Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
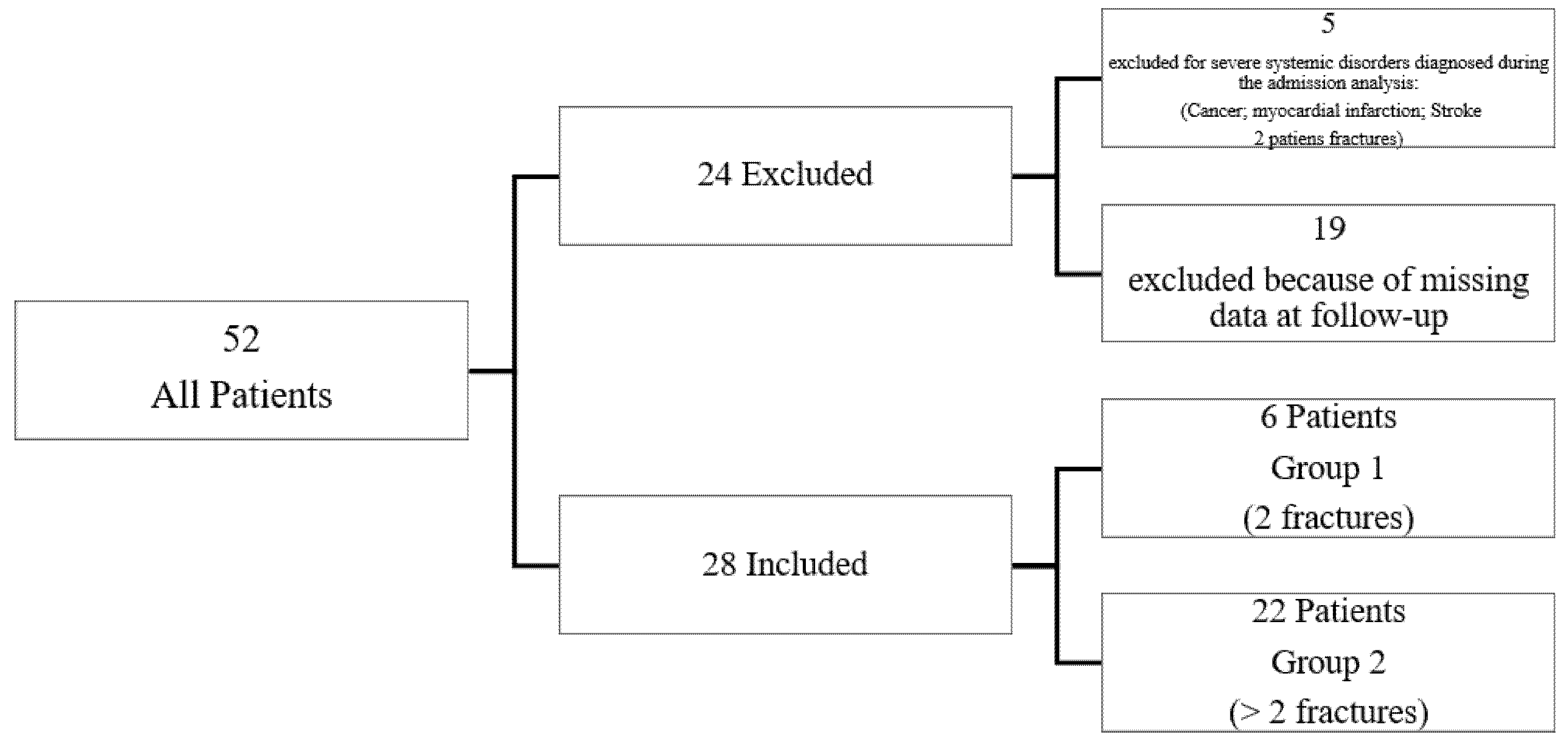
2.1. Study Design and Population
2.2. Participant Selection
2.3. Intervention
2.4. Outcome Measures
2.4.1. Numerical Rating Scale
2.4.2. SF-36
2.4.3. Mini-OQOL
2.4.4. Timed-Up and Go
2.4.5. Dizziness Handicap Inventory (DHI)
2.4.6. Instrumental Assessment of Balance and Gait
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cultrera, P.; Pratelli, E.; Petrai, V.; Postiglione, M.; Zambelan, G.; Pasquetti, P. Evaluation with stabilometric platform of balance disorders in osteoporosis patients. A proposal for a diagnostic protocol. Clin. Cases Miner. Bone Metab. 2010, 7, 123–125. [Google Scholar] [PubMed]
- Tarantino, U.; Iolascon, G.; Cianferotti, L.; Masi, L.; Marcucci, G.; Giusti, F.; Marini, F.; Parri, S.; Feola, M.; Rao, C.; et al. Clinical guidelines for the prevention and treatment of osteoporosis: Summary statements and recommendations from the Italian Society for Orthopaedics and Traumatology. J. Orthop. Traumatol. 2017, 18, 3–36. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.L.; March, L. Vertebral fragility fractures—How to treat them? Best Pract. Res. Clin. Rheumatol. 2019, 33, 227–235. [Google Scholar] [CrossRef]
- Hernlund, E.; Svedbom, A.; Ivergård, M.; Compston, J.; Cooper, C.; Stenmark, J.; McCloskey, E.V.; Jönsson, B.; Kanis, J.A. Osteoporosis in the European Union: Medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch. Osteoporos. 2013, 8, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, E.M.; Gooberman-Hill, R.; Peters, T.J. Using self-reports of pain and other variables to distinguish between older women with back pain due to vertebral fractures and those with back pain due to degenerative changes. Osteoporos. Int. 2016, 27, 1459–1467, Erratum in 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, T.; Tanaka, S.; Kawakami, K.; Miyazaki, T.; Hagino, H.; Shiraki, M.; A-TOP (Adequate Treatment of Osteoporosis) Research Group. Health state utility values and patient-reported outcomes before and after vertebral and non-vertebral fractures in an osteoporosis clinical trial. Osteoporos. Int. 2017, 28, 1893–1901. [Google Scholar] [CrossRef] [PubMed]
- Balzini, L.; Vannucchi, L.; Benvenuti, F.; Benucci, M.; Monni, M.; Cappozzo, A.; Stanhope, S.J. Clinical characteristics of flexed posture in elderly women. J. Am. Geriatr. Soc. 2003, 51, 1419–1426. [Google Scholar] [CrossRef] [PubMed]
- Lorbergs, A.L.; Murabito, J.M.; Jarraya, M.; Guermazi, A.; Allaire, B.T.; Yang, L.; Kiel, D.P.; Cupples, L.A.; Bouxsein, M.L.; Travison, T.G.; et al. Thoracic Kyphosis and Physical Function: The Framingham Study. J. Am. Geriatr. Soc. 2017, 65, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Izzo, R.; Guarnieri, G.; Guglielmi, G.; Muto, M. Biomechanics of the spine. Part I: Spinal stability. Eur. J. Radiol. 2013, 82, 118–126. [Google Scholar] [CrossRef]
- Iolascon, G.; Moretti, A.; Giamattei, M.T.; Migliaccio, S.; Gimigliano, F. Prevalent fragility fractures as risk factor for skeletal muscle function deficit and dysmobility syndrome in post-menopausal women. Aging Clin. Exp. Res. 2015, 27 (Suppl. 1), S11–S16. [Google Scholar] [CrossRef]
- Iolascon, G.; de Sire, A.; Calafiore, D.; Benedetti, M.G.; Cisari, C.; Letizia Mauro, G.; Migliaccio, S.; Nuti, R.; Resmini, G.; Gonnelli, S.; et al. Multifactorial Assessment of Risk of Falling in 753 Post-Menopausal Women: A Multicenter Cross-Sectional Study by the Italian Group for the Study of Metabolic Bone Diseases. Clin. Interv. Aging 2020, 15, 1077–1084. [Google Scholar] [CrossRef]
- Fernández, L.; Breinbauer, H.A.; Delano, P.H. Vertigo and Dizziness in the Elderly. Front. Neurol. 2015, 6, 144. [Google Scholar] [CrossRef] [Green Version]
- Jahn, K. The Aging Vestibular System: Dizziness and Imbalance in the Elderly. Adv. Otorhinolaryngol. 2019, 82, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Falossi, F.; Notarstefano, C.; Miccoli, M.; Pelagatti, A.; Raffaetà, G. Balance impairment and fragility vertebral fractures. Clin. Ter. 2020, 171, e240–e244. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Miyakoshi, N.; Kasukawa, Y.; Hongo, M.; Shimada, Y. Spinal curvature and postural balance in patients with osteoporosis. Osteoporos. Int. 2009, 20, 2049–2053. [Google Scholar] [CrossRef]
- Greig, A.M.; Bennell, K.L.; Briggs, A.M.; Wark, J.D.; Hodges, P.W. Balance impairment is related to vertebral fracture rather than thoracic kyphosis in individuals with osteoporosis. Osteoporos. Int. 2006, 18, 543–551. [Google Scholar] [CrossRef]
- Iolascon, G.; Moretti, A.; Toro, G.; Gimigliano, F.; Liguori, S.; Paoletta, M. Pharmacological Therapy of Osteoporosis: What’s New? Clin. Interv. Aging 2020, 15, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, Y.Z.; Lee, J.H.; Xu, B.; Cho, M. Effect of medications on prevention of secondary osteoporotic vertebral compression fracture, non-vertebral fracture, and discontinuation due to adverse events: A meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2019, 20, 399. [Google Scholar] [CrossRef] [Green Version]
- Moretti, A.; Gimigliano, F.; Di Pietro, G.; Gimigliano, R.; Iolascon, G. Back pain-related disability and quality of life in patients affected by vertebral fractures: Data from baseline characteristics of population enrolled in Denosumab In Real Practice (DIRP). Aging Clin. Exp. Res. 2015, 27 (Suppl. 1), S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Moretti, A.; de Sire, A.; Curci, C.; Toro, G.; Gimigliano, F.; Iolascon, G. Effectiveness of denosumab on back pain-related disability and quality-of-life in patients with vertebral fragility fractures. Curr. Med. Res. Opin. 2018, 35, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, S.; Francomano, D.; Romagnoli, E.; Marocco, C.; Fornari, R.; Resmini, G.; Buffa, A.; Di Pietro, G.; Corvaglia, S.; Gimigliano, F.; et al. Persistence with denosumab therapy in women affected by osteoporosis with fragility fractures: A multicenter observational real practice study in Italy. J. Endocrinol. Investig. 2017, 40, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Brox, W.T.; Roberts, K.C.; Taksali, S.; Wright, D.G.; Wixted, J.J.; Tubb, C.C.; Patt, J.C.; Templeton, K.J.; Dickman, E.; Adler, R.A.; et al. The American Academy of Orthopaedic Surgeons Evidence-Based Guideline on Management of Hip Fractures in the Elderly. J. Bone Jt. Surg. Am. Vol. 2015, 97, 1196–1199. [Google Scholar] [CrossRef]
- Giangregorio, L.M.; Papaioannou, A.; Macintyre, N.J.; Ashe, M.C.; Heinonen, A.; Shipp, K.; Wark, J.; McGill, S.; Keller, H.; Jain, R.; et al. Too Fit To Fracture: Exercise recommendations for individuals with osteoporosis or osteoporotic vertebral fracture. Osteoporos. Int. 2014, 25, 821–835. [Google Scholar] [CrossRef] [Green Version]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef]
- Ware, J.E., Jr. SF-36 health survey update. Spine (Phila Pa 1976) 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Cook, D.J.; Guyatt, G.H.; Adachi, J.D.; Epstein, R.S.; Juniper, E.F.; Austin, P.A.; Clifton, J.; Rosen, C.J.; Kessenich, C.R.; Stock, J.L.; et al. Development and validation of the mini-osteoporosis quality of life questionnaire (OQLQ) in osteoporotic women with back pain due to vertebral fractures. Osteoporosis Quality of Life Study Group. Osteoporos. Int. 1999, 10, 207–213. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Nola, G.; Mostardini, C.; Salvi, C.; Ercolani, A.P.; Ralli, G. Validity of Italian adaptation of the Dizziness Handicap Inventory (DHI) and evaluation of the quality of life in patients with acute dizziness. Acta Otorhinolaryngol. Ital. 2010, 30, 190. [Google Scholar] [PubMed]
- Martines, F.; Salvago, P.; Dispenza, F.; Rizzo, S.; Letizia Mauro, G.; Puglisi, S. Treatment with a new nutraceutical compound on patients suffering from balance disorders: Dizziness handicap inventory scores. Acta Med. Mediterr. 2019, 35, 2029–2034. [Google Scholar]
- Silverman, S.; Viswanathan, H.N.; Yang, Y.C.; Wang, A.; Boonen, S.; Ragi-Eis, S.; Fardellone, P.; Gilchrist, N.; Lips, P.; Nevitt, M.; et al. Impact of clinical fractures on health-related quality of life is dependent on time of assessment since fracture: Results from the FREEDOM trial. Osteoporos. Int. 2011, 23, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Adachi, J.D.; Ioannidis, G.; Olszynski, W.P.; Brown, J.P.; Hanley, D.A.; Sebaldt, R.J.; Petrie, A.; Tenenhouse, A.; Stephenson, G.F.; Papaioannou, A.; et al. The impact of incident vertebral and non-vertebral fractures on health related quality of life in postmenopausal women. BMC Musculoskelet. Disord. 2002, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Bergland, A. Associations between health-related quality of life, physical function and pain in older women with osteoporosis and vertebral fracture. BMC Geriatr. 2019, 19, 298. [Google Scholar] [CrossRef] [PubMed]
- Makarova, E.V.; Marchenkova, L.A.; Eryomushkin, M.A.; Styazkina, E.M.; Chesnikova, E.I. Balance and muscle strength tests in patients with osteoporotic vertebral fractures to develop tailored rehabilitation programs. Eur. J. Transl. Myol. 2020, 30, 9236. [Google Scholar] [CrossRef] [PubMed]
- Iolascon, G.; Giamattei, M.T.; Moretti, A.; Di Pietro, G.; Gimigliano, F.; Gimigliano, R. Sarcopenia in women with vertebral fragility fractures. Aging Clin. Exp. Res. 2013, 25 (Suppl. 1), S129–S131. [Google Scholar] [CrossRef]
- Tetsunaga, T.; Tetsunaga, T.; Nishida, K.; Tanaka, M.; Sugimoto, Y.; Takigawa, T.; Takei, Y.; Ozaki, T. Denosumab and alendronate treatment in patients with back pain due to fresh osteoporotic vertebral fractures. J. Orthop. Sci. 2017, 22, 230–236. [Google Scholar] [CrossRef]
- Rolvien, T.; Schmidt, T.; Butscheidt, S.; Amling, M.; Barvencik, F. Denosumab is effective in the treatment of bone marrow oedema syndrome. Injury 2017, 48, 874–879. [Google Scholar] [CrossRef]
- Dufresne, S.S.; Dumont, N.A.; Bouchard, P.; Lavergne, E.; Penninger, J.M.; Frenette, J. Osteoprotegerin protects against muscular dystrophy. Am. J. Pathol. 2015, 185, 920–926. [Google Scholar] [CrossRef]
- Dufresne, S.S.; Dumont, N.A.; Boulanger-Piette, A.; Fajardo, V.A.; Gamu, D.; Kake-Guena, S.A.; David, R.O.; Bouchard, P.; Lavergne, É.; Penninger, J.M.; et al. Muscle RANK is a key regulator of Ca2+ storage, SERCA activity, and function of fast-twitch skeletal muscles. Am. J. Physiol. Cell Physiol. 2016, 310, C663–C672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, I.F.; Snijders, T.; Smeets, J.S.J.; Leenders, M.; van Kranenburg, J.; den Hoed, M.; Verdijk, L.B.; Poeze, M.; van Loon, L.J.C. Extensive Type II Muscle Fiber Atrophy in Elderly Female Hip Fracture Patients. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Chotiyarnwong, P.; McCloskey, E.; Eastell, R.; McClung, M.R.; Gielen, E.; Gostage, J.; McDermott, M.; Chines, A.; Huang, S.; Cummings, S.R. A Pooled Analysis of Fall Incidence From Placebo-Controlled Trials of Denosumab. J. Bone Miner. Res. 2020, 35, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, J.C.; MacIntyre, N.J.; Ponzano, M.; Templeton, J.A.; Thabane, L.; Papaioannou, A.; Giangregorio, L.M. Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst. Rev. 2019, 7, CD008618. [Google Scholar] [CrossRef] [PubMed]
- Ziebart, C.; Gibbs, J.C.; McArthur, C.; Papaioannou, A.; Mittmann, N.; Laprade, J.; Kim, S.; Khan, A.; Kendler, D.L.; Wark, J.D.; et al. Are osteoporotic vertebral fractures or forward head posture associated with performance-based measures of balance and mobility? Arch Osteoporos. 2019, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, S.; Sanfilippo, V.; Terrana, P.; Scaturro, D.; Lauricella, L.; Letizia Mauro, G. Presbyastasis: From diagnosis to management. In Sensorineural Hearing Loss: Pathophysiology, Diagnosis and Treatment; Nova Science Publishers: New York, NY, USA, 2019; pp. 355–364. [Google Scholar]
- Watson, S.L.; Weeks, B.K.; Weis, L.J.; Harding, A.T.; Horan, S.A.; Beck, B.R. High-intensity exercise did not cause vertebral fractures and improves thoracic kyphosis in postmenopausal women with low to very low bone mass: The LIFTMOR trial. Osteoporos. Int. 2019, 30, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Berk, E.; Koca, T.T.; Güzelsoy, S.S.; Nacitarhan, V.; Demirel, A. Evaluation of the relationship between osteoporosis, balance, fall risk, and audiological parameters. Clin. Rheumatol. 2019, 38, 3261–3268. [Google Scholar] [CrossRef]
- Kerr, C.; Bottomley, C.; Shingler, S.; Giangregorio, L.; de Freitas, H.M.; Patel, C.; Randall, S.; Gold, D.T. The importance of physical function to people with osteoporosis. Osteoporos. Int. 2017, 28, 1597–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| All Patients (n = 28) | Group 1: 2 Fractures (n = 6) | Group 2: >2 Fractures (n = 22) | p-Value between-Group in T0 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p-Value | T0 | T1 | p-Value | T0 | T1 | p-Value | ||
| Age (years) | 66.5 ± 5.3 | 65.5 ± 7.6 | 66.8 ± 4.6 | 0.71 | ||||||
| BMI (kg/m2) | 26.5 ± 4.0 | 24.0 ± 4.6 | 27.2 ± 3.6 | 0.16 | ||||||
| NRS | 6.5 (1.0) | 5.0 (2.0) | <0.05 | 5.0 (2.7) | 3.0 (0.7) | 0.54 | 7.0 (1.7) | 6.0 (1.7) | <0.05 | 0.65 |
| SF-36 | 42.2 ± 15.8 | 50.4 ± 13.2 | <0.05 | 45.0 ± 18.5 | 58.0 ± 10.4 | 0.17 | 41.5 ± 15.4 | 48.3 ± 1.2 | 0.12 | 0.48 |
| Mini-OQOL | 47.0 ± 10.0 | 51.9 ± 9.4 | 0.06 | 52.7 ± 8.3 | 55.5 ± 9.5 | 0.59 | 45.5 ± 10.0 | 51.0 ± 9.3 | 0.07 | 0.11 |
| DHI-I | 38.3 ± 25.5 | 32.7 ± 22.1 | 0.38 | 31.5 ± 25.5 | 29.2 ± 25.2 | 0.88 | 40.2 ± 25.8 | 33.7 ± 21.8 | 0.37 | 0.68 |
| TUG | 13.0 (2.0) | 11.5 (2.5) | 0.78 | 12.0 (0.0) | 10.5 (1.0) | <0.05 | 14.0 (1.7) | 12.7 (2.5) | 0.76 | 0.02 |
| All Patients (n = 28) | Group 1: 2 Fractures (n = 6) | Group 2: >2 Fractures (n = 22) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p-Value | T0 | T1 | p-Value | T0 | T1 | p-Value | |
| Left surface cm2 | 104.6 ± 21.5 | 101.0 ± 25.2 | 0.57 | 97.7 ± 21.0 | 102.8 ± 16.0 | 0.64 | 106.5 ± 21.7 | 100.5 ± 27.5 | 0.43 |
| Right surface cm2 | 104.6 ± 20.1 | 102.6 ± 19.5 | 0.71 | 103.8 ± 22.1 | 101.7 ± 11.5 | 0.84 | 104.8 ± 20.1 | 102.9 ± 21.4 | 0.76 |
| Left Forefoot Surf. cm2 | 56.8 ± 13.6 | 54.4 ± 17.1 | 0.56 | 54.5 ± 11.9 | 58.7 ± 11.9 | 0.56 | 57.4 ± 14.3 | 53.2 ± 18.3 | 0.40 |
| Right Forefoot Surf. cm2 | 56.9 ± 12.8 | 55.1 ± 13.4 | 0.61 | 58.7 ± 13.3 | 57.7 ± 10.4 | 0.89 | 56.5 ± 12.9 | 54.5 ± 14.2 | 0.63 |
| Left Backfoot Surf. cm2 | 47.7 ± 9.3 | 46.6 ± 9.5 | 0.66 | 43.0 ± 9.2 | 44.0 ± 7.0 | 0.84 | 49.0 ± 9.1 | 47.3 ± 10.1 | 0.56 |
| Right Backfoot Surf. cm2 | 47.8 ± 9.7 | 47.4 ± 8.1 | 0.87 | 45.5 ± 9.8 | 44.0 ± 3.2 | 0.73 | 48.5 ± 9.9 | 48.4 ± 8.8 | 0.97 |
| Left Load % | 49.9 ± 5.7 | 48.5 ± 6.0 | 0.39 | 47.8 ± 7.2 | 50.5 ± 8.7 | 0.58 | 50.4 ± 5.3 | 48.0 ± 5.1 | 0.13 |
| Right Load % | 50.1 ± 5.7 | 51.5 ± 6.0 | 0.39 | 52.2 ± 7.2 | 49.5 ± 8.7 | 0.58 | 49.6 ± 5.3 | 52.0 ± 5.1 | 0.13 |
| Left Forefoot Load % | 42.6 ± 8.0 | 42.3 ± 11.9 | 0.92 | 45.5 ± 3.2 | 51.0 ± 12.8 | 0.35 | 41.8 ± 8.8 | 39.9 ± 10.8 | 0.53 |
| Right Forefoot Load % | 44.9 ± 10.4 | 44.9 ± 10.7 | 0.99 | 45.7 ± 5.0 | 49.5 ± 10.1 | 0.43 | 44.7 ± 11.6 | 43.6 ± 10.8 | 0.75 |
| Left Backfoot Load % | 57.4 ± 8.0 | 57.7 ± 11.9 | 0.92 | 54.5 ± 3.2 | 49.0 ± 12.8 | 0.35 | 58.2 ± 8.8 | 60.1 ± 10.8 | 0.53 |
| Right Backfoot Load % | 55.1 ± 10.4 | 55.1 ± 10.7 | 0.99 | 54.3 ± 5.0 | 50.5 ± 10.1 | 0.43 | 55.3 ± 11.6 | 56.4 ± 10.8 | 0.75 |
| CoP X Coord | 13.9 ± 2.4 | 14.2 ± 2.2 | 0.67 | 12.6 ± 1.8 | 13.0 ± 2.7 | 0.78 | 14.3 ± 2.4 | 14.5 ± 1.9 | 0.74 |
| CoP Y Coord | 15.9 ± 2.2 | 16.2 ± 2.2 | 0.59 | 14.3 ± 0.7 | 14.7 ± 2.5 | 0.74 | 16.3 ± 2.3 | 16.6 ± 1.9 | 0.64 |
| Left Pod Degree | 6.3 ± 4.0 | 7.5 ± 3.7 | 0.28 | 4.8 ± 3.2 | 6.8 ± 2.6 | 0.26 | 6.7 ± 4.2 | 7.6 ± 4.0 | 0.47 |
| Right Pod Degree | 7.6 ± 4.8 | 9.4 ± 5.5 | 0.19 | 4.8 ± 4.1 | 10.0 ± 3.7 | 0.04 | 8.4 ± 4.8 | 9.3 ± 5.9 | 0.58 |
| Open Eyes | |||||||||
| All Patients (n = 28) | Group 1: 2 Fractures (n = 6) | Group 2: >2 Fractures (n = 22) | |||||||
| T0 | T1 | p-Value | T0 | T1 | p-Value | T0 | T1 | p-Value | |
| Surface ellipse cm | 129.9 ± 101.1 | 152.9 ± 205.8 | 0.60 | 87.8 ± 61.9 | 89.8 ± 56.3 | 0.95 | 141.4 ± 107.6 | 170.1 ± 228.6 | 0.60 |
| Bundle length mm | 493.3 ± 154.3 | 529.0 ± 170.4 | 0.42 | 475.5 ± 175.9 | 582.2 ± 143.6 | 0.28 | 498.2 ± 152.1 | 514.5 ± 177.2 | 0.75 |
| Oscillation maximum | 2.0 ± 1.3 | 2.0 ± 0.6 | 0.79 | 1.6 ± 0.3 | 1.9 ± 0.4 | 0.19 | 2.2 ± 1.5 | 2.0 ± 0.7 | 0.61 |
| Velocity average mm/s | 10.1 ± 3.1 | 10.7 ± 3.4 | 0.48 | 9.7 ± 3.6 | 11.8 ± 2.8 | 0.30 | 10.2 ± 3.1 | 10.4 ± 3.5 | 0.82 |
| X average | 0.1 ± 7.4 | −1.5 ± 9.6 | 0.50 | −1.8 ± 7.9 | 3.0 ± 11.0 | 0.41 | 0.6 ± 7.4 | −2.7 ± 9.0 | 0.19 |
| Y average | −17.3 ± 12.9 | −17.0 ± 11.7 | 0.93 | −164 ± 11.3 | −11.9 ± 13.9 | 0.55 | −17.6 ± 13.6 | −18.4 ± 11.0 | 0.82 |
| Standard Deviation X | 2.2 ± 1.0 | 2.5 ± 1.3 | 0.30 | 1.6 ± 0.8 | 2.1 ± 0.5 | 0.21 | 2.4 ± 1.0 | 2.7 ± 1.4 | 0.47 |
| Standard Deviation Y | 2.8 ± 1.2 | 2.7 ± 1.5 | 0.95 | 2.6 ± 0.9 | 2.2 ± 1.2 | 0.54 | 2.8 ± 1.3 | 2.9 ± 1.6 | 0.86 |
| Closed Eyes | |||||||||
| All Patients (n = 28) | Group 1: 2 Fractures (n = 6) | Group 2: >2 Fractures (n = 22) | |||||||
| T0 | T1 | p-Value | T0 | T1 | p-Value | T0 | T1 | p-Value | |
| Surface ellipse cm | 248.4 ± 370.9 | 192.3 ± 205.1 | 0.49 | 148.3 ± 134.3 | 102.4 ± 101.4 | 0.52 | 275.8 ± 411.0 | 216.9 ± 220.7 | 0.56 |
| Bundle length mm | 536.5 ± 142.6 | 560.8 ± 209.9 | 0.61 | 559.0 ± 172.0 | 516.9 ± 82.3 | 0.61 | 530.4 ± 137.6 | 572.8 ± 233.1 | 0.47 |
| Oscillation maximum | 5.6 ± 4.3 | 6.3 ± 5.1 | 0.53 | 5.0 ± 2.9 | 8.2 ± 8.4 | 0.41 | 5.7 ± 4.6 | 5.9 ± 3.9 | 0.91 |
| Velocity average mm/s | 10.8 ± 2.9 | 11.3 ± 4.1 | 0.61 | 11.3 ± 3.5 | 10.4 ± 1.5 | 0.60 | 10.6 ± 2.8 | 11.5 ± 4.6 | 0.45 |
| X average | 0.3 ± 8.4 | −1.5 ± 8.7 | 0.42 | −3.5 ± 12.1 | 2.2 ± 8.0 | 0.36 | 1.4 ± 7.1 | −2.6 ± 8.8 | 0.11 |
| Y average | −17.2 ± 12.7 | −16.5 ± 10.3 | 0.83 | −13.5 ± 9.0 | −13.3 ± 10.9 | 0.97 | −18.2 ± 13.5 | −17.4 ± 10.2 | 0.83 |
| Standard Deviation X | 3.0 ± 2.8 | 2.5 ± 1.6 | 0.37 | 2.1 ± 1.1 | 1.9 ± 1.3 | 0.79 | 3.2 ± 3.0 | 2.6 ± 1.6 | 0.39 |
| Standard Deviation Y | 3.0 ± 2.0 | 3.2 ± 2.2 | 0.74 | 3.0 ± 1.9 | 2.3 ± 1.8 | 0.51 | 3.1 ± 2.0 | 3.5 ± 2.3 | 0.51 |
| All Patients (n = 28) | Group 1: 2 Fractures (n = 6) | Group 2: >2 Fractures (n = 22) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | p-Value | T0 | T1 | p-Value | T0 | T1 | p-Value | |
| Length Left Gait Line mm | 187.6 ± 36.5 | 186.9 ± 23.9 | 0.93 | 162.7 ± 63.5 | 175.7 ± 26.6 | 0.66 | 194.5 ± 23.0 | 190.0 ± 22.8 | 0.52 |
| Length Right Gait Line mm | 184.3 ± 44.8 | 186.5 ± 18.1 | 0.80 | 177.5 ± 40.7 | 184.7 ± 9.9 | 0.69 | 186.1 ± 46.6 | 187.0 ± 19.9 | 0.93 |
| Left Forefoot Load % | 60.4 ± 6.2 | 62.9 ± 5.4 | 0.11 | 60.0 ± 6.7 | 65.2 ± 5.1 | 0.17 | 60.5 ± 6.2 | 62.3 ± 5.5 | 0.31 |
| Right Forefoot Load % | 61.7 ± 5.8 | 61.0 ± 5.8 | 0.63 | 65.0 ± 5.7 | 60.3 ± 5.6 | 0.19 | 60.8 ± 5.6 | 61.1 ± 6.0 | 0.86 |
| Left Backfoot Load % | 39.6 ± 6.2 | 37.1 ± 5.4 | 0.11 | 40.0 ± 6.7 | 34.8 ± 5.1 | 0.17 | 39.5 ± 6.2 | 37.7 ± 5.5 | 0.31 |
| Right Backfoot Load % | 38.3 ± 5.8 | 39.0 ± 5.8 | 0.63 | 35.0 ± 5.7 | 39.7 ± 5.6 | 0.19 | 39.2 ± 5.6 | 38.9 ± 6.0 | 0.86 |
| Left side Load % | 50.7 ± 6.6 | 50.4 ± 6.3 | 0.85 | 53.5 ± 7.7 | 53.3 ± 7.8 | 0.97 | 49.9 ± 6.2 | 49.5 ± 5.7 | 0.84 |
| Right side Load % | 48.7 ± 5.6 | 50.0 ± 5.5 | 0.39 | 47.7 ± 5.8 | 53.8 ± 5.5 | 0.09 | 49.0 ± 5.7 | 48.9 ± 5.1 | 0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaturro, D.; Rizzo, S.; Sanfilippo, V.; Giustino, V.; Messina, G.; Martines, F.; Falco, V.; Cuntrera, D.; Moretti, A.; Iolascon, G.; et al. Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study. J. Funct. Morphol. Kinesiol. 2021, 6, 24. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6010024
Scaturro D, Rizzo S, Sanfilippo V, Giustino V, Messina G, Martines F, Falco V, Cuntrera D, Moretti A, Iolascon G, et al. Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study. Journal of Functional Morphology and Kinesiology. 2021; 6(1):24. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6010024
Chicago/Turabian StyleScaturro, Dalila, Serena Rizzo, Valeria Sanfilippo, Valerio Giustino, Giuseppe Messina, Francesco Martines, Vincenzo Falco, Daniele Cuntrera, Antimo Moretti, Giovanni Iolascon, and et al. 2021. "Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study" Journal of Functional Morphology and Kinesiology 6, no. 1: 24. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6010024