to restore gait patterns. Conventional rehabilitative interventions using robotic technology facilitate sensorimotor recovery by supporting and motivating participants to practice specific tasks [17,18]. Exoskeletons are a promising task-oriented tool intended to restore a more physiological gait pattern in highly compromised individuals [6,7,8] and to recover physiological alternated activations of lower limb muscles [19].
- Neurophysiological signals as predictors of gait trajectory. EEG and EMG signals related to gait in healthy older adults and stroke survivors are attracting researchers’ attention [20,21]. Concurrent analysis of these physiological signals may deepen the understanding of the neuro-motor control of walking [22,23]. We need to single out a clear-cut biomarker that precedes biomechanical modifications and which is most likely to be a cerebral signature, i.e., specific anticipatory potentials [24].
2. Materials and Methods
2.1. Inclusion Criteria & Clinical Data
2.1.1. Control Participants
- sample size: N ≥ 10 participants;
- 50% female (F), 50% male (M) participants;
- 40–60 years-old.
- previous or ongoing orthopedic or rheumatological disease;
- central and peripheral nervous system diseases;
- dermatological problems or anthropometric measurements limiting exoskeleton use;
- intake of any drug with a central nervous system effect;
- scalp lesions.
2.1.2. Stroke Survivors
- sample size: N ≥ 20;
- 50% F, 50% M;
- (40–60) years-old;
- Within 3 months from stroke;
- First ever supratentorial ischemic stroke (lesion localization will be collected and considered as a covariate for the statistical analyses);
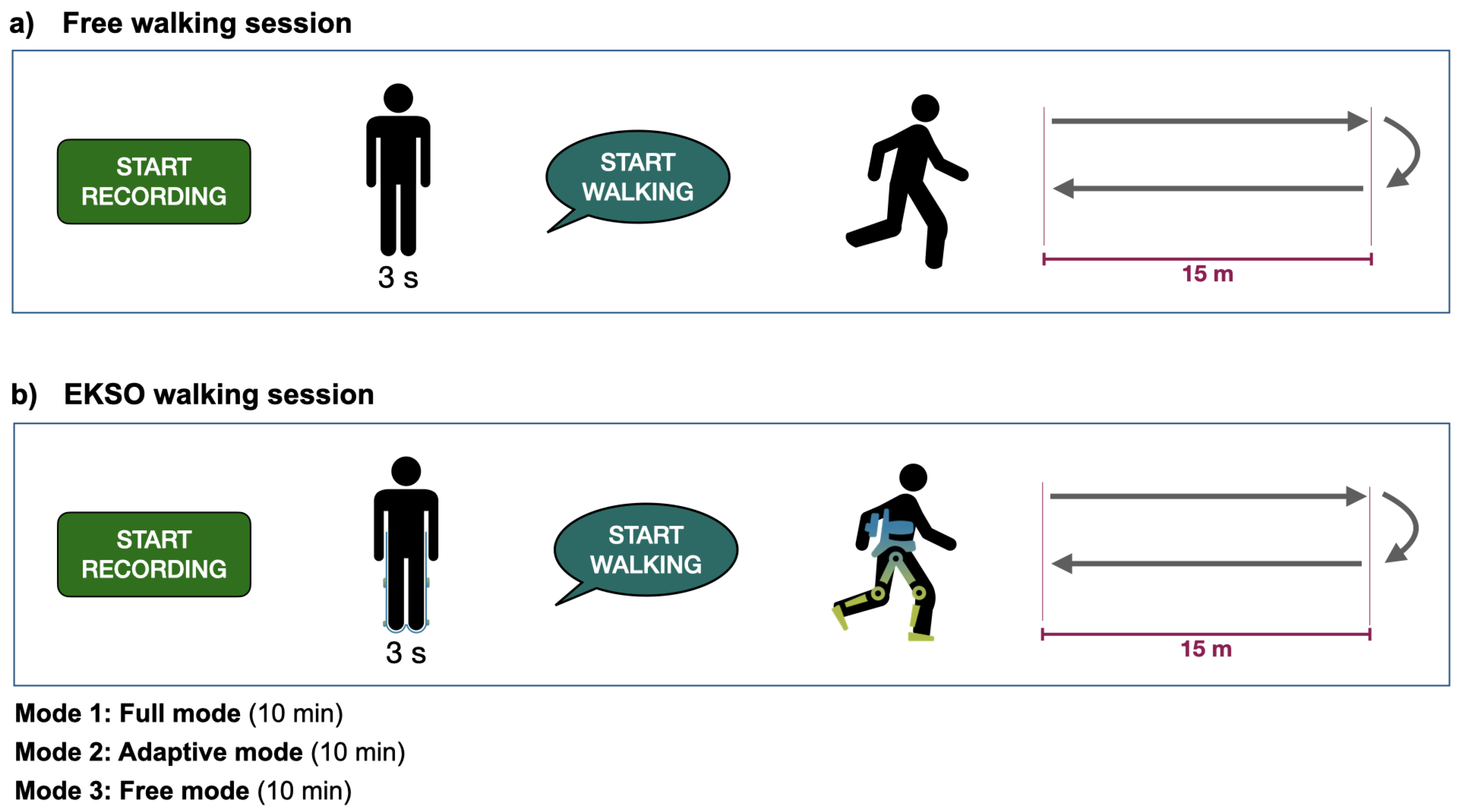
- FAC [26], as stroke survivors are required to perform a free overground walking trial before and after the EKSO training session, as well as the EKSO walking in free mode (i.e., with motors off).
- receptive aphasia;
- unilateral spatial neglect or cognitive issues that may limit capacity for informed consent or full cooperation;
- co-existing orthopaedic, dermatological or neuromuscular disorders that limit EMG data testing;
- previous history of EEG abnormalities or epilepsy;
- scalp lesions (breaches).
2.1.3. Clinical Data to Collect from Stroke Survivors
- Drugs intake;
- Medical therapy;
- Date of the clinical event;
- Lesion location (Bamford classification [27]);
- Intervention (e.g., thrombolysis, thrombectomy or standard medical care);
- Neuroimaging data (Magnetic Resonance Imaging and/or Computed Tomography);
- National Institutes of Health Stroke Scale to assess the impairment caused by the stroke (NIHSS) [28];
- Medical therapy;
- Oxford Cognitive Screen, which was developed to identify common deficits after stroke, such as aphasia, spatial neglect, apraxia, and reading/writing problems [29];
- Muscle strength assessed with the Medical Research Council (MRC) Scale [30] of ileopasoas, quadriceps femoris, hamstrings, tibialis anterior, triceps surae;
- Sensory testing: light touch, pain, proprioception and vibration;
- Modified Ashworth Scale of the affected lower Limb (MAS): to evaluate the muscle spasticity of the hip adductor, knee extensor, and ankle plantar flexor [31];
- Functional Ambulation Category (FAC) to evaluate functional ambulation [26], collected retrospectively (i.e., before) and after the acute event;
- Modified Barthel Index (mBI) to assess independence in activities of daily living [34];
- Orpington Prognostic Score as assessment of stroke severity, e.g., motor deficits, proprioception, motion and cognition [35].
2.1.4. EKSO Inclusion Criteria
- Subjects must tolerate standing;
- Height: 1.6–1.9 m;
- Body mass kg;
- Upper leg length discrepancy cm;
- Lower leg length discrepancy cm;
- Muscle hypertonia quantified as MAS at lower limbs [31];
- No muscle-tendons retractions.
2.2. Materials
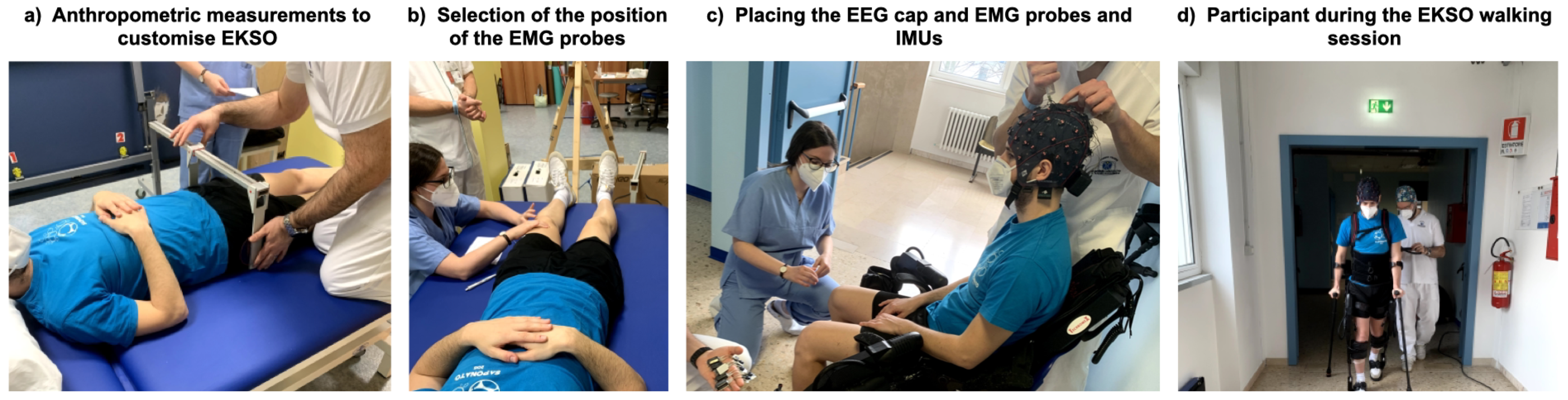
2.3. Procedure
2.3.1. Data Acquisition
2.3.2. Experimental Protocol
2.4. System Usability and Wearability
2.5. Foreseen Data Processing
3. Expected Results
- Investigate how a robotic device interacts with the end-user in able bodied subjects and individuals with neurological disorders;
- Define the neurophysiological processes underlying both locomotor control with and without an exoskeleton and gait recovery through a robot-assisted gait training;
- Determine optimal training parameters for individualized gait training (based on knowledge built on 1. and 2.).
- Boost the clinical use of EEG, EMG and exoskeletons for gait rehabilitation in clinical settings both for clinical and research purposes and help breaking down barriers associated with cultural background and lack of expertise of the multi-disciplinary teams, which are crucial for this kind of intervention [6,60,61];
- Determine the feasibility of controlling an exoskeleton with physiological (e.g., EEG and/or EMG) signals.
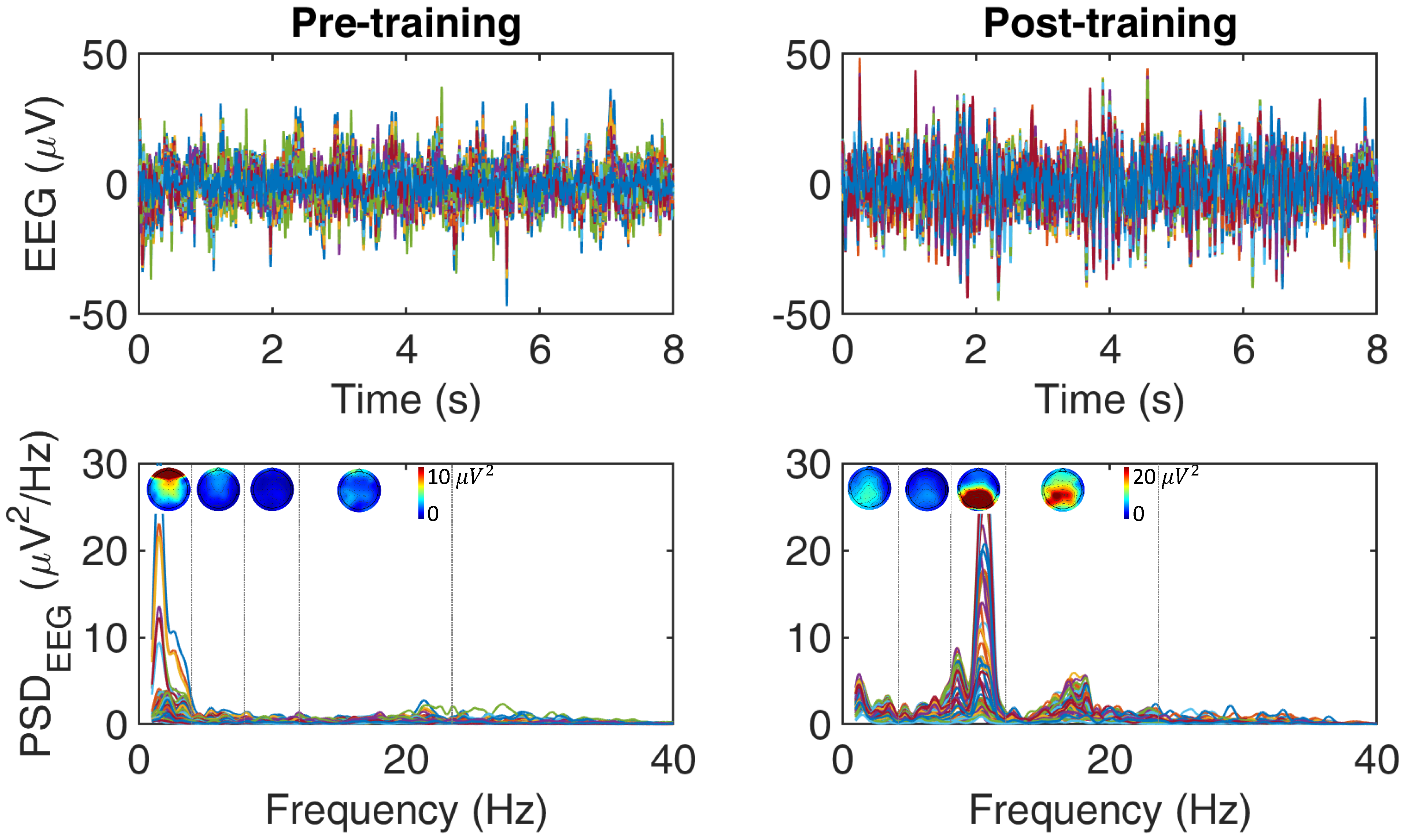
- A high-density EEG set-up is required to reconstruct the brain cortical activity minimizing leakage effects, targeting the brain areas involved in the tasks (e.g., through power spectra or time-frequency analysis) and their interactions (e.g., effective connectivity and network/graph analysis [69,70,71])
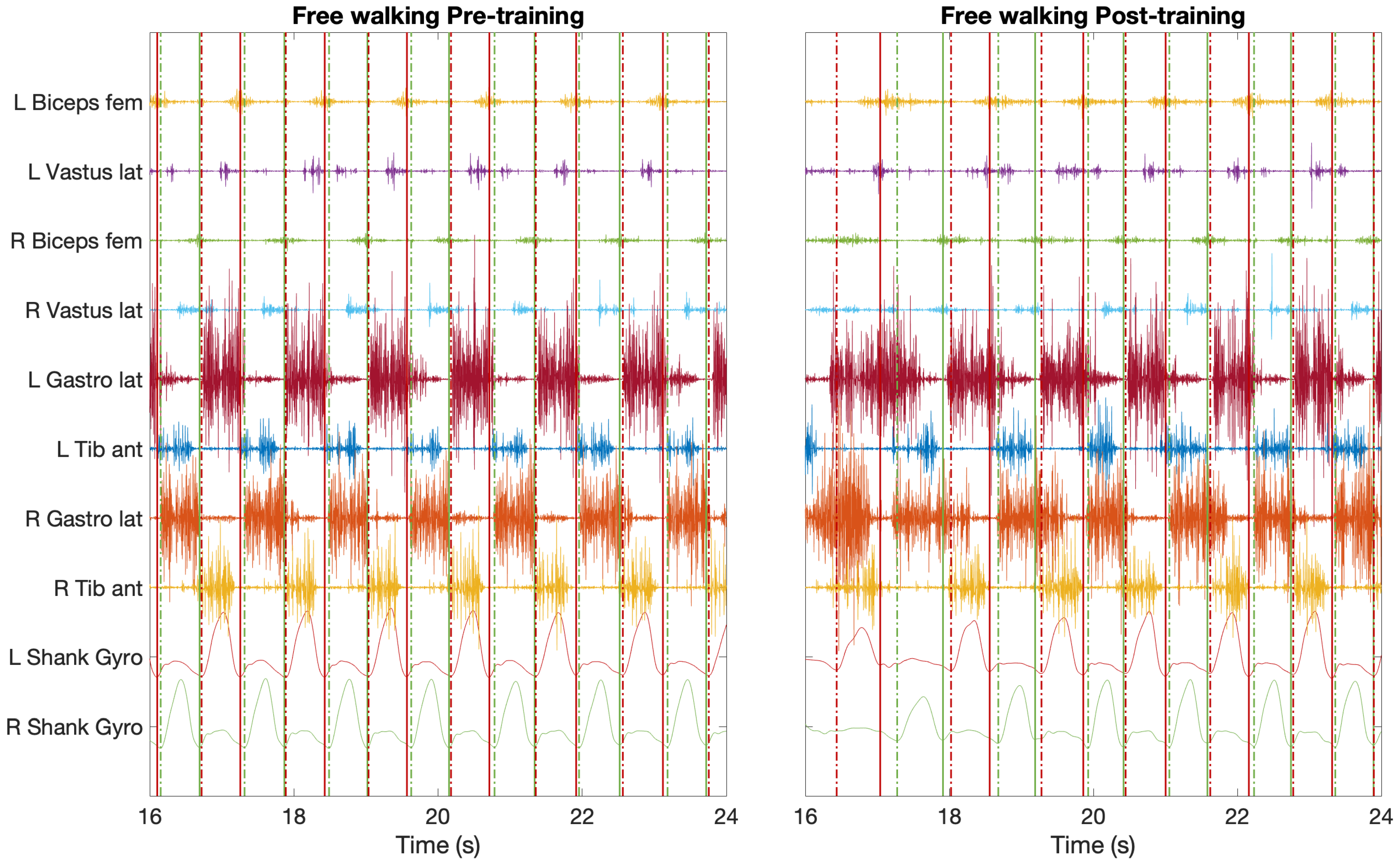
- The synchronous EMG signals are required to identify antagonistic-agonistic muscular activation during gait and muscles response to exoskeleton.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AP | Anterior-Posterior direction |
| CoA | Centre of Activity |
| CoM | Centre of Mass |
| CRS | Comfort Rating Scale |
| DALYs | Disability Adjusted Life Years |
| EEG | Electroencephalography |
| EMG | Electromyography |
| FAC | Functional Ambulation Category |
| IMU | Inertial Measurement Units |
| L5 | Fifth lumbar vertebra |
| MAS | Modified Ashworth Scale |
| mBI | Modified Barthel Index |
| MCA | Minimal Crosstalk Area |
| ML | Medial-lateral direction |
| MRC | Medical Research Council Scale |
| NIHSS | National Institutes of Health Stroke Scale |
| VT | Vertical direction |
References
- Winters, C.; Van Wegen, E.E.H.; Daffertshofer, A.; Kwakkel, G. Generalizability of the Proportional Recovery Model for the Upper Extremity After an Ischemic Stroke. Neurorehabilit. Neural Repair 2015, 29, 614–622. [Google Scholar] [CrossRef]
- Ward, N.S. Restoring brain function after stroke—bridging the gap between animals and humans. Nat. Rev. Neurol. 2017, 13, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Salem, Y.; Pappas, E. Overground gait training for individuals with chronic stroke: A Cochrane systematic review. J. Neurol. Phys. Ther. 2009, 33, 179–186. [Google Scholar]
- Hornby, T.G.; Holleran, C.L.; Leddy, A.L.; Hennessy, P.; Leech, K.A.; Connolly, M.; Moore, J.L.; Straube, D.; Lovell, L.; Roth, E. Feasibility of focused stepping practice during inpatient rehabilitation poststroke and potential contributions to mobility outcomes. Neurorehabilit. Neural Repair 2015, 29, 923–932. [Google Scholar] [CrossRef] [PubMed]
- Dee, M.; Lennon, O.; O’Sullivan, C. A systematic review of physical rehabilitation interventions for stroke in low and lower-middle income countries. Disabil. Rehabil. 2020, 42, 473–501. [Google Scholar] [CrossRef] [PubMed]
- Lennon, O.; Tonellato, M.; Del Felice, A.; Di Marco, R.; Fingleton, C.; Korik, A.; Guanziroli, E.; Molteni, F.; Guger, C.; Otner, R.; et al. A Systematic Review Establishing the Current State-of-the-Art, the Limitations, and the DESIRED Checklist in Studies of Direct Neural Interfacing With Robotic Gait Devices in Stroke Rehabilitation. Front. Neurosci. 2020, 14, 578. [Google Scholar] [CrossRef]
- Caliandro, P.; Molteni, F.; Simbolotti, C.; Guanziroli, E.; Iacovelli, C.; Reale, G.; Giovannini, S.; Padua, L. Exoskeleton-assisted gait in chronic stroke: An EMG and functional near-infrared spectroscopy study of muscle activation patterns and prefrontal cortex activity. Clin. Neurophysiol. 2020, 131, 1775–1781. [Google Scholar] [CrossRef]
- Molteni, F.; Guanziroli, E.; Goffredo, M.; Calabrò, R.S.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Galafate, D.; et al. Gait Recovery with an Overground Powered Exoskeleton: A Randomized Controlled Trial on Subacute Stroke Subjects. Brain Sci. 2021, 11, 104. [Google Scholar] [CrossRef]
- Gandolfi, M.; Formaggio, E.; Geroin, C.; Storti, S.F.; Boscolo Galazzo, I.; Bortolami, M.; Saltuari, L.; Picelli, A.; Waldner, A.; Manganotti, P.; et al. Quantification of upper limb motor recovery and EEG power changes after robot-assisted bilateral arm training in chronic stroke patients: A prospective pilot study. Neural Plast. 2018, 2018, 8105480. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Eguren, D.; Azorín, J.M.; Grossman, R.G.; Luu, T.P.; Contreras-Vidal, J.L. Brain–machine interfaces for controlling lower-limb powered robotic systems. J. Neural Eng. 2018, 15, 021004. [Google Scholar] [CrossRef]
- Tonin, L.; Millán, J.d.R. Noninvasive Brain–Machine Interfaces for Robotic Devices. Annu. Rev. Control. Robot. Auton. Syst. 2021, 4. [Google Scholar] [CrossRef]
- Donati, A.R.; Shokur, S.; Morya, E.; Campos, D.S.; Moioli, R.C.; Gitti, C.M.; Augusto, P.B.; Tripodi, S.; Pires, C.G.; Pereira, G.A.; et al. Long-term training with a brain-machine interface-based gait protocol induces partial neurological recovery in paraplegic patients. Sci. Rep. 2016, 6, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokur, S.; Donati, A.R.; Campos, D.S.; Gitti, C.; Bao, G.; Fischer, D.; Almeida, S.; Braga, V.A.; Augusto, P.; Petty, C.; et al. Training with brain-machine interfaces, visuo-tactile feedback and assisted locomotion improves sensorimotor, visceral, and psychological signs in chronic paraplegic patients. PLoS ONE 2018, 13, e0206464. [Google Scholar] [CrossRef]
- He, Y.; Nathan, K.; Venkatakrishnan, A.; Rovekamp, R.; Beck, C.; Ozdemir, R.; Francisco, G.E.; Contreras-Vidal, J.L. An integrated neuro-robotic interface for stroke rehabilitation using the NASA X1 powered lower limb exoskeleton. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 3985–3988. [Google Scholar]
- Contreras-Vidal, J.L.; Bortole, M.; Zhu, F.; Nathan, K.; Venkatakrishnan, A.; Francisco, G.E.; Soto, R.; Pons, J.L. Neural decoding of robot-assisted gait during rehabilitation after stroke. Am. J. Phys. Med. Rehabil. 2018, 97, 541–550. [Google Scholar] [CrossRef] [PubMed]
- Pierella, C.; Pirondini, E.; Kinany, N.; Coscia, M.; Giang, C.; Miehlbradt, J.; Magnin, C.; Nicolo, P.; Dalise, S.; Sgherri, G.; et al. A multimodal approach to capture post-stroke temporal dynamics of recovery. J. Neural Eng. 2020, 17, 045002. [Google Scholar] [CrossRef] [PubMed]
- Scalona, E.; Taborri, J.; Hayes, D.R.; Del Prete, Z.; Rossi, S.; Palermo, E. Is the Neuromuscular Organization of Throwing Unchanged in Virtual Reality? Implications for Upper Limb Rehabilitation. Electronics 2019, 8, 1495. [Google Scholar] [CrossRef] [Green Version]
- Colombo, R.; Sterpi, I.; Mazzone, A.; Delconte, C.; Pisano, F. Robot-aided neurorehabilitation in sub-acute and chronic stroke: Does spontaneous recovery have a limited impact on outcome? NeuroRehabilitation 2013, 33, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Gandolla, M.; Guanziroli, E.; D’Angelo, A.; Cannaviello, G.; Molteni, F.; Pedrocchi, A. Automatic setting procedure for exoskeleton-assisted overground gait: Proof of concept on stroke population. Front. Neurorobot. 2018, 12, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubega, M.; Di Marco, R.; Zampini, M.; Formaggio, E.; Menegatti, E.; Masiero, S.; Bonato, P.; Del Felice, A. Muscular and cortical activation during dynamic and static balance in the elderly: A scoping review. Aging Brain 2021, 1, 100013. [Google Scholar] [CrossRef]
- Rubega, M.; Formaggio, E.; Di Marco, R.; Bertuccelli, M.; Tortora, S.; Menegatti, E.; Cattelan, M.; Bonato, P.; Masiero, S.; Del Felice, A. Cortical Correlates in Upright Dynamic and Static Balance in the Elderly. Sci. Rep. 2021, 11, 1–15. [Google Scholar] [CrossRef]
- Artoni, F.; Fanciullacci, C.; Bertolucci, F.; Panarese, A.; Makeig, S.; Micera, S.; Chisari, C. Unidirectional brain to muscle connectivity reveals motor cortex control of leg muscles during stereotyped walking. Neuroimage 2017, 159, 403–416. [Google Scholar] [CrossRef]
- Gennaro, F.; De Bruin, E.D. Assessing brain–muscle connectivity in human locomotion through mobile brain/body imaging: Opportunities, pitfalls, and future directions. Front. Public Health 2018, 6, 39. [Google Scholar] [CrossRef] [Green Version]
- Rubega, M.; Formaggio, E.; Molteni, F.; Guanziroli, E.; Di Marco, R.; Baracchini, C.; Ermani, M.; Ward, N.S.; Masiero, S.; Del Felice, A. EEG Fractal Analysis Reflects Brain Impairment after Stroke. Entropy 2021, 23, 592. [Google Scholar] [CrossRef]
- ProGait. Available online: http://www.progait.eu/ (accessed on 12 July 2021).
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired: Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef]
- Bamford, J.; Sandercock, P.; Dennis, M.; Warlow, C.; Burn, J. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 1991, 337, 1521–1526. [Google Scholar] [CrossRef]
- Cincura, C.; Pontes-Neto, O.M.; Neville, I.S.; Mendes, H.F.; Menezes, D.F.; Mariano, D.C.; Pereira, I.F.; Teixeira, L.A.; Jesus, P.A.; De Queiroz, D.C.; et al. Validation of the National Institutes of Health Stroke Scale, modified Rankin Scale and Barthel Index in Brazil: The role of cultural adaptation and structured interviewing. Cerebrovasc. Dis. 2009, 27, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Demeyere, N.; Riddoch, M.; Slavkova, E.; Jones, K.; Reckless, I.; Mathieson, P.; Humphreys, G. Domain-specific versus generalized cognitive screening in acute stroke. J. Neurol. 2016, 263, 306–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paternostro-Sluga, T.; Grim-Stieger, M.; Posch, M.; Schuhfried, O.; Vacariu, G.; Mittermaier, C.; Bittner, C.; Fialka-Moser, V. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J. Rehabil. Med. 2008, 40, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W.; Smith, M.B. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys. Ther. 1987, 67, 206–207. [Google Scholar] [CrossRef]
- Rankin, J. Cerebral vascular accidents in patients over the age of 60: II. Prognosis. Scott. Med. J. 1957, 2, 200–215. [Google Scholar] [CrossRef]
- Van Swieten, J.; Koudstaal, P.; Visser, M.; Schouten, H.; Van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsueh, I.P.; Lin, J.H.; Jeng, J.S.; Hsieh, C.L. Comparison of the psychometric characteristics of the functional independence measure, 5 item Barthel index, and 10 item Barthel index in patients with stroke. J. Neurol. Neurosurg. Psychiatry 2002, 73, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Kalra, L.; Crome, P. The role of prognostic scores in targeting stroke rehabilitation in elderly patients. J. Am. Geriatr. Soc. 1993, 41, 396–400. [Google Scholar] [CrossRef]
- Strausser, K.A.; Kazerooni, H. The development and testing of a human machine interface for a mobile medical exoskeleton. In Proceedings of the 2011 IEEE/RSJ International Conference on Intelligent Robots and Systems, San Francisco, CA, USA, 25–30 September 2011; pp. 4911–4916. [Google Scholar]
- Molteni, F.; Gasperini, G.; Gaffuri, M.; Colombo, M.; Giovanzana, C.; Lorenzon, C.; Farina, N.; Cannaviello, G.; Scarano, S.; Proserpio, D.; et al. Wearable robotic exoskeleton for overground gait training in sub-acute and chronic hemiparetic stroke patients: Preliminary results. Eur. J. Phys. Rehabil. Med. 2017, 53, 676–684. [Google Scholar] [CrossRef]
- Blanc, Y.; Dimanico, U. Electrode Placement in Surface Electromyography (sEMG) “Minimal Crosstalk Area”. Open Rehabil. J. 2010, 3, 110–126. [Google Scholar] [CrossRef] [Green Version]
- Basmajian, J.V. Electrode Placement in Electromyographic Biofeedback; Williams & Wilkins: Philadelphia, PA, USA, 1983. [Google Scholar]
- Campanini, I.; Merlo, A.; Degola, P.; Merletti, R.; Vezzosi, G.; Farina, D. Effect of electrode location on EMG signal envelope in leg muscles during gait. J. Electromyogr. Kinesiol. 2007, 17, 515–526. [Google Scholar] [CrossRef]
- Latt, M.D.; Menz, H.B.; Fung, V.S.; Lord, S.R. Acceleration patterns of the head and pelvis during gait in older people with Parkinson’s disease: A comparison of fallers and nonfallers. J. Gerontol. Ser. A 2009, 64, 700–706. [Google Scholar] [CrossRef] [Green Version]
- Pasciuto, I.; Bergamini, E.; Iosa, M.; Vannozzi, G.; Cappozzo, A. Overcoming the limitations of the Harmonic Ratio for the reliable assessment of gait symmetry. J. Biomech. 2017, 53, 84–89. [Google Scholar] [CrossRef]
- Bisi, M.; Tamburini, P.; Stagni, R. A ‘fingerprint’ of locomotor maturation: Motor development descriptors, reference development bands and data-set. Gait Posture 2019, 68, 232–237. [Google Scholar] [CrossRef] [PubMed]
- El-Gohary, M.; Pearson, S.; McNames, J.; Mancini, M.; Horak, F.; Mellone, S.; Chiari, L. Continuous monitoring of turning in patients with movement disability. Sensors 2014, 14, 356–369. [Google Scholar] [CrossRef] [Green Version]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.; Dehollain, C.; Blanc, Y.; Burkhard, P.R.; Aminian, K. Gait assessment in Parkinson’s disease: Toward an ambulatory system for long-term monitoring. IEEE Trans. Biomed. Eng. 2004, 51, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Moe-Nilssen, R. A new method for evaluating motor control in gait under real-life environmental conditions. Part 1: The instrument. Clin. Biomech. 1998, 13, 320–327. [Google Scholar] [CrossRef]
- Borg, G. Simple rating for estimation of perceived exertion. Phys. Work Effort 1975, 39–46. [Google Scholar]
- Knight, J.F.; Baber, C. A tool to assess the comfort of wearable computers. Hum. Factors 2005, 47, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.F.; Deen-Williams, D.; Arvanitis, T.N.; Baber, C.; Sotiriou, S.; Anastopoulou, S.; Gargalakos, M. Assessing the wearability of wearable computers. In Proceedings of the 2006 10th IEEE International Symposium on Wearable Computers, Montreux, Switzerland, 11–14 October 2006; pp. 75–82. [Google Scholar]
- Lewis, J.R. The system usability scale: Past, present, and future. Int. J. Hum. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Pirondini, E.; Coscia, M.; Minguillon, J.; Millán, J.d.R.; Van De Ville, D.; Micera, S. EEG topographies provide subject-specific correlates of motor control. Sci. Rep. 2017, 7, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Rubega, M.; Carboni, M.; Seeber, M.; Pascucci, D.; Tourbier, S.; Toscano, G.; Van Mierlo, P.; Hagmann, P.; Plomp, G.; Vulliemoz, S.; et al. Estimating EEG source dipole orientation based on singular-value decomposition for connectivity analysis. Brain Topogr. 2019, 32, 704–719. [Google Scholar] [CrossRef] [Green Version]
- Siragy, T.; Nantel, J. Quantifying dynamic balance in young, elderly and Parkinson’s individuals: A systematic review. Front. Aging Neurosci. 2018, 10, 387. [Google Scholar] [CrossRef] [Green Version]
- Wheaton, L.A.; Mizelle, J.; Forrester, L.W.; Bai, O.; Shibasaki, H.; Macko, R.F. How does the brain respond to unimodal and bimodal sensory demand in movement of the lower extremity? Exp. Brain Res. 2007, 180, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Butt, M.; Naghdy, G.; Naghdy, F.; Murray, G.; Du, H. Patient-Specific Robot-Assisted Stroke Rehabilitation Guided by EEG—A Feasibility Study. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 2841–2844. [Google Scholar]
- Van Criekinge, T.; Vermeulen, J.; Wagemans, K.; Schröder, J.; Embrechts, E.; Truijen, S.; Hallemans, A.; Saeys, W. Lower limb muscle synergies during walking after stroke: A systematic review. Disabil. Rehabil. 2020, 42, 2836–2845. [Google Scholar] [CrossRef]
- Srivastava, S.; Kao, P.C.; Reisman, D.S.; Scholz, J.P.; Agrawal, S.K.; Higginson, J.S. Robotic assist-as-needed as an alternative to therapist-assisted gait rehabilitation. Int. J. Phys. Med. Rehabil. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Sylos-Labini, F.; La Scaleia, V.; d’Avella, A.; Pisotta, I.; Tamburella, F.; Scivoletto, G.; Molinari, M.; Wang, S.; Wang, L.; van Asseldonk, E.; et al. EMG patterns during assisted walking in the exoskeleton. Front. Hum. Neurosci. 2014, 8, 423. [Google Scholar] [CrossRef] [PubMed]
- Berens, P. CircStat: A MATLAB toolbox for circular statistics. J. Stat. Softw. 2009, 31, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Campanini, I.; Rymer, W.Z.; Disselhorst-Klug, C. Surface Electromyography: Barriers Limiting Widespread Use of sEMG in Clinical Assessment and Neurorehabilitation. Front. Neurol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Goffredo, M.; Infarinato, F.; Pournajaf, S.; Romano, P.; Ottaviani, M.; Pellicciari, L.; Galafate, D.; Gabbani, D.; Gison, A.; Franceschini, M. Barriers to sEMG assessment during overground robot-assisted gait training in subacute stroke patients. Front. Neurol. 2020, 11, 1263. [Google Scholar] [CrossRef]
- Rojek, A.; Mika, A.; Oleksy, Ł.; Stolarczyk, A.; Kielnar, R. Effects of exoskeleton gait training on balance, load distribution, and functional status in stroke: A randomized controlled trial. Front. Neurol. 2020, 10, 1344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffredo, M.; Guanziroli, E.; Pournajaf, S.; Gaffuri, M.; Gasperini, G.; Filoni, S.; Baratta, S.; Damiani, C.; Franceschini, M.; Molteni, F.; et al. Overground wearable powered exoskeleton for gait training in subacute stroke subjects: Clinical and gait assessments. Eur. J. Phys. Rehabil. Med. 2019, 55, 710–721. [Google Scholar] [CrossRef]
- Seeber, M.; Scherer, R.; Wagner, J.; Solis-Escalante, T.; Müller-Putz, G.R. EEG beta suppression and low gamma modulation are different elements of human upright walking. Front. Hum. Neurosci. 2014, 8, 485. [Google Scholar] [CrossRef] [Green Version]
- Seeber, M.; Scherer, R.; Wagner, J.; Solis-Escalante, T.; Müller-Putz, G.R. High and low gamma EEG oscillations in central sensorimotor areas are conversely modulated during the human gait cycle. Neuroimage 2015, 112, 318–326. [Google Scholar] [CrossRef]
- Knaepen, K.; Mierau, A.; Swinnen, E.; Tellez, H.F.; Michielsen, M.; Kerckhofs, E.; Lefeber, D.; Meeusen, R. Human-robot interaction: Does robotic guidance force affect gait-related brain dynamics during robot-assisted treadmill walking? PLoS ONE 2015, 10, e0140626. [Google Scholar] [CrossRef] [Green Version]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; De Luca, R.; Balletta, T.; Buda, A.; La Rosa, G.; Bramanti, A.; Bramanti, P. The role of virtual reality in improving motor performance as revealed by EEG: A randomized clinical trial. J. Neuroeng. Rehabil. 2017, 14, 1–16. [Google Scholar] [CrossRef]
- Tortora, S.; Ghidoni, S.; Chisari, C.; Micera, S.; Artoni, F. Deep learning-based BCI for gait decoding from EEG with LSTM recurrent neural network. J. Neural Eng. 2020, 17, 046011. [Google Scholar] [CrossRef]
- Rubega, M.; Pascucci, D.; Queralt, J.R.; Van Mierlo, P.; Hagmann, P.; Plomp, G.; Michel, C.M. Time-varying effective EEG source connectivity: The optimization of model parameters. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6438–6441. [Google Scholar]
- Pascucci, D.; Rubega, M.; Plomp, G. Modeling time-varying brain networks with a self-tuning optimized Kalman filter. PLoS Comput. Biol. 2020, 16, e1007566. [Google Scholar] [CrossRef] [PubMed]
- Damborská, A.; Honzírková, E.; Barteček, R.; Hořínková, J.; Fedorová, S.; Ondruš, Š.; Michel, C.M.; Rubega, M. Altered directed functional connectivity of the right amygdala in depression: High-density EEG study. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfurtscheller, G.; Brunner, C.; Schlögl, A.; Da Silva, F.L. Mu rhythm (de) synchronization and EEG single-trial classification of different motor imagery tasks. NeuroImage 2006, 31, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Perry, J. Gait Analysis: Normal and Pathological Function; SLACK Incorporated: Thorofare, NJ, USA, 1992. [Google Scholar]
- De Luca, A.; Bellitto, A.; Mandraccia, S.; Marchesi, G.; Pellegrino, L.; Coscia, M.; Leoncini, C.; Rossi, L.; Gamba, S.; Massone, A.; et al. Exoskeleton for gait rehabilitation: Effects of assistance, mechanical structure, and walking aids on muscle activations. Appl. Sci. 2019, 9, 2868. [Google Scholar] [CrossRef] [Green Version]
- Androwis, G.J.; Pilkar, R.; Ramanujam, A.; Nolan, K.J. Electromyography assessment during gait in a robotic exoskeleton for acute stroke. Front. Neurol. 2018, 9, 630. [Google Scholar] [CrossRef] [Green Version]
- Molteni, F.; Formaggio, E.; Bosco, A.; Guanziroli, E.; Piccione, F.; Masiero, S.; Del Felice, A. Brain connectivity modulation after exoskeleton-assisted gait in chronic hemiplegic stroke survivors: A pilot study. Am. J. Phys. Med. Rehabil. 2020, 99, 694–700. [Google Scholar] [CrossRef]
- Zhu, F.; Kern, M.; Fowkes, E.; Afzal, T.; Contreras-Vidal, J.L.; Francisco, G.E.; Chang, S.H. Effects of an exoskeleton-assisted gait training on post-stroke lower-limb muscle coordination. J. Neural Eng. 2021, 18, 046039. [Google Scholar] [CrossRef] [PubMed]
- Gwin, J.T.; Gramann, K.; Makeig, S.; Ferris, D.P. Removal of movement artifact from high-density EEG recorded during walking and running. J. Neurophysiol. 2010, 103, 3526–3534. [Google Scholar] [CrossRef] [Green Version]
- Snyder, K.L.; Kline, J.E.; Huang, H.J.; Ferris, D.P. Independent component analysis of gait-related movement artifact recorded using EEG electrodes during treadmill walking. Front. Hum. Neurosci. 2015, 9, 639. [Google Scholar] [CrossRef] [Green Version]
- Wagner, J.; Solis-Escalante, T.; Grieshofer, P.; Neuper, C.; Müller-Putz, G.; Scherer, R. Level of participation in robotic-assisted treadmill walking modulates midline sensorimotor EEG rhythms in able-bodied subjects. Neuroimage 2012, 63, 1203–1211. [Google Scholar] [CrossRef]
- Delisle-Rodriguez, D.; Villa-Parra, A.C.; Bastos-Filho, T.; López-Delis, A.; Frizera-Neto, A.; Krishnan, S.; Rocon, E. Adaptive spatial filter based on similarity indices to preserve the neural information on eeg signals during on-line processing. Sensors 2017, 17, 2725. [Google Scholar] [CrossRef] [Green Version]
- Kilicarslan, A.; Grossman, R.G.; Contreras-Vidal, J.L. A robust adaptive denoising framework for real-time artifact removal in scalp EEG measurements. J. Neural Eng. 2016, 13, 026013. [Google Scholar] [CrossRef] [PubMed]
- Bhagat, N.A.; Venkatakrishnan, A.; Abibullaev, B.; Artz, E.J.; Yozbatiran, N.; Blank, A.A.; French, J.; Karmonik, C.; Grossman, R.G.; O’Malley, M.K.; et al. Design and optimization of an EEG-based brain machine interface (BMI) to an upper-limb exoskeleton for stroke survivors. Front. Neurosci. 2016, 10, 122. [Google Scholar] [CrossRef] [PubMed]
- Tortora, S.; Tonin, L.; Chisari, C.; Micera, S.; Menegatti, E.; Artoni, F. Hybrid Human-Machine Interface for Gait Decoding Through Bayesian Fusion of EEG and EMG Classifiers. Front. Neur. 2020, 14, 89. [Google Scholar] [CrossRef]
- Chowdhury, A.; Raza, H.; Dutta, A.; Prasad, G. EEG-EMG based hybrid brain computer interface for triggering hand exoskeleton for neuro-rehabilitation. In Proceedings of the Advances in Robotics, New Delhi, India, 28 June–2 July 2017; pp. 1–6. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anatomical District | Participant Positioning | Measurement |
|---|---|---|
| Hip width | Supine (lying down) | Distance between great throcanters |
| Upper leg (left/right) | Supine (flexed knee) | From gluteus to the top of the flexed knee |
| Lower leg (left/right) | Sitting | From shoe soles to the top of flexed knee |
| General Guidelines | |
| Electrode type | Kendall ARBO Ref 31.1245.21 |
| Inter-electrode distance (IED) | 1.5 cm |
| Skin preparation | Dry skin: |
| · Wet the skin on the MCA | |
| · Rub the skin to remove dead cells | |
| · Dry the skin before sticking electrodes | |
| Oily/Creamy skin: | |
| · Rub the skin on MCAs with alcoholic wipes | |
| · Rub the skin to remove dead cells | |
| · Dry the skin before sticking electrodes | |
| Inter-electrode line | Longitudinally to muscle fibers |
| Starting posture | |
| Vastus lateralis | Supine, lying down |
| Biceps femoris | Prone, lying down |
| Tibialis anterior | Supine, lying down |
| Gastrocnemius lateralis | Prone, lying down |
| Electrode location | |
| Vastus lateralis | 25% on the line between the Gerdy’s prominence and the anterior iliac spine |
| Biceps femoris | Lateral side of back thigh, halfway between ischial tuberosity and lateral epicondyle of the tibia |
| Tibialis anterior | On muscle belly at 25% of the line between head of fibula and lateral malleolus |
| Gastrocnemius lateralis | On muscle belly at 25% of the line between head of fibula and lateral malleolus |
| Selectivity check | |
| Vastus lateralis | With flexed hip, complete knee extension |
| Biceps femoris | With neutral hip flexion, complete knee flexion |
| Tibialis anterior | Pull up the toes. Talus-varus movement to check for minimal crosstalk from peroneus longus |
| Gastrocnemius lateralis | Push toes against resistance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Marco, R.; Rubega, M.; Lennon, O.; Formaggio, E.; Sutaj, N.; Dazzi, G.; Venturin, C.; Bonini, I.; Ortner, R.; Cerrel Bazo, H.A.; et al. Experimental Protocol to Assess Neuromuscular Plasticity Induced by an Exoskeleton Training Session. Methods Protoc. 2021, 4, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030048
Di Marco R, Rubega M, Lennon O, Formaggio E, Sutaj N, Dazzi G, Venturin C, Bonini I, Ortner R, Cerrel Bazo HA, et al. Experimental Protocol to Assess Neuromuscular Plasticity Induced by an Exoskeleton Training Session. Methods and Protocols. 2021; 4(3):48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030048
Chicago/Turabian StyleDi Marco, Roberto, Maria Rubega, Olive Lennon, Emanuela Formaggio, Ngadhnjim Sutaj, Giacomo Dazzi, Chiara Venturin, Ilenia Bonini, Rupert Ortner, Humberto Antonio Cerrel Bazo, and et al. 2021. "Experimental Protocol to Assess Neuromuscular Plasticity Induced by an Exoskeleton Training Session" Methods and Protocols 4, no. 3: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/mps4030048