The Impact of Participants’ Anthropometry on Muscle Activation Levels While Interacting with the Level of Expertise, Task Type, and Single Muscles

 ,
,  ,
,
Abstract
:1. Introduction
- To investigate the impact of carpenters’ body dimensions on their muscle activation levels;
- To examine the impact of carpenters’ body dimensions on novice versus expert carpenter’s muscle activation levels;
- To check the impact of carpenters’ body dimensions on the different muscle usages of carpenters;
- To test the impact of carpenters’ body dimensions on their muscle activation levels during two simulated tasks.
2. Materials and Methods
2.1. Data Collection Procedure and Participants
2.2. Experimental Design
2.3. Data Analysis Method
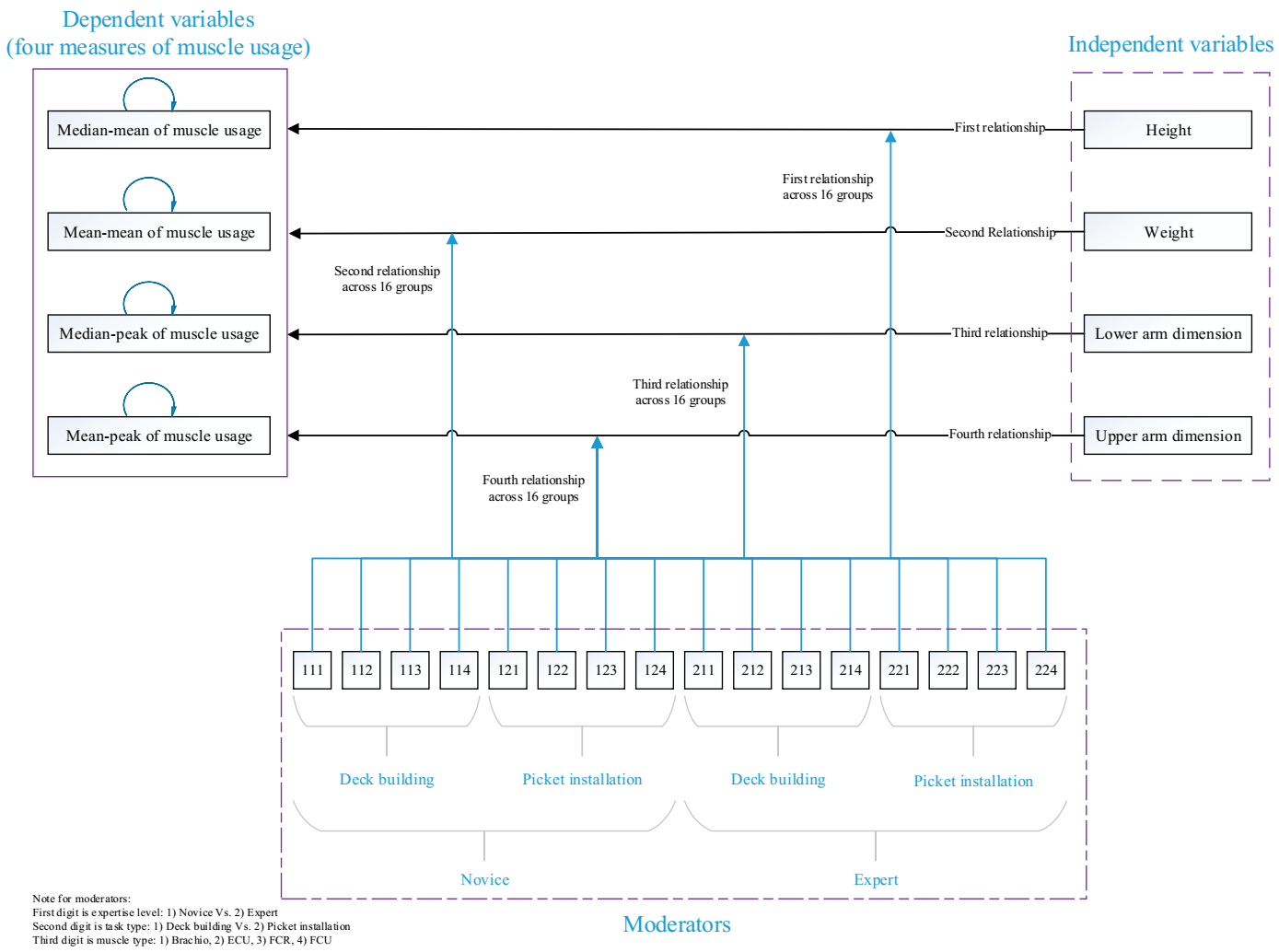
2.4. The Proposed Theoretical Model
2.5. Research Variables and Measures
2.5.1. Independent Variables
2.5.2. Dependent Variables
2.5.3. Moderators
Participant Experience Level
- Have three or more years of construction work experience.
- Have not missed more than three months of work in the previous year.
- Two of their three years of experience must have been as a carpenter.
- Have a minimal injury history, and their work time loss must be less than four days missed per year due to work-induced discomfort/injuries.
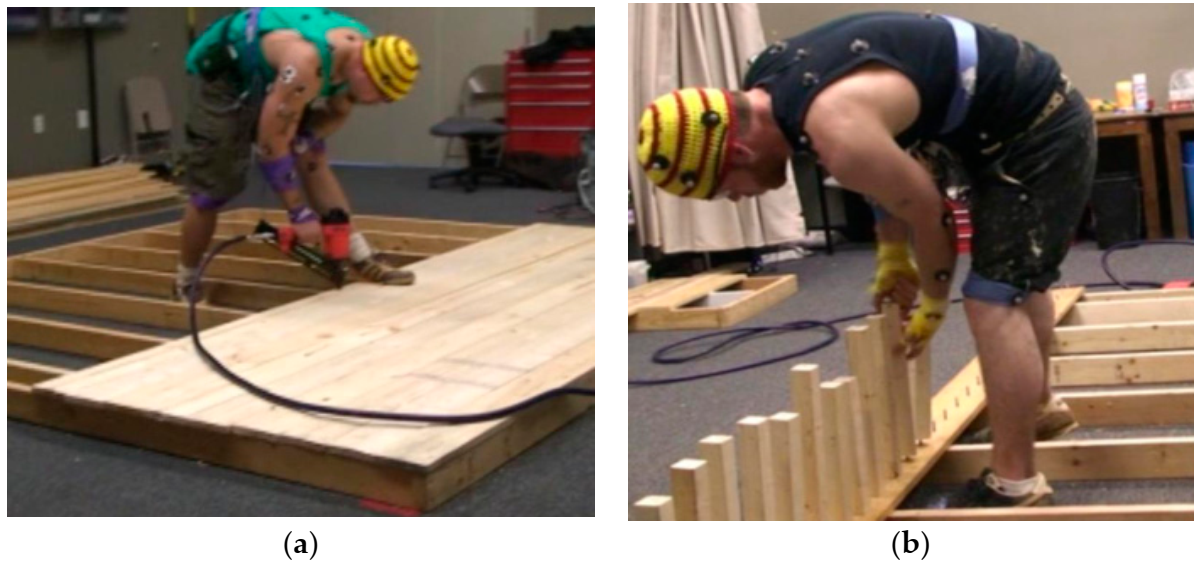
Work Task Simulations
Four Arm Muscles and SEMG Measurement
3. Results
3.1. Findings of the First Hypothesis
- The relationship between height and muscle activation level is moderated by participants’ expertise. Height only influences the FCR muscle activation level in the expert sample, while all four muscle activation levels of the novice participants are influenced by height. The reverse impact of height on muscle activity is stronger for novices than experts.
- The relationship between height and muscle activation level is not moderated by the simulation task. The impact of height on the muscle activation level in the deck-building task is not significantly different from the picket installation task. On the other hand, BR and ECU usage are better predictors of the deck building task than the picket installation task, while FCR and FCU are better predictors of the picket installation task than the deck building task.
- The relationship between height and muscle activation level is not moderated by the type of the single muscle. However, the impact of height on the muscle activation level is not significantly different across single muscles, and this relationship is stronger for FCR and BR usage.
3.2. Findings of the Second Hypothesis
- The relationship between weight and muscle activation level is moderated by participants’ expertise. The overall relationship between weight and muscle activation level is different for experts and novices, especially with regard to the ECU muscle.
- The relationship between weight and muscle activation level is not moderated by the simulation task. The impact of weight on muscle activation level in the deck-building task is not significantly different from the picket installation task; however, this relationship is stronger for the picket installation than the deck building task.
- The relationship between weight and muscle activation level is moderated by the type of the single muscle. The impact of weight on the muscle activation level is significantly different across single muscles, and this moderation effect is stronger for the FCR and ECU muscles, and is the weakest for the FCU muscle.
3.3. Findings of the Third Hypothesis
- The relationship between the lower arm dimensions and the muscle activation level is moderated by the participants’ expertise. The overall relationship between the lower arm and the muscle activation level is stronger for novices than experts.
- The relationship between the lower arm dimensions and the muscle activation level is not moderated by the simulation task. The impact of the lower arm on the muscle activation level in the picket installation task is stronger than in the deck-building task, especially for the FCU and BR muscles.
- The relationship between the lower arm dimensions and the muscle activation level is moderated by the type of the single muscle. The impact of lower-arm dimensions on the muscle activation level is significantly different among single muscles, especially among experts.
3.4. Findings of the Fourth Hypothesis
4. Discussion
4.1. Consistency with the Literature
4.2. Hypothesis 1 Interpretation
4.3. Hypothesis 2 Interpretation
4.4. Hypothesis 3 Interpretation
4.5. Hypothesis 4 Interpretation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thatcher, A. Green ergonomics: Definition and scope. Ergonomics 2013, 56, 389–398. [Google Scholar] [CrossRef] [PubMed]
- Wahlström, J. Ergonomics, musculoskeletal disorders and computer work. Occup. Med. 2005, 55, 168–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagberg, M.; Silverstein, B.; Wells, R.; Smith, M.J.; Hendrich, W.H.; Carayon, P.; Perusse, M. Work Related Musculoskeletal Disorders (WMSDs): A Reference Book for Prevention; Taylor & Francis: London, UK, 1995. [Google Scholar]
- Bongers, P.M.; Kremer, A.M.; Laak, J.T. Are psychosocial factors, risk factors for symptoms and signs of the shoulder, elbow, or hand/wrist? A review of the epidemiological literature. Am. J. Ind. Med. 2002, 41, 315–342. [Google Scholar] [CrossRef] [PubMed]
- Eaves, S.; Gyi, D.E.; Gibb, A.G. Building healthy construction workers: Their views on health, wellbeing and better workplace design. Appl. Ergon. 2016, 54, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Data USA. Workforce. 2020. Available online: https://datausa.io/profile/naics/construction-group#:~:text=The%20Bureau%20of%20Labor%20Statistics,9.07M%20people%20in%202018 (accessed on 28 July 2020).
- Jones, K. Increase in Number of Fatal and Nonfatal Injuries for Construction Workers in 2018. December 2019. Available online: https://www.constructconnect.com/blog/increase-in-number-of-fatal-and-nonfatal-injuries-for-construction-workers-in-2018#:~:text=The%20construction%20industry%20represented%2019,industry%20worker%20deaths%20in%202018.&text=The%20number%20of%20nonfatal%20injuries,2017%20to%203.0%20in%202018 (accessed on 28 July 2020).
- Jones, K. Construction Leads All Industries in Total Worker. December 2016. Available online: https://www.constructconnect.com/blog/construction-leads-industries-worker-deaths (accessed on 28 July 2020).
- Lemasters, G.K.; Atterbury, M.R.; Booth-Jones, A.D.; Bhattacharya, A.; Ollila-Glenn, N.; Forrester, C.; Forst, L. Prevalence of work related musculoskeletal disorders in active union carpenters. Occup. Environ. Med. 1998, 55, 421–427. [Google Scholar] [CrossRef] [Green Version]
- Reddy, G.M.; Nisha, B.; Prabhushankar, T.G.; Vishwambhar, V. Musculoskeletal morbidity among construction workers: A cross-sectional community-based study. Indian J. Occup. Environ. Med. 2016, 20, 144. [Google Scholar] [CrossRef]
- Cook, T.M.; Rosecrance, J.C.; Zimmermann, C.L. Work-related musculoskeletal disorders in bricklaying: A symptom and job factors survey and guidelines for improvements. Appl. Occup. Environ. Hyg. 1996, 11, 1335–1339. [Google Scholar] [CrossRef]
- Carson, R.G.; Riek, S. Changes in muscle recruitment patterns during skill acquisition. Exp. Brain Res. 2001, 138, 71–87. [Google Scholar] [CrossRef]
- Gabriel, D.A. Changes in kinematic and EMG variability while practicing a maximal performance task. J. Electromyogr. Kinesiol. 2002, 12, 407–412. [Google Scholar] [CrossRef]
- Babski-Reeves, K.; Govindu, K.; Close, D.; Littlejohn, R. Muscular loading during simulated carpentry tasks. In Proceedings of the 2010 Industrial Engineering Research Conference, Cancun, Mexico, 6−9 June 2010; Institute of Industrial and Systems Engineers: Cancun, Mexico, 2010; p. 1. [Google Scholar]
- Govindu, N.K.; Babski-Reeves, K. Quantifying Differences in Shoulder Muscular Exertions during Simulated Carpentry Tasks. In Proceedings of the 2012 Industrial and Systems Engineering Research Conference, Orlando, FL, USA, 19–23 May 2012; p. 1. [Google Scholar]
- Ganon, M.; Plamondon, A.; Gravel, D.; Lortie, M. Knee movement strategies differentiate expert from novice workers in asymmetrical manual materials handling. J. Biomech. 1996, 29, 1445–1453. [Google Scholar] [CrossRef]
- Salunke, M.P.; Kallurkar, S. Identifying Anthropometric Parameters Considered for the Improvement in Ergonomic Design of Classroom Furniture. Int. J. Ind. Eng. 2015, 6, 1–13. [Google Scholar]
- Sepehri, S.; Habibi, A.H.; Shakerian, S. The relationship between ergonomic chair and musculoskeletal disorders in north of Khuzestan’s students. Eur. J. Exp. Biol. 2013, 3, 181–187. [Google Scholar]
- Del Prado-Lu, J.L. Anthropometric measurement of Filipino manufacturing workers. Int. J. Ind. Ergon. 2007, 37, 497–503. [Google Scholar] [CrossRef]
- Gurney, B.; Mermier, C.; Robergs, R.; Gibson, A.; Rivero, D. Effects of limb-length discrepancy on gait economy and lower-extremity muscle activity in older adults. JBJS 2001, 83, 907–915. [Google Scholar] [CrossRef]
- Kern, D.S.; Semmler, J.G.; Enoka, R.M. Long-term activity in upper-and lower-limb muscles of humans. J. Appl. Physiol. 2001, 91, 2224–2232. [Google Scholar] [CrossRef] [Green Version]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand. J. Work Environ. Health 1990, 16 (Suppl. S1), 55–58. [Google Scholar] [CrossRef]
- Authier, M.; Lortie, M.; Gagnon, M. Manual handling techniques: Comparing novices and experts. Int. J. Ind. Ergon. 1996, 17, 419–429. [Google Scholar] [CrossRef]
- Gagnon, M. The efficacy of training for three manual handling strategies based on the observation of expert and novice workers. Clin. Biomech. 2003, 18, 601–611. [Google Scholar] [CrossRef]
- Perotto, A.O.; Delagi, E.F.; Iazzetti, J.; Morrison, D. Anatomical Guide for the Electromyographer: The Limbs and Trunk; Charles C Thomas: Springfield, IL, USA, 1994. [Google Scholar]
- Soderberg, G. Recording techniques. In Selected Topics in Surface Electromyography for Use in the Occupational Setting: Expert Perspectives; Soderberg, G., Ed.; US Department of Health and Human Services/Public Health Service, CDC/NIOSH, US Government Printing Office: Washington, DC, USA, 1992; pp. 22–41. [Google Scholar]
- Jamar Adjustable Dynamometer. Jamar Adjustable Dynamometer, Asimow Engineering Co. 2020. Available online: https://www.worthpoint.com/worthopedia/jamar-adjustable-dynamometer-asimow-416827979 (accessed on 8 April 2020).
- Juul-Kristensen, B.; Fallentin, N.; Hansson, G.Å.; Madeleine, P.; Andersen, J.H.; Ekdahl, C. Physical workload during manual and mechanical deboning of poultry. Int. J. Ind. Ergon. 2002, 29, 107–115. [Google Scholar] [CrossRef]
- Granata, K.P.; Marras, W.S.; Davis, K.G. Variation in spinal load and trunk dynamics during repeated lifting exertions. Clin. Biomech. 1999, 14, 367–375. [Google Scholar] [CrossRef]
- Marras, W.S.; Karwowski, W. Fundamentals and Assessment Tools for Occupational Ergonomics; CRC: Boca Raton, FL, USA, 2006. [Google Scholar]
- Hodder, J.N.; MacKinnon, S.N.; Ralhan, A.; Keir, P.J. Effects of training and experience on patient transfer biomechanics. Int. J. Ind. Ergon. 2010, 40, 282–288. [Google Scholar] [CrossRef]
- Callan, D.E.; Naito, E. Neural processes distinguishing elite from expert and novice athletes. Cogn. Behav. Neurol. 2014, 27, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Woods, E.A.; Hernandez, A.E.; Wagner, V.E.; Beilock, S.L. Expert athletes activate somatosensory and motor planning regions of the brain when passively listening to familiar sports sounds. Brain Cogn. 2014, 87, 122–133. [Google Scholar] [CrossRef]
- Ghasemi, A.; Momeni, M.; Rezaee, M.; Gholami, A. The difference in visual skills between expert versus novice soccer referees. J. Hum. Kinet. 2009, 22, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Govindu, N.K.; Littlejohn, R.; Close, D.; Babski-Reeves, K. Quantifying Differences in Muscular Exertion Levels during Simulated Carpentry Tasks. In Proceedings of the 2011 Industrial Engineering Research Conference, Reno, NV, USA, 21–25 May 2011; Institute of Industrial and Systems Engineers (IISE): Reno, NV, USA, 2011; p. 1. [Google Scholar]
- Chen, Y.L.; Lee, Y.C.; Chen, C.J. Differences in lifting strength profiles between experienced workers and novices at various exertion heights. Int. J. Ind. Ergon. 2011, 41, 53–58. [Google Scholar] [CrossRef]
- Min, S.N.; Kim, J.Y.; Parnianpour, M. The effects of experience and the presence of a scaffold handrail on postural and spinal stability in construction workers. Int. J. Occup. Saf. Ergon. 2014, 20, 491–502. [Google Scholar] [CrossRef]
- Hogrel, J.-Y.; Decostre, V.; Alberti, C.; Canal, A.; Ollivier, G.; Josserand, E.; Taouil, I.; Simon, D. Stature is an essential predictor of muscle strength in children. BMC Musculoskelet. Disord. 2012, 13, 176. [Google Scholar] [CrossRef]
- Niempoog, S.; Siripakarn, Y.; Suntharapa, T. An estimation of grip strength during puberty. J. Med. Assoc. Thail. 2007, 90, 699. [Google Scholar]
- Jürimäe, T.; Hurbo, T.; Jürimäe, J. Relationship of handgrip strength with anthropometric and body composition variables in prepubertal children. Homo 2009, 60, 225–238. [Google Scholar] [CrossRef]
- Era, P.; Rantanen, T.; Avlund, K.; Gause-Nilsson, I.; Heikkinen, E.; Schroll, M.; Steen, B.; Suominen, H. Maximal isometric muscle strength and anthropometry in 75-year-old men and women in three Nordic localities. Scand. J. Med. Sci. Sports 1994, 4, 26–31. [Google Scholar] [CrossRef]
- Rantanen, T.; Masaki, K.; Foley, D.; Izmirlian, G.; White, L.; Guralnik, J.M. Grip strength changes over 27 yr in Japanese-American men. J. Appl. Physiol. 1998, 85, 2047–2053. [Google Scholar] [CrossRef] [Green Version]
- Davis, D.S.; Barnette, B.J.; Kiger, J.T.; Mirasola, J.J.; Young, S.M. Physical characteristics that predict functional performance in Division I college football players. J. Strength Cond. Res. 2004, 18, 115–120. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Novice M (SD) | Expert M (SD) | |
|---|---|---|---|
| Age (years) | 24.3 (5.9) | 34.5 (11.5) | |
| Carpentry experience (years) | 0.003 (0.017) | 13.1 (9.6) | |
| Construction experience (years) | 0.125 (0.3) | 12.8 (8.9) | |
| Weight (Kg) | 82.2 (22.6) | 82.4 (12.7) | |
| Height (M) | 1.770 (0.08) | 1.80 (0.09) | |
| Upper Arm (M) | 0.337 (0.025) | 0.770 (0.094) | |
| Lower Arm (M) | 0.199 (0.014) | 0.193 (0.020) | |
| Gender | Male | 17 | 20 |
| Female | 4 | 1 | |
| Groups | Height Has a Significant Impact on the Following Measure of Muscle Activation Level | Unstandardized Coefficient | Standard Error | t-Value | Standardized Coefficient | ||
|---|---|---|---|---|---|---|---|
| Expertise | Task | Muscle | |||||
| Novice | Deck | BR | Median of average | −0.029 *** | 0.010 | −2.938 | −0.740 *** |
| Mean of average | −0.026 *** | 0.009 | −2.776 | −0.708 *** | |||
| Median of the peak | −0.102 *** | 0.039 | −2.640 | −0.689 *** | |||
| Mean of the peak | −0.108 *** | 0.040 | −2.732 | −0.704 *** | |||
| ECU | Median of average | −0.030 **** | 0.007 | −4.332 | −0.908 **** | ||
| Mean of average | −0.029 **** | 0.006 | −4.559 | −0.934 **** | |||
| Median of the peak | −0.082 *** | 0.031 | −2.701 | −0.672 *** | |||
| Mean of the peak | −0.085 *** | 0.034 | −2.507 | −0.632 *** | |||
| FCR | Median of average | −0.074 **** | 0.019 | −3.992 | −0.894 **** | ||
| Mean of average | −0.075 **** | 0.020 | −3.833 | −0.882 **** | |||
| Median of the peak | −0.349 **** | 0.095 | −3.684 | −0.878 **** | |||
| Mean of the peak | −0.390 **** | 0.100 | −3.879 | −0.909 **** | |||
| FCU | Median of average | −0.034 ** | 0.016 | −2.079 | −0.586 ** | ||
| Mean of average | −0.034 ** | 0.017 | −2.046 | −0.581 ** | |||
| Median of the peak | −0.123 * | 0.064 | −1.904 | −0.551 * | |||
| Mean of the peak | −0.119 * | 0.063 | −1.887 | −0.543 * | |||
| Picket | BR | Median of average | −0.020 *** | 0.007 | −2.986 | −0.710 *** | |
| Mean of average | −0.021 *** | 0.007 | −3.070 | −0.726 *** | |||
| Median of the peak | −0.103 *** | 0.035 | −2.976 | −0.666 *** | |||
| Mean of the peak | −0.098 *** | 0.033 | −2.959 | −0.662 *** | |||
| ECU | Median of average | −0.035 **** | 0.009 | −3.822 | −0.831 **** | ||
| Mean of average | −0.035 **** | 0.009 | −3.870 | −0.829 **** | |||
| Median of the peak | −0.130 **** | 0.054 | −2.387 | −0.593 **** | |||
| Mean of the peak | −0.134 **** | 0.055 | −2.457 | −0.600 **** | |||
| FCR | Median of average | −0.073 **** | 0.014 | −5.423 | −0.953 **** | ||
| Mean of average | −0.075 **** | 0.014 | −5.186 | −0.939 **** | |||
| Median of the peak | −0.435 **** | 0.087 | −4.994 | −0.935 **** | |||
| Mean of the peak | −0.510 **** | 0.105 | −4.851 | −0.916 **** | |||
| FCU | Median of average | −0.018 ** | 0.008 | −2.405 | −0.653 ** | ||
| Mean of average | −0.018 ** | 0.008 | −2.323 | −0.636 ** | |||
| Median of the peak | −0.093 ** | 0.038 | −2.423 | −0.644 ** | |||
| Mean of the peak | −0.094 ** | 0.038 | −2.491 | −0.656 ** | |||
| Expert | Deck | BR | - | - | - | - | - |
| ECU | - | - | - | - | - | ||
| FCR | Median of average | −0.015 ** | 0.007 | −2.187 | −0.552 ** | ||
| Mean of average | −0.016 ** | 0.007 | −2.108 | −0.546 ** | |||
| Median of the peak | −0.163 ** | 0.067 | −2.427 | −0.643 ** | |||
| Mean of the peak | −0.185 ** | 0.071 | −2.588 | −0.667 ** | |||
| FCU | Median of average | 0.007 * | 0.004 | 1.700 | 0.089 * | ||
| Picket | BR | - | - | - | - | - | |
| ECU | - | - | - | - | - | ||
| FCR | Median of average | −0.020 ** | 0.008 | −2.561 | −0.648 ** | ||
| Mean of average | −0.020 ** | 0.008 | −2.557 | −0.644 ** | |||
| Median of the peak | −0.190 ** | 0.077 | −2.450 | −0.643 ** | |||
| Mean of the peak | −0.190 ** | 0.073 | −2.591 | −0.666 ** | |||
| FCU | - | - | - | - | - | ||
| Groups | Weight Has a Significant Impact on Muscle Activation Level | Unstandardized Coefficient | Standard Error | t-Value | Standardized Coefficient | ||
|---|---|---|---|---|---|---|---|
| Expertise | Task | Muscle | |||||
| Novice | Deck | BR | Median of average | 0.005 * | 0.003 | 1.708 | 0.088 * |
| ECU | Median of average | 0.001 *** | 0.001 | 2.787 | 0.651 *** | ||
| Mean of average | 0.002 *** | 0.001 | 3.082 | 0.703 *** | |||
| Median of the peak | 0.004 * | 0.002 | 1.793 | 0.497 * | |||
| Mean of the peak | 0.004 * | 0.003 | 1.665 | 0.467 * | |||
| FCR | Median of average | 0.003 ** | 0.001 | 2.417 | 0.603 ** | ||
| Mean of average | 0.004 ** | 0.002 | 2.322 | 0.595 ** | |||
| Median of the peak | 0.017 ** | 0.007 | 2.298 | 0.610 ** | |||
| Mean of the peak | 0.020 ** | 0.008 | 2.565 | 0.670 ** | |||
| FCU | - | - | - | - | - | ||
| Picket | BR | Median of average | 0.001 ** | 0.001 | 1.982 | 0.525 ** | |
| Mean of average | 0.001 ** | 0.001 | 2.055 | 0.541 ** | |||
| Median of the peak | 0.005 * | 0.003 | 1.798 | 0.448 * | |||
| Mean of the peak | 0.005 * | 0.003 | 1.889 | 0.471 * | |||
| ECU | Median of average | 0.002 ** | 0.001 | 2.118 | 0.513 ** | ||
| Mean of average | 0.001 ** | 0.001 | 2.117 | 0.505 ** | |||
| FCR | Median of average | 0.004 **** | 0.001 | 3.909 | 0.846 **** | ||
| Mean of average | 0.004 **** | 0.001 | 3.767 | 0.841 **** | |||
| Median of the peak | 0.023 **** | 0.007 | 3.443 | 0.795 **** | |||
| Mean of the peak | 0.028 **** | 0.008 | 3.394 | 0.792 **** | |||
| FCU | - | - | - | - | - | ||
| Expert | Deck | BR | - | - | - | - | - |
| ECU | Median of average | −0.001 ** | 0.001 | −2.056 | −0.439 ** | ||
| Mean of average | −0.001 ** | 0.001 | −2.011 | −0.434 ** | |||
| Median of the peak | −0.006 ** | 0.003 | −2.344 | −0.511 ** | |||
| Mean of the peak | −0.006 ** | 0.003 | −2.106 | −0.467 ** | |||
| FCR | Median of peak | 0.013 * | 0.007 | 1.822 | 0.392 * | ||
| Mean of peak | 0.016 ** | 0.008 | 2.039 | 0.427 ** | |||
| FCU | - | - | - | - | - | ||
| Picket | BR | Mean of average | 0.001 * | 0.001 | 1.742 | 0.399 * | |
| Median of the peak | 0.009 * | 0.005 | 1.871 | 0.380 * | |||
| Mean of the peak | 0.011 * | 0.006 | 1.794 | 0.369 * | |||
| ECU | Median of average | −0.001 * | 0.001 | −1.947 | −0.406 * | ||
| Mean of average | −0.001 ** | 0.001 | −1.985 | −0.421 ** | |||
| Median of the peak | −0.005 ** | 0.002 | −1.988 | −0.437 ** | |||
| Mean of the peak | −0.005 ** | 0.002 | −1.957 | −0.430 ** | |||
| FCR | Median of average | 0.001 * | 0.001 | 1.706 | 0.350 * | ||
| Mean of average | 0.001 * | 0.001 | 1.719 | 0.351 * | |||
| Median of the peak | 0.016 ** | 0.008 | 1.957 | 0.417 ** | |||
| Mean of the peak | 0.016 ** | 0.008 | 2.035 | 0.425 ** | |||
| FCU | - | - | - | - | - | ||
| Groups | Lower Arm as a Significant Impact on Muscle Activation Level | Unstandardized Coefficient | Standard Error | t-Value | Standardized Coefficient | ||
|---|---|---|---|---|---|---|---|
| Expertise | Task | Muscle | |||||
| Novice | Deck | BR | Median of average | −0.094 ** | 0.045 | −2.095 | −0.437 ** |
| Mean of average | −0.092 ** | 0.043 | −2.122 | −0.448 ** | |||
| Median of the peak | −0.369 ** | 0.178 | −2.077 | −0.449 ** | |||
| Mean of the peak | −0.389 ** | 0.182 | −2.143 | −0.457 ** | |||
| ECU | Median of average | −0.099 *** | 0.032 | −3.129 | −0.542 *** | ||
| Mean of average | −0.096 *** | 0.029 | −3.282 | −0.556 *** | |||
| Median of the peak | −0.393 *** | 0.140 | −2.811 | −0.579 *** | |||
| Mean of the peak | −0.438 *** | 0.155 | −2.826 | −0.589 *** | |||
| FCR | Median of average | −0.206 ** | 0.085 | −2.42 | −0.448 ** | ||
| Mean of average | −0.199 ** | 0.089 | −2.228 | −0.424 ** | |||
| Median of the peak | −0.845 * | 0.434 | −1.948 | −0.384 * | |||
| Mean of the peak | −0.887 * | 0.460 | −1.930 | −0.374 * | |||
| FCU | - | - | - | - | - | ||
| Picket | BR | Median of average | −0.089 *** | 0.03 | −2.95 | −0.581 *** | |
| Mean of average | −0.091 *** | 0.031 | −2.956 | −0.578 *** | |||
| Median of the peak | −0.530 **** | 0.159 | −3.335 | −0.618 **** | |||
| Mean of the peak | −0.528 **** | 0.152 | −3.473 | −0.643 **** | |||
| ECU | Median of average | −0.136 **** | 0.042 | −3.220 | −0.575 **** | ||
| Mean of average | −0.138 **** | 0.042 | −3.325 | −0.589 **** | |||
| Median of the peak | −0.715 *** | 0.249 | −2.873 | −0.591 *** | |||
| Mean of the peak | −0.755 *** | 0.250 | −3.016 | −0.609 *** | |||
| FCR | Median of average | −0.170 *** | 0.062 | −2.735 | −0.439 *** | ||
| Mean of average | −0.170 *** | 0.066 | −2.587 | −0.427 *** | |||
| Median of the peak | −0.880 ** | 0.399 | −2.207 | −0.379 ** | |||
| Mean of the peak | −1.066 ** | 0.481 | −2.217 | −0.384 ** | |||
| FCU | Median of average | −0.066 * | 0.035 | −1.901 | −0.427 * | ||
| Mean of average | −0.066 * | 0.035 | −1.866 | −0.423 * | |||
| Median of the peak | −0.384 ** | 0.175 | −2.192 | −0.482 ** | |||
| Mean of the peak | −0.383 ** | 0.173 | −2.205 | −0.481 ** | |||
| Expert | Deck | BR | - | - | - | - | - |
| ECU | Median of average | −0.047 ** | 0.023 | −2.037 | −0.538 ** | ||
| Mean of average | −0.044 ** | 0.023 | −2.002 | −0.513 ** | |||
| FCR | - | - | - | - | - | ||
| FCU | Median of average | −0.048 *** | 0.019 | −2.588 | −0.705 *** | ||
| Mean of average | −0.045 *** | 0.017 | −2.609 | −0.713 *** | |||
| Median of the peak | −0.181 * | 0.103 | −1.759 | −0.516 * | |||
| Mean of the peak | −0.191 ** | 0.095 | −2.012 | −0.573 ** | |||
| Picket | BR | Mean of average | −0.023 * | 0.014 | −1.687 | −0.478 * | |
| Median of the peak | −0.670 *** | 0.218 | −3.072 | −0.772 *** | |||
| Mean of the peak | −0.804 *** | 0.279 | −2.881 | −0.733 *** | |||
| ECU | Median of average | −0.048 * | 0.025 | −1.950 | −0.503 * | ||
| Mean of average | −0.047 * | 0.025 | −1.905 | −0.500 * | |||
| Median of the peak | −0.186 * | 0.108 | −1.723 | −0.469 * | |||
| Mean of the peak | −0.188 * | 0.107 | −1.763 | 0.479 * | |||
| FCR | - | - | - | - | - | ||
| FCU | Median of average | -0.032 * | 0.018 | −1.793 | −0.507 * | ||
| Mean of average | −0.031 * | 0.018 | −1.748 | −0.501 * | |||
| Groups | The Upper Arm Has a Significant Impact on Muscle Activation Level | Unstandardized Coefficient | Standard Error | t-Value | Standardized Coefficient | ||
|---|---|---|---|---|---|---|---|
| Expertise | Task | Muscle | |||||
| Novice | Deck | BR | - | - | - | - | - |
| ECU | - | - | - | - | - | ||
| FCR | - | - | - | - | - | ||
| FCU | - | - | - | - | - | ||
| Picket | BR | - | - | - | - | - | |
| ECU | Median of the peak | 0.230 * | 0.139 | 1.652 | 0.365 * | ||
| Mean of the peak | 0.231 * | 0.140 | 1.649 | 0.358 * | |||
| FCR | - | - | - | - | - | ||
| FCU | - | - | - | - | - | ||
| Expert | Deck | BR | - | - | - | - | - |
| ECU | - | - | - | - | - | ||
| FCR | - | - | - | - | - | ||
| FCU | - | - | - | - | - | ||
| Picket | BR | Mean of the peak | 0.285 * | 0.165 | 1.724 | 0.085 * | |
| ECU | - | - | - | - | - | ||
| FCR | - | - | - | - | - | ||
| FCU | - | - | - | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagahi, M.; Ibne Hossain, N.U.; Dayarathna, V.L.; Karam, S.; Babski-Reeves, K.; Jaradat, R. The Impact of Participants’ Anthropometry on Muscle Activation Levels While Interacting with the Level of Expertise, Task Type, and Single Muscles. J. Funct. Morphol. Kinesiol. 2020, 5, 88. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk5040088
Nagahi M, Ibne Hossain NU, Dayarathna VL, Karam S, Babski-Reeves K, Jaradat R. The Impact of Participants’ Anthropometry on Muscle Activation Levels While Interacting with the Level of Expertise, Task Type, and Single Muscles. Journal of Functional Morphology and Kinesiology. 2020; 5(4):88. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk5040088
Chicago/Turabian StyleNagahi, Morteza, Niamat Ullah Ibne Hossain, Vidanelage L. Dayarathna, Sofia Karam, Kari Babski-Reeves, and Raed Jaradat. 2020. "The Impact of Participants’ Anthropometry on Muscle Activation Levels While Interacting with the Level of Expertise, Task Type, and Single Muscles" Journal of Functional Morphology and Kinesiology 5, no. 4: 88. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk5040088