
Migrants’ Sexual Violence in the Mediterranean Region: A Regional Analysis

Department of Psychology and Social Sciences, Frederick University, Nicosia 1036, Cyprus
*
Author to whom correspondence should be addressed.
Sexes 2021, 2(3), 305-314; https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2030024
Submission received: 22 May 2021
/
Revised: 20 June 2021
/
Accepted: 29 June 2021
/
Published: 5 July 2021
(This article belongs to the Special Issue Sexual and Reproductive Health of Female Migrants)
Abstract
:Migration in the Mediterranean region has increased greatly during the last years. Reports and studies reveal that violence and injuries among refugees and migrants is a common occurrence in the WHO Europe Region. Available literature indicates that sexual violence incidents take place: (a) during the migratory journey to the host country, (b) while in detention centers, (c) once migrants have reached their destination, and (d) during the period in which a woman is subject of trafficking. This manuscript explores how sexual violence against refugee/immigrant women is presented in the international literature; a narrative review of the literature was conducted on the phenomenon of migration in the Mediterranean area, and specifically on sexual violence of migrant women. In order to face the challenges faced by migrant women victims of sexual violence, the following policies are suggested by international literature: (a) offer emergency medical and health care to sexual violence survivors, which is usually relatively limited, (b) offer mental health care and psychological support for sexual violence when planning services to provide clinical care, and (c) work towards the aim of transforming norms and values in order to promote gender equality and support non-violent behaviours.
1. Introduction–Migration in Mediterranean Region
In 2019, the global number of migrants reached an estimated 272 million [1], 51 million more than in 2010. International migrants now comprise 3.5 per cent of the global population [1]. While many individuals migrate out of choice, many others migrate out of necessity. The number of globally forcibly displaced people topped 70 million for the first time in United Nations High Commissioner for Refugees almost 70-year history at the end of 2018. This number includes almost 26 million refugees, 3.5 million asylum seekers, and over 41 million internally displaced persons [1]. Of course, there are numerous unaccompanied minors among this population, which are estimated to be almost 20,000 [2]. This is a common issue for south European countries (e.g., Cyprus, Greece, Malta and Spain), which are close to countries in a state of war or with extremely high percentages of poverty.
This increase in mixed flows is largely due to the geopolitical fracture in the SEM region originating from the 2011 civil society uprisings in Tunisia and Egypt and the outbreak of civil wars in Libya and Syria, whose consequences continue to have a significant impact on Europe, inter alia in terms of managing migrant and refugee flows [3]. Southern European countries like Spain and Italy have seen large increases in their migrant populations over the last two decades, and conflicts such as the Syrian crisis have reshaped migratory equilibria in the Eastern Mediterranean region, with large inflows to countries such as Jordan, Turkey and Lebanon [4]. Also, trans-Saharan migration has amounted to a serious humanitarian situation, with people being smuggled across deadly routes, trapped in detention centers, or dying at sea [5]. The lethal effects of irregular migration have become particularly salient in the Euro Mediterranean region since the beginning of the Arab Spring in 2011, as several thousand migrants have been losing their lives every year [6]. The Mediterranean Sea has been the deadliest region for migrants in the world for almost a decade. The Mediterranean context opens up its own policy specificities, which relate to the dilemmas surrounding the experiences of people trying to enter the EU through dangerous trips by sea. These trips often involve extreme hardship and risks to the people involved, which in many cases have led to lives being lost in the Mediterranean [7]. As a death toll rises, people have increasingly turned into numbers [8]. From 2014 to the end of 2016, over 450,000 people crossed from North Africa towards Italy via the Central Mediterranean route. The number of people recorded as dead or missing in the same stretch of water steadily increased, too [9]. Estimates reveal that there were about 4690 deaths in 2016 [7]. In 2015, the number of arrivals peaked, with more than a million persons reaching the EU by sea, and nearly 4000 perishing en route. While the number of arrivals dropped to just over 356,000 the following year, the rate of dead and missing increased to more than 5000. This is a significant proportion of the 7763 total migrant deaths recorded worldwide for the same period [10]. Europe’s Mediterranean border is by far the world’s deadliest: between 2000 and 2017, 33,761 migrants were reported to have died or gone missing in the Mediterranean during their journeys. The highest number of fatalities (5096) was recorded in 2016, after the short and relatively less dangerous route from Turkey to Greece was shut following the European Union–Turkey statement [11].
2. Materials and Methods
A narrative review of the literature was conducted on the phenomenon of migration in the Mediterranean area, and specifically on sexual violence of migrant women. English-language publications in PubMed, Medline/Ovid, Google Scholar, Scopus and other databases were searched in order to identify additional relevant material.
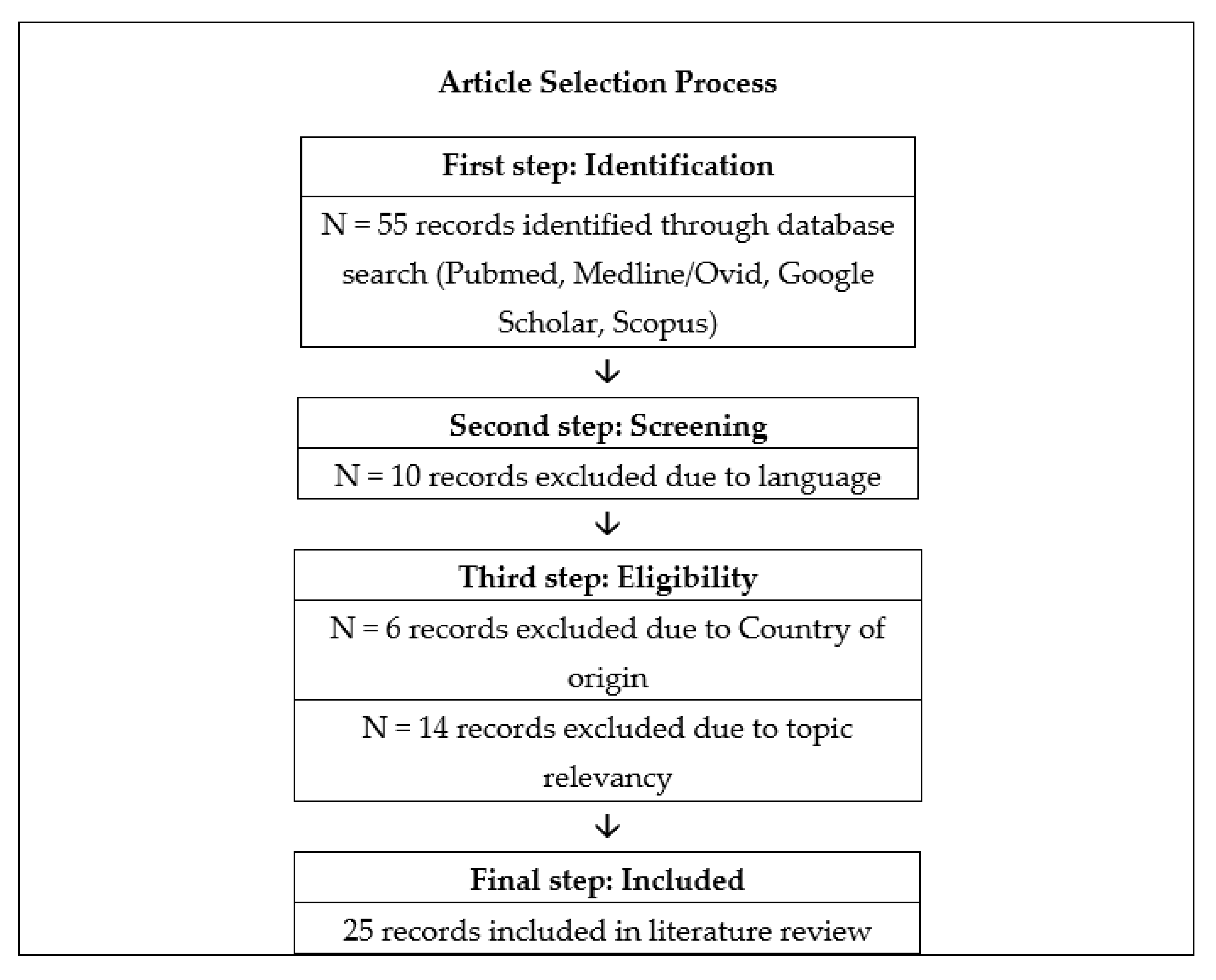
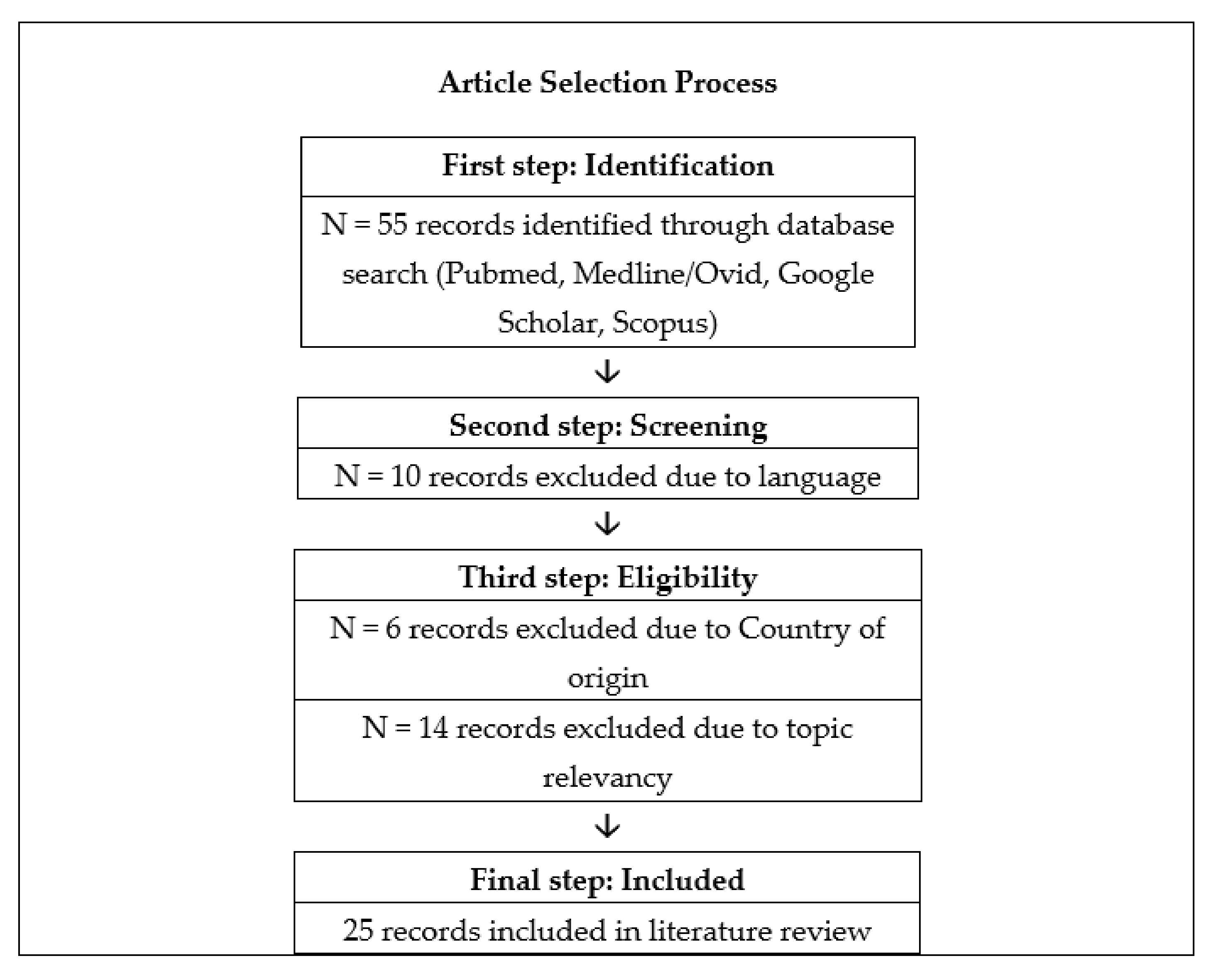
Our search included both free text key words and acronyms of the following terms: “women”, “migration”, “Mediterranean”, “sexual violence”. Boolean operators and star truncation (*) were used as needed. We further conducted an in-depth review of the available grey literature on the same topic such as official documentation, policy and technical reports published by the European Union and other European, local and/or global organisations. Using a narrative synthesis approach, two authors independently extracted and analyzed data from published papers. After removal of duplicates, screening, and assessing for eligibility of 55 initially identified citations, 25 papers and policy papers were used for the purposes of this manuscript (see Figure 1).
3. Migration and Sexual Violence in the Mediterranean Region
It is estimated that 1 in 4 women will experience at least one incident of sexual violence during their lifetime. An international report by the World Health Organisation [12] reports that, globally, 35.6% of women experience sexual or physical violence at least once in their lifetime. Sexual assault includes an unwanted sexual act, an attempt to obtain a sexual act, or contact or communication with unwanted sexual attention not amounting to rape. It also includes sexual assault with or without physical contact, including drug-facilitated sexual assault; sexual assault committed against a marital partner against her/his will, sexual assault against a helpless person, unwanted groping or fondling, harassment and threats of a sexual nature [13,14]. Sexualized forms of torture has be to recognized as sexual violence, as opposed to solely torture because this has specific legal implications [15].
Reports and studies published by international organizations and NGOs (and to a limited extent by academic literature) have focused on specific gender issues relating to migration and asylum or on specific “gendered” subjects, e.g., migrant women, refugee women, victims of trafficking and sexual exploitation, Lesbian-Gay-Bisexual-Transgender (LGBT) refugees, gender violence in migration contexts, etc. [3]. The World Health Organisation in 2020 [16] published the technical guide titled “Strategies and interventions on preventing and responding to violence and injuries among refugees and migrants”, in order to outline current evidence, knowledge and best practice relating to incidences of violence and injuries among refugees and migrants in the WHO Europe Region. Available evidence suggests that incidences of harm are significant among refugees and migrants at all stages of the migratory process. Current knowledge is covered under: (1) injuries associated with different migratory modes of transport, (2) violence and intentional injuries en route, (3) SGBV, (4) human trafficking and smuggling, (5) occupational injuries and violence, and (6) racially incited violence and hate crimes, and religious discrimination [17]. In addition, gender-based violence comprises multiple forms such as child marriage and women being used as sex-slaves [18].
In addition, available literature indicates that sexual violence incidents take place (a) during the migratory journey to the host country, (b) during being kept in detention centers, (c) once migrants have reached their destination, and (d) during the period in which a woman is subject of trafficking (see Table 1 below).
There are numerous references regarding incidents of sexual violence and other traumatic experiences against women during the migration journey. Available information suggests that the vast majority of women and girls, as well as many men and boys, have been victims of sexual and gender-based violence and torture, including sexual assault and rape, sometimes by multiple perpetrators, during their journeys [19]. According to UNICEF [20], women’s experiences of sexual violence on the migrant journey include being forced to have sex by smugglers, being compelled to sell their bodies in order to buy a seat or to avoid torture and violence. Baklacioğlu [21] stated that there are references according to which Syrian women on the Euro-Mediterranean transit region reported experiences with violence during the passage. In addition, Keygnaert et al. [22] highlighted the risk of sexual violence that sub-Saharan migrants and asylum seekers faced when attempting to cross to Europe from Morocco [23]. In addition, Freedman [24] underlined that migrant women traveling alone or without male partners are particularly vulnerable to attack, and there were several accounts of women who had been raped and sexually assaulted on their journeys. Moreover, the vast majority of migrants who used the Central Mediterranean Route reported having been victims of violence during their transit in Libya [25]. Women are at particular risk of sexual violence. Similarly, a study conducted at a free clinic in Israel to examine exposure to trauma among asylum seekers en route to Israel from Eritrea and Sudan found that almost half (mostly men) reported being victims of violence [26]; exposure to shootings and beatings was most prevalent, yet instances of sexual assault, electric shock, burning, threats of execution and deprivation of food and/or water were also recorded [26]. Overall, sexually transmitted infections are often prevalent in migrants with high-risk behaviours or due to sexual abuse during the transit phase [27].
Violence and insecurity in migrant reception and detention centers are widespread, with extensive reporting of multiple types of violence, and multiple cases of sexual and gender-based violence in asylum settings [28]. Similarly, migrants might face abusing behavior and treatment during their attempt to reach Europe. For example, foreign nationals who have entered Libya with the aim of reaching Europe, they found themselves stuck in the country, being kept in detention centers where they are exposed to all sorts of abuse, from sexual slavery to assassination [11]. Kalt et al. [29] supported that over one third (35.7%) of women in detention centers have faced sexual harassment by detention officers, and during medical consultations the rate of sexual violence was reported to be 44.2%. In addition, the occurrence of transactional sex has also been reported, where women have been coerced into sex in return for help on their passage to Europe or while in detention facilities in return for help with their cases [30]. Staff, guards and volunteers are very often the perpetrators of such violence, including using transactional sex whereby women are promised priority case assessment and faster release if they agreed to sexual activities with male guards [28].
The available literature also indicates that violence incidents also occur once migrants have reached their destination. Reports state that the unsafe conditions of the journey are often confirmed at landing in the new country [31,32]. This includes physical, psychological, sexual and economic harm perpetrated by a current or former partner and can occur throughout the migration process as well as in the destination country [33]. Sexual violence against immigrant women is widespread yet even after migration, women are exposed to multiple forms of insecurity and sexual violence with major effects on their health [34,35]. Evidence shows that migrant sex workers have been beaten, raped and robbed by police, and in some cases are forced to exchange sexual services for protection [36]. This trend is also evident since violence against migrant workers in the form of exposure to sexual harassment and other forms of psychological pressure and discrimination have also been recorded and are higher than for the local populations [37]. Women infected with HIV after migration reported experience of forced sexual intercourse after migration 4 times more frequently than uninfected women [34]. Also, relational situations are themselves closely linked to women’s living conditions and to the sexual violence they experience; reported having transactional sexual relations after arriving in France to obtain money or other necessities, such as a place to sleep [34]. Overall, it could be illustrated that women who migrate to escape violence in their home country are more likely to also experience violence (this time sexual) at destination [34].
Finally, there are many references in the international literature regarding sexual violence faced by migrants and/or migrants being subject of trafficking [5,11]. In one case, young women from Nigeria expressed their experiences according to which they were unable to leave the place of residence and suffered physical and sexual violence [9]. Moreover, their accusations were based on the fact that they were placed in a stable and treated as animals, whereas they were raped many times by the men who were supposed to watch them [9]. Similarly, Mountz and Loyd [38] stated that migrants’ women are also vulnerable to human trafficking and smuggling industries and women in particular can be subjected to sexual violence during the migration journey. In addition, the human trafficking ring can act directly by kidnapping these women. Women irregular migrants (WIMs) can be tricked, kidnapped, forced to hide to avoid being discovered, transported secretly, and sexually exploited [39]. Piscitelli et al. [40] highlighted that migrants from sub-Saharan Africa are at a high risk of sexual victimisation and that many women are forced to pay for their migration through prostitution or are subject to brutal sexual exploitation and torture along the journey. The consequences of migrants’ sexual violence and policies to tackle them are further discussed in the following section (briefly presented in Table 2 below).
4. Discussion
Data presented above reveal that sexual violence faced by migrants is currently a tremendous issue in the Mediterranean region. Even though available statistics cannot reflect the exact extent of the problem, it is be estimated that incidents of sexual violence could have been increased due to the large increases in migrant populations in the region over the last two decades. Incidents of sexual violence lead to significant health consequences such as injuries, sexually transmitted infections including HIV, unintended pregnancies, gynecological problems, and adverse mental health effects leading to PTSD, anxiety or depression [15], vaginal/rectal bleeding, other genital or body injuries, pain during sexual intercourse, psychosomatic issues, mental health problems, and even suicidal ideation, self-harm, and death [41]. Longer-term impacts may include behavioral problems, isolation, guilt, rejection by the family, or an inability to take care of the family, and may prevent a woman from marrying due to cultural taboos [42].
In addition, one of the main issues that have to be considered is the link between sexual violence and other infections and/or diseases. A study revealed that for a share of women infected with HIV after migration, sexual violence is associated with situations of high HIV-transmission risk in an extremely insecure social environment [33]. A study in Malta revealed that high-risk behaviours, sexual abuse, poor living conditions and barriers to accessing health care might affect migrants’ sexual health, leading to infections [26]. Madise and Onyango [43] and WHO [42], stated that sexual violence is not only a crime, but also a public health concern since it is associated with ill-health including depression, low birthweight babies, and infection from HIV.
Moreover, reproductive health issues have to be seriously taken into account. A study revealed that women who belong to a human trafficking network that makes all the decisions for them, including their sexual and reproductive health. They decide where WIMs will be prostituted and if she will use any contraceptive methods; if a woman is pregnant, the human trafficking network will decide whether she will abort or carry the baby to term [39]. According to Brabcová et al. [37], it was revealed that 11 women and one man were sexually abused during their migration to Europe. Ten of them claimed to have been sexually abused and tortured during their stay in Libyan camps or prisons; two during the African route. Six people (including the man) were raped by a group of men and six by a single man. One showed HIV seroconversion. Eight women became pregnant as a result of the sexual violence, of whom seven asked for an abortion in Italy.
In order to face the challenges described above action has to be taken. In first place, emergency and medical care has to be offered to victims of sexual violence. The medical care that could be offered to sexual violence survivors was usually relatively limited, as most sought care months after the event, limiting the treatment options available [23]. Of course, in some cases access to health care is almost non-existent (e.g., Libya) [42]. It is suggested that emergency care for new arrived migrants in the European Union must include gynecological examinations and must make detecting sexual violence and human trafficking of WIMs part of their care protocols, since WIMs who arrive to Europe in small boats have a history of violence, rape, prostitution, forced pregnancy and human trafficking [39]. To be effective, medical care needs to be provided as soon as possible after the incident [23]. Also, it is recommended that health services should be available for survivors of sexual violence and to ensure people without documentation can still access protection services in these transit countries, as well as in EU Member States [23,35].
McGinn and Casey [43] claimed that refugee women escaping from conflict violence created the need for better targeting of reproductive health services and psychosocial services in refugee settings. It is the responsibility of humanitarian non-governmental organisations and of the host countries to provide safe abortions to women who become pregnant as a result of rape [22].
Secondly, mental health needs for sexual violence victims have to be seriously considered when planning services to provide clinical care [23]. According to La Cascia et. al. [44], mental health of migrants seems to be influenced by experiences in the home country before migration, the process of migration itself, and the living conditions in the country of settlement. Most of migrants, when they arrive at the host countries, show wounds, signs and symptoms of violence suffered and of their psychological suffering. Additionally, psychological support has to be offered to victims of sexual violence. Current literature underlines the fact that the psychological impact of sexual violence was often complex due to cross-cultural issues, while the lack of access to mental health care contributed to delays in the psychological assessment and adequate support of the patient [22].
According to Reques et al. [42] most migrants requested for psychological support due to how mental health disorders occur as a consequence of migration, mainly linked to forced, unplanned, poorly planned or illegal migration, low educational level, isolation, lack of support and perceived discrimination [45,46,47].
Thirdly, it is critical to start by aiming to change norms and values in order to promote gender equality and support non-violent, respectful and positive relationships [48]. Transforming social norms and behaviours is a long-term and complex process that requires reinforcement at multiple levels; it will need to be enabled by appropriate legal and policy reforms that address structural inequalities more broadly [49]. Preventive measures and awareness raising campaigns could be also beneficial in the attempt to face sexual violence against migrant women. The study outcomes support the need of improving awareness about sexual/gender-based violence and sexual transmitted infections risks. Also, community-based education interventions e.g., by distributing multilingual educational material in reception centres and via culturally sensitive information sessions targeting different migrant groups, could be a beneficial practice [27].
The host countries have to protect migrants from sexual violence with proper designing of the camp. It’s vital, the geographical location of a refugee camp. For example, if the camp is located in an area which has a serious crime problem or is geographically isolated from the local population may increase the likelihood of sexual violence. Additionally, camps are often overcrowded and unrelated families may need to share communal living and sleeping space and increased possibilities to sexual violence, especially to migrant women. The lack of police protection and general lawlessness in some camps is also a factor that may also expose them to danger [50].
Migrant workers can take a number of important practical steps to reduce the risk of sexual violence. They have to develop appropriate strategies to address particular protection to vulnerable individuals, mostly women and children. Migrant workers have to ensure that refugee women have proper personal documentation and access on an equal basis with men to whatever registration processes are used to determine eligibility for assistance. Migrant women should have ready access to female protection staff and female interpreters, as well as to reproductive health facilities including female medical staff and gynecologists. Also, where sexual violence is suspected but the person is reluctant to report the incident, it is advisable for a social worker or health worker to meet privately with the suspected victim either alone or with a trusted person of her choice. One of the most effective ways of “tapping” the refugee information network to identify cases of sexual violence is to facilitate the establishment of women’s groups and associations, thereby giving individual women a channel to report attacks. Experience has shown that an effective mechanism is a women’s health clinic, which deals with women’s physical health, and thus offers a “safe” environment for revealing attacks [51].
5. Conclusions
In order to prevent the continuation of this reality, it is necessary to put in place a coordinated attempt by all involved stakeholders in a higher European level. For this ethnically diverse group, a specialist service which can provide clinical corroboration of self reported histories of physical violence and torture to support asylum applications is an essential minimum [52]. In addition, more efforts have to be made to establish a common European standard for migrants’ sexual health testing at reception and during settlement [27]. Therefore, a better understanding of the patterns of sexual violence and the needs of its survivors in the context of migration is required, in order to improve and upscale the provision of care to this extraordinarily vulnerable population [53]. Also, health projects in migration settings have to be advanced, as they offer an opportunity to understand and document the risks and needs of migrants and asylum seekers who have experienced sexual violence; ideally, similar projects will result in better packages of care for sexual violence survivors [23]. There is a great room for development; it is up to EU administration to focus on this sensitive population and adopt new policies and practices for its protection.
Author Contributions
Conceptualization, S.P; methodology, D.H.; formal analysis, S.P.; resources, D.H.; writing-review and editing, S.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- United Nations. Department of Economic and Social Affairs, Population Division, International Migration. Available online: https://www.un.org/en/development/desa/population/migration/data/estimates2/estimates19.asp (accessed on 15 April 2021).
- Eurostat. Almost 20000 Unaccompanied Minors among Asylum Seekers Registered in the EU in 2018; Eurostat Press Office: Luxembourg, 2019. [Google Scholar]
- Roman, E.; Pastore, F.; Ponzo, I.; Harramim, N.; Lahmidani, M. Investigating Cognitive and Normative Frames of Southern and Eastern Mediterranean Stakeholders on Migration and Mobility Issues in Their Relations with the EU; Methodology and Concept Papers 2017, No.6; TEPSA: Rome, Italy, 2017. [Google Scholar]
- Nilsson, B.; Ramadan, R. Migration and Inequalities around the Mediterranean Sea; LIS Working Paper Series, No.788; Luxembourg Income Study (LIS): Luxembourg, 2020. [Google Scholar]
- Kirwin, M.; Anderson, J. Identifying the Factors Driving West African Migration; West African Papers, No 17; OECD: Paris, France, 2018. [Google Scholar]
- Pécoud, A. Death at the Border: Revisiting the Debate in Light of the Euro-Mediterranean Migration Crisis. Am. Behav. Sci. 2019, 64, 379–388. [Google Scholar] [CrossRef]
- Centre for European Policy Studies. The European Border and Coast. Guard: Addressing Migration and Asylum Challenges in the Mediterranean? Report of a CEPS Task Force; Centre for European Policy Studies: Brussels, Belgium, 2017. [Google Scholar]
- Mainwaring, C. At Europe’s Edge: Migration and Crisis in the Mediterranean. Available online: https://www.law.ox.ac.uk/research-subject-groups/centre-criminology/centreborder-criminologies/blog/2019/10/europes-edge (accessed on 12 April 2021).
- McMahon, S.; Sigona, N. Navigating the Central Mediterranean in a Time of ‘Crisis’: Disentangling Migration Governance and Migrant Journeys. Sociology 2018, 52, 497–514. [Google Scholar] [CrossRef] [Green Version]
- Ghezelbash, D.; Moreno-Lax, V.; Klein, N.; Opeskin, B. Securitization of search and rescue at sea: The response to boat migration in the mediterranean and offshore australia. Int. Comp. Law Q. 2018, 67, 315–351. [Google Scholar] [CrossRef] [Green Version]
- IOM. Four Decades of Cross-Mediterranean Undocumented Migration to Europe. A Review of the Evidence; IOM: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organisation. Understanding and Addressing Violence against Women; The World Health Organisation: Geneva, Switzerland, 2012. [Google Scholar]
- Krause, U. Violence against Women in Camps? Exploring Links between Refugee Camp Conditions and the Prevalence of Violence. In Health in Diversity—Diversity in Health; Springer: Wiesbaden, Germany, 2020; pp. 187–208. [Google Scholar]
- Nittari, G.; Sagaro, G.; Feola, A.; Scipioni, M.; Ricci, G.; Sirignano, A. First Surveillance of Violence against Women during COVID-19 Lockdown: Experience from “Niguarda” Hospital in Milan, Italy. Int. J. Environ. Res. Public Health 2021, 18, 3801. [Google Scholar] [CrossRef] [PubMed]
- Women’s Refugee Commission. More than One Million Pains: Sexual Violence against Men and Boys on the Central Mediterranean Route to Italy; Women’s Refugee Commission: New York, NY, USA, 2019. [Google Scholar]
- Barbara, G.; Collini, F.; Cattaneo, C.; Marasciuolo, L.; Chiappa, L.; Fedele, L.; Kustermann, A. Sexual violence and unwanted pregnancies in migrant women. Lancet Glob. Health 2017, 5, e396–e397. [Google Scholar] [CrossRef]
- Jiménez-Lasserrotte, M.; López-Domene, E.; Hernández-Padilla, J.; Fernández-Sola, C.; Fernández-Medina, I.; Faqyr, K.; Dobarrio-Sanz, I.; Granero-Molina, J. Understanding Violence against Women Irregular Migrants Who Arrive in Spain in Small Boats. Health 2020, 8, 299. [Google Scholar] [CrossRef]
- Guha-Sapir, D.; de Almeida, R.M.M. The Syrian Crisis: Refugees. Thematic Groups C: Contribution from the Centre for Research on the Epidemiology of Disasters; CRED: Brussels, Belgium, 2017. [Google Scholar]
- UN High Commissioner for Refugees. Desperate Journeys: Refugees and Migrants Arriving in Europe and at Europe’s Borders January–December 2018; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2019. [Google Scholar]
- UNICEF. A Deadly Journey for Children: The Central Mediterranean Migration Route. Available online: https://www.unicef.org/publications/files/EN_UNICEF_Central_Mediterranean_Migration.pdf (accessed on 15 April 2021).
- Baklacioğlu, N.O. Gendering Migration across Euro-Mediterranean Borders: Syrian refugee women on the way to the Europe. Türkiye Ortadoğu Çalışmaları Dergisi 2017, 4, 75–101. [Google Scholar] [CrossRef] [Green Version]
- Keygnaert, I.; Dialmy, A.; Manço, A.; Keygnaert, J.; Vettenburg, N.; Roelens, K.; Temmerman, M. Sexual violence and sub-Saharan migrants in Morocco: A community-based participatory assessment using respondent driven sampling. Glob. Health 2014, 10, 32. [Google Scholar] [CrossRef] [Green Version]
- Belanteri, R.A.; Hinderaker, S.G.; Wilkinson, E.; Episkopou, M.; Timire, C.; De Plecker, E.; Mabhala, M.; Takarinda, K.C.; Bergh, R.V.D. Sexual violence against migrants and asylum seekers. The experience of the MSF clinic on Lesvos Island, Greece. PLoS ONE 2020, 15, e0239187. [Google Scholar] [CrossRef]
- Freedman, J. Engendering Security at the Borders of Europe: Women Migrants and the Mediterranean Crisis. J. Refug. Stud. 2016, 29, 568–582. [Google Scholar] [CrossRef] [Green Version]
- Aranda-Fernandez, Ε.; Rolland, C.; Grippon, A.; Reboul, C.; Godard, N.; Luhmann, N. Episodes of violence suffered by migrants transiting through Libya: A criss sectional study. Confl. Health 2020, 14, 12. [Google Scholar] [CrossRef] [Green Version]
- Langer, B.; Davidovitch, N.; Nakash, O.; Nagar, M.; Lurie, I.; Shoham, S. Exposure to traumatic experiences among asylum seekers from Eritrea and Sudan during migration to Israel. Ann. Glob. Health 2015, 81, 181–182. [Google Scholar] [CrossRef]
- Padovese, V.; Farrugia, A.; Ghath, S.A.A.; Rossoni, I. Sexually transmitted infections’ epidemiology and knowledge, attitude and practice survey in a set of migrants attending the sexual health clinic in Malta. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Keygnaert, I.; Martins, M.D.R.O.; Dias, S. Assessing reported cases of sexual and gender-based violence, causes and preventive strategies, in European asylum reception facilities. Glob. Health 2018, 14, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalt, A.; Hossain, M.; Kiss, L.; Zimmerman, C. Asylum Seekers, Violence and Health: A Systematic Review of Research in High-Income Host Countries. Am. J. Public Health 2013, 103, e30–e42. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J. Sexual and gender-based violence against refugee women: A hidden aspect of the refugee crisis. Reprod. Health Matters 2016, 24, 18–26. [Google Scholar] [CrossRef]
- Amnesty International. Female Refugees Face Physical Assault, Exploitation and Sexual Harassment on their Journey through Europe. Available online: https://www.amnesty.org/en/latest/news/2016/01/female-refugees-face-physical-assault-exploitation-and-sexual-harassment-on-theirjourney-through-europe/ (accessed on 10 April 2021).
- Amnesty International. Lives Adrift. Refugees and Migrants in Peril in the Central Mediterranean; Amnesty International: London, UK, 2014. [Google Scholar]
- Zakar, R.; Zakar, M.Z.; Faist, T.; Kraemer, A. Intimate partner violence against women and its related immigration stressors in Pakistani immigrant families in Germany. SpringerPlus 2012, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pannetier, J.; Ravalihasy, A.; Desgrees du Lou, A.; Lert, F. Sexual violence against women from sub-Saharan Africa after migration to France. Popul. Soc. 2020, 577, 1–4. [Google Scholar]
- Nittari, G.; Battineni, G.; Messinetti, M.; Campanozzi, L.; Sirignano, A. Critical reflections and solutions for health problems of Italian refugees. Clin. Terap. 2021, 172, 158–162. [Google Scholar]
- Global Network of Sex. Work Projects Migrant Sex Workers; Global Network of Sex Work Projects: Edinburgh, Scotland, 2017. [Google Scholar]
- Brabcová, I.; Vacková, J.; Dvořáčková, O. Working environment and its impact on the health of immigrants. Kontakt 2014, 16, 228–235. [Google Scholar] [CrossRef]
- Mountz, A.; Loyd, J.M. Constructing the Mediterranean region: Obscuring violence in the bordering of Europe’s migration crises. ACME Int. J. Crit. Geogr. 2014, 13, 173–195. [Google Scholar]
- Piscitelli, V.; Iadicicco, A.; De Angelis, D.; Porta, D.; Cattaneo, C. Italy’s battle to identify dead migrants. Lancet Glob. Health 2016, 4, e512–e513. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Strategies and Interventions on Preventing and Responding to Violence and Injuries among Refugees and Migrants; The World Health Organisation, Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Madise, N.J.; Onyango, B. Protecting female migrants from forced sex and HIV infection. Lancet Public Health 2018, 3, e2–e3. [Google Scholar] [CrossRef]
- Reques, L.; Aranda-Fernandez, E.; Rolland, C.; Grippon, A.; Fallet, N.; Reboul, C.; Godard, N.; Luhmann, N. Episodes of violence suffered by migrants transiting through Libya: A cross-sectional study in “Médecins du Monde’s” reception and healthcare centre in Seine-Saint-Denis, France. Confl. Health 2020, 14, 12–16. [Google Scholar] [CrossRef]
- McGinn, T.; Casey, S.E. Why don’t humanitarian organizations provide safe abortion services? Confl. Health 2016, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- La Cascia, C.; Cossu, G.; Lindert, J.; Holzinger, A.; Zreik, T.; Ventriglio, A.; Bhugra, D. Migrant Women-experiences from the Mediterranean Region. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 101–108. [Google Scholar] [CrossRef]
- Crepet, A.; Rita, F.; Reid, A.; Boogaard, W.V.D.; Deiana, P.; Quaranta, G.; Barbieri, A.; Bongiorno, F.; Di Carlo, S. Mental health and trauma in asylum seekers landing in Sicily in 2015: A descriptive study of neglected invisible wounds. Confl. Health 2017, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, A. The troubled minds of migrants. Nature 2016, 538, 158–160. [Google Scholar] [CrossRef] [Green Version]
- Bianucci, R.; Charlier, P.; Perciaccante, A.; Lippi, D.; Appenzeller, O. The Ulysses syndrome: An eponym identifies a psychosomatic disorder in modern migrants. Eur. J. Intern. Med. 2017, 41, 30–32. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. INSPIRE: Seven Strategies for Ending Violence against Children; The World Health Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- United Nations Women. Preventing Violence against Women and Girls through Social Norm Change. Learning Paper from the Asia–Pacific Forum on Preventing Violence against Women and Girls: Evidence and Tools for Social Norm Change; UN Women, United Nations Population Fund, Department of Foreign Affairs and Trade: Bangkok, Thailand, 2016. [Google Scholar]
- Loescher, G.; Betts, A.; Milner, J. The United Nations High Commissioner for Refugees (UNHCR): The Politics and Practice of Refugee Protection into the 21st Century; University of Oxford: London, UK, 2008. [Google Scholar]
- Robbers, G.M.L.; Morgan, A. Programme potential for the prevention of and response to sexual violence among female refugees: A literature review. Reprod. Health Matters 2017, 25, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Deps, P.; Collin, S.M.; Aborghetti, H.P.; Charlier, P. Evidence of physical violence and torture in refugees and migrants seeking asylum in France. J. Forensic Leg. Med. 2021, 77, 102104. [Google Scholar] [CrossRef] [PubMed]
- De Schrijver, L.; Beken, T.V.; Krahé, B.; Keygnaert, I. Prevalence of Sexual Violence in Migrants, Applicants for International Protection, and Refugees in Europe: A Critical Interpretive Synthesis of the Evidence. Int. J. Environ. Res. Public Health 2018, 15, 1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Diagram of the systematic literature review regarding migrants’ sexual violence in the Mediterranean region.
Figure 1.
Diagram of the systematic literature review regarding migrants’ sexual violence in the Mediterranean region.

{kind=link}
Table 1.
Main findings based on literature review.
| Sexual Violence Incidents Take Place: | Migrants’ Sexual Violence in the Mediterranean Region |
|---|---|
| During the migratory journey to the host country |
|
| During being kept in detention centres |
|
| Once migrants have reached their destination |
|
| During the period in which a woman is subject of trafficking |
|
Table 2.
Main findings of the study and suggestions.
| Findings | Suggestions |
|---|---|
|
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hadjicharalambous, D.; Parlalis, S. Migrants’ Sexual Violence in the Mediterranean Region: A Regional Analysis. Sexes 2021, 2, 305-314. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2030024
AMA Style
Hadjicharalambous D, Parlalis S. Migrants’ Sexual Violence in the Mediterranean Region: A Regional Analysis. Sexes. 2021; 2(3):305-314. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2030024
Chicago/Turabian StyleHadjicharalambous, Demetris, and Stavros Parlalis. 2021. "Migrants’ Sexual Violence in the Mediterranean Region: A Regional Analysis" Sexes 2, no. 3: 305-314. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2030024