Endocrine Management of Transgender Adults: A Clinical Approach

 ,
,  ,
, 
Abstract
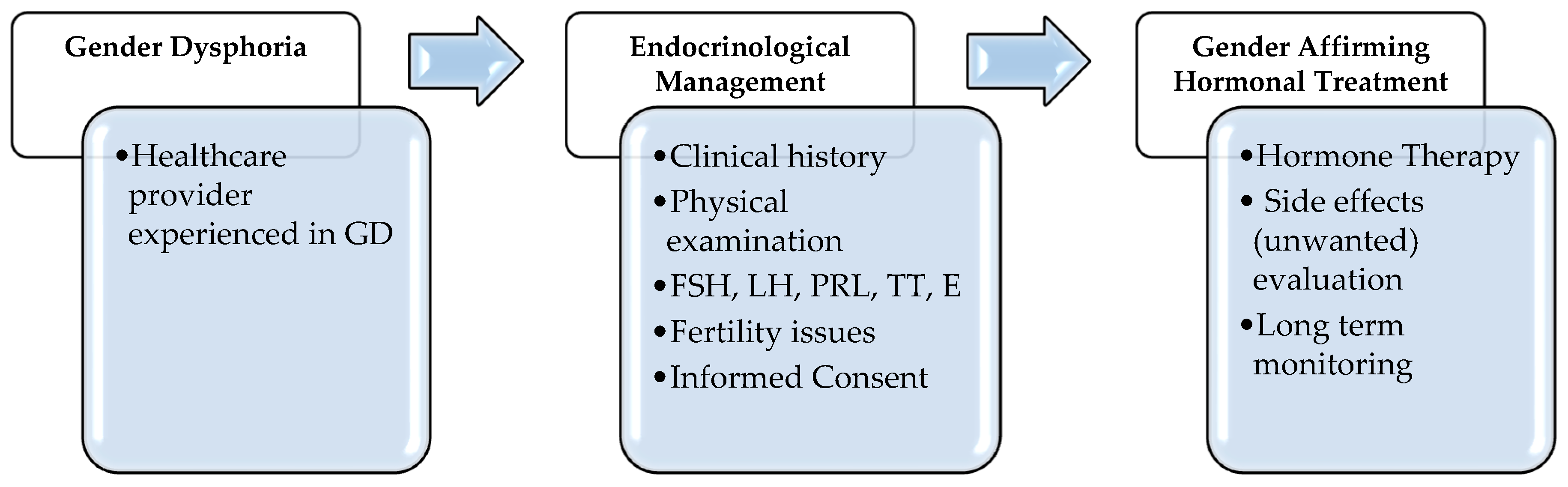
:1. Introduction
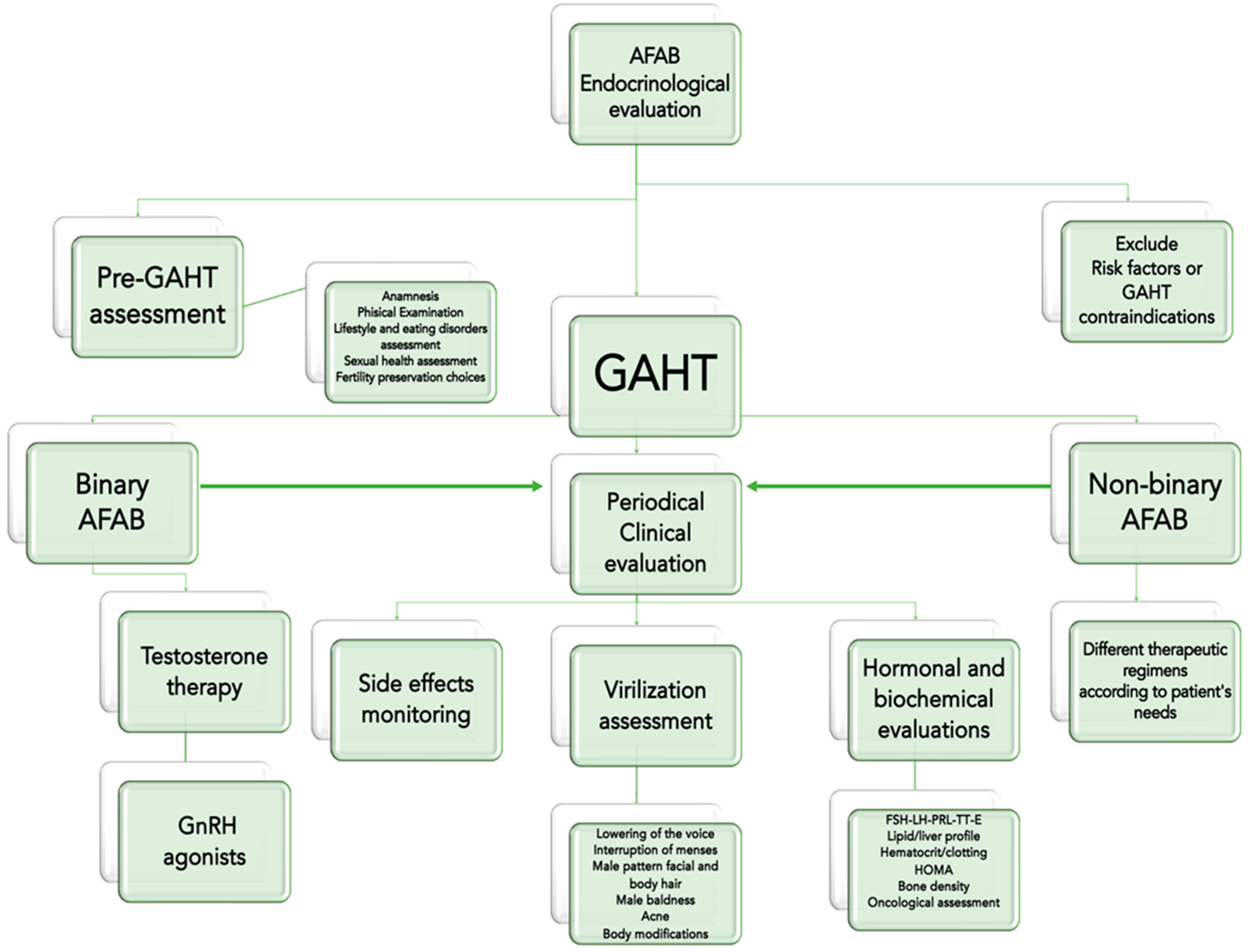
2. The Endocrinological Management of Transgender Men

{kind=link}
{kind=link}
{kind=link}
| Class | Drug | Administration Route | Dose | Risk Factors for Adverse Outcomes [11] | Side Effects |
|---|---|---|---|---|---|
| Androgens | Testosterone undecanoate | Oral | 160–240 mg/die | Very high: Breast/uterine cancer, polycythemia, venous thromboembolism Moderate: baseline hematocrit > 50%, uncontrolled congestive heart failure, untreated Obstructive Sleep Apnoea Syndrome | Hypertension, acute hepatitis, erythrocytosis, hydrosaline retention/edema, increased libido, psychiatric disturbances (in predisposed individuals) |
| Testosterone enanthate or cypionate | Intramuscular | 100–200 mg/2 weeks | |||
| Testosterone undecanoate | Intramuscular | 1000 mg/12 weeks | |||
| Testosterone gel | Transdermal | 40–80 mg/die | |||
| Testosterone patch | 2.5–7.5 mg/die | ||||
| GnRH agonists | Leuprolide acetate | Subcutaneous | 3.75 mg/30 days | Not Reported | Female hormones deprivation Sexual disturbances |
| Triptorelin | 11.25 mg/90 days | ||||
| Goserelin | 3.6 mg/30 days | ||||
| 10.8 mg/90 days |
2.1. GAHT Regimens and Side Effects
2.2. Clinical, Hormonal and Biochemical Evaluations
2.3. Psychological Aspects in Transgender Men during Gender Affirming Hormonal Treatment (GAHT)
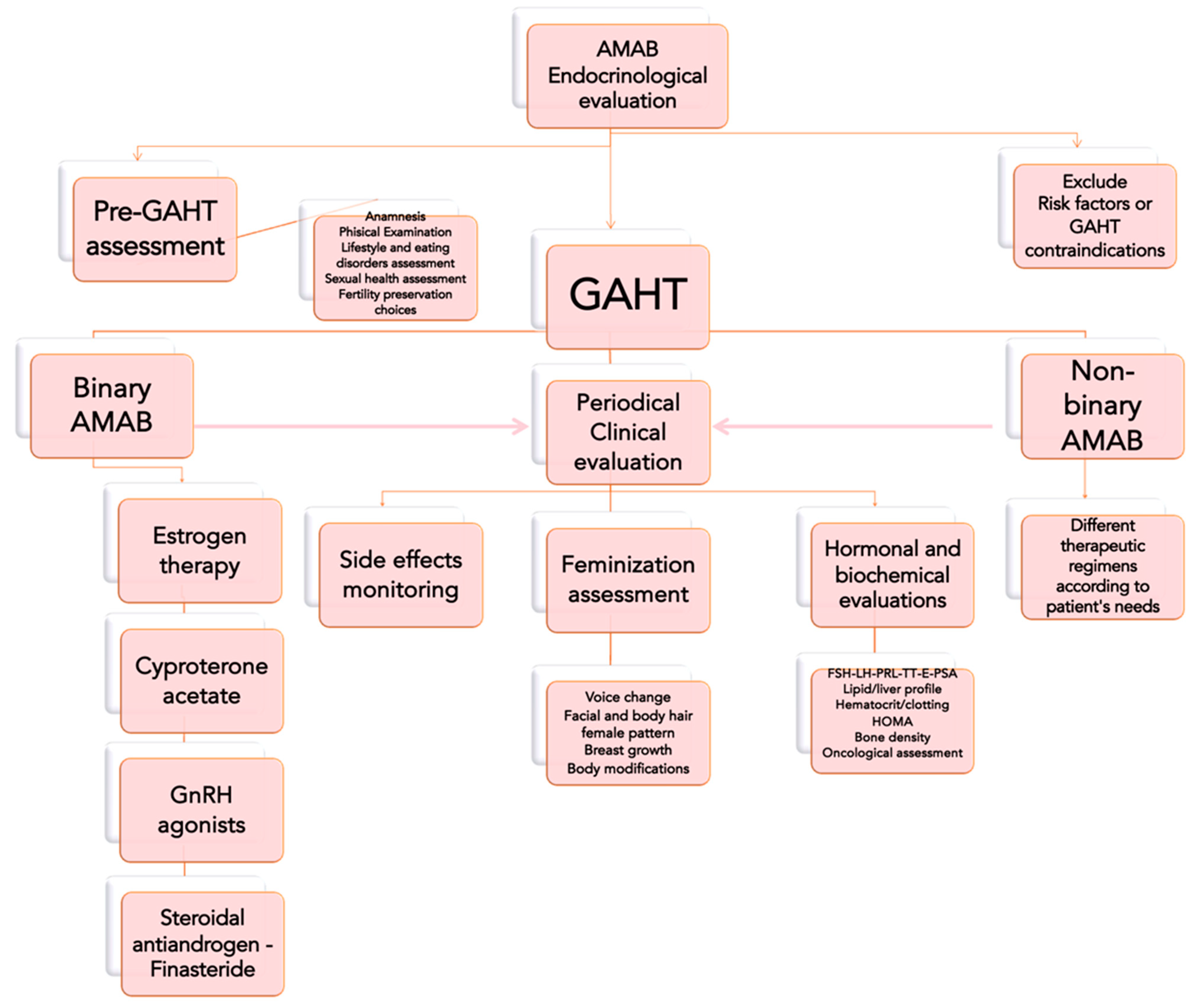
3. The Endocrinological Management of Transgender Women
3.1. GAHT Regimens and Side Effects
3.2. Clinical, Hormonal, and Biochemical Evaluations
3.3. Psychological Aspects in Transgender Women during Gender Affirming Hormonal Treatment (GAHT)
4. Pharmacological Issues in Transgender People during Gender Affirming Hormonal Treatment (GAHT)
5. GAHT and COVID-19 Pandemic
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- American Psychological Association. Guidelines for Psychological Practice with Transgender and Gender Nonconforming People. Am. Psychol. J. 2015, 70, 832–864. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Nguyen, H.B.; Chavez, A.M.; Lipner, E.; Hantsoo, L.; Kornfield, S.L.; Davies, R.D.; Epperson, C.N. Gender-Affirming Hormone Use in Transgender Individuals: Impact on Behavioral Health and Cognition. Curr. Psychiatry Rep. 2018, 20, 110. [Google Scholar] [CrossRef] [PubMed]
- T’Sjoen, G.; Arcelus, J.; De Vries, A.L.C.; Fisher, A.D.; Nieder, T.O.; Özer, M.; Motmans, J. European Society for Sexual Medicine Position Statement “Assessment and Hormonal Management in Adolescent and Adult Trans People, With Attention for Sexual Function and Satisfaction. ” J. Sex. Med. 2020, 17, 570–584. [Google Scholar] [CrossRef] [PubMed]
- Hembree, W.C.; Cohen-Kettenis, P.; Delemarre-van de Waal, H.A.; Gooren, L.J.; Meyer, W.J.; Spack, N.P.; Tangpricha, V.; Montori, V.M. Endocrine Treatment of Transsexual Persons:An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2009, 94, 3132–3154. [Google Scholar] [CrossRef] [Green Version]
- Hembree, W.C.; Cohen-Kettenis, P.T.; Gooren, L.; Hannema, S.E.; Meyer, W.J.; Murad, M.H.; Rosenthal, S.M.; Safer, J.D.; Tangpricha, V.; T’Sjoen, G.G. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society* Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 3869–3903. [Google Scholar] [CrossRef]
- Wierckx, K.; Stuyver, I.; Weyers, S.; Hamada, A.; Agarwal, A.; De Sutter, P.; T’Sjoen, G. Sperm Freezing in Transsexual Women. Arch. Sex. Behav. 2012, 41, 1069–1071. [Google Scholar] [CrossRef]
- Dekker, M.J.H.J.; Wierckx, K.; Van Caenegem, E.; Klaver, M.; Kreukels, B.P.; Elaut, E.; Fisher, A.D.; van Trotsenburg, M.A.A.; Schreiner, T.; den Heijer, M.; et al. A European Network for the Investigation of Gender Incongruence: Endocrine Part. J. Sex. Med. 2016, 13, 994–999. [Google Scholar] [CrossRef]
- T’Sjoen, G.; Van Caenegem, E.; Wierckx, K. Transgenderism and Reproduction. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 575–579. [Google Scholar] [CrossRef]
- De Roo, C.; Tilleman, K.; T’Sjoen, G.; De Sutter, P. Fertility Options in Transgender People. Int. Rev. Psychiatry 2016, 28, 112–119. [Google Scholar] [CrossRef]
- Petering, R.C.; Brooks, N.A.; Health, O.; University, S. Testosterone Therapy: Review of Clinical Applications. Am. Fam. Physician 2017, 96, 441–449. [Google Scholar]
- Bhasin, S.; Cunningham, G.R.; Hayes, F.J.; Matsumoto, A.M.; Snyder, P.J.; Swerdloff, R.S.; Montori, V.M. Testosterone Therapy in Men with Androgen Deficiency Syndromes: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2010, 95, 2536–2559. [Google Scholar] [CrossRef] [PubMed]
- Wierckx, K.; Van Caenegem, E.; Schreiner, T.; Haraldsen, I.; Fisher, A.; Toye, K.; Kaufman, J.M.; T’Sjoen, G. Cross-Sex Hormone Therapy in Trans Persons Is Safe and Effective at Short-Time Follow-Up: Results from the European Network for the Investigation of Gender Incongruence. J. Sex. Med. 2014, 11, 1999–2011. [Google Scholar] [CrossRef] [PubMed]
- Defreyne, J.; Vantomme, B.; Van Caenegem, E.; Wierckx, K.; De Blok, C.J.M.; Klaver, M.; Nota, N.M.; Van Dijk, D.; Wiepjes, C.M.; Den Heijer, M.; et al. Prospective Evaluation of Hematocrit in Gender-Affirming Hormone Treatment: Results from European Network for the Investigation of Gender Incongruence. Andrology 2018, 6, 446–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giltay, E.; Toorians, A.; Sarabdjitsingh, A.; de Vries, N.; Gooren, L. Established Risk Factors for Coronary Heart Disease Are Unrelated to Androgen-Induced Baldness in Female-to-Male Transsexuals. J. Endocrinol. 2004, 180, 107–112. [Google Scholar] [CrossRef]
- Wierckx, K.; Van de Peer, F.; Verhaeghe, E.; Dedecker, D.; Van Caenegem, E.; Toye, K.; Kaufman, J.M.; T’Sjoen, G. Short- and Long-Term Clinical Skin Effects of Testosterone Treatment in Trans Men. J. Sex. Med. 2014, 11, 222–229. [Google Scholar] [CrossRef]
- Koehler, A.; Eyssel, J.; Nieder, T.O. Genders and Individual Treatment Progress in (Non-)Binary Trans Individuals. J. Sex. Med. 2018, 15, 102–113. [Google Scholar] [CrossRef] [Green Version]
- Cocchetti, C.; Ristori, J.; Romani, A.; Maggi, M.; Fisher, A.D. Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals. J. Clin. Med. 2020, 9, 1609. [Google Scholar] [CrossRef]
- Moore, E.; Wisniewski, A.; Dobs, A. Endocrine Treatment of Transsexual People: A Review of Treatment Regimens, Outcomes, and Adverse Effects. J. Clin. Endocrinol. Metab. 2003, 88, 3467–3473. [Google Scholar] [CrossRef]
- Velho, I.; Fighera, T.M.; Ziegelmann, P.K.; Spritzer, P.M. Effects of Testosterone Therapy on BMI, Blood Pressure, and Laboratory Profile of Transgender Men: A Systematic Review. Andrology 2017, 5, 881–888. [Google Scholar] [CrossRef] [Green Version]
- Roberts, T.K.; Kraft, C.S.; French, D.; Ji, W.; Wu, A.H.B.; Tangpricha, V.; Fantz, C.R. Interpreting Laboratory Results in Transgender Patients on Hormone Therapy. Am. J. Med. 2014, 127, 159–162. [Google Scholar] [CrossRef]
- van Kesteren, P.; Lips, P.; Gooren, L.J.G.; Asscheman, H.; Megens, J. Long-Term Follow-up of Bone Mineral Density and Bone Metabolism in Transsexuals Treated with Cross-Sex Hormones. Clin. Endocrinol. 1998, 48, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Elamin, M.B.; Garcia, M.Z.; Murad, M.H.; Erwin, P.J.; Montori, V.M. Effect of Sex Steroid Use on Cardiovascular Risk in Transsexual Individuals: A Systematic Review and Meta-Analyses: Cardiovascular Effects of Sex Steroid Therapy in Transsexuals. Clin. Endocrinol. 2010, 72, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Monami, M.; Rastrelli, G.; Aversa, A.; Tishova, Y.; Saad, F.; Lenzi, A.; Forti, G.; Mannucci, E.; Maggi, M. Testosterone and Metabolic Syndrome: A Meta-Analysis Study. J. Sex. Med. 2011, 8, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Meriggiola, M.C.; Armillotta, F.; Costantino, A.; Altieri, P.; Saad, F.; Kalhorn, T.; Perrone, A.M.; Ghi, T.; Pelusi, C.; Pelusi, G. Effects of Testosterone Undecanoate Administered Alone or in Combination with Letrozole or Dutasteride in Female to Male Transsexuals. J. Sex. Med. 2008, 5, 2442–2453. [Google Scholar] [CrossRef]
- Shadid, S.; Abosi-Appeadu, K.; De Maertelaere, A.-S.; Defreyne, J.; Veldeman, L.; Holst, J.J.; Lapauw, B.; Vilsbøll, T.; T’Sjoen, G. Effects of Gender-Affirming Hormone Therapy on Insulin Sensitivity and Incretin Responses in Transgender People. Diabetes Care 2020, 43, 411–417. [Google Scholar] [CrossRef]
- Wierckx, K.; Mueller, S.; Weyers, S.; Van Caenegem, E.; Roef, G.; Heylens, G.; T’Sjoen, G. Long-Term Evaluation of Cross-Sex Hormone Treatment in Transsexual Persons. J. Sex. Med. 2012, 9, 2641–2651. [Google Scholar] [CrossRef]
- Fallahtafti, E.; Nasehi, M.; Rasuli, R.; Farhud, D.D.; Pourebrahim, T.; Zareeeimahmoodabadi, H. Happiness and Mental Health in Pre-Operative and PostOperative Transsexual People. Iran. J. Public Health 2019, 48, 2277. [Google Scholar] [CrossRef]
- Anzani, A.; De Panfilis, C.; Scandurra, C.; Prunas, A. Personality Disorders and Personality Profiles in a Sample of Transgender Individuals Requesting Gender-Affirming Treatments. Int. J. Environ. Res. Public. Health 2020, 17, 1521. [Google Scholar] [CrossRef] [Green Version]
- Ristori, J.; Fisher, A.D.; Castellini, G.; Maggi, M. Psychiatric Aspects of Gender Dysphoria. In Sexual Dysfunctions in Mentally Ill Patients; Jannini, E.A., Siracusano, A., Eds.; Trends in Andrology and Sexual Medicine; Springer: Cham, Switzerland, 2018; pp. 127–139. ISBN 978-3-319-68305-8. [Google Scholar]
- Jones, T.; del Pozo de Bolger, A.; Dune, T.; Lykins, A.; Hawkes, G. Female-to-Male (FtM) Transgender People’s Experiences in Australia; Springer Briefs in Sociology; Springer: Cham, Switzerland, 2015; ISBN 978-3-319-13828-2. [Google Scholar]
- Testa, R.J.; Michaels, M.S.; Bliss, W.; Rogers, M.L.; Balsam, K.F.; Joiner, T. Suicidal Ideation in Transgender People: Gender Minority Stress and Interpersonal Theory Factors. J. Abnorm. Psychol. 2017, 126, 125–136. [Google Scholar] [CrossRef]
- Lai, M.-C.; Chiu, Y.-N.; Gadow, K.D.; Gau, S.S.-F.; Hwu, H.-G. Correlates of Gender Dysphoria in Taiwanese University Students. Arch. Sex. Behav. 2010, 39, 1415–1428. [Google Scholar] [CrossRef]
- Keo-Meier, C.L.; Herman, L.I.; Reisner, S.L.; Pardo, S.T.; Sharp, C.; Babcock, J.C. Testosterone Treatment and MMPI–2 Improvement in Transgender Men: A Prospective Controlled Study. J. Consult. Clin. Psychol. 2015, 83, 143–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, R.P. Gender Identity Disorder and Schizophrenia: Neurodevelopmental Disorders with Common Causal Mechanisms? Schizophr. Res. Treat. 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Colizzi, M.; Costa, R. The Effect of Cross-Sex Hormonal Treatment on Gender Dysphoria Individuals’ Mental Health: A Systematic Review. Neuropsychiatr. Dis. Treat. 2016, 12, 1953–1966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colizzi, M.; Costa, R.; Pace, V.; Todarello, O. Hormonal Treatment Reduces Psychobiological Distress in Gender Identity Disorder, Independently of the Attachment Style. J. Sex. Med. 2013, 10, 3049–3058. [Google Scholar] [CrossRef]
- Fisher, A.D.; Castellini, G.; Ristori, J.; Casale, H.; Cassioli, E.; Sensi, C.; Fanni, E.; Amato, A.M.L.; Bettini, E.; Mosconi, M.; et al. Cross-Sex Hormone Treatment and Psychobiological Changes in Transsexual Persons: Two-Year Follow-Up Data. J. Clin. Endocrinol. Metab. 2016, 101, 4260–4269. [Google Scholar] [CrossRef] [Green Version]
- McClain, Z.; Peebles, R. Body Image and Eating Disorders Among Lesbian, Gay, Bisexual, and Transgender Youth. Pediatr. Clin. N. Am. 2016, 63, 1079–1090. [Google Scholar] [CrossRef]
- Silverstein, B.; Carpman, S.; Perliek, D.; Perdue, L. Nontraditional Sex Role Aspirations, Gender Identity Conflict, and Disordered Eating among College Women. Sex Roles 1990, 23, 687–695. [Google Scholar] [CrossRef]
- Ålgars, M.; Alanko, K.; Santtila, P.; Sandnabba, N.K. Disordered Eating and Gender Identity Disorder: A Qualitative Study. Eat. Disord. 2012, 20, 300–311. [Google Scholar] [CrossRef]
- Bandini, E.; Fisher, A.D.; Castellini, G.; Lo Sauro, C.; Lelli, L.; Meriggiola, M.C.; Casale, H.; Benni, L.; Ferruccio, N.; Faravelli, C.; et al. Gender Identity Disorder and Eating Disorders: Similarities and Differences in Terms of Body Uneasiness. J. Sex. Med. 2013, 10, 1012–1023. [Google Scholar] [CrossRef]
- Ibrahim, C.; Haddad, R.; Richa, S. Les comorbidités psychiatriques dans le transsexualisme: Étude sur une population de transgenres libanais. L’Encéphale 2016, 42, 517–522. [Google Scholar] [CrossRef]
- T’Sjoen, G.; Arcelus, J.; Gooren, L.; Klink, D.T.; Tangpricha, V. Endocrinology of Transgender Medicine. Endocr. Rev. 2019, 40, 97–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dittrich, R.; Binder, H.; Cupisti, S.; Hoffmann, I.; Beckmann, M.; Mueller, A. Endocrine Treatment of Male-to-Female Transsexuals Using Gonadotropin-Releasing Hormone Agonist. Exp. Clin. Endocrinol. Diabetes 2005, 113, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Tangpricha, V.; den Heijer, M. Oestrogen and Anti-Androgen Therapy for Transgender Women. Lancet Diabetes Endocrinol. 2017, 5, 291–300. [Google Scholar] [CrossRef] [Green Version]
- Gooren, L.; Lips, P. Conjectures Concerning Cross-Sex Hormone Treatment of Aging Transsexual Persons. J. Sex. Med. 2014, 11, 2012–2019. [Google Scholar] [CrossRef]
- Klaver, M.; Dekker, M.J.H.J.; de Mutsert, R.; Twisk, J.W.R.; den Heijer, M. Cross-Sex Hormone Therapy in Transgender Persons Affects Total Body Weight, Body Fat and Lean Body Mass: A Meta-Analysis. Andrologia 2017, 49, e12660. [Google Scholar] [CrossRef]
- Giltay, E.J.; Gooren, L.J.G. Effects of Sex Steroid Deprivation/Administration on Hair Growth and Skin Sebum Production in Transsexual Males and Females. J. Clin. Endocrinol. Metab. 2000, 85, 2913–2921. [Google Scholar] [CrossRef]
- Gennari, L.; Khosla, S.; Bilezikian, J.P. Estrogen and Fracture Risk in Men. J. Bone Miner. Res. 2008, 23, 1548–1551. [Google Scholar] [CrossRef]
- Valentini, F.M.; Aversa, A.; Bruzziches, R.; Fornari, R.; Greco, E.A.; Rossi, F.; Brama, M.; Spera, G.; Migliaccio, S. Characterization of Bone Mineral Density in Male-to-Female Transsexuals Receiving Treatment for Reassignment Surgery: 15 Years of Follow-Up. J. Men’s Health 2008, 5, 227–233. [Google Scholar] [CrossRef]
- Turo, R.; Jallad, S.; Cross, W.R.; Prescott, S. Metastatic Prostate Cancer in Transsexual Diagnosed after Three Decades of Estrogen Therapy. Can. Urol. Assoc. J. 2013, 7, 544. [Google Scholar] [CrossRef] [Green Version]
- Kesteren, P.; Meinhardt, W.; van der Valk, P.; Geldof, A.; Gooren, L. Effects of Estrogens Only on the Prostates of Aging Men. J. Urol. 1996, 156, 1349–1353. [Google Scholar] [CrossRef]
- Asscheman, H.; Giltay, E.J.; Megens, J.A.J.; de Ronde, W.P.; van Trotsenburg, M.A.A.; Gooren, L.J.G. A Long-Term Follow-up Study of Mortality in Transsexuals Receiving Treatment with Cross-Sex Hormones. Eur. J. Endocrinol. 2011, 164, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, G.; Sumner, B.E.H. Oestrogen and Mental State. Nature 1996, 383, 306. [Google Scholar] [CrossRef] [PubMed]
- Asscheman, H.; Gooren, L.J.G.; Eklund, P.L.E. Mortality and Morbidity in Transsexual Patients with Cross-Gender Hormone Treatment. Metabolism 1989, 38, 869–873. [Google Scholar] [CrossRef]
- Colizzi, M.; Costa, R.; Todarello, O. Transsexual Patients’ Psychiatric Comorbidity and Positive Effect of Cross-Sex Hormonal Treatment on Mental Health: Results from a Longitudinal Study. Psychoneuroendocrinology 2014, 39, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Leavitt, F.; Berger, J.C.; Hoeppner, J.-A.; Northrop, G. Presurgical Adjustment in Male Transsexuals with and without Hormonal Treatment. J. Nerv. Ment. Dis. 1980, 168, 693–697. [Google Scholar] [CrossRef]
- Slabbekoorn, D.; Van Goozen, S.H.M.; Gooren, L.J.G.; Cohen-Kettenis, P.T. Effects of Cross-Sex Hormone Treatment on Emotionality in Transsexuals. Int. J. Transgenderism 2001, 5, 2. [Google Scholar]
- Fuxjager, M.J.; Trainor, B.C.; Marler, C.A. What Can Animal Research Tell Us about the Link between Androgens and Social Competition in Humans? Horm. Behav. 2017, 92, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Defreyne, J.; T’Sjoen, G.; Bouman, W.P.; Brewin, N.; Arcelus, J. Prospective Evaluation of Self-Reported Aggression in Transgender Persons. J. Sex. Med. 2018, 15, 768–776. [Google Scholar] [CrossRef]
- Mirabella, M.; Giovanardi, G.; Fortunato, A.; Senofonte, G.; Lombardo, F.; Lingiardi, V.; Speranza, A.M. The Body I Live in. Perceptions and Meanings of Body Dissatisfaction in Young Transgender Adults: A Qualitative Study. J. Clin. Med. 2020, 9, 3733. [Google Scholar] [CrossRef]
- Webb, A.J.; McManus, D.; Rouse, G.E.; Vonderheyde, R.; Topal, J.E. Implications for Medication Dosing for Transgender Patients: A Review of the Literature and Recommendations for Pharmacists. Am. J. Health. Syst. Pharm. 2020, 77, 427–433. [Google Scholar] [CrossRef]
- Jue, J.S.; Alameddine, M. Assessment of Renal Function in Transgender Patients. Am. J. Health-Syst. Pharm. 2020, 77, 1460–1461. [Google Scholar] [CrossRef] [PubMed]
- Cirrincione, L.R.; Senneker, T.; Scarsi, K.; Tseng, A. Drug Interactions with Gender-Affirming Hormone Therapy: Focus on Antiretrovirals and Direct Acting Antivirals. Expert Opin. Drug Metab. Toxicol. 2020, 16, 565–582. [Google Scholar] [CrossRef] [PubMed]
- Sevelius, J.M.; Deutsch, M.B.; Grant, R. The Future of PrEP among Transgender Women: The Critical Role of Gender Affirmation in Research and Clinical Practices. J. Int. AIDS Soc. 2016, 19, 21105. [Google Scholar] [CrossRef] [PubMed]
- Yager, J.L.; Anderson, P.L. Pharmacology and Drug Interactions with HIV PrEP in Transgender Persons Receiving Gender Affirming Hormone Therapy. Expert Opin. Drug Metab. Toxicol. 2020, 16, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Shieh, E.; Marzinke, M.A.; Fuchs, E.J.; Hamlin, A.; Bakshi, R.; Aung, W.; Breakey, J.; Poteat, T.; Brown, T.; Bumpus, N.N.; et al. Transgender Women on Oral HIV Pre-exposure Prophylaxis Have Significantly Lower Tenofovir and Emtricitabine Concentrations When Also Taking Oestrogen When Compared to Cisgender Men. J. Int. AIDS Soc. 2019, 22, e25405. [Google Scholar] [CrossRef]
- Johnson, E.L.; Kaplan, P.W. Caring for Transgender Patients with Epilepsy. Epilepsia 2017, 58, 1667–1672. [Google Scholar] [CrossRef] [Green Version]
- Jarrett, B.A.; Peitzmeier, S.M.; Restar, A.; Adamson, T.; Howell, S.; Baral, S.; Beckham, S.W. Gender-Affirming Care, Mental Health, and Economic Stability in the Time of COVID-19: A Global Cross-Sectional Study of Transgender and Non-Binary People. medRxiv 2020. [Google Scholar] [CrossRef]
- Wozniak, R.J.; Nixon, D.F.; Marston, J.L. Involvement of Cisgender and Transgender Individuals in Studies on the Impact of Hormonal Therapy on COVID-19. AIDS Patient Care STDs 2020, 34, 367–368. [Google Scholar] [CrossRef]
- Cannarella, R.; Calogero, A.E.; Condorelli, R.A.; Aversa, A.; La Vignera, S. Systemic Effects of the Hormonal Treatment of Male Hypogonadism with Preliminary Indications for the Management of COVID-19 Patients. Ther. Adv. Endocrinol. Metab. 2020, 11, 204201882096643. [Google Scholar] [CrossRef]
- Mohamed, M.S.; Moulin, T.C.; Schiöth, H.B. Sex Differences in COVID-19: The Role of Androgens in Disease Severity and Progression. Endocrine 2020, 71, 3–8. [Google Scholar] [CrossRef]
- Bhowmick, N.A.; Oft, J.; Dorff, T.; Pal, S.; Agarwal, N.; Figlin, R.A.; Posadas, E.M.; Freedland, S.J.; Gong, J. COVID-19 and Androgen-Targeted Therapy for Prostate Cancer Patients. Endocr. Relat. Cancer 2020, 27, R281–R292. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S.; Cannarella, R.; Condorelli, R.A.; Torre, F.; Aversa, A.; Calogero, A.E. Sex-Specific SARS-CoV-2 Mortality: Among Hormone-Modulated ACE2 Expression, Risk of Venous Thromboembolism and Hypovitaminosis D. Int. J. Mol. Sci. 2020, 21, 2948. [Google Scholar] [CrossRef] [PubMed]
- Drobnis, E.Z.; Nangia, A.K. Immunosuppressants and Male Reproduction. In Impacts of Medications on Male Fertility; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2017; Volume 1034, pp. 179–210. ISBN 978-3-319-69534-1. [Google Scholar]
- Schroeder, M.; Schaumburg, B.; Müller, Z.; Parplys, A.; Jarczak, D.; Nierhaus, A.; Kloetgen, A.; Schneider, B.; Peschka, M.; Stoll, F.; et al. Sex Hormone and Metabolic Dysregulations are Associated with Critical Illness in Male Covid-19 Patients. medRxiv 2020. [Google Scholar] [CrossRef]
- Suba, Z. Prevention and Therapy of COVID-19 via Exogenous Estrogen Treatment for Both Male and Female Patients; An Opinion Paper. J. Pharm. Pharm. Sci. 2020, 23, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connors, J.M.; Levy, J.H. Thromboinflammation and the Hypercoagulability of COVID-19. J. Thromb. Haemost. 2020, 18, 1559–1561. [Google Scholar] [CrossRef] [PubMed]
- Di Luigi, L.; Pigozzi, F.; Sgrò, P.; Frati, L.; Di Gianfrancesco, A.; Cappa, M. The Use of Prohibited Substances for Therapeutic Reasons in Athletes Affected by Endocrine Diseases and Disorders: The Therapeutic Use Exemption (TUE) in Clinical Endocrinology. J. Endocrinol. Invest. 2020, 43, 563–573. [Google Scholar] [CrossRef] [PubMed]
- World Anti-Doping Agency. Therapeutic Use Exemptions. Available online: https://www.wada-ama.org/en/what-we-do/science-medical/therapeutic-use-exemptions (accessed on 6 January 2021).



| Class | Drug | Administration Route | Dose | Risk Factors for Adverse Outcomes | Side Effects |
|---|---|---|---|---|---|
| Estrogens | Estradiol | Oral | 2–6 mg/die | Very high: venous thromboembolism, prostate cancer Moderate: macroprolactinoma, breast cancer, coronary artery diseases, cerebrovascular diseases, cholelithiasis and hypertriglyceridemia. | Increase of thrombotic risk and hepatotoxicity |
| Estradiol valerate | |||||
| Estradiol valerate or cypionate | Intramuscular | 2–10 mg/week 5–30 mg/2 weeks | |||
| Estradiol patch | Transdermal | 0.025–0.2 mg/die | Increase of thrombotic risk, hepatotoxicity and cutaneous reactions | ||
| Antiandrogen-Progestin | Cyproterone acetate | Oral | 25–50 mg/die | Not Reported | Increased risk of meningiomas, depression, and hyperprolactinemia |
| GnRH agonists | Leuprolide acetate | Subcutaneous | 3.75 mg/30 days 11.25 mg/90 days | Not Reported | Male hormones deprivation, flushing |
| Triptorelin | |||||
| Goserelin | 3.6 mg/30 days 10.8 mg/90 days | ||||
| Steroidal antiandrogen | Spironolactone | Oral | 100–300 mg/die | Not Reported | Hypotension, hyperkalaemia and hyperprolactinemia. |
| 5-α-reductase inhibitor | Finasteride | Oral | 2.5–5 mg/die | Not Reported | Depression and sexual dysfunctions |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iuliano, S.; Izzo, G.; Zagari, M.C.; Vergine, M.; Brunetti, F.S.; Brunetti, A.; Di Luigi, L.; Aversa, A. Endocrine Management of Transgender Adults: A Clinical Approach. Sexes 2021, 2, 104-118. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010009
Iuliano S, Izzo G, Zagari MC, Vergine M, Brunetti FS, Brunetti A, Di Luigi L, Aversa A. Endocrine Management of Transgender Adults: A Clinical Approach. Sexes. 2021; 2(1):104-118. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010009
Chicago/Turabian StyleIuliano, Stefano, Giulia Izzo, Maria Carmela Zagari, Margherita Vergine, Francesco Saverio Brunetti, Antonio Brunetti, Luigi Di Luigi, and Antonio Aversa. 2021. "Endocrine Management of Transgender Adults: A Clinical Approach" Sexes 2, no. 1: 104-118. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2010009