
Functional Translation of Exercise Responses from Exercise Testing to Exercise Training: The Test of a Model


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
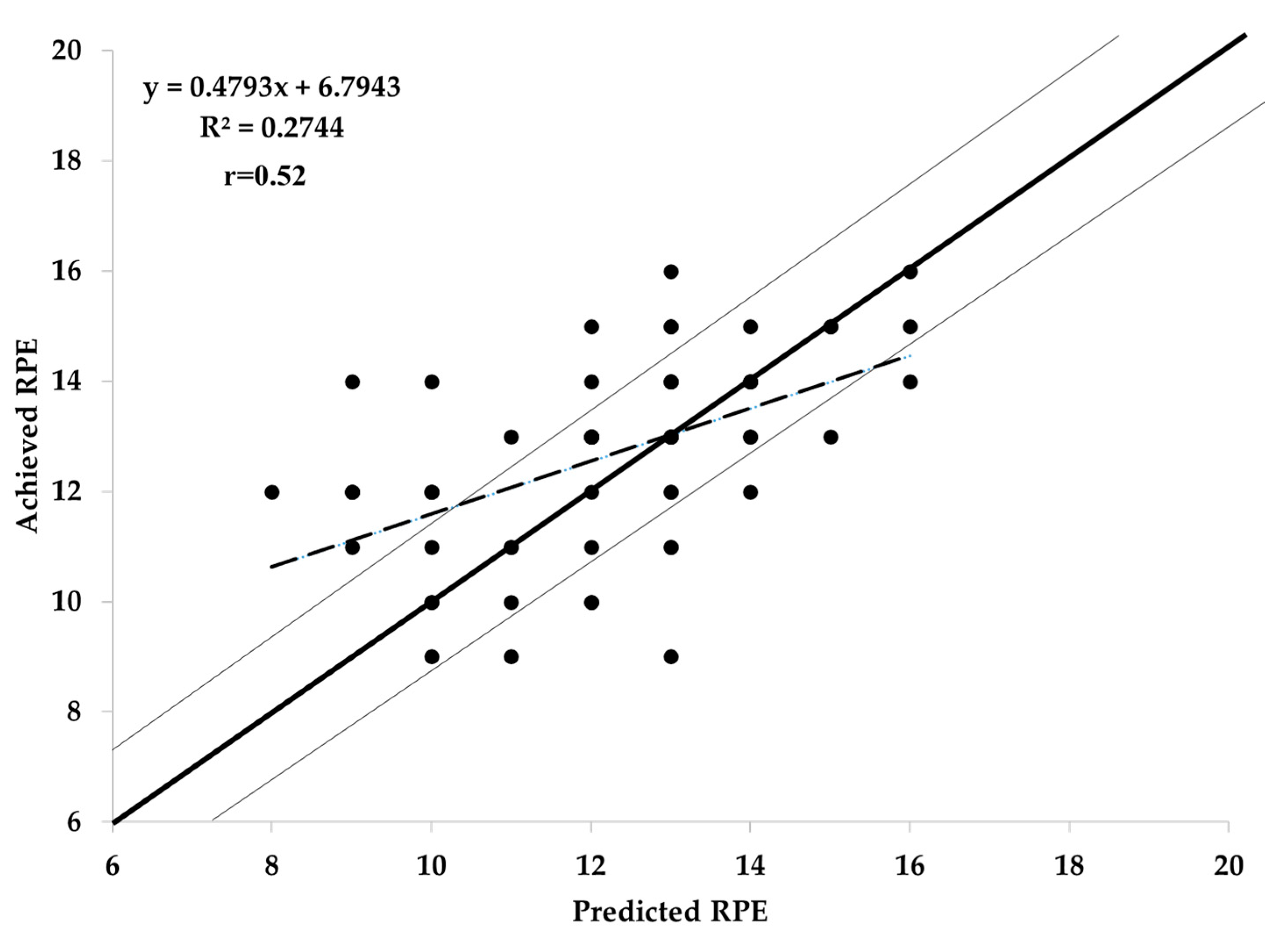
3. Results
4. Discussion
5. Conclusions
6. Practical Applications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arem, H.; Mozre, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- O’Keefe, J.; Lavie, C.J.; Guazzi, M. Potential danger of extreme endurance exercise: How much is too much? Prog. Cardiovas. Dis. 2015, 57, 396–405. [Google Scholar] [CrossRef] [Green Version]
- Kraus, W.E.; Janz, K.F.; Powell, K.E.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Daily step counts for measuring physical activity exposure and its relation to health. Med. Sci. Sports Exerc. 2019, 51, 1206–1212. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puslza, P.; Blair, S.N.; Katzmarek, P.J. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectany. Lancet 2012, 380, 21–27. [Google Scholar] [CrossRef] [Green Version]
- Paffenbarger, R.S.J.; Hyde, R.T.; Wing, A.L.; Hsieh, C.C. Physical activity and all-cause mortality and longevity of college alumni. N. Engl. J. Med. 1986, 314, 605–613. [Google Scholar] [CrossRef]
- Foster, C.; Pollock, M.L.; Anholm, J.D.; Squires, R.W.; Ward, A.; Dymond, D.S.; Rod, J.L.; Saichek, R.P.; Schmidt, D.H. Work capacity and left ventricular function during rehabilitation from myocardial revascularization surgery. Circulation 1984, 69, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Neibauer, J.; Hambrecht, R.; Velicht, T.; Hauer, K.; Marburger, C.; Kälberer, B.; Weiss, C.; von Hodenberg, E.; Schlierf, G.; Schuler, G.; et al. Attenuate progression of coronary artery disease after 6-years of multi-factorial risk intervention. Circulation 1997, 96, 2534–2541. [Google Scholar] [CrossRef]
- Haskell, W.; Alderman, E.; Fair, J. Intensive risk factor management in men and women with coronary artery disease. The Stanford coronary risk intervention project (SCRIP). Atherosclerosis 1984, 109, 182–189. [Google Scholar] [CrossRef]
- O’Connor, G.T.; Buring, J.E.; Yuset, S.; O’Connor, G.T.; Buring, J.E.; Yusuf, S.; Goldhaber, S.Z.; Olmstead, E.M.; Paffenbarger, R.S., Jr.; Hennekens, C.H. An overview of randomized trials of rehabilitation with exercise after myocardial infarction. Circulation 1989, 80, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Rauch, B.; Davod, C.O.; Doherty, P.; Saure, D.; Metzendorf, M.I.; Salzwedel, A.; Voeller, H.; Jensen, K.; Schmid, J.P. The prognostic effect of cardiac rehabilitation in the era of acute revascularization and statin therapy: A systematic review and meta analysis of randomized and non-randomized trails. Eur. J. Prev. Cardiol. 2016, 23, 1914–1939. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Porcari, J.P.; Battista, R.A.; Udermann, B.; Wright, G.; Lucia, A. The risk of exercise training. Am. J. Lifestyle Med. 2008, 2, 279–284. [Google Scholar] [CrossRef]
- Franklin, B.; Billezke, S. Putting the benefits and risks of aerobic exercise in perspective. Curr. Sports Med. Repts. 2012, 12, 201–208. [Google Scholar] [CrossRef]
- Hassock, K.H.; Hartwig, R. Cardiac arrest associated with supervised cardiac rehabilitation. J. Cardiopulm. Rehabil. 1982, 2, 402–408. [Google Scholar]
- Oldridge, N.B. Compliance and experience in primary and secondary prevention of coronary heard disease: A review. Prev. Med. 1982, 12, 52–70. [Google Scholar]
- Burgomaster, K.A.; Hughes, S.C.; Heigenhauser, G.I.F.; Bradwell, S.N.; Gibala, M.J. Six sessions of sprint interval training increases muscle oxidative potential and cycle endurance capacity in humans. J. Appl. Physiol. 2005, 98, 1985–1998. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; Macdonald, M.J.; Hawley, J.A. Physiological adaptation to low volume, high intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef]
- Meyer, K.; Foster, C.; Georgakopoulous, N.; Hajric, R.; Westbrook, S.; Ellestad, A.; Tilman, K.; Fitzgerald, D.; Young, H.; Weinstein, H.; et al. Comparison of left ventricular function during interval and steady state exercise in patients with chronic heart failure. Am. J. Cardiol. 1998, 82, 1382–1387. [Google Scholar] [CrossRef]
- Babraj, J.A.; Volland, N.B.J.; Keast, C.; Guppy, F.M.; Cottrell, G.; Tiernan, J.A. Extremely short duration, high intensity interval training substantially improves insulin action in young healthy males. BMC Endoc. Dis. 2009, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wisloff, U.; Stoylen, A.; Loeuuecker, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Farland, C.V.; Guidotti, F.; Harbin, M.; Roberts, B.; Schuette, J.; Tuuri, A.; Doberstein, S.T.; Porcari, J.P. The effects of high intensity training vs steady state training on aerobic and anaerobic capacity. J. Sports Sci. Med. 2015, 14, 747–755. [Google Scholar]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Parfitt, G.; Evans, H.; Eston, R. Perceptually regulated training at RPE13 is pleasant and improves physical health. Med. Sci. Sports Exerc. 2012, 44, 1613–1618. [Google Scholar] [CrossRef] [Green Version]
- Mezzani, A.; Hamm, L.F.; Jones, A.M.; McBride, P.E.; Moholdt, T.; Stone, J.A.; Urhausen, A.; Williams, M.A. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation. J. Cardiopulm. Rehab. Prev. 2012, 32, 327–350. [Google Scholar] [CrossRef]
- Foster, C.; Porcari, J.P.; Doro, K.; Dubiel, J.; Engen, M.; Kolman, D.; Xiong, S. Exercise prescription when there is no exercise test: The Talk Test. Kinesiology 2018, 50, 333–348. [Google Scholar]
- Porcari, J.P.; Falck, K.; Turek, J.; Sweeney, S.; Wargowski, A.; Doberstein, S.T.; Foster, C. Comparison of %HRR and Talk Test for exercise prescription. Kinesiology 2018, 50, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Cannon, C.; Foster, C.; Porcari, J.P.; Skemp-Arlt, K.M.; Fater, D.C.W.; Backes, R. The Talk Test as a measure of exertional ischemia. Am. J. Med. Sport 2004, 6, 52–57. [Google Scholar]
- Foster, C.; Porcari, J.P.; Gibson, M.; Wright, G.; Greany, J.; Talati, N.; Recalde, P. Translation of submaximal exercise test responses to exercise prescription using the Talk Test. J. Str. Cond. Res. 2009, 23, 2425–2429. [Google Scholar] [CrossRef]
- Foster, C.; Lemberger, K.; Thompson, N.N.; Sennett, S.M.; Hare, J.; Pollock, M.L.; Pels, A.E., III; Schmidt, D.H. Functional translation of exercise responses from graded exercise testing to exercise training. Am. Heart J. 1986, 112, 1309–1316. [Google Scholar] [CrossRef]
- Foster, C.; Thompson, N.N.; Bales, S. Functional translation of exercise responses using combined arm and leg ergometery. Cardiology 1991, 78, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Foster, C.; Thompson, N.N. Functional translation of exercise test responses to recreational activities. J. Cardiopulm. Rehabil. 1991, 11, 373–377. [Google Scholar] [CrossRef]
- Foster, C.; Anholm, J.D.; Bok, D.; Boullosa, D.; Condello, G.; Cortis, C.; Fusco, A.; Jaime, S.J.; de Koning, J.J.; Lucia, A.; et al. Generalized approach to translating exercise tests and prescribing exercise. J. Funct. Morph. Kin. 2020, 5, 63. [Google Scholar] [CrossRef]
- Foster, C.; Porcari, J.P.; Hipp, M. Clinical exercise testing. In ACSM’s Guidebook for Clinical Exercise Physiologists; Thompson, W., Ed.; Wolters Kluwer: Baltimore, MD, USA, 2019; pp. 349–364. [Google Scholar]
- Borg, G.A.V. Borg’s Perceived Exertion and Pain Scales; Human Kinetics Press: Champaign, IL, USA, 1998. [Google Scholar]
- Foster, C.; Cotter, H.M. Blood lactate, respiratory and heart rate markers on the capacity for sustained exercise. In Physiological Assessment of Human Fitness, 2nd ed.; Maud, P.J., Foster, C., Eds.; Human Kinetics Press: Champaign, IL, USA, 2005; pp. 63–76. [Google Scholar]
- Eston, R.; Lambrecht, D.; Shephard, K.; Parfitt, G. Prediction of maximal oxygen uptake from a perceptually regulated sub-maximal graded exercise test. J. Sports Sci. 2008, 26, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Alamji, R.A.; Foster, C.; Porcari, J.P.; Radtke, K.; Doberstein, S. Comparison of non-maximal tests for estimating exercise capacity. Kinesiology 2020, 52, 10–18. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Males (n = 10) | Females (n = 10) |
|---|---|---|
| Age (years) | 23.5 ± 2.2 | 22.3 ± 0.9 |
| Height (cm) | 183.1 ± 7.3 | 167.6 ± 6.7 |
| Weight (kg) | 82.3 ± 18.4 | 70.0 ± 13.2 |
| VO2max (ml·kg−1·min−1) | 53.3 ± 6.1 | 40.3 ± 5.3 |
| HRmax (bpm) | 189 ± 7 | 185 ± 5 |
| RPEmax | 19.9 ± 0.2 | 19.9 ± 0.2 |
| % HRR | Predicted HR | Achieved HR | Predicted RPE | Achieved RPE |
|---|---|---|---|---|
| 60% | 135.1 ± 4.3 | 130.2 ± 7.6 * | 11.8 ± 1.2 | 11.2 ± 1.5 |
| 70% | 147.9 ± 4.6 | 142.8 ± 8.9 * | 13.0 ± 1.4 | 12.4 ± 1.7 |
| 80% | 160.4 ± 5.4 | 157.3 ± 9.7 | 14.1 ± 1.1 | 13.8 ± 1.3 |
| Speed (m·s−1) | Grade (%) | METs [21] | HR | RPE |
|---|---|---|---|---|
| 0 | 0 | 1 | 70 | 6 |
| 1.34 | 0 | 3.3 | 95 | 8 |
| 1.34 | 2 | 4.1 | 115 | 10 |
| 1.34 | 4 | 4.9 | 133 | 12 |
| 1.34 | 6 | 5.8 | 150 | 14 |
| 1.34 | 8 | 6.6 | 155 | 16 |
| 1.34 | 10 | 7.4 | 160 | 18.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tyrrell, T.; Pavlock, J.; Bramwell, S.; Cortis, C.; Doberstein, S.T.; Fusco, A.; Porcari, J.P.; Foster, C. Functional Translation of Exercise Responses from Exercise Testing to Exercise Training: The Test of a Model. J. Funct. Morphol. Kinesiol. 2021, 6, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030066
Tyrrell T, Pavlock J, Bramwell S, Cortis C, Doberstein ST, Fusco A, Porcari JP, Foster C. Functional Translation of Exercise Responses from Exercise Testing to Exercise Training: The Test of a Model. Journal of Functional Morphology and Kinesiology. 2021; 6(3):66. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030066
Chicago/Turabian StyleTyrrell, Tristan, Jessica Pavlock, Susan Bramwell, Cristina Cortis, Scott T. Doberstein, Andrea Fusco, John P. Porcari, and Carl Foster. 2021. "Functional Translation of Exercise Responses from Exercise Testing to Exercise Training: The Test of a Model" Journal of Functional Morphology and Kinesiology 6, no. 3: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk6030066