
Does Bed Sharing with an Infant Influence Parents’ Sexual Life? A Scoping Review in Western Countries


1
First Department of Psychiatry, Medical School, University of Athens, 157 72 Athens, Greece
2
Department of Psychology, American College of Greece, 153 42 Paraskevi, Greece
*
Author to whom correspondence should be addressed.
Sexes 2021, 2(4), 406-414; https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040032
Submission received: 20 July 2021
/
Revised: 17 September 2021
/
Accepted: 24 September 2021
/
Published: 29 September 2021
(This article belongs to the Special Issue Sexual Health Challenges in Emerging Nations, Populations, and Minorities: Research, Applications, and Recommendations)
Abstract
:Bed sharing—the sharing of a sleeping surface by parents and children—is a common, yet controversial, practice. While most research has focused on the public health aspect of this practice, much less is known regarding its effect on the marital relationship. The aim of the present study was to conduct a scoping review on the impact of parent–infant bed sharing sleeping practices on the sexual and marital relationship of couples. The qualitative synthesis of six studies on this topic suggests that overall, bed sharing does not exert a significant negative impact on family functioning; when it does, it appears to be related to incongruent parental beliefs and expectations, especially when bed sharing is not an intentional choice of sleep arrangement, and there are other confounding factors such as fatigue and psychological distress. Suggestions for future studies and clinical implications are discussed.
1. Introduction
Bed sharing—the sharing of a sleeping surface by parents and children—has been a common sleeping strategy throughout human evolution [1,2], offering the mother–infant dyad a sense of security and facilitating breastfeeding on demand [3]. In recent years, however, it has become the center of a polarized debate, due to its association with possible public health risks, particularly Sudden Infant Death Syndrome [4].
Parent–infant sleep practices differ significantly across and within various cultural contexts [5,6]. Ample evidence suggests that bed sharing is a highly common practice among parents in non-Western contexts [7,8,9], and while it is practiced less in Western countries, there is a well-documented increase in bed-sharing practices over the recent decades in traditionally non-bed-sharing countries [10], possibly reflecting a change of social attitudes regarding the importance of parent–infant contact and breastfeeding. Recent reports from the US and the UK suggest that up to 30% of parents share their bed with their young infant [10,11,12].
Bed sharing is a common choice among breastfeeding mothers, as it facilitates frequent and on-demand feedings [3,13,14]. The centrality of bed sharing in facilitating breastfeeding through skin-to-skin contact and frequent awakening throughout the night has been strongly argued by McKenna and Gettler (2016) who coined the term “breastsleeping”. Evidence from randomized controlled trials and observational studies shows that bed-sharing infants have more night arousals, more breastfeeding sessions, and shorter sleeping intervals compared to solitary sleeping babies [3,13].
1.1. Defining Types of Sleeping Arrangements
Parent–infant bed sharing refers to the practice whereby parents and child are sharing the same sleeping surface or bed, while room sharing is when the child sleeps in the same room with their parents. Bed sharing, together with room sharing, falls under the umbrella term of parent-infant co-sleeping, defined by McKenna and Volpe [14] as sleeping in close enough proximity “to permit the exchange of at least two sensory stimuli (touch, smell, movement, sight, and/or sound)”. Co-sleeping does not necessarily last for the entire night, but a portion of the night [15]. The most common form of co-sleeping is dyadic (mothers co-sleep with their babies); nevertheless, triadic co-sleeping (mother–father–infant) is not an uncommon bed sharing practice [16]. Solitary or independent sleeping, on the other hand, describes a child who sleeps separately in their own place.
The review of the current literature suggests two different profiles of parents with regards to their bed-sharing practices: the intentional and the reactive bed sharers [17]. Intentional bed sharers adopt bed sharing by choice, as such practice is consistent with their parenting principles and beliefs [18]. In contrast, reactive bed-sharers do not originally intend to share beds with their babies, but end up adopting this practice out of their need to respond to the baby’s unique needs and temperament [19]. Reactive bed sharers may be further grouped into remediators and acquiescers, depending on the amount of parents’ effort whether or not parents made meaningful attempts to keep the children in their own beds [20]. Importantly, bed sharing is a dynamic process that may change over time. For instance, reactive bed-sharing parents may eventually become intentional, as they may grow to enjoy the proximity with their baby.
1.2. Why Focus on Marital/Sexual Life of the Parents?
Most research on the topic has focused on the public health debate regarding the role of bed sharing practice on SIDS. Limited research has investigated parent–infant sleep practices during early infancy from a purely observational, psychological point of view, and few studies have investigated the impact of bed sharing practices in the marital and sexual relationship of the couple.
This gap in the literature is of great concern, given the vast and all-encompassing changes a couple undergoes during the transition to parenthood. There is a whole generation shift upon the baby’s arrival [21]. Parents, and mothers in particular, go through unprecedented changes in their roles and identities, faced with new responsibilities and roles [22]. Inevitably, the relationship with the partner also undergoes significant transition, bringing up challenges in the new parents’ sex life [23,24].
Apart from the social and contextual factors that may influence a couple’s sex life, birth-related anatomical issues may further reduce libido. A significant number of women, as high as 80%, experience dyspareunia after a traumatic or operative delivery, due to tenderness, bruising, knots of the episiotomy or laceration [21,22,23,24], decreased vaginal lubrication due to high prolactin levels that decrease estrogen levels, and decreased sexual desire due to lower androgen levels [23,25]. Breastfeeding is another issue that may influence parents’ sexual life; except from the sore nipples and the breast tenderness that may negatively affect mother’s desire, the frequent night awakenings lead to fatigue and decrease desire for sexual intimacy [23,24]. Maternal body changes may cause women to experience feelings of unattractiveness, which itself may lead to a disinterest in sexual activity. Moreover, mental health difficulties, particularly postnatal depression, may negatively impact sexual desire and cause prolonged sexual difficulties [21,24].
In view of these challenges, it is possible that prolonged bed sharing may further alienate the couple, especially if such practice is not a joint decision. There are several early accounts of the putative adverse influence of parent–infant bed sharing and co sleeping on sexual intimacy and marital satisfaction [26,27]. Among other concerns, Stein and colleagues [28] discuss the “interference with the resumption and elaboration of perinatal sexuality and intimacy”, given that “a third person in the sexual bed is at least a distraction and always a competitor for the concern, attention, and affection of one or both of the sexual partners.” However, such criticism is unclear whether it is empirically supported, given that research on this topic is scarce.
In this article, we aim to shed light on the understudied topic of the impact of bed sharing on couples’ sexual relationship. Our review seeks to combine two realities taking place in early parenthood, i.e., on the one hand the presence of the baby in the matrimonial bed, and the need for sexual intimacy among the parents on the other. Given the limited research on this topic, we decided to conduct a scoping review on the topic, focusing on bed sharing during the first two years of life. The scoping review aims to answer the research question “Does parent–infant bed sharing influence a couple’s sexual relationship?” The scoping review further aims to identify gaps in the literature, address methodological shortcomings, and make recommendations for future research.
2. Methods
2.1. Search Strategy
The study utilized the scoping review approach proposed by Arksey and O’Malley [29]. The electronic search included two databases, MEDLINE and PsycInfo. We also performed targeted searches for grey literature (i.e., difficult to locate or unpublished material) by searching (1) Google and (2) Google Scholar. From the articles retrieved in the first round of searching, additional references were identified by a manual search among the cited references. The following search terms were used: “sex”, “parenthood”, “infant” and “bed sharing” or “co sleeping.” Because previous literature did not sufficiently distinguish between bed and room sharing, the umbrella term co-sleeping was included. See Supplementary File S1 for an example of search terms used in MEDLINE.
2.2. Study Selection Process
The inclusion criteria were: (a) the article investigated bed sharing practices in young infants aged 0–3 years and (b) focused on the sexual/marital relationship among parents. All study designs were considered, including qualitative and quantitative methods. Because of the great cultural variation observed in the practice of bed sharing, we decided to focus on Western countries only. All types of articles were eligible, including dissertations and books. Articles were excluded if (a) their focus was on Sudden Infant Death Syndrome (SIDS); (b) they investigated bed sharing practices among older children. Articles for which full text was not available or were not in English were also excluded. From the articles retrieved in the first round of search, additional references were identified by a manual search among the cited references.
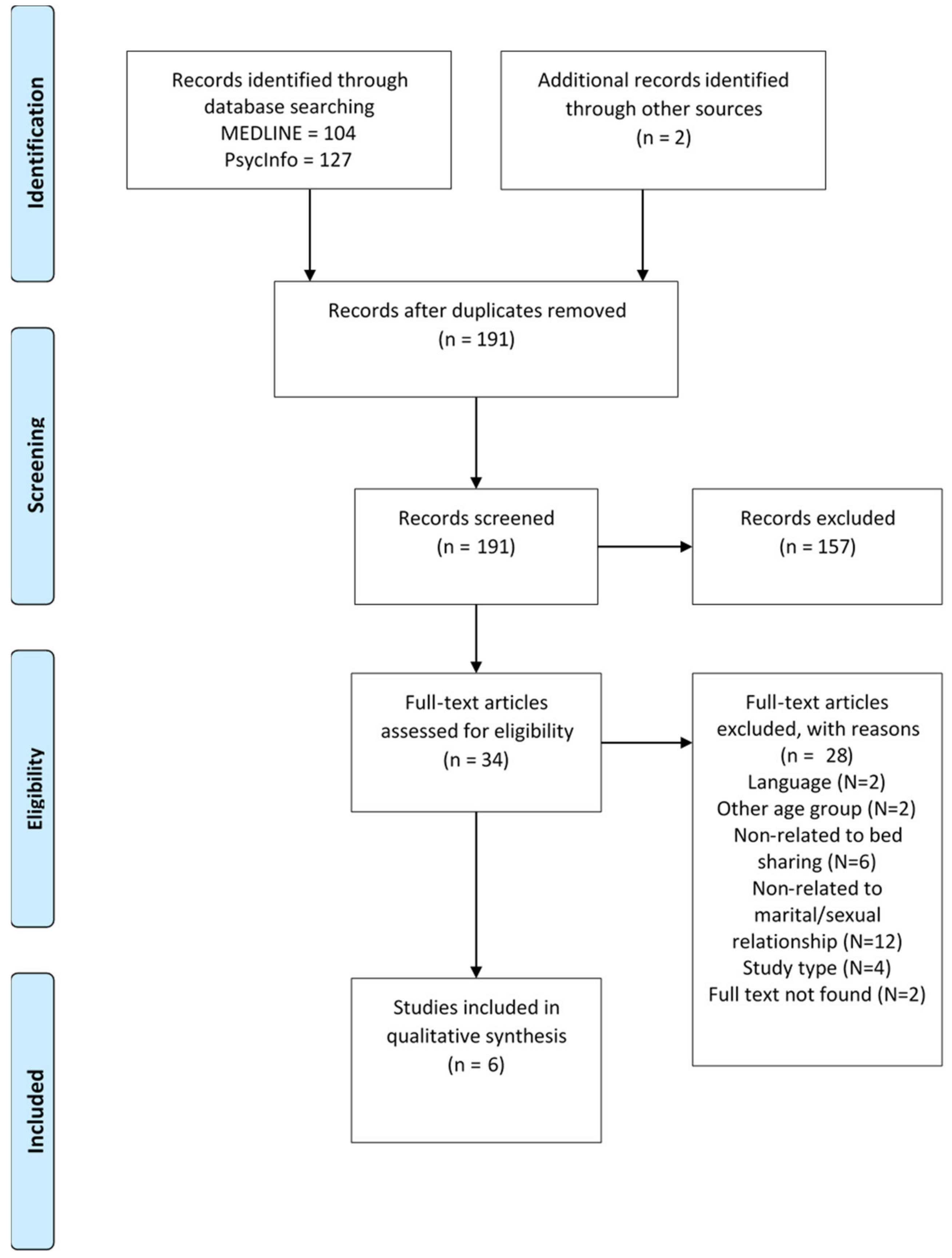
The screening process was conducted independently by the two reviewers in a two-step process: (1) quick inspection of title and abstract; and (2) inspection of the full-text articles. Discrepancies were discussed among the pair until consensus was reached; in cases where consensus was not reached, discrepancies were resolved by discussion with a third reviewer (IMZ). The study selection process is shown in Figure 1.
2.3. Data Extraction and Synthesis
A data extraction spreadsheet was devised by the two reviewers and was tested independently on a random sample of four articles and revised iteratively, as needed. The spreadsheet included the following items: (1) study characteristics (e.g., first author, year of publication); (2) characteristics related to the method (e.g., research design, measures); (3) outcomes related to marital/sexual relationship. The two investigators independently read each article and extract the relevant data. Differences in abstraction were resolved by discussion or the involvement of the third reviewer. Given that the aim of this scoping review was to conduct a rapid assessment of the current evidence base and to target topic areas for future studies, methodological quality was not formally appraised.
3. Results
Overall, six studies met the inclusion criteria and were included in this scoping review. Of these, four studies were quantitative, employing either cross-sectional or longitudinal designs, and two were qualitative, using semi-structured interviews and focus groups. Of note, two of the studies used a sample from the same survey (i.e., Study of Infants’ Emergent Sleep Trajectories; SIESTA). Studies were conducted in Australia, Canada, the United Kingdom, and the United States.
All studies defined bed sharing as the sharing of sleep surface between parents/parent and infant. Most studies classified bed sharing and sleep arrangements using standardized tools, including the Sleep Practices Questionnaire (SPQ) [30] and the Sleeping Arrangement Questionnaire (SAQ) [19], the latter of which incorporated items from of Ramos’ Family Sleep Survey [31]. The most commonly used instrument to measure marital satisfaction and sexual relationship was the Dyadic Adjustment Scale (DAS [32]), which was employed in short or full version in three quantitative studies [19,33]. The majority of the studies focused on the mothers’ report of marital and sexual relationship with their partners, except in Ball et al.’s study [16] that was conducted in fathers and in Teti et al.’s study [33], where fathers participated partly. The characteristics of the included studies are presented in Table A1 in Appendix A.
4. Discussion
Even though parent–infant sleeping arrangements are an important aspect of parenting, the impact of such practices on the marital and sexual life of new parents has received little attention. Our study aimed to address this critical gap in the literature by conducting a scoping review of the topic. Below, we discuss the major findings of the existing literature.
Overall, the published literature on this topic is scarce and methodologically heterogenous. The limited published research to date implies that bed sharing may introduce challenges in the couple’s marital relationship and sex life, yet this depends on many factors.
A relatively consistent finding across the published studies is the importance of the type of motivation driving the decision for bed-sharing practice. The literature distinguishes between bed sharing as an ideological endorsement (intentional bed sharers) or an adaptation to the baby’s needs (reactive bed sharers). It appears that marital relationship may be differentially affected by intentional versus reactive bed sharing. For instance, Messmer’s study [19] found no association between time spent bed sharing with marital satisfaction among intentional bed sharers. Reactive bed sharers, on the other hand, reported worsening of marital satisfaction as time spent bed sharing increased.
One possible explanation for this finding is that different sleep arrangements may reflect different levels of congruence with parental beliefs about infants’ sleeping routines. Intentional bed sharers choose to share beds with their infant to facilitate responses to the baby’s needs during the night, while parents who endorse solitary sleeping are mainly driven by their intention to promote their child’s independency [34]. On the other hand, reactive bed sharers may experience greater dissatisfaction and ambivalence regarding this sleep arrangement as it is less congruent to their parenting beliefs.
It is also possible that infant sleeping difficulties may be the outcome, and not the cause, of poor marital functioning. In accordance with the emotional security hypothesis [35], child adjustment difficulties arise as a response to insecurity in the family subsystem. New parents struggling to transition to their new role, who receive little emotional and practical support and who develop a hostile and non-supportive marital interaction may find it difficult to respond to their baby’s needs with enjoyment and emotional attunement, which may further exacerbate the infant’s quality of sleep [36].
Research has emphasized mothers’ experiences. The few studies having included fathers in their samples suggests that fathers respond positively to bed sharing, even when it occurs unexpectedly, and do not experience sharing beds as an obstacle or intrusion on their marital relationship [16].
An important point for consideration is that bed sharing is not a static variable, but rather changes and evolves over time. For instance, in the longitudinal study by Teti et al. [37] a significant number of families shifted to solitary sleeping arrangements from 1 to 6 months. Additionally, bed sharing is not an exclusive sleep practice. In the study by Messmer et al. [19], most participants used bed sharing in combination with room sharing or independent, solitary sleep. These findings point towards the importance of standardizing the operationalization and measurement of co-sleeping and bed sharing practices, allowing for a complex and dynamic assessment that is tracked and monitored longitudinally, over time.
It is possible that the putative relationship between bed sharing and marital relationship is moderated by other third variables, particularly maternal psychological functioning and postpartum depression more specifically. Research evidence suggests that mothers with elevated depressive symptoms at postpartum are more likely to share their bed with their infants compared to the mothers with non-clinical depressive symptoms [38]. Given the well-established link between depressive symptoms and decreased libido and sexual dysfunction, it is possible that disruptions in the marital function of the couple are driven by depression symptoms, which are common in postpartum women [39].
To our knowledge, this is the first study ever to review in a systematic way the existing literature on the impact of parent–infant bed sharing practices on marital functioning. Our flexible inclusion criteria maximized the number of studies to be included for review with varied methodological designs. We paid particular attention to the operationalization and measurement of sleeping arrangements, given the significant methodological heterogeneity of published reports, which we hope could guide future research studies in employing valid instruments. Notwithstanding these strengths, there are several limitations of the present review that should be mentioned. The limited amount of published data on this subject did not allow for a meta-analytic study of the effect of sleeping arrangements on marital functioning. Therefore, the results of this review should be interpreted with caution. We only included studies conducted in Western contexts, with the exception of one study that included a subsample of Aboriginal women. Finally, studies were conducted in traditional heterosexual and non-minoritized families.
Future research studies need to consider longitudinal designs that employ sensitive and valid instruments for measuring bed sharing. The appropriate distinction between intentional vs. reactive bed sharing is of great importance; including a measure of perceived infant sleep problems which may help distinguish between those parents who choose ideologically to share beds or resort to bed sharing because of their infant’s sleeping difficulties [40]. Additional confounding variables should be assessed, including parental psychopathology, levels of fatigue, and racial and ethnic characteristics. Studies should also consider adopting qualitative designs to allow a more in-depth understanding of the impact of co-sleeping on new parents’ marital and sexual relationship.
The study findings have some important clinical implications. Health professionals need to be prepared and vigilant to identify any ruptures in a couple’s relationship. Especially, those professionals who offer home services should pay particular attention to parent–infant sleeping practices and observe where and how the baby and the baby’s parents sleep. Research shows that parents appreciate balanced and non-judgmental parenting advice offered to expecting parents during pregnancy and throughout the first years of parenthood [41]. Professionals should encourage the couple to discuss their marital and sexual challenges and should serve as facilitators, offering, advising, and suggesting alternatives. Professionals should listen and encourage parents to talk about their needs, feelings, and worries, as talk is always therapeutic [42]. Psychoeducation on the physiological and psychological changes that accompany the first months of the transition to motherhood may be of great benefit to new parents. Women and their partners with significant distress comprise a high-risk group in need of specialized interventions that aim to strengthen the marital and co-parenting relationship by clarifying expectations and beliefs and increasing parental agreement regarding infant sleeping arrangements [33].
5. Conclusions
Undoubtedly, parenting is accompanied by many challenges and key changes in a couple’s life. A couple’s marital relationship and sex life is redefined during the transition to parenthood. Through this lens, it is possible that parenting practices, such as sleeping arrangements, may influence a couple’s marital relationship and sexual satisfaction. That said, the qualitative synthesis of existing studies on this topic suggests that overall, bed sharing does not exert significant negative impact on family functioning; and, when it does, it appears to be related to parental beliefs and incongruent expectations, and other confounding factors such as fatigue and psychological distress. In this light, the sex life of young parents needs further study, honest discussion, personalized approach, and specialized interventions tailored to the unique needs of new parents. Our findings are limited by the small number of published studies on the topic, reflecting the need for further investigation on this complex and multifaceted topic, which often stirs up conflict among professionals or parents.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/sexes2040032/s1, File S1: Supplemental file: Search Terms in Pubmed.
Author Contributions
Conceptualization, methodology and investigation, all authors; writing-original draft preparation, E.V.; writing-review and editing, C.E.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
Table A1.
Characteristics of included studies.
| Authors | Publication Year | Country | Sample | Design | Definition of Bed Sharing | Measurements | Measurements on Marital Relationship/Satisfaction/Sexual Life etc. |
|---|---|---|---|---|---|---|---|
| Ball, Hooker, and Kelly | 2000 | United Kingdom | 36 sets of parents | Qualitative, prospective, | Study focused on triadic co-sleeping (no a priori definition was provided by the authors) | Semi-structured interview at pre-birth on expectations/intentions regarding sleep arrangements; semi-structured interview at 10 weeks following birth assessing implemented sleeping arrangements | Semi-structured interview at 10 weeks following birth assessing effect of the baby on the parents’ relationship and family |
| Germo, Chang, Keller, and Goldberg | 2007 | United States | 100 mothers and 38 fathers of pre-school aged children | Quantitative, cross-sectional | Defined as (a) solitary sleepers; (b) early bed sharers who slept in the parents’ bed for part or all of the night prior to 12 months of age, (c) early co-sleepers who either slept in the parents’ room exclusively or alternated between parents’ room and their bed, and (d) reactive co-sleepers who began co-sleeping after the first year or were early bed sharers or co-sleepers who returned to the parent bedroom after an extended period of solitary sleep | Sleep Practices Questionnaire (SPQ; [18]) completed at 6, 12, 24, and 36 months for mothers and 6, and 12 months for fathers | For mothers, marital intimacy was assessed using an adapted version of the Personal Assessment of Intimacy in Relationships [43]; for fathers, an adapted version of Braiker and Kelley’s four-factor intimate relationship scale [44]. |
| Messmer et al. [19] | 2012 | Canada | 81 bed sharing mothers who had given birth to their first child between 6 and 12 months prior to the study | Quantitative, cross-sectional | Defined as mothers who responded positively to the item: “Do you ever, or did you in the past, share your bed with your baby either for the whole night or part of the night?” | Questionnaire designed for this study based on Ramos’ Family Sleep Survey [31] | Marital relationship was assessed by the Dyadic Adjustment Scale (DAS) [32] Sexual satisfaction was measured by a specifically designed question assessed on a 5-point scale |
| Teti et al. [37] | 2015 | United States | 149 mothers examined at and across 1 and 6 months of infant age | Quantitative, prospective | Defined as infant having slept in the same bed with their parents. Other classifications were solitary sleep, room sharing, and combination | Sleep Practices Questionnaire (SPQ; [18]) completed at the 1st and 6th month | Marital Adjustment Test (MAT; [45]) Dyadic Adjustment Scale (DAS) [32] |
| Teti et al. | 2016 | United States | 139 families at 1, 3, 6, 9, and 12 months of infant age | Quantitative, prospective | Aggregated data across all five age points created five sleep arrangements: (1) consistent solitary sleeping (from 1–12 months); (2) early switch to solitary sleep (infant switched to solitary sleep by 3 or 6 months); (3) late switch to solitary sleep (infant switched to solitary sleep by 9 or 12 months); (4) consistent co-sleeping (room sharing or bed sharing from 1 through 12 months); and (5) inconsistent co-sleeping (non-specific sleep pattern across the first year) | Sleep Practices Questionnaire (SPQ; [18]) completed at the 1st and 6th month | Marital Adjustment Test (MAT; [45]) Dyadic Adjustment Scale (DAS) [32] |
| Dodd and Jackiewicz [46] | 2015 | Australia | 24 mothers (Aboriginal and non-Aboriginal) who had birthed within the previous 2–12 months | Qualitative, cross-sectional | Defined as either one or both parents sleeping with the infant on the bed or on a couch intentionally or accidently | Semi-structured interview and focus groups discussions | Semi-structured interview and focus groups discussions on sexual and emotional intimacy (partner’s fear of losing it) |
References
- Thoman, E.B. Co-sleeping, an ancient practice: Issues of the past and present, and possibilities for the future. Sleep Med. Rev. 2006, 10, 407–417. [Google Scholar] [CrossRef]
- Ball, H.L.; Tomori, C.; McKenna, J.J. Toward an Integrated Anthropology of Infant Sleep. Am. Anthropol. 2019, 121, 595–612. [Google Scholar] [CrossRef]
- Mileva-Seitz, V.R.; Bakermans-Kranenburg, M.J.; Battaini, C.; Luijk, M.P.C.M. Parent-child bed-sharing: The good, the bad, and the burden of evidence. Sleep Med. Rev. 2017, 32, 4–27. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. The Changing Concept of Sudden Infant Death Syndrome: Diagnostic Coding Shifts, Controversies Regarding the Sleeping Environment, and New Variables to Consider in Reducing Risk. Pediatrics 2005, 116, 1245–1255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luijk, M.P.C.M.; Mileva-Seitz, V.R.; Jansen, P.W.; van IJzendoorn, M.H.; Jaddoe, V.W.V.; Raat, H.; Hofman, A.; Verhulst, F.C.; Tiemeier, H. Ethnic differences in prevalence and determinants of mother–child bed-sharing in early childhood. Sleep Med. 2013, 14, 1092–1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morelli, G.A.; Rogoff, B.; Oppenheim, D.; Goldsmith, D. Cultural variation in infants’ sleeping arrangements: Questions of independence. Dev. Psychol. 1992, 28, 604–613. [Google Scholar] [CrossRef]
- Nelson, E.A.; Taylor, B.; Jenik, A.; Vance, J.; Walmsley, K.; Pollard, K.; Freemantle, M.; Ewing, D.; Einspieler, C.; Engele, H.; et al. International Child Care Practices Study: Infant sleeping environment. Early Hum. Dev. 2001, 62, 43–55. [Google Scholar] [CrossRef]
- Tahhan, D.A. Depth and Space in Sleep: Intimacy, Touch and the Body in Japanese Co-sleeping Rituals. Body Soc. 2008, 14, 37–56. [Google Scholar] [CrossRef]
- Chung, S.; An, H. Cultural Issues of Co-Sleeping in Korea. Sleep Med. Res. 2014, 5, 37–42. [Google Scholar] [CrossRef]
- Willinger, M.; Ko, C.-W.; Hoffman, H.J.; Kessler, R.C.; Corwin, M.J. Trends in Infant Bed Sharing in the United States, 1993-2000. Arch. Pediatr. Adolesc. Med. 2003, 157, 43. [Google Scholar] [CrossRef] [Green Version]
- Blair, P.S.; Ball, H.L. The prevalence and characteristics associated with parent-infant bed-sharing in England. Arch. Dis. Child. 2004, 89, 1106–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, L.A.; Geller, N.L.; Kellams, A.L.; Colson, E.R.; Rybin, D.V.; Heeren, T.; Corwin, M.J. Infant Sleep Location and Breastfeeding Practices in the United States, 2011–2014. Acad. Pediatr. 2016, 16, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Mosko, S.; Richard, C.; McKenna, J. Maternal Sleep and Arousals During Bedsharing With Infants. Sleep 1997, 20, 142–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, J.J.; Volpe, L.E. Sleeping with baby: An internet-based sampling of parental experiences, choices, perceptions, and interpretations in a western industrialized context. Infant Child Dev. 2007, 16, 359–385. [Google Scholar] [CrossRef]
- Ball, H.L. Triadic bed-sharing and infant temperature. Child. Care. Health Dev. 2002, 28, 55–58. [Google Scholar] [CrossRef] [PubMed]
- Ball, H.L.; Hooker, E.; Kelly, P.J. Parent-Infant Co-Sleeping: Fathers’ Roles and Perspectives. Infant Child Dev. 2000, 9, 67–74. [Google Scholar] [CrossRef]
- Ramos, K.D. Intentional versus reactive cosleeping. Sleep Res. Online 2003, 5, 141–147. [Google Scholar]
- Goldberg, W.A.; Keller, M.A. Co-sleeping during infancy and early childhood: Key findings and future directions. Infant Child Dev. 2007, 16, 457–469. [Google Scholar] [CrossRef]
- Messmer, R.; Miller, L.D.; Yu, C.M. The Relationship Between Parent-Infant Bed Sharing and Marital Satisfaction for Mothers of Infants. Fam. Relat. 2012, 61, 798–810. [Google Scholar] [CrossRef]
- Stewart, S.D.; Riegle, A.L. Musical Beds: The “Typical” Night of Parents and Children Who Co-Sleep; 2014 Working Paper Series; Bowling Green State University’s Center for Family and Demographic Research: Bowling Green, OH, USA, 2014. [Google Scholar]
- Walton, I. Wait six weeks. In Sexuality and Motherhood; Books For Midwives: Cheshire, UK, 1994; pp. 97–107. [Google Scholar]
- Serrano Drozdowskyj, E.; Gimeno Castro, E.; Trigo López, E.; Bárcenas Taland, I.; Chiclana Actis, C. Factors Influencing Couples’ Sexuality in the Puerperium: A Systematic Review. Sex. Med. Rev. 2020, 8, 38–47. [Google Scholar] [CrossRef]
- Leeman, L.M.; Rogers, R.G. Sex After Childbirth. Obstet. Gynecol. 2012, 119, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Škodi Zakošek, T. Sexual Activity during Pregnancy in Childbirth and after Childbirth. In Sexology in Midwifery; InTech: London, UK, 2015. [Google Scholar]
- Glazener, C.M.A. Sexual function after childbirth: Women’s experiences, persistent morbidity and lack of professional recognition. BJOG An Int. J. Obstet. Gynaecol. 1997, 104, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Spock, B. Baby and Child Care; Pocket Books: New York, NY, USA, 1976. [Google Scholar]
- Weissbluth, M. Healthy Sleep Habits, Happy Child: A Step-by-Step Program for a Good Night’s Sleep; Ballantine Books: New York, NY, 1999. [Google Scholar]
- Stein, M.T.; Colarusso, C.A.; McKenna, J.T.; Powers, N.G. Cosleeping (bedsharing) among infants and toddlers. J. Dev. Behav. Pediatr. 1997, 18, 408–412. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.A.; Goldberg, W.A. Co-sleeping: Help or hindrance for young children’s independence? Infant Child Dev. 2004, 13, 369–388. [Google Scholar] [CrossRef]
- Ramos, K.D. Parent-Child Co-Sleeping in the Context of Parental Belief Systems; University of Missouri-Columbia: Columbia, MO, USA, 2001. [Google Scholar]
- Spanier, G.B. Measuring Dyadic Adjustment: New Scales for Assessing the Quality of Marriage and Similar Dyads. J. Marriage Fam. 1976, 38, 15. [Google Scholar] [CrossRef]
- Teti, D.M.; Shimizu, M.; Crosby, B.; Kim, B.-R. Sleep arrangements, parent–infant sleep during the first year, and family functioning. Dev. Psychol. 2016, 52, 1169–1181. [Google Scholar] [CrossRef]
- Germo, G.R.; Chang, E.S.; Keller, M.A.; Goldberg, W.A. Child sleep arrangements and family life: Perspectives from mothers and fathers. Infant Child Dev. 2007, 16, 433–456. [Google Scholar] [CrossRef]
- Davies, P.T.; Cummings, E.M. Marital conflict and child adjustment: An emotional security hypothesis. Psychol. Bull. 1994, 116, 387–411. [Google Scholar] [CrossRef]
- Rhoades, K.A.; Leve, L.D.; Harold, G.T.; Mannering, A.M.; Neiderhiser, J.M.; Shaw, D.S.; Natsuaki, M.N.; Reiss, D. Marital hostility and child sleep problems: Direct and indirect associations via hostile parenting. J. Fam. Psychol. 2012, 26, 488–498. [Google Scholar] [CrossRef] [Green Version]
- Teti, D.M.; Crosby, B.; McDaniel, B.T.; Shimizu, M.; Whitesell, C.J. Marital And Emotional Adjustment In Mothers And Infant Sleep Arrangements During The First Six Months. Monogr. Soc. Res. Child Dev. 2015, 80, 160–176. [Google Scholar] [CrossRef]
- Teti, D.M.; Crosby, B. Maternal Depressive Symptoms, Dysfunctional Cognitions, and Infant Night Waking: The Role of Maternal Nighttime Behavior. Child Dev. 2012, 83, 939–953. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W. Postpartum depression: What we know. J. Clin. Psychol. 2009, 65, 1258–1269. [Google Scholar] [CrossRef]
- Ramos, K.D.; Youngclarke, D.; Anderson, J.E. Parental perceptions of sleep problems among co-sleeping and solitary sleeping children. Infant Child Dev. 2007, 16, 417–431. [Google Scholar] [CrossRef]
- Hatton, R.E.M.; Gardani, M. Maternal perceptions of advice on sleep in young children: How, what, and when? Br. J. Health Psychol. 2018, 23, 476–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daws, D.; Rementeria, A. Finding Your Way with Your Baby—The Emotional Life of Parents and Babies; Routledge: Oxfordshire, UK, 2015. [Google Scholar]
- Schaefer, M.T.; Olson, D.H. Assessing Intimacy: The Pair Inventory*. J. Marital Fam. Ther. 1981, 7, 47–60. [Google Scholar] [CrossRef]
- Braiker, H.; Kelley, H. Conflict in the development of close relationships. In Social Exchange in Developing Relationships; Burgess, R., Huston, T., Eds.; Academic Press: Cambridge, MA, USA, 1979; pp. 135–168. [Google Scholar]
- Locke, H.J.; Wallace, K.M. Short marital adjustment and prediction tests: Their reliability and validity. Marriage Fam. Living 1959, 21, 251–255. [Google Scholar] [CrossRef]
- Dodd, J.; Jackiewicz, T. The negotiations of involved fathers and intensive mothers around shared-bed sleeping with infants (co-sleeping). Heal. Sociol. Rev. 2015, 24, 213–225. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart of the scoping review process.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Vousoura, E.; Ekizoglou, C. Does Bed Sharing with an Infant Influence Parents’ Sexual Life? A Scoping Review in Western Countries. Sexes 2021, 2, 406-414. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040032
AMA Style
Vousoura E, Ekizoglou C. Does Bed Sharing with an Infant Influence Parents’ Sexual Life? A Scoping Review in Western Countries. Sexes. 2021; 2(4):406-414. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040032
Chicago/Turabian StyleVousoura, Eleni, and Chryssa Ekizoglou. 2021. "Does Bed Sharing with an Infant Influence Parents’ Sexual Life? A Scoping Review in Western Countries" Sexes 2, no. 4: 406-414. https://0-doi-org.brum.beds.ac.uk/10.3390/sexes2040032