Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”



1
Premature Ejaculation Help, Montreal, QC H1X 1S8, Canada
2
Department of Psychology, Valparaiso University, Valparaiso, IN 46383, USA
*
Author to whom correspondence should be addressed.
Sexes 2020, 1(1), 72-86; https://0-doi-org.brum.beds.ac.uk/10.3390/sexes1010007
Submission received: 15 October 2020
/
Revised: 4 December 2020
/
Accepted: 15 December 2020
/
Published: 18 December 2020
(This article belongs to the Special Issue Sexual Health Challenges in Emerging Nations, Populations, and Minorities: Research, Applications, and Recommendations)
Abstract
:“Ejaculatory control” and “bother/distress” are key criteria for diagnosing men with premature ejaculation (PE), yet compared with ejaculatory latency (EL), these constructs have received only minimal attention. In addition, they have not been characterized in men having different sexual orientations or subtypes of PE. This study aimed to characterize relationships among ejaculatory control, bother/distress, and EL; to assess differences across men having different sexual orientations, PE status, and PE subtypes (i.e., lifelong vs. acquired); and to determine the importance of ejaculatory control to men’s sexual partners. In total, 1071 men and sexual partners of men rated their ejaculatory control and bother/distress and estimated their EL; these measures were compared across sexual orientation, PE status, PE subtype, and male and female partners of men. Results revealed a monotonic though slightly curvilinear relationship between ejaculatory control and bother/distress. These PE criteria differed significantly between PE and non-PE men, to a lesser extent between gay and straight men, and not at all between men having lifelong vs. acquired PE. Female and male partners of men affirmed the importance of ejaculatory control during partnered sex, indicating lack of control as a potential reason for ending a relationship.
1. Introduction
It has been more than 12 years since the International Society of Sexual Medicine (ISSM)—and 8 years since the American Psychiatric Association (APA: DSM-5)—first laid out the three-pronged diagnostic criteria for premature ejaculation (PE): a short ejaculatory latency (EL); the inability to control, delay, or postpone ejaculation; and bother or distress about the condition [1,2,3]. The inclusion of these specific criteria relied on several seminal studies that lent preliminary support to each prong of the definition; subsequently, these criteria became benchmarks for establishing the efficacy of various treatment strategies for men with PE, e.g., [4,5]. Despite an initial flurry of research on these constructs to establish the PE criteria, once embraced, the number of studies designed to further understand and quantify two of the constructs, “ejaculatory control” and “bother/distress,” dwindled to a mere handful.
1.1. Role of Ejaculatory Control
Ejaculatory control may be viewed as a measure of self-efficacy, as the degree to which a man feels that he can achieve a particular outcome—in this case, the approximate timing of ejaculation. Men with PE—75–95% of them—feel no, little, or “poor” control over the timing of ejaculation during intercourse, compared with only around 5% of men without PE [6,7,8]. The central role for ejaculatory control in the characterization of PE was initially demonstrated through path analysis, where perceived control over ejaculation—in contrast with EL—had significant direct effects on both sexual satisfaction and personal distress related to the PE condition [9]. This construct subsequently emerged as the most important explanatory variable in nearly every model predicting PE status [6,7,8,9], and its centrality with respect to distress, PE severity, sexual satisfaction, and, equally important, clinical assessment and treatment, has been confirmed by a number of recent investigations and reports on the topic [10,11,12,13].
1.2. The Role of Bother/Distress
Both ISSM and APA definitions of PE assume some type of functional impairment which causes bother/distress or a negative outcome for the man, his partner, or their relationship. A high percentage of men with PE report at least “moderate” personal distress related to their condition [8,9]. Indeed, when assessed with standardized psychological instruments, men with PE view their problem as distressful as men with erectile dysfunction (ED) [14]. PE also affects men’s partners and relationships: nearly two-thirds of men with PE avoid discussing their problem with their partner, and half worry about their inability to satisfy their partner [14,15,16,17,18]. Furthermore, the man’s focus on performance, along with diminished intimacy and partner attention, may result in significant distress for the female partner, with over 20% reporting relationship break-ups as a result [19]. Even non-partnered men are affected, often reporting reluctance to establish new relationships due to their PE.
Various analyses have demonstrated that all three criteria for PE—EL, ejaculatory control, and bother/distress—correlate significantly with one another, although these correlations tend to be low-to-moderate, around 0.20 to 0.50 [8,9,11,12,13,14,15,16]. While such correlations indicate the relative independence of these measures [15,19], they also indicate that substantial variation in these variables is due to other (unassessed) variables or, equally plausible, to the non-linear or non-monotonic nature of their relationships [11,16,20]. Specifically, non-linear and/or non-monotonic relationships would typically diminish the value of Pearson r, which assumes linearity between variables. The Pearson r has sometimes been used as a measure of association between these variables.
1.3. Rationale and Aims
Why the need for further investigation of the relationships among ejaculatory control, bother/distress, and EL? In short, because important questions about these constructs remain unanswered. First, in view of the relatively low to moderate correlations among measures, more precise delineation of the relationships between variables (beyond simple correlation values) needs to be specified within both the overall and PE populations. Second, the constructs of ejaculatory control and bother/distress have not been extensively investigated in non-heterosexual men, in men with acquired PE, or in partners of men with PE.
In this reexamination of the PE criteria, we pursued four goals. (1) To further specify the relationships among ejaculatory control, bother/distress, and estimated EL in terms of monotonicity and linearity in both the overall and PE populations. (2) To compare ejaculatory control and bother/distress across men with different sexual orientations and PE status (i.e., with or without PE), and (3) across men with different PE subtypes (i.e., lifelong vs. acquired PE). Finally (4), to determine the importance of (lack of) ejaculatory control to men’s sexual partners as well its potential role in sexual relationship dissatisfaction/termination.
2. Method
2.1. Participants
Participants were recruited via paid and non-paid listings on Reddit and Facebook, with postings of the survey link on subreddit forums (r/askmen, r/askwomen, etc.). To optimize exposure, paid Reddit Ads campaigns targeted these forums. A similar approach was used for Facebook, with the survey link posted in conjunction with a Facebook Ads campaign on the personal Facebook page of one of the authors. Both Reddit and Facebook Ads campaigns targeted worldwide participants who used Facebook or Reddit in English.
To provide an incentive, respondents were offered the possibility for a giveaway by linking to an independent webpage (onlinesexsurveys.com) where they could win a USD 50 prepaid credit card; no link existed between respondents’ data and the link for the giveaway. Finally, to complement social media recruitment, 100 additional respondents were identified through Amazon Mechanical Turk, a service that engages participants in simple tasks, including answering surveys, in exchange for monetary compensation (USD 1) (Table 1 lists recruitment strategies and yields). To guard against random replies among participants, responses to several questions related to EL were checked for extreme outliers or nonsensical answers (see below). In addition, cookie-based safeguards were used to avoid multiple survey submissions from the same participant (for details, see Appendix A: Document on Social Media Recruiting and Controls).
The preliminary sample consisted of 1121 participants. Those who did not meet the inclusion criteria of appropriate age and consent, did not provide a full complement of data, identified themselves as “asexual” or “lesbian,” or responded 3 SD over the mean on an item querying about “typical ejaculatory latency” (see Data Cleaning and Analytical Strategy section for rationale) were excluded from the analysis. Included in the final sample were 1071 respondents, 572 men and 499 women. The sample included men who identified as straight (n = 398), gay (n = 56), bisexual (n = 108), pansexual (n = 3), and other (n = 7), as well as men who identified as having PE (n = 154), not having PE (n = 321), or not sure (n = 97).
2.2. Measures
This analysis was part of a more extensive survey designed to address multiple questions regarding sexual response and PE, with other analyses focusing on issues related to ejaculatory latency [21] and worldwide similarities and differences in ejaculatory latency, control, and bother/distress [22]. Only the outcome measures and group/organizing variables used in this analysis are included here.
2.2.1. Outcome Measures
Ejaculation Latency (EL): Respondents estimated (in minutes and/or fractions thereof) their SELF-EL, based on the following question: Excluding foreplay, estimate how long you last on average before ejaculating after you penetrate your partner (e.g., vaginal or anal penetration). If you don’t have a partner, please leave this question blank. Estimated latencies have been used interchangeably with stopwatch measured ELs [23,24].
Ejaculatory Control: Male participants responded to three questions regarding ejaculatory control. (1) How difficult is it for you to control the general timing of your ejaculation during intercourse? (1 = very easy, 5 = very difficult). (2) Is your ability to control the approximate timing of your ejaculation important for you? (1= extremely important, 5 = not at all important). (3) Which of the following statements best describes your situation (asked only of participants with partners)? (a) I would like to last longer when having sex with my partner, (b) I’m satisfied with how long I last when having sex with my partner, or (c) I would like to ejaculate sooner when having sex with my partner. The first question above was based on one included in the Premature Ejaculation Diagnostic Tool (PEDT), a validated instrument for assessing PE [25].
Ejaculatory Control, Partner Perspective: Men who have sex with men (MSM) and women who have sex with men (WSM)—that is, male and female sexual partners of men—were asked two questions regarding ejaculatory control. (1) Is your partner’s ability to control his ejaculation timing important for you? (1 = extremely important, 5 = not at all important). (2) If your partner always ejaculates within about one minute of penetration, would this be a deal-breaker for a long-term relationship with you? A set of ordered response options (from large effect to no effect) were possible: (a) Yes, I can’t be with a man that can’t last over one minute; (b) By itself, it’s not a deal breaker but it can be a factor; (c) If other than penetration time our sex life is satisfying, then it doesn’t matter; (d) No, it doesn’t matter.
Bother/distress: Participants were asked two questions about bother/distress: (1) If you ejaculate very quickly when having sex with your partner, does this bother, annoy, or upset you? (1 = I never ejaculate quickly during sex with my partner, 2 = not at all, 7 = very much). (2) If you feel that you cannot have some control over when you ejaculate, does this bother, annoy, or upset you? (1 = I always feel in control over when I ejaculate, 2 = not at all, 6 = very much). These questions were based on ones used in the PEDT, a validated instrument for assessing PE [25], and the Premature Ejaculation Profile (PEP), also validated for assessing PE [9].
2.2.2. Input/Defining Variables
Four categorizing variables were included: (1) sex of the respondent; (2) sexual orientation of the respondent; (3) PE or non-PE status; and (4) if self-identified as having PE, the onset/duration of the PE, with response options as follows: (a) All of my sex life, as far back as I can recall, (lifelong) (b) Most of my sex life, (c) Beginning with the past several months or years, (acquired) (d) I’m not sure or I don’t know. For this last set of categorizations, we were interested in comparing “lifelong” and “acquired” groupings.
2.2.3. Control Covariates
Three control covariates were included in the analyses: age, estimated number of lifetime sexual partners (1 = none, 2 = <5, 3 = 6–10, 4 = 11–20, 5 = probably > 20), and “importance of sex within your relationship” (1 = extremely important, 5 = not at all important). The first two covariates also stood as general proxies for sexual experience.
2.3. Procedure
The 22-item anonymous online survey, as approved by the Institutional Review Board (IRB number: 19-001) of the author’s university, took around 10–15 min. Participation occurred through self-selection (opt-in), was voluntary, and was conducted through an individual online portal, with age and informed consent required before receiving access to the survey. Participants could end participation at any time by closing the webpage.
2.4. Data Cleaning and Analytical Strategy
To eliminate extreme outliers that suggested measurement error (or lack of attention by the respondent) in EL estimation (e.g., inability to ascertain whether the respondent had answered in seconds rather than minutes, for example, indicating a typical EL of over 50, values lying 3 or more standard deviations above the mean were excluded from the analysis (n = 16, 1.46% of respondents) [26]. Group comparisons were made with ANCOVA. Non-parametric measures of association or comparison were used when data were skewed. Due to the number of comparisons, alpha was set at 0.01.
3. Results
3.1. General Description of the Sample and Subsamples
Table 2 provides respondents’ country of origin, showing participation over a wide range of countries. Table 3 indicates characteristics of sample subpopulations, including group size, relationship status, estimated number of lifetime partners, and self-reported importance of sex. Briefly, groups differed significantly (p < 0.01) on only three measures. Non-straight men were slightly younger than straight men, and compared with men, women reported fewer lifetime sexual partners and were more likely to be in a relationship.
3.2. Aim 1: Relationships among Ejaculatory Control, Bother/Distress, and ELT
Two approaches were taken to address the nature of the relationships among the three defining variables for PE (EL, ejaculatory control, and bother/distress). First, we ran correlations among them. Second, using the ordered response categories for both ejaculatory control and bother/distress, we generated average ratings for the other variables based on each response category.
3.2.1. Correlations
Spearman correlations among the three measures were significant but generally small. For the overall sample, ejaculatory control difficulty and bother/distress were correlated at 0.30 (p < 0.001): as control difficulty increased, bother/distress also increased. Correlations between EL and the other two variables, ejaculatory control difficulty and bother/distress, were 0.23 and −0.24 (p < 0.001, respectively): as ejaculatory latency decreased, control also decreased and bother/distress increased.
Relationships were also examined in PE and non-PE men separately. For PE men, ejaculatory control difficulty and bother/distress correlated at 0.34 (p < 0.001). For non-PE men, ejaculatory control difficulty and bother/distress correlated at 0.21 (p < 0.001). EL did not correlate significantly with either measure for either PE or non-PE subgroups.
3.2.2. Patterns of Change
To characterize monotonicity and linearity between ejaculatory control and bother/distress, we determined (1) how incremental increases in the question related to ejaculatory control corresponded to changes in the question related to bother/distress, and (2) how incremental increases in the question related to bother/distress corresponded to changes in the question related to ejaculatory control.
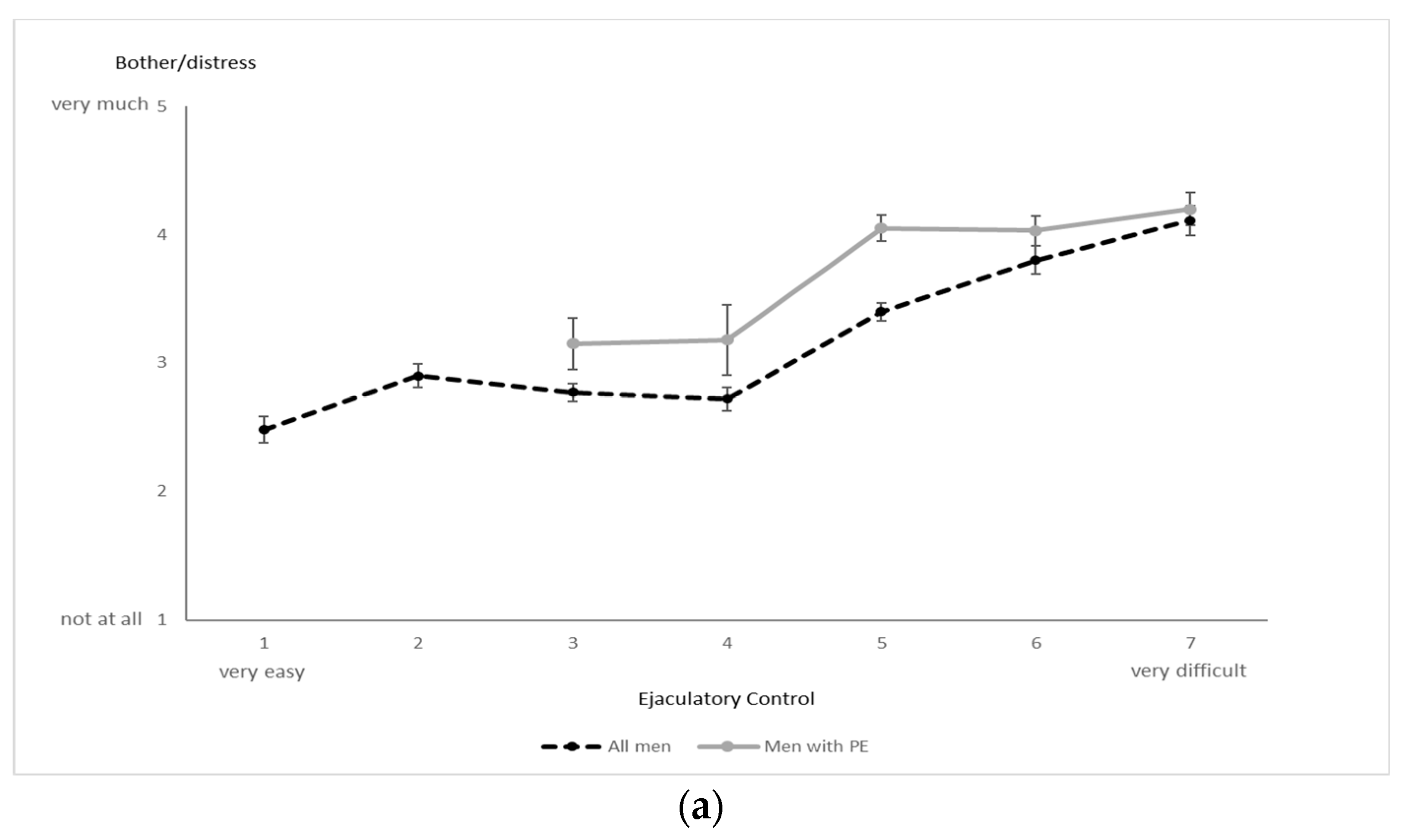
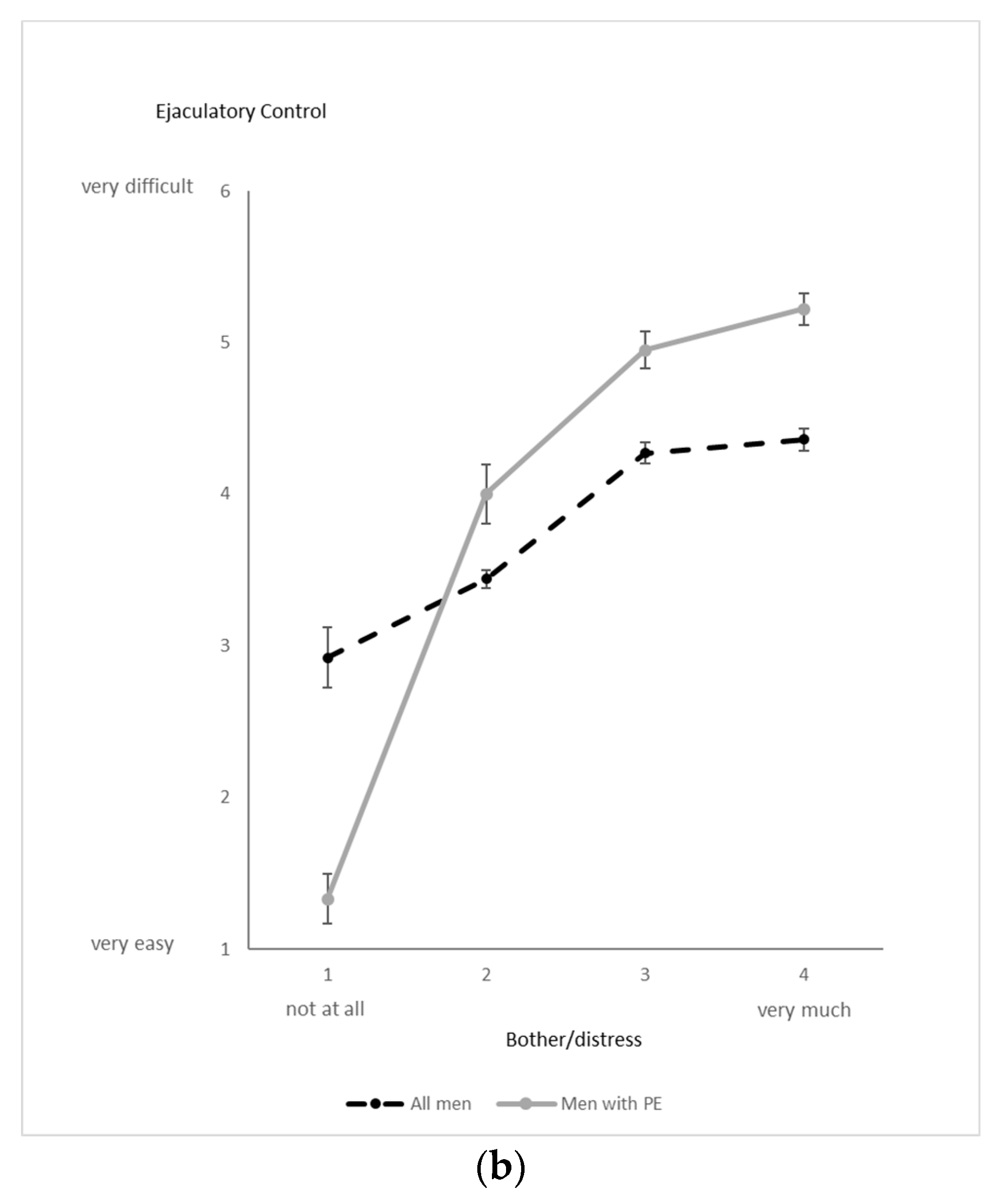
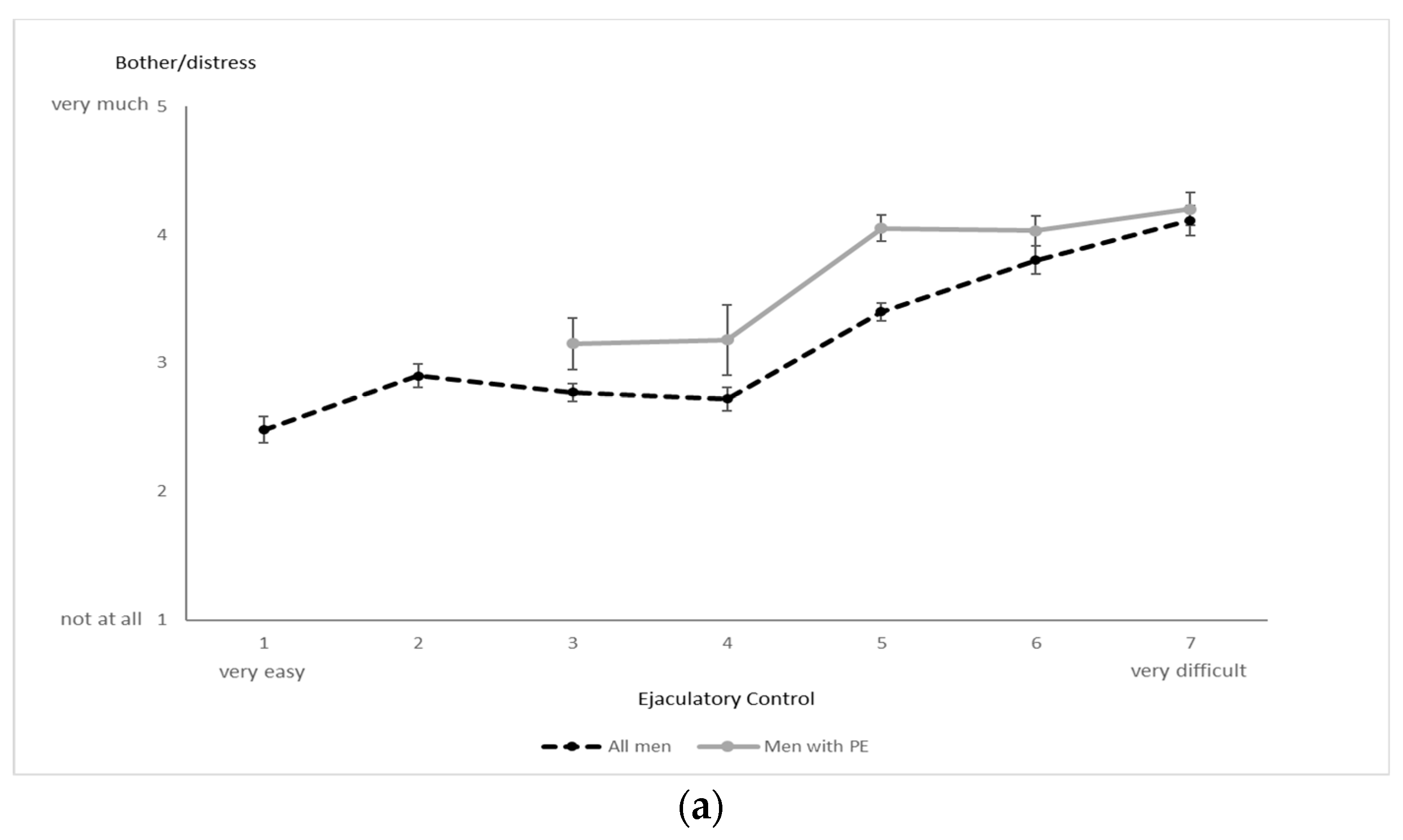
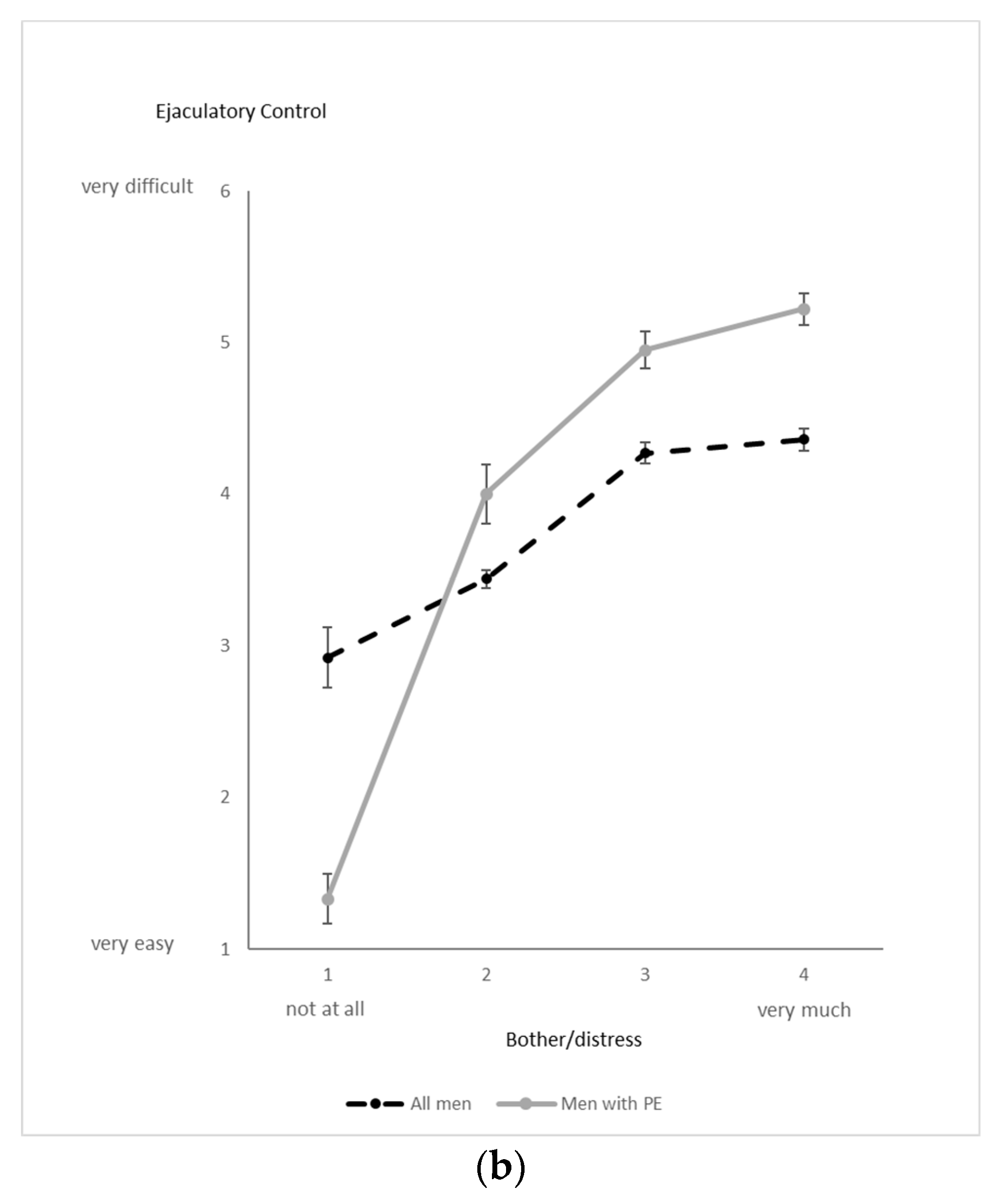
When ejaculatory control was used as the anchor variable (Figure 1a: the “x” axis), the relationship with bother/distress was generally monotonic but mildly curvilinear in both the overall and PE subsamples; most of the increase in bother/distress occurred only when ejaculatory control difficulty transitioned out of the “easy” range and into the “difficult” range. When the level of bother/distress was used as the anchor question (Figure 1b), its relationship with ejaculatory control difficulty was monotonic and, again, slightly curvilinear, with transition to the highest levels of bother/distress resulting in a moderate flattening of the ejaculatory control slope.
3.3. Aim 2: PE Status (PE vs. Non-PE) and Sexual Orientation Comparisons on Control and Bother/Distress
3.3.1. PE vs. Non-PE Men
Consistent with the PE definition, ANCOVA revealed that men with PE reported greater ejaculatory control difficulty and greater importance of ejaculatory control than non-PE counterparts (p < 0.001 for each). These men also indicated greater bother/distress related to both ejaculating quickly and not having control over ejaculation (p < 0.001 for each). Consistent with this pattern, 86% of men with PE indicated the desire to last longer during partnered sex, whereas only 37% of men without PE indicated such desire (χ2 = 96.2, p < 0.001).
3.3.2. Sexual Orientation
A second set of ANCOVAs compared ejaculatory control and bother/distress across men of different sexual orientations. For an initial analysis, non-straight men (gay, bisexual, pansexual) were combined to form a single group due to the relatively limited numbers in subgroups. For the overall sample of men, straight and non-straight groups did not differ significantly on either measure of ejaculatory control (difficulty or importance), or on either measure of bother/distress (related to short latency or lack of control) (p = 0.131, 0.068, 0.412, and 0.051, respectively) (Table 4).
When only the subset of men with PE was analyzed, ejaculatory control difficulty (but not importance) was marginally greater in straight men (p = 0.015, p = 0.770, respectively). Neither bother/distress measure showed group differences (p = 0.374, 0.061). Straight and non-straight men with PE also did not differ with respect to their desired ejaculatory latency, i.e., wanting to last longer, satisfied with where they were, or wanting ejaculate sooner (χ2 = 5.24, p = 0.073).
In a follow-up analysis (Table 4), straight men were compared just with gay men. Gay men indicated less importance regarding ejaculatory control (p < 0.001) and less bother/distress regarding not having control (p < 0.001) than straight men.
3.3.3. Covariates
For group comparisons involving PE vs. non-PE men and straight vs. non-straight men, the importance of sex within the relationship emerged as a significant covariate; generally, the greater the importance of sex, the greater the distress about not having ejaculatory control (p < 0.01), and the greater the importance of having ejaculatory control (p < 0.001). Neither age nor estimated number of sexual partners was significant.
3.4. Aim 3: Comparison of Men with Lifelong vs. Acquired PE
Men who reported that their PE was a lifelong condition (“all my sex life, as far as I can remember”) were compared with men who reported more recently acquired PE (“began within the past several months or years”). No differences were found on either measure of ejaculatory control (difficulty or importance), on either bother/distress item, or on SELF-EL (Table 5). When analysis was rerun to include an intermediary group that indicated PE as occurring “most of my sex life”—that is, between lifelong and acquired—again, no significant group differences emerged. None of the covariates, including those standing as proxies for sexual experience, was significant.
3.5. Aim 4: Partner Response Regarding Ejaculatory Control during Partnered Sex
Respondents who had sex with men (MSM and WSM) were asked about the importance of ejaculatory control during partnered sex. The average importance of control fell between “somewhat” and “very” important, with WSM reporting greater importance than MSM (p < 0.001). Furthermore, nearly 60% of women and 56% of men considered ejaculation occurring ≤ 1 min to be either a “potential” or “definite” reason for ending a relationship, with women showing the greater likelihood (p = 0.022) (see Table 6 for details). For this last item, both the number of lifetime partners and the self-reported “importance of sex” emerged as significant covariates. As each increased, the greater was the likelihood of ending the relationship (p < 0.001 for each).
4. Discussion
This study has (1) provided a clearer characterization of the relationship between ejaculatory control and bother/distress; (2) reiterated the large differences in these measures between men with and without PE; (3) demonstrated that although straight and non-straight men do not differ in their understanding/assessment of ejaculatory control and bother/distress, straight and gay men do differ on the importance of ejaculatory control; (4) shown that men with lifelong PE do not differ from men with acquired PE in their assessment of ejaculatory control or bother/distress; and (5) elaborated on the partner’s perspective regarding the detrimental effects of PE on the dyadic relationship.
4.1. Overall Sample Patterns
Reported correlations between ejaculatory control and bother/distress have ranged from low to moderate [9,11,12,20]. Results from the current study also show low to moderate correlations, with similar values for both the overall sample and the PE subsample. When illustrated graphically, these relationships were generally monotonic though slightly curvilinear. The nature of this relationship between these two variables depends, to some extent, on the wording used to assess each of the constructs. For example, had we limited our response options for ejaculatory control to only the “difficult” end of the spectrum (eliminating the “easy” response options), the relationship would have shown greater linearity (see Figure 1a,b). Moreover, with greater linearity, Pearson correlation values typically increase, perhaps explaining the range of correlations reported across various studies. Such findings indicate the need to rely on precisely worded standardized questions such as the one provided in the PEDT [25], which assesses the “difficulty” of delaying ejaculation, with response options ranging from “not at all” to “extremely difficult”.
4.2. Patterns in Men with and without PE and in Men with Different Sexual Orientations
As expected, men with PE showed higher ejaculatory control difficulty and greater bother/distress than non-PE men. The great majority of men with PE (86%) also reported the desire to last longer during partnered sex. Even so, 37% of men without PE desired this same outcome, a finding consistent with previous analyses in which estimations of the ideal EL in a sample of men were consistently longer than estimations of the typical EL, usually by around 5–7 min [21,22]. The longer ideal vs. typical EL in that study, and the general desire to last longer in the current study by both PE and non-PE men, suggest that many men, even those with normal-range ELs, see benefit to either themselves or their partners (or both) in being able to prolong sexual intercourse. Such findings caution against using broadly worded questions about “wanting to last longer” as an indication of premature ejaculation and reiterate the critical importance of assessing ejaculatory control and bother/distress as part of the PE diagnostic process.
Another new finding from this analysis is that non-straight men were not different from straight men in their assessments of either ejaculatory control (difficulty and importance) or bother/distress (about ejaculating quickly and about not having control). In addition, for the subset of men with PE, only one of the four items (ejaculatory control difficulty) related to ejaculatory control and bother/distress differed between straight and non-straight men. In contrast, in a post hoc analysis comparing straight men with just gay men, gay men reported significantly lower importance of ejaculatory control and less bother/distress about not having control. These findings suggest that ejaculatory control may be less concerning to gay couples, where a short EL during anal penetration (as well as during oral sex) may have less or no bearing on the partner’s capacity to reach orgasm, quite different from heterosexual couples engaging primarily in penile–vaginal intercourse.
The ISSM and APA criteria for PE—originally derived from data based on heterosexual intercourse [1,2,3]—have general applicability to gay and non-straight men in terms of ELs, as self-estimated ELs for straight, non-straight, and gay men do not differ (whether or not they have PE) [22]. However, bother/concern about (lack of) ejaculatory control may be less of an issue for gay men, where rapid ejaculation may impact sexual satisfaction less. Such findings need to be further explored and/or replicated in community samples comparing ejaculatory control and bother/distress in gay and straight men.
4.3. Lifelong and Acquired PE
ISSM distinguishes between lifelong and acquired PE in terms of both etiology and EL [3]. In contrast, neither the DSM nor International Classification of Diseases (ICD-11) definition of PE makes this distinction [2,27], indicating inconsistency in the approaches to PE by these professional standards. Although lifelong and acquired PE subtypes may have different etiologies, our results suggest that the symptomologies may not be different. Specifically, together with other recent research indicating similarities between men with lifelong and acquired PE [28], our study has shown that these groups do not differ in either their (lack of) control over ejaculation or their level of PE-related distress. In addition, self-reported ELs do differ between men with lifelong and acquired PE [22], generally around 1.5 min for both groups.
Such findings question whether, specifically, the distinction of the 1-min vs. 3-min thresholds (for lifelong vs. acquired PE) suggested by the ISSM definitions should be reconsidered, and perhaps more generally, whether the differentiation between men with lifelong and acquired PE has been overestimated. One approach might consider extending the latency criterion for any type of PE to 2 min [22]. This suggestion is supported by a number of other studies investigating ELs in men with PE, often reporting median latencies in the 1.5–2.5 min range, e.g., [9,10,29]. Furthermore, now, even the appropriateness of the “lifelong” subtype is being questioned, with one longitudinal study demonstrating that men with untreated (presumably lifelong) PE varied by several minutes or more in their ELs over a 6-year period [30]. Indeed, data from the current study indicated that 25% of the men with PE indicated a duration of “most of their sex life,” as opposed to lifelong (“all of my sex life…”) or acquired (“only recently”), and 10% responded “unsure or did not know.” That is, within our sample of 153 men with PE, some 35% did not fall into the standard classifications of lifelong or acquired.
4.4. Partner Response to Poor Ejaculatory Control and Short Ejaculatory Latency
A number of studies have documented the negative effects that PE has on the partner and relationship [8,14,17,18,19], a point strongly reiterated in this study. Ejaculatory control during partnered sex was considered somewhat to very important to the majority of male and female partners of men. Female partners deemed ejaculatory control more important than male partners, and female partners were more likely than male partners to consider ending a long-term relationship if the man’s EL was consistently less than 1 min, a finding that showed consistency when analyses were focused on similarities and differences across various world regions [21]. These findings indicate that ejaculatory control and adequate ELs are important to the partner’s sexual satisfaction [14,17], and even more so for women partners who likely rely on clitoral and vaginal stimulation during intercourse to become sufficiently aroused to reach orgasm. The importance of ejaculatory control for the partner increased with the partner’s sexual experience, as measured by his/her age and number of sexual partners. Given such findings, it is not surprising that men with PE worry about the impact of their rapid ejaculation on their relationship, and that non-partnered men with PE feel anxiety and hesitation about pursuing a new sexual relationship [14,16,17,18].
4.5. Strengths and Limitations
Our study included the benefits common to many online surveys [31,32], including a large, globally diverse sample that included men of varying sexual orientations, PE status, and PE subtypes. Furthermore, the anonymity afforded through an Internet approach likely reduced social desirability and improved openness in responding, which are essential when dealing with sensitive topics related to sexual experiences [33]. Control over submission of multiple surveys by participants and attention checks further increased confidence in the results of the study.
We also recognize the study’s limitations, including self-identification of men with and without PE (vs. a clinical diagnosis). Given that recruitment relied heavily on social media (internet) and that 9% of the sample was eligible for a monetary incentive of USD 1, sample characteristics and motivations may have affected the results and therefore generalization to the population at large requires caution. Regarding this point, however, we note that in examining the characteristics of this 9% subsample, patterns of sexual responding did not differ significantly from those of other participants. In addition, we did not specifically assess men on ejaculatory control and bother/distress who might have had both PE and erectile dysfunction, a fairly common subgroup that has generally been understudied and may not conform to the patterns demonstrated in this analysis. Nor did we extract men with delayed ejaculation from the group of non-PE men; thus, the group of non-PE men may have included some men with other types of sexual problems such as erectile dysfunction and delayed ejaculation, and we did not control for these effects. Future studies need to replicate our findings in community samples drawing more participants from PE subgroups and from wider socioeconomic and age groups; they might also benefit from controlling for the presence of other sexual dysfunctions in men.
5. Conclusions
Ejaculatory control and bother/distress are widely used criteria in the diagnosis of PE. These two variables are moderately correlated and exhibit a slightly curvilinear (though monotonic) relationship. Straight and non-straight men differed only minimally on these constructs, but straight and gay men showed differences on ejaculatory control importance and bother/distress related to lack of ejaculatory control, suggesting that ejaculatory control may be less important for gay couples where (anal) penetration and/or oral sex is less tied to the partner’s orgasm (compared to vaginal penetration in heterosexual couples). No differences in these constructs emerged between men with lifelong PE vs. men with acquired PE.
Author Contributions
Project development: D.L.R. and P.C.-L.; data collection: P.C.-L. and D.L.R.; data analysis: D.L.R.; writing and editing: D.L.R. and P.C.-L.; final approval: D.L.R. and P.C.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
D.L.R. reports no conflict of interest. P.C.-L. notes the following: Philippe Côté-Léger is the owner of Premature Ejaculation Help, a self-help website. As a participant in different affiliate programs, Premature Ejaculation Help can earn a commission on certain product sales generated via links placed on its website. Participants were not referred to the website during the study, but the website was mentioned as the sponsor of the giveaway on the consent page.
Appendix A. Document on Social Media Recruiting and Controls
It is important to understand the advantages and limitations of recruiting through social media. We note that the only targeting criterion for our ads used on Facebook and Reddit was that of English language, the major reason that comparatively few respondents were from East Asia. However, given the way in which social media advertising works, the ads are shown to those who are most likely to click on them. Therefore, the ads are exposed more to people with specific interests. For example, if Facebook saw that people who like content about subject X click more on our ads, other people that engaged with content about subject X will be more likely to be exposed to our ads. For non-paid impressions, the same strategy applies. Most social media use an algorithm that shows posts to people who are more likely to engage with the post. The platform calculates an “engagement likeliness” based on previous content that the person engaged with. This system also acts as a limitation of social media recruiting.
Since we targeted English-speaking users of specific social media, our country distribution is uneven, drawing more heavily from English-speaking regions of the world. In addition, some regions are more represented than others because regions use different social media than Facebook or Reddit or use social media in their native (non-English) language. We intentionally limited our ads to English users to circumvent the problems often encountered in semantic challenges resulting from translation, providing reasonable assurance that questions were being interpreted correctly.
For the above reasons, it is not surprising that some regions like East Asia are underrepresented. For example, since Facebook is available in both Korean and Japanese, people in these countries use it primarily in their native language. In contrast, in many sub-Saharan countries, a large percentage of the population uses social media in English (a British legacy). Not only are many of them English native or second speakers, but in these countries, Facebook is often not available in their native language; therefore, they use the English version.
In some world regions, Facebook has less market share due to local competition. For example, Russia is underrepresented in our sample, partly because Facebook has a significant competitor, VK (B Kohtakte), here. In Japan, “Line” is used as a replacement for Facebook products, limiting the available ad inventory for this country. When added to the fact that most Japanese Facebook users do so in their native language, recruitment from these countries faces significant barriers. Finally, Facebook and Reddit are both censored in mainland China, which represents a large percentage of the East Asian population. Even within other regions, there is a disparity. For example, in the sub-Saharan region, most respondents come from countries with a tradition of English language use, such as Nigeria and Kenya.
Cookie-based safeguards were implemented to prevent individuals from taking the survey more than once. Specifically, we deactivated the option to store IP addresses of respondents to honor the promise of disabling any linkage between survey responses and personal data required for the opt-in incentive gift card—this general approach to ensure anonymity is also suggested by the EU’s General Data Protection Regulation. However, the tool that we used (Survey Monkey) allows participants to access the survey only once, using cookies to recognize whether someone had already taken the survey. Therefore, respondents could not attempt the survey a second time using the same browser. Since cookies are browser-dependent, a respondent could circumvent this safeguard by using a different browser (switching from Chrome to Safari) or a different device (computer vs. phone). Thus, although the safeguard is not 100% effective, an individual wanting to circumvent the safeguard would require a clear understanding of how cookies function and take deliberate steps to circumvent them.
References
- McMahon, C.G.; Althof, S.; Waldinger, M.D.; Porst, H.; Dean, J.; Sharlip, I.; Adaikan, P.G.; Becher, E.; Broderick, G.A.; Buvat, J.; et al. An evidence-based definition of lifelong premature ejaculation: Report of the International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. BJU Int. 2008, 102, 338–350. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Serefoglu, E.C.; McMahon, C.G.; Waldinger, M.D.; Althof, S.E.; Shindel, A.; Adaikan, G.; Becher, E.F.; Dean, J.; Giuliano, F.; Hellstrom, W.J.; et al. An evidence-based unified definition of lifelong and acquired premature ejaculation: Report of the second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014, 2, 41–59. [Google Scholar] [CrossRef] [Green Version]
- Dinsmore, W.W.; Wyllie, M.G. PSD502 improves ejaculatory latency, control and sexual satisfaction when applied topically 5 min before intercourse in men with premature ejaculation: Results of a phase III, multicentre, double-blind, placebo-controlled study. BJU Int. 2009, 103, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Buvat, J.; Tesfaye, F.; Rothman, M.; Rivas, D.A.; Giuliano, F. Dapoxetine for the treatment of premature ejaculation: Results from a randomized, double-blind, placebo-controlled phase 3 trial in 22 countries. Eur. Urol. 2009, 55, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, R.; Rowland, D. The Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision as an appropriate diagnostic for premature ejaculation. J. Sex. Med. 2007, 4, 1468–1478. [Google Scholar] [CrossRef] [PubMed]
- Waldinger, M.; McIntosh, J.; Schweitzer, D.H. A five-nation survey to assess the distribution of the intravaginal ejaculation time among the general male population. J. Sex. Med. 2009, 6, 2888–2895. [Google Scholar] [CrossRef]
- Patrick, D.; Althof, S.; Pryor, J.; Rosen, R.; Rowland, D.; Ho, K.; McNulty, P.; Rothman, M.; Jamieson, C. Premature ejaculation: An observational study of men and their partners. J. Sex. Med. 2005, 2, 358–367. [Google Scholar] [CrossRef]
- Patrick, D.A.; Rowland, D.L.; Rothman, M. Interrelationship among measures of premature ejaculation: The central role of perceived control over ejaculation. J. Sex. Med. 2007, 4, 780–788. [Google Scholar] [CrossRef]
- Rowland, D.L.; Kolba, T.N. Understanding the effects of establishing various cut-off criteria in the definition of men with premature ejaculation. J. Sex. Med. 2015, 12, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Jern, P.; Gunst, A.; Sandqvist, F.; Sandnabba, N.K.; Santtila, P. Using ecological momentary assessment to investigate associations between ejaculatory latency and control in partnered and non-partnered sexual activities. J. Sex. Res. 2011, 48, 316–324. [Google Scholar] [CrossRef]
- Gao, J.; Zhang, X.; Su, P.; Shi, K.; Tang, D.; Hao, Z.; Zhou, J.; Liang, C. Prevalence and impact of premature ejaculation in outpatients complaining of ejaculating prematurely: Using the instruments of intravaginal ejaculatory latency time and patient-reported outcome measures. Int. J. Impot. Res. 2014, 26, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Sansone, A.; Aversa, A.; Corona, G.; Fisher, A.D.; Isidori, A.M.; La Vignera, S.; Limoncin, E.; Maggi, M.; Merico, M.; Jannini, E.A. Management of premature ejaculation: A clinical guideline from the Italian Society of Andrology and Sexual Medicine (SIAMS). J. Endocrinol. Investig. 2020. [Google Scholar] [CrossRef] [PubMed]
- Rowland, D.L.; Patrick, D.L.; Rothman, M.; Gagnon, D.D. The psychological burden of premature ejaculation. J. Urol. 2007, 177, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Rowland, D.; Perelman, M.; Althof, S.; Barada, J.; McCullough, A.; Bull, S.; Jamieson, C.; Ho, K.F. Self-reported premature ejaculation and aspects of sexual functioning and satisfaction. J. Sex. Med. 2004, 1, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Grenier, G.; Byers, E.S. The relationships among ejaculatory control, ejaculatory latency, and attempts to prolong heterosexual intercourse. Arch. Sex. Behav. 1997, 26, 27–47. [Google Scholar] [CrossRef]
- Rosen, R.C.; Althof, S. Impact of premature ejaculation: The psychological, quality of life, and sexual relationship consequences. J. Sex. Med. 2008, 5, 1296–1307. [Google Scholar] [CrossRef]
- Revicki, D.; Howard, K.; Hanlon, J.; Mannix, S.; Greene, A.; Rothman, M. Characterizing the burden of premature ejaculation from a patient and partner perspective: A multi-country qualitative analysis. Health Qual. Life Outcomes 2008, 6. [Google Scholar] [CrossRef] [Green Version]
- Burri, A.; Giuliano, F.; McMahon, C.; Porst, H. Female partner’s perception of premature ejaculation and its impact on relationship breakups, relationship quality, and sexual satisfaction. J. Sex. Med. 2014, 11, 2243–2255. [Google Scholar] [CrossRef]
- Rowland, D.L.; Strassberg, D.S.; de Gouveia Brazao, C.A.; Slob, A.K. Ejaculatory latency and control in men with premature ejaculation: An analysis across sexual activities using multiple sources of information. J. Psychosom. Res. 2000, 48, 69–77. [Google Scholar] [CrossRef]
- Cote-Leger, P.; Rowland, D.L. Global perspectives on the three criteria for premature ejaculation: An observational study of ejaculatory latency, ejaculatory control and bother/distress. Andrologia 2020, 52. [Google Scholar] [CrossRef]
- Côté-Léger, P.; Rowland, D.L. Estimations of typical, ideal, premature ejaculation, and actual latencies by men and female sexual partners of men during partnered sex. J. Sex. Med. 2020, 17, 1448–1456. [Google Scholar] [CrossRef]
- Rosen, R.C.; McMahon, C.G.; Niederberger, C.; Broderick, G.A.; Jamieson, C.; Gagnon, D.D. Correlates to the clinical diagnosis of premature ejaculation: Results from a large observational study of men and their partners. J. Urol. 2007, 177, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.K.; Cho, S.T.; Lee, Y.S.; Lee, Y.G.; Oh, C.Y.; Yoo, C.; Cho, J.S.; Shin, T.Y.; Lee, S.K.; Lee, S.H.; et al. Can estimated intravaginal ejaculatory latency time be used interchangeably with stopwatch-measured intravaginal ejaculatory latency time for the diagnosis of lifelong premature ejaculation? Urology 2015, 85, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Symonds, T.; Perelman, M.; Althof, S.; Giuliano, F.; Martin, M.; Abraham, L.; Crossland, A.; Morris, M.; May, K. Further evidence of the reliability and validity of the premature ejaculation diagnostic tool. Int. J. Impot. Res. 2007, 19, 521–525. [Google Scholar] [CrossRef] [Green Version]
- Siddharth, K. Statistical Outliers. 2009. Available online: https://explorable.com/statistical-outliers (accessed on 18 March 2020).
- International Classification of Diseases, 11th Revision. World Health Organization. Available online: https://www.who.int/classifications/icd/en/ (accessed on 12 October 2020).
- Kempeneers, P.; Andrianne, R.; Cuddy, M.; Blairy, S. Sexual cognitions, trait anxiety, sexual anxiety, and distress in men with different subtypes of premature ejaculation and in their partners. J. Sex. Marital Ther. 2017, 44, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, U.; Schedlowski, M.; Krüger, T.H.C. Cognitive and partner-related factors in rapid ejaculation: Differences between dysfunctional and functional men. World J. Urol. 2005, 23, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ventus, D.; Ristila, M.; Gunst, A.; Karna, A.; Arver, S.; Piha, J.; Jern, P. A longitudinal analysis of premature ejaculation symptoms raises concern regarding the appropriateness of a “Lifelong” subtype. Eur. Urol. Focus 2017, 3, 243–245. [Google Scholar] [CrossRef]
- Catania, J.A.; Dolcini, M.M.; Orellana, R.; Narayanan, V. Non-probability and probability-based sampling strategies in sexual science. J. Sex. Res. 2015, 52, 396–411. [Google Scholar] [CrossRef]
- Manzo, A.N.; Burke, J.M. Increasing response rate in web-based/internet surveys. In Handbook of Survey Methodology for the Social Sciences; Gideon, L., Ed.; Springer: New York, NY, USA, 2012; pp. 327–343. [Google Scholar]
- Ong, A.D.; Weiss, D.J. The impact of anonymity on responses to sensitive questions. J. Appl. Soc. Psychol. 2000, 30, 1691–1708. [Google Scholar] [CrossRef]
Figure 1.
(a) Bother/distress in relation to ejaculatory control; (b) Ejaculatory control in relation to bother/distress.
Figure 1.
(a) Bother/distress in relation to ejaculatory control; (b) Ejaculatory control in relation to bother/distress.

{kind=link}
{kind=link}
Table 1.
General information about the recruitment portal.
| Source | N | % Sample |
|---|---|---|
| Facebook Paid Ads | 626 | 58.07% |
| Giveaway Websites | 136 | 12.62% |
| Amazon Mechanical Turk | 98 | 9.09% |
| Reddit Organic | 98 | 9.09% |
| Reddit Paid Ads | 80 | 7.42% |
| Facebook Organic | 21 | 1.95% |
| Other or Unknown | 19 | 1.76% |
Table 2.
World region origin of participants.
| Region | N | % Sample |
|---|---|---|
| North America | 299 | 27.74% |
| Sub-Saharan Africa | 262 | 24.30% |
| South Asia | 137 | 12.71% |
| Europe | 125 | 11.60% |
| Latin America | 113 | 10.48% |
| Oceania | 86 | 7.98% |
| Middle East | 36 | 3.34% |
| Unknown | 14 | 1.30% |
| East Asia | 4 | 0.37% |
| Central and Western Asia | 2 | 0.19% |
Table 3.
Characteristics of the sample subgroups.
| Group | Men | Women | Men with PE | Men No PE 2 | Straight Men | Non-Straight Men |
|---|---|---|---|---|---|---|
| N | 572 | 499 | 154 | 321 | 398 | 174 |
| Age (mean + SD) | 33.27 (11.92) | 33.61 (11.07) | 34.95 (12.42) | 33.47 (11.78) | 34.35 (12.43) 3 | 30.82 (10.27) |
| Relationship Status 4 | ||||||
| (N and % of group) | ||||||
| Not in a relationship | 164 (28.67%) | 98 (19.84%) | 35 (22.73%) | 88 (27.41%) | 103 (25.88%) | 61 (35.06%) |
| Married | 180 (31.47%) | 159 (32.19%) | 65 (42.21%) | 102 (31.78%) | 143 (35.93%) | 37 (21.26%) |
| Relationship but not married | 209 (36.54%) | 225 (45.54%) | 49 (31.82%) | 122 (38.01%) | 142 (35.68%) | 67 (38.51%) |
| Polyamorous relationship or marriage | 11 (1.92%) | 7 (1.42%) | 4 (2.60%) | 4 (1.25%) | 6 (1.51%) | 5 (2.87%) |
| Other | 8 (1.39%) | 10 (2.02%) | 1 (0.65%) | 5 (1.56%) | 4 (1.01%) | 4 (2.30%) |
| Number (% of total) of Lifetime Sexual Partners 4 | ||||||
| 0 | 36 (6.38%) | 26 (5.23%) | 8 (5.26%) | 9 (2.82%) | 29 (7.29%) | 7 (4.02%) |
| 1 | 110 (19.50%) | 111 (22.33%) | 32 (21.05%) | 64 (20.06%) | 80 (20.10%) | 30 (17.24%) |
| Probably < 5 | 143 (25.35%) | 155 (31.19%) | 42 (27.63%) | 74 (23.20%) | 93 (23.37%) | 50 (28.74%) |
| About 6–10 | 112 (19.86%) | 94 (18.91%) | 34 (22.37%) | 61 (19.12%) | 80 (20.10%) | 32 (18.39%) |
| About 11–20 | 62 (10.99%) | 47 (9.46%) | 12 (7.89%) | 44 (13.79%) | 47 (11.81%) | 15 (8.62%) |
| Probably > 20 | 101 (17.91%) | 64 (12.88%) | 24 (15.79%) | 67 (21.00%) | 63 (15.83%) | 38 (21.84%) |
| Did not answer | 8 (1.40%) | 2 (0.40%) | 2 (1.30%) | 2 (0.62%) | 6 (1.51%) | 2 (1.15%) |
| Importance of Sex in the Relationship (mean + SD) 1 | 3.98 (0.97) | 3.82 (1.00) | 4.16 (0.93) | 4.01 (0.91) | 3.96 (1.00) | 4.03 (0.91) |
1 1 = not at all, 5 = extremely important; 2 Does not include people who answered “I’m not sure” to the question “Would you consider yourself a premature ejaculator?”, 3 p < 0.01 compared with non-straight men, 4 Compared with men, women were more likely to be in a relationship and had fewer lifetime sexual partners (p < 0.01).
Table 4.
Ejaculatory control and bother/distress in straight, non-straight, and gay men for the overall sample and PE subsample.
Table 4.
Ejaculatory control and bother/distress in straight, non-straight, and gay men for the overall sample and PE subsample.
| All Men | Straight Men | Non-Straight Men | p 1 | Gay Men | p 2 |
|---|---|---|---|---|---|
| (N = 321) | (N = 153) | (N = 56) | |||
| Ejaculatory Control Difficulty 3 | 3.8 (0.10) | 3.6 (0.13) | 0.131 | 3.3 (0.19) | 0.017 |
| Ejaculatory Control Importance 4 | 2.1 (0.05) | 2.3 (0.08) | 0.068 | 2.7 (0.14) | <0.001 |
| Bother/distress if ejaculate quickly 5 | 3.1 (0.09) | 2.9 (0.13) | 0.412 | 3.3 (0.23) | 0.096 |
| Bother/distress if cannot have control 5 | 3.4 (0.08) | 3.1 (0.10) | 0.051 | 2.0 (0.19) | <0.001 |
| PE Men Only | Straight Men | Non-Straight Men | p 1 | ||
| (N = 105) | (N = 45) | ||||
| Ejaculatory Control Difficulty 3 | 5.0 (0.17) | 4.2 (0.28) | 0.015 | * | |
| Ejaculatory Control Importance 4 | 1.8 (0.08) | 1.7 (0.11) | 0.770 | * | |
| Bother/distress if ejaculate quickly 5 | 3.8 (0.14) | 3.6 (0.24) | 0.374 | * | |
| Bother/distress if cannot have control 5 | 4.0 (0.13) | 3.6 (0.20) | 0.061 | * |
1 Comparisons of straight and non-straight groups; 2 Comparison of straight and gay men; 3 Higher values represent greater difficulty; 4 Lower values represent greater importance; 5 Higher values represent greater bother/distress; * Sample size too small to analyze.
Table 5.
Comparison of ejaculatory control, distress/bother, and EL across men with “lifelong” and “recently acquired” PE.
Table 5.
Comparison of ejaculatory control, distress/bother, and EL across men with “lifelong” and “recently acquired” PE.
| Variable | Lifelong (N = 64) | Acquired (N = 31) | p 1 |
|---|---|---|---|
| Ejaculatory Control Difficulty 2 | 4.9 (0.24) | 4.9 (0.26) | 0.97 |
| Ejaculatory Control Importance 3 | 1.8 (0.10) | 1.5 (0.12) | 0.16 |
| Distress/bother if ejaculate quickly 4 | 3.7 (0.20) | 3.9 (0.25) | 0.69 |
| Distress/bother if cannot have control 4 | 3.9 (0.17) | 3.9 (0.22) | 0.86 |
| EL (min) 5 | 2.0 (1,5) | 3.0 (1,4) | 0.72 |
1 Comparisons made with ANCOVA unless otherwise noted. 2 Higher values represent greater difficulty; 3 Lower values represent greater importance; 4 Higher values represent greater distress/bother; 5 Medians and Q1, Q3 are reported and compared using the Mann–Whitney test due to the skewed distribution.
Table 6.
Partners’ response regarding men’s ejaculatory control.
| Item | MSM 1 (N = 165) | WSM 2 (N = 499) | p 3 |
|---|---|---|---|
| Importance of partner’s control over timing of ejaculation 4 | 2.90 (0.09) | 2.30 (0.05) | p < 0.001 |
| If ejaculation ≤ 1 min, deal breaker in long-term relationship? | |||
| Yes, definitely | 38 (23.0%) | 110 (22.0%) | p = 0.022 |
| Potential factor | 54 (32.7%) | 189 (37.9%) | |
| Not if otherwise satisfying sex life | 42 (25.5%) | 139 (27.9%) | |
| No, does not matter | 31 (18.8%) | 61 (12.2%) |
1 MSM = Men who have sex with men; 2 WSM = Women who have sex with men; 3 Comparison was made with ANCOVA or, in the case of frequencies, with the chi-square test; 4 Lower value indicates greater importance.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Cote-Leger, P.; Rowland, D.L. Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”. Sexes 2020, 1, 72-86. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes1010007
AMA Style
Cote-Leger P, Rowland DL. Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”. Sexes. 2020; 1(1):72-86. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes1010007
Chicago/Turabian StyleCote-Leger, Philippe, and David L. Rowland. 2020. "Diagnostic Criteria for Premature Ejaculation: Clarifying the Role of “Ejaculatory Control” and “Bother/Distress”" Sexes 1, no. 1: 72-86. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes1010007