
Effects of Exercise on Skeletal Muscle Pathophysiology in Huntington’s Disease

 ,
,  ,
,  , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
3. The Effects of Physical Activity in Mouse Models and Patients with HD
3.1. The Effects of Physical Activity in HD Rodent Models
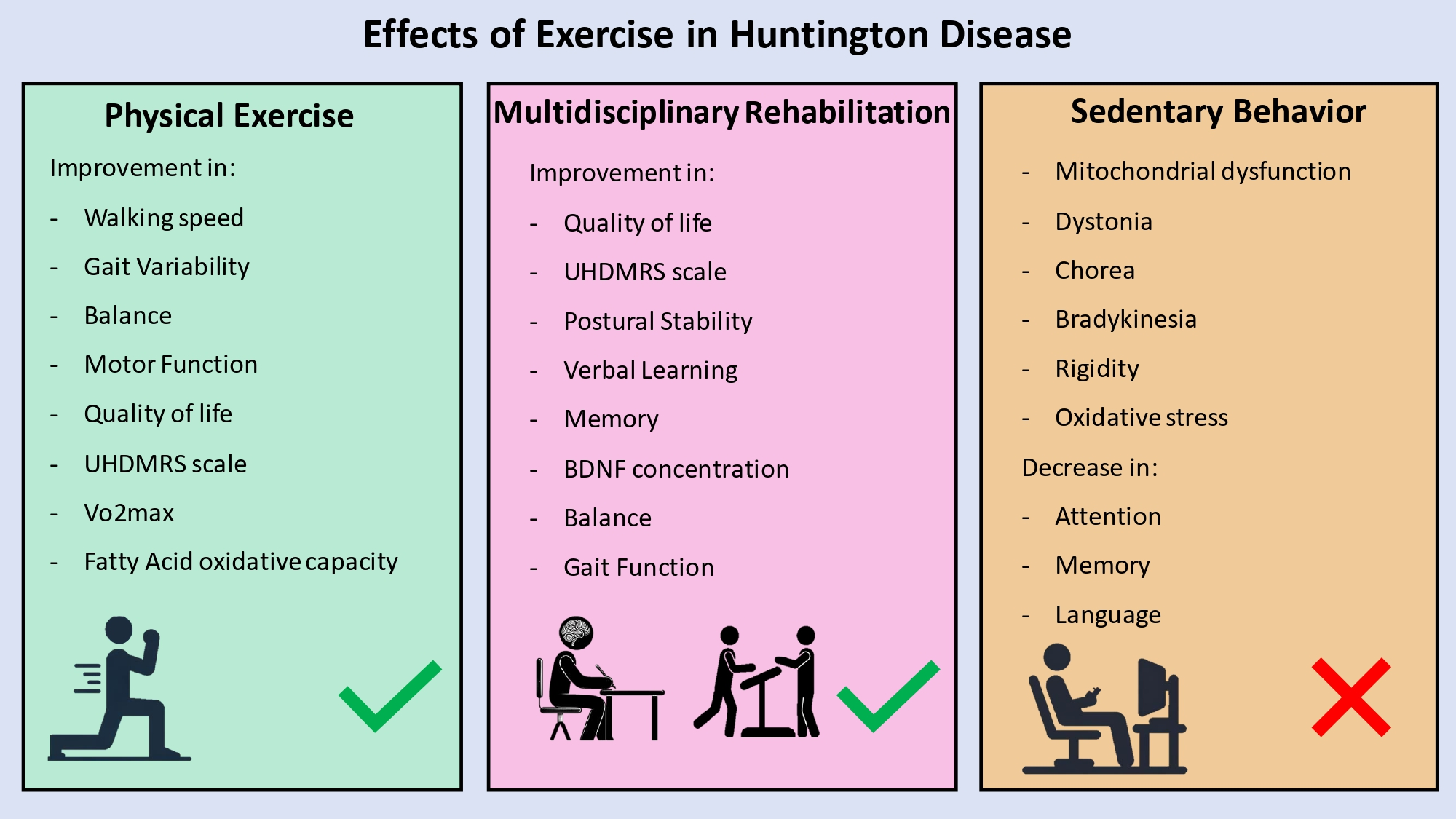
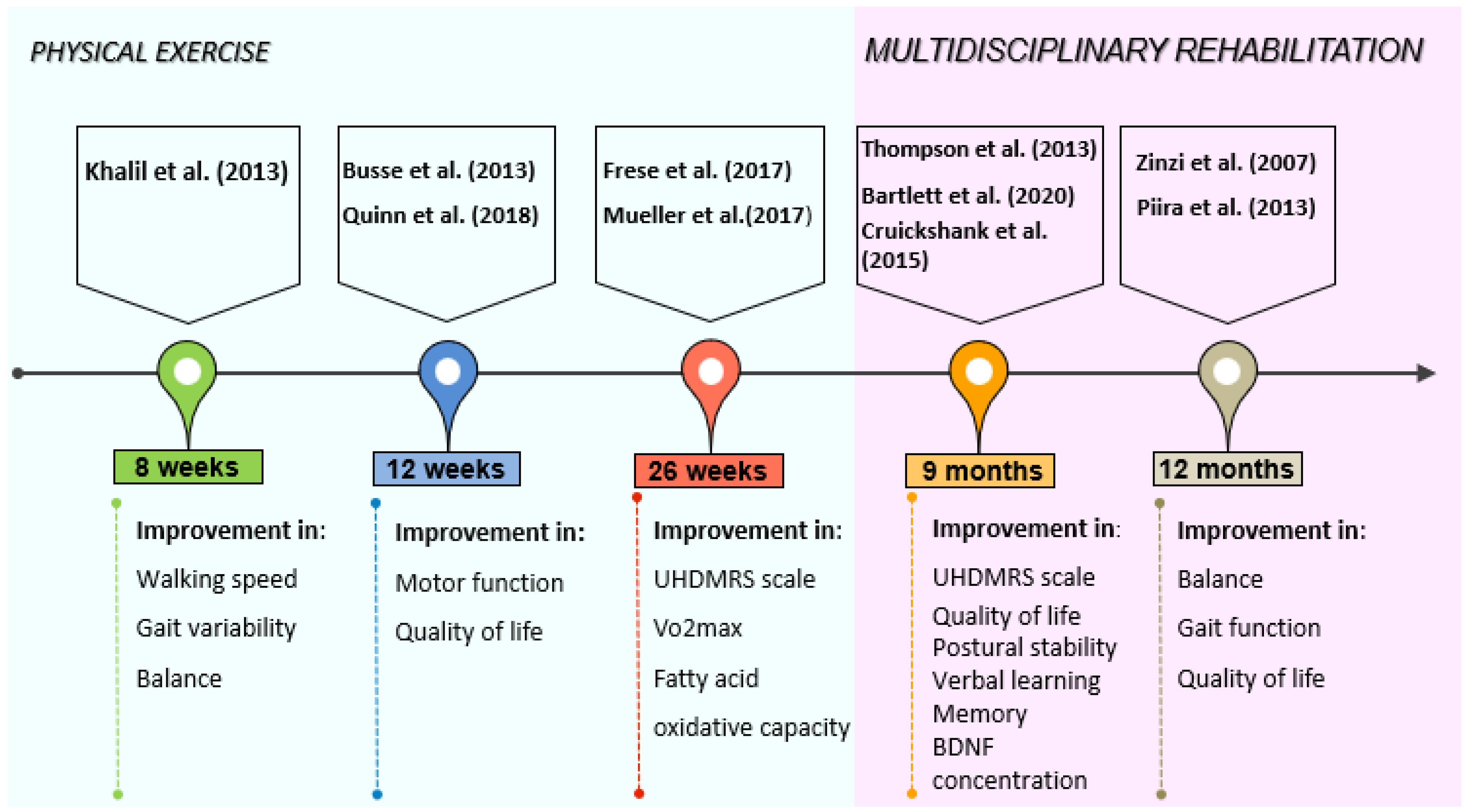
3.2. The Effects of Physical Activity in HD Patients
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jimenez-Sanchez, M.; Licitra, F.; Underwood, B.R.; Rubinsztein, D.C. Huntington’s Disease: Mechanisms of Pathogenesis and Therapeutic Strategies. Cold Spring Harb. Perspect. Med. 2017, 7, a024240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, C.A.; Aylward, E.H.; Wild, E.J.; Langbehn, D.R.; Long, J.D.; Warner, J.H.; Scahill, R.I.; Leavitt, B.R.; Stout, J.C.; Paulsen, J.S.; et al. Huntington disease: Natural history, biomarkers and prospects for therapeutics. Nat. Rev. Neurol. 2014, 10, 204–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlau, M.; Winkelmann, J.; Rujescu, D.; Giegling, I.; Koutsouleris, N.; Gaser, C.; Arsic, M.; Weindl, A.; Reiser, M.; Meisenzahl, E.M. Variation within the Huntington’s disease gene influences normal brain structure. PLoS ONE 2012, 7, e29809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, C.A.; Tabrizi, S.J. Huntington’s disease: From molecular pathogenesis to clinical treatment. Lancet Neurol. 2011, 10, 83–98. [Google Scholar] [CrossRef]
- Cattaneo, E.; Zuccato, C.; Tartari, M. Normal huntingtin function: An alternative approach to Huntington’s disease. Nat. Rev. Neurosci. 2005, 6, 919–930. [Google Scholar] [CrossRef]
- Hamilton, J.M.; Salmon, D.P.; Corey-Bloom, J.; Gamst, A.; Paulsen, J.S.; Jerkins, S.; Jacobson, M.W.; Peavy, G. Behavioural abnormalities contribute to functional decline in Huntington’s disease. J. Neurol. Neurosurg. Psychiatry 2003, 74, 120–122. [Google Scholar] [CrossRef] [Green Version]
- Andrew, S.E.; Goldberg, Y.P.; Kremer, B.; Telenius, H.; Theilmann, J.; Adam, S.; Starr, E.; Squitieri, F.; Lin, B.; Kalchman, M.A.; et al. The relationship between trinucleotide (CAG) repeat length and clinical features of Huntington’s disease. Nat. Genet. 1993, 4, 398–403. [Google Scholar] [CrossRef]
- Schultz, J.L.; van der Plas, E.; Langbehn, D.R.; Conrad, A.L.; Nopoulos, P.C. Age-Related Cognitive Changes as a Function of CAG Repeat in Child and Adolescent Carriers of Mutant Huntingtin. Ann. Neurol. 2021, 89, 1036–1040. [Google Scholar] [CrossRef]
- Nana, A.L.; Kim, E.H.; Thu, D.C.; Oorschot, D.E.; Tippett, L.J.; Hogg, V.M.; Synek, B.J.; Roxburgh, R.; Waldvogel, H.J.; Faull, R.L. Widespread heterogeneous neuronal loss across the cerebral cortex in Huntington’s disease. J. Huntingt. Dis. 2014, 3, 45–64. [Google Scholar] [CrossRef]
- Weydt, P.; Dupuis, L.; Petersen, Å. Thermoregulatory disorders in Huntington disease. Handb. Clin. Neurol. 2018, 157, 761–775. [Google Scholar] [CrossRef]
- Reiner, A.; Albin, R.L.; Anderson, K.D.; D’Amato, C.J.; Penney, J.B.; Young, A.B. Differential loss of striatal projection neurons in Huntington disease. Proc. Natl. Acad. Sci. USA 1988, 85, 5733–5737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vonsattel, J.P.; Myers, R.H.; Stevens, T.J.; Ferrante, R.J.; Bird, E.D.; Richardson, E.P., Jr. Neuropathological classification of Huntington’s disease. J. Neuropathol. Exp. Neurol. 1985, 44, 559–577. [Google Scholar] [CrossRef] [PubMed]
- Beste, C.; Konrad, C.; Saft, C.; Ukas, T.; Andrich, J.; Pfleiderer, B.; Hausmann, M.; Falkenstein, M. Alterations in voluntary movement execution in Huntington’s disease are related to the dominant motor system: Evidence from event-related potentials. Exp. Neurol. 2009, 216, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.A.; Pantelyat, A.; Kogan, J.; Brandt, J. Determinants of functional disability in Huntington’s disease: Role of cognitive and motor dysfunction. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 1351–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblatt, A.; Abbott, M.H.; Gourley, L.M.; Troncoso, J.C.; Margolis, R.L.; Brandt, J.; Ross, C.A. Predictors of neuropathological severity in 100 patients with Huntington’s disease. Ann. Neurol. 2003, 54, 488–493. [Google Scholar] [CrossRef]
- Marder, K.; Zhao, H.; Myers, R.H.; Cudkowicz, M.; Kayson, E.; Kieburtz, K.; Orme, C.; Paulsen, J.; Penney, J.B., Jr.; Siemers, E.; et al. Rate of functional decline in Huntington’s disease. Huntington Study Group. Neurology 2000, 54, 452–458. [Google Scholar] [CrossRef]
- Zhunina, O.A.; Yabbarov, N.G.; Orekhov, A.N.; Deykin, A.V. Modern approaches for modelling dystonia and Huntington’s disease in vitro and in vivo. Int. J. Exp. Pathol. 2019, 100, 64–71. [Google Scholar] [CrossRef]
- Gibson, J.S.; Claassen, D.O. State-of-the-art pharmacological approaches to reduce chorea in Huntington’s disease. Expert Opin. Pharmacother. 2021, 22, 1015–1024. [Google Scholar] [CrossRef]
- Sassone, J.; Colciago, C.; Cislaghi, G.; Silani, V.; Ciammola, A. Huntington’s disease: The current state of research with peripheral tissues. Exp. Neurol. 2009, 219, 385–397. [Google Scholar] [CrossRef]
- Miranda, D.R.; Reed, E.; Jama, A.; Bottomley, M.; Ren, H.; Rich, M.M.; Voss, A.A. Mechanisms of altered skeletal muscle action potentials in the R6/2 mouse model of Huntington’s disease. Am. J. Physiol. Cell Physiol. 2020, 319, C218–C232. [Google Scholar] [CrossRef]
- Gizatullina, Z.Z.; Lindenberg, K.S.; Harjes, P.; Chen, Y.; Kosinski, C.M.; Landwehrmeyer, B.G.; Ludolph, A.C.; Striggow, F.; Zierz, S.; Gellerich, F.N. Low stability of Huntington muscle mitochondria against Ca2+ in R6/2 mice. Ann. Neurol. 2006, 59, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Bozzi, M.; Sciandra, F. Molecular Mechanisms Underlying Muscle Wasting in Huntington’s Disease. Int. J. Mol. Sci. 2020, 21, 8314. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, R.K.; Adhihetty, P.; Shukla, S.; Hennessy, T.; Calingasan, N.; Yang, L.; Starkov, A.; Kiaei, M.; Cannella, M.; Sassone, J.; et al. Impaired PGC-1alpha function in muscle in Huntington’s disease. Hum. Mol. Genet. 2009, 18, 3048–3065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciammola, A.; Sassone, J.; Alberti, L.; Meola, G.; Mancinelli, E.; Russo, M.A.; Squitieri, F.; Silani, V. Increased apoptosis, Huntingtin inclusions and altered differentiation in muscle cell cultures from Huntington’s disease subjects. Cell Death Differ. 2006, 13, 2068–2078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braubach, P.; Orynbayev, M.; Andronache, Z.; Hering, T.; Landwehrmeyer, G.B.; Lindenberg, K.S.; Melzer, W. Altered Ca2+ signaling in skeletal muscle fibers of the R6/2 mouse, a model of Huntington’s disease. J. Gen. Physiol. 2014, 144, 393–413. [Google Scholar] [CrossRef]
- Romer, S.H.; Metzger, S.; Peraza, K.; Wright, M.C.; Jobe, D.S.; Song, L.S.; Rich, M.M.; Foy, B.D.; Talmadge, R.J.; Voss, A.A. A mouse model of Huntington’s disease shows altered ultrastructure of transverse tubules in skeletal muscle fibers. J. Gen. Physiol. 2021, 153, e202012637. [Google Scholar] [CrossRef]
- Lodi, R.; Schapira, A.H.; Manners, D.; Styles, P.; Wood, N.W.; Taylor, D.J.; Warner, T.T. Abnormal in vivo skeletal muscle energy metabolism in Huntington’s disease and dentatorubropallidoluysian atrophy. Ann. Neurol. 2000, 48, 72–76. [Google Scholar] [CrossRef]
- Ciammola, A.; Sassone, J.; Sciacco, M.; Mencacci, N.E.; Ripolone, M.; Bizzi, C.; Colciago, C.; Moggio, M.; Parati, G.; Silani, V.; et al. Low anaerobic threshold and increased skeletal muscle lactate production in subjects with Huntington’s disease. Mov. Disord. 2011, 26, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Gehrig, S.M.; Petersen, J.A.; Frese, S.; Mueller, S.M.; Mihaylova, V.; Ligon-Auer, M.; Lundby, C.; Toigo, M.; Jung, H.H. Skeletal muscle characteristics and mitochondrial function in Huntington’s disease patients. Mov. Disord. 2017, 32, 1258–1259. [Google Scholar] [CrossRef]
- Busse, M.E.; Hughes, G.; Wiles, C.M.; Rosser, A.E. Use of hand-held dynamometry in the evaluation of lower limb muscle strength in people with Huntington’s disease. J. Neurol. 2008, 255, 1534–1540. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F. Huntington disease and other choreas. Neurol. Clin. 2009, 27, 719–736. [Google Scholar] [CrossRef] [PubMed]
- Roos, R.A. Huntington’s disease: A clinical review. Orphanet J. Rare Dis. 2010, 5, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, K.; Canning, C.G.; Menant, J.C.; Loy, C.T. Gait, balance, and falls in Huntington disease. Handb. Clin. Neurol. 2018, 159, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Stoker, T.B.; Mason, S.L.; Greenland, J.C.; Holden, S.T.; Santini, H.; Barker, R.A. Huntington’s disease: Diagnosis and management. Pract. Neurol. 2022, 22, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Fritz, N.E.; Rao, A.K.; Kegelmeyer, D.; Kloos, A.; Busse, M.; Hartel, L.; Carrier, J.; Quinn, L. Physical Therapy and Exercise Interventions in Huntington’s Disease: A Mixed Methods Systematic Review. J. Huntingt. Dis. 2017, 6, 217–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zinzi, P.; Salmaso, D.; De Grandis, R.; Graziani, G.; Maceroni, S.; Bentivoglio, A.; Zappata, P.; Frontali, M.; Jacopini, G. Effects of an intensive rehabilitation programme on patients with Huntington’s disease: A pilot study. Clin. Rehabil. 2007, 21, 603–613. [Google Scholar] [CrossRef]
- Van Dellen, A.; Cordery, P.M.; Spires, T.L.; Blakemore, C.; Hannan, A.J. Wheel running from a juvenile age delays onset of specific motor deficits but does not alter protein aggregate density in a mouse model of Huntington’s disease. BMC Neurosci. 2008, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Potter, M.C.; Yuan, C.; Ottenritter, C.; Mughal, M.; van Praag, H. Exercise is not beneficial and may accelerate symptom onset in a mouse model of Huntington’s disease. PLoS Curr. 2010, 2, RRN1201. [Google Scholar] [CrossRef]
- Thompson, J.A.; Cruickshank, T.M.; Penailillo, L.E.; Lee, J.W.; Newton, R.U.; Barker, R.A.; Ziman, M.R. The effects of multidisciplinary rehabilitation in patients with early-to-middle-stage Huntington’s disease: A pilot study. Eur. J. Neurol. 2013, 20, 1325–1329. [Google Scholar] [CrossRef]
- Piira, A.; van Walsem, M.R.; Mikalsen, G.; Nilsen, K.H.; Knutsen, S.; Frich, J.C. Effects of a One Year Intensive Multidisciplinary Rehabilitation Program for Patients with Huntington’s Disease: A Prospective Intervention Study. PLoS Curr. 2013, 5, ecurrents.hd.9504af71e0d1f87830c25c394be47027. [Google Scholar] [CrossRef]
- Busse, M.; Quinn, L.; Debono, K.; Jones, K.; Collett, J.; Playle, R.; Kelly, M.; Simpson, S.; Backx, K.; Wasley, D.; et al. A randomized feasibility study of a 12-week community-based exercise program for people with Huntington’s disease. J. Neurol. Phys. Ther. 2013, 37, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H.; Quinn, L.; van Deursen, R.; Dawes, H.; Playle, R.; Rosser, A.; Busse, M. What effect does a structured home-based exercise programme have on people with Huntington’s disease? A randomized, controlled pilot study. Clin. Rehabil. 2013, 27, 646–658. [Google Scholar] [CrossRef] [PubMed]
- Piira, A.; van Walsem, M.R.; Mikalsen, G.; Øie, L.; Frich, J.C.; Knutsen, S. Effects of a Two-Year Intensive Multidisciplinary Rehabilitation Program for Patients with Huntington’s Disease: A Prospective Intervention Study. PLoS Curr. 2014, 6, ecurrents.hd.2c56ceef7f9f8e239a59ecf2d94cddac. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, T.M.; Thompson, J.A.; Domínguez, D.J.; Reyes, A.P.; Bynevelt, M.; Georgiou-Karistianis, N.; Barker, R.A.; Ziman, M.R. The effect of multidisciplinary rehabilitation on brain structure and cognition in Huntington’s disease: An exploratory study. Brain Behav. 2015, 5, e00312. [Google Scholar] [CrossRef] [PubMed]
- Quinn, L.; Hamana, K.; Kelson, M.; Dawes, H.; Collett, J.; Townson, J.; Roos, R.; van der Plas, A.A.; Reilmann, R.; Frich, J.C.; et al. A randomized, controlled trial of a multi-modal exercise intervention in Huntington’s disease. Parkinsonism Relat. Disord. 2016, 31, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Frese, S.; Petersen, J.A.; Ligon-Auer, M.; Mueller, S.M.; Mihaylova, V.; Gehrig, S.M.; Kana, V.; Rushing, E.J.; Unterburger, E.; Kägi, G.; et al. Exercise effects in Huntington disease. J. Neurol. 2017, 264, 32–39. [Google Scholar] [CrossRef]
- Mueller, S.M.; Gehrig, S.M.; Petersen, J.A.; Frese, S.; Mihaylova, V.; Ligon-Auer, M.; Khmara, N.; Nuoffer, J.M.; Schaller, A.; Lundby, C.; et al. Effects of endurance training on skeletal muscle mitochondrial function in Huntington disease patients. Orphanet J. Rare Dis. 2017, 12, 184. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, D.M.; Dominguez, D.J.; Lazar, A.S.; Kordsachia, C.C.; Rankin, T.J.; Lo, J.; Govus, A.D.; Power, B.D.; Lampit, A.; Eastwood, P.R.; et al. Multidisciplinary rehabilitation reduces hypothalamic grey matter volume loss in individuals with preclinical Huntington’s disease: A nine-month pilot study. J. Neurol. Sci. 2020, 408, 116522. [Google Scholar] [CrossRef]
- Caldwell, C.C.; Petzinger, G.M.; Jakowec, M.W.; Cadenas, E. Treadmill exercise rescues mitochondrial function and motor behavior in the CAG(140) knock-in mouse model of Huntington’s disease. Chem. Biol. Interact. 2020, 315, 108907. [Google Scholar] [CrossRef]
- Ji, E.S.; Kim, Y.M.; Shin, M.S.; Kim, C.J.; Lee, K.S.; Kim, K.; Ha, J.; Chung, Y.R. Treadmill exercise enhances spatial learning ability through suppressing hippocampal apoptosis in Huntington’s disease rats. J. Exerc. Rehabil. 2015, 11, 133–139. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.M.; Ji, E.S.; Kim, S.H.; Kim, T.W.; Ko, I.G.; Jin, J.J.; Kim, C.J.; Kim, T.W.; Kim, D.H. Treadmill exercise improves short-term memory by enhancing hippocampal cell proliferation in quinolinic acid-induced Huntington’s disease rats. J. Exerc. Rehabil. 2015, 11, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Wood, N.I.; Glynn, D.; Morton, A.J. “Brain training” improves cognitive performance and survival in a transgenic mouse model of Huntington’s disease. Neurobiol. Dis. 2011, 42, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Renoir, T.; Pang, T.Y.; Zajac, M.S.; Chan, G.; Du, X.; Leang, L.; Chevarin, C.; Lanfumey, L.; Hannan, A.J. Treatment of depressive-like behaviour in Huntington’s disease mice by chronic sertraline and exercise. Br. J. Pharmacol. 2012, 165, 1375–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanko, D.P.; Shah, V.D.; Yamasaki, W.K.; Petzinger, G.M.; Jakowec, M.W. Treadmill exercise delays the onset of non-motor behaviors and striatal pathology in the CAG(140) knock-in mouse model of Huntington’s disease. Neurobiol. Dis. 2017, 105, 15–32. [Google Scholar] [CrossRef]
- Harrison, D.J.; Busse, M.; Openshaw, R.; Rosser, A.E.; Dunnett, S.B.; Brooks, S.P. Exercise attenuates neuropathology and has greater benefit on cognitive than motor deficits in the R6/1 Huntington’s disease mouse model. Exp. Neurol. 2013, 248, 457–469. [Google Scholar] [CrossRef] [Green Version]
- Corrochano, S.; Blanco, G.; Williams, D.; Wettstein, J.; Simon, M.; Kumar, S.; Moir, L.; Agnew, T.; Stewart, M.; Landman, A.; et al. A genetic modifier suggests that endurance exercise exacerbates Huntington’s disease. Hum. Mol. Genet. 2018, 27, 1723–1731. [Google Scholar] [CrossRef] [Green Version]
- Mahalakshmi, B.; Maurya, N.; Lee, S.D.; Bharath Kumar, V. Possible Neuroprotective Mechanisms of Physical Exercise in Neurodegeneration. Int. J. Mol. Sci. 2020, 21, 5895. [Google Scholar] [CrossRef]
- Öhman, H.; Savikko, N.; Strandberg, T.E.; Kautiainen, H.; Raivio, M.M.; Laakkonen, M.L.; Tilvis, R.; Pitkälä, K.H. Effects of Exercise on Cognition: The Finnish Alzheimer Disease Exercise Trial: A Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2016, 64, 731–738. [Google Scholar] [CrossRef]
- Van Praag, H.; Christie, B.R.; Sejnowski, T.J.; Gage, F.H. Running enhances neurogenesis, learning, and long-term potentiation in mice. Proc. Natl. Acad. Sci. USA 1999, 96, 13427–13431. [Google Scholar] [CrossRef] [Green Version]
- Patterson, S.L.; Grover, L.M.; Schwartzkroin, P.A.; Bothwell, M. Neurotrophin expression in rat hippocampal slices: A stimulus paradigm inducing LTP in CA1 evokes increases in BDNF and NT-3 mRNAs. Neuron 1992, 9, 1081–1088. [Google Scholar] [CrossRef]
- Boncompagni, S.; Michelucci, A.; Pietrangelo, L.; Dirksen, R.T.; Protasi, F. Exercise-dependent formation of new junctions that promote STIM1-Orai1 assembly in skeletal muscle. Sci. Rep. 2017, 7, 14286. [Google Scholar] [CrossRef] [PubMed]
- Michelucci, A.; Boncompagni, S.; Pietrangelo, L.; García-Castañeda, M.; Takano, T.; Malik, S.; Dirksen, R.T.; Protasi, F. Transverse tubule remodeling enhances Orai1-dependent Ca2+ entry in skeletal muscle. Elife 2019, 8, e47576. [Google Scholar] [CrossRef] [PubMed]
- Protasi, F.; Pietrangelo, L.; Boncompagni, S. Calcium entry units (CEUs): Perspectives in skeletal muscle function and disease. J. Muscle Res. Cell Motil. 2021, 42, 233–249. [Google Scholar] [CrossRef]
- Lee, B.; Shin, M.; Park, Y.; Won, S.Y.; Cho, K.S. Physical Exercise-Induced Myokines in Neurodegenerative Diseases. Int. J. Mol. Sci. 2021, 22, 5795. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Hayden, M.R.; Xu, B. BDNF overexpression in the forebrain rescues Huntington’s disease phenotypes in YAC128 mice. J. Neurosci. 2010, 30, 14708–14718. [Google Scholar] [CrossRef]
- Giralt, A.; Carretón, O.; Lao-Peregrin, C.; Martín, E.D.; Alberch, J. Conditional BDNF release under pathological conditions improves Huntington’s disease pathology by delaying neuronal dysfunction. Mol. Neurodegener. 2011, 6, 71. [Google Scholar] [CrossRef] [Green Version]
- Pang, T.Y.C.; Stam, N.C.; Nithianantharajah, J.; Howard, M.L.; Hannan, A.J. Differential effects of voluntary physical exercise on behavioral and brain-derived neurotrophic factor expression deficits in Huntington’s disease transgenic mice. Neuroscience 2006, 141, 569–584. [Google Scholar] [CrossRef]
- Herbst, E.A.; Holloway, G.P. Exercise training normalizes mitochondrial respiratory capacity within the striatum of the R6/1 model of Huntington’s disease. Neuroscience 2015, 303, 515–523. [Google Scholar] [CrossRef]
- Ju, T.C.; Chen, H.M.; Lin, J.T.; Chang, C.P.; Chang, W.C.; Kang, J.J.; Sun, C.P.; Tao, M.H.; Tu, P.H.; Chang, C.; et al. Nuclear translocation of AMPK-alpha1 potentiates striatal neurodegeneration in Huntington’s disease. J. Cell Biol. 2011, 194, 209–227. [Google Scholar] [CrossRef] [Green Version]
- Unified Huntington’s Disease Rating Scale: Reliability and consistency. Huntington Study Group. Mov. Disord. 1996, 11, 136–142. [CrossRef]
- McColgan, P.; Tabrizi, S.J. Huntington’s disease: A clinical review. Eur. J. Neurol. 2018, 25, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.M.; Petersen, J.A.; Jung, H.H. Exercise in Huntington’s Disease: Current State and Clinical Significance. Tremor Other Hyperkinet. Mov. 2019, 9, 601. [Google Scholar] [CrossRef]
- Quinn, L.; Debono, K.; Dawes, H.; Rosser, A.E.; Nemeth, A.H.; Rickards, H.; Tabrizi, S.J.; Quarrell, O.; Trender-Gerhard, I.; Kelson, M.J.; et al. Task-specific training in Huntington disease: A randomized controlled feasibility trial. Phys. Ther. 2014, 94, 1555–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosinski, C.M.; Schlangen, C.; Gellerich, F.N.; Gizatullina, Z.; Deschauer, M.; Schiefer, J.; Young, A.B.; Landwehrmeyer, G.B.; Toyka, K.V.; Sellhaus, B.; et al. Myopathy as a first symptom of Huntington’s disease in a Marathon runner. Mov. Disord. 2007, 22, 1637–1640. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Study Design | Model | Sample Size | Intervention | Result | Conclusion |
|---|---|---|---|---|---|---|
| Zinzi et al. (2007) [36] | Pilot clinical trials | Humans | n = 40 | 8 h a day for 5 days and 4 h a day for one day per week, repeated three times afor 1 year of physical, occupational and speech therapy, cognitive rehabilitation and respiratory exercises | Significant improvement of motor performance and activities of day living and maintaining of cognitive function | Intensive rehabilitation treatments may have a positive effest on motor and functional performance in patients with Huntington’s disease |
| Van Dellen et al. (2008) [37] | Mouse general health and behavioral assessment | Mice | n/a | Voluntary wheel running exercise from juvenile age (4 weeks) to adulthood (9 months). Open field and rotarod test at 5 months of age | Motor deficts on rotarod test delayed by wheel running as well as rear-paw clasping. Enviormental enrichment and wheel running decreased the abnormal locomotor activities | Voluntary wheel running started before the symptomatic stage of the disease can delay the onset of some motor deficits in HD mice |
| Potter et al. (2010) [38] | Mouse general health and behavioral assessment | Mice | n = 54 | Voluntary running exercise from an age of 44 days to an age of 113 days. Morris water maze test at 88 days old, rotarod test at 100 days old and open field test at 103 days old | Running exercise worsened the HD motor deficits and accelerated its onset | Running is not effective in delaying HD symptoms. Exercise is not beneficial and may have a negative effect in the mouse model analyzed |
| Thompson et al. (2013) [39] | Randomized controlled trials | Humans | n = 20 | Supervised group sessions of 9 months, once per week; 5 min warm-up, 10 min aerobic exercise, 40 min resistance exercise, 5 min cool-down. 6 months of home-based exercise 3 times per week. Occupational therapy for 1 h fortnight, for 6 months | Reduction of the loss of postural and dynamic stability; mild improvement in quality of life, depression and cognition; significant improvement in fat-free mass and strength | Multidisciplinary rehabilitation program is feasible and well tollerated in early to middle stage HD patients. Patients also reported therapeutic benefits |
| Piira et al. (2013) [40] | Prospective intervention study | Humans | n = 37 | Physiotherapy, occupational and speech therapy, gym and/or swimming training, 8 h 5 days per week for 1 year. | Significant gains in balance, gait, activities of day living, quality of life, anxiety and depression | Multidisciplinary rehabilitation improved balance, gait function, and quality of life |
| Busse et al. (2013) [41] | Randomized feasibility study | Humans | n = 31 | 12 weeks of walking and cycling aerobic training at 55–75% of predicted HRmax; resistance exercises for lower limbs (2× 8–12 reps at 60–70% of 1 RM) | Moderate effect sizes showed benefits for cognitive and walking measures. | A structured exercise intervention gives improvements in motor function and quality of life in HD patients |
| Khalil et al. (2013) [42] | Randomized controlled pilot study | Humans | n = 25 | home-based exercise for 8 weeks consisting of gradual progressive walking exercise 3 times per week | Walking speed and gait variability improvement with large effect sizes. Balance, funtion and level of phisical activity also had a significant improvement | Home based exercise are feasible, beneficial and safe for HD mid-stage patients |
| Piira et al. (2014) [43] | Prospective intervention study | Humans | n = 10 | Physiotherapy occupational and speech therapy, gym and/or swimming training, 8 h five days per week for two years | Non significant decline of gait, balance and cognitive measures. Not significant increasing for quality of life, activities of day living and motor function | Intensive multidisciplinary rehabilitation is well tollerated among midlle stage HD patients. |
| Cruickshawk et al. (2015) [44] | Exploratory study | Humans | n = 15 | 1 h of aerobic and resistance training per week in clinic; 1 h of home based exercises 3 times per week; occupational therapy once every 2 weeks | Significant volumetric grey matter improvement and significant increasing of verbal learning and memory | Multidisciplinary rehabilitation may have a positive impacts on gray matter changes and cognitive functions in HD patients. |
| Quinn et al. (2016) [45] | Randomized controlled trial | Humans | n = 32 | 12 weeks of 30 min cycling training (65–85% of age predicted HRmax) and 10–15 min of strengthening exercises (2× 10–12 reps) | Improvement in VO2max, general fitness and motor function | A short-term exercise progam is safe, feasible and may be beneficial for midlle stage HD patients |
| Frese et al. (2017) [46] | Clinical trials | Humans | n = 24 | 10 weeks of 30 min cycling (65%VO2peak) 3 times per week, 8 weeks of HIIT (4 × 4 min at 90–95% of HRpeak with 3 min low-intensity rest intervals at 70% of HRpeak) 3 times per week and endurance training 3 times per week | Motor deficit stabilization, VO2max significant improvement | Specified exercise programs may induce therapeutic beneficial effects in HD patients |
| Mueller et al. (2017) [47] | Clinical trials | Humans | n = 24 | 10 weeks of 30 min cycling (65%VO2peak) 3 times per week, 8 weeks of HIIT (4 × 4 min at 90–95% of HRpeak with 3 min low-intensity rest intervals at 70% of HRpeak) 3 times per week and endurance training 3 times per week | Increasing in the activity of citrate synthase, complex III, complex V and succinate cytochrome c reductase | HD patients could benefit from an endurance training program in terms of delaying the progressive muscular dysfunction. The training program was also safe and feasible. |
| Bartlett et al. (2020) [48] | Pilot clinical trials | Humans | n = 29 | 9 months of aerobic and resistance training 2 times per week, bilingual exercise, dual-task training 1 time per week for 1-h, computerized cognitive training 3 times per week for 1 h and social activities. | Maintanance of serum BDNF levels, decreasing of cortisol and melatonin concentration | A program of multidisciplinary rehabilitation may be useful for maintaining peripheral BDNF levels and decreasing the hypothalamic volume loss in preclinical HD individuals |
| Caldwell et al. (2020) [49] | Mouse general health and behavioral assessment | Mice | n = 16 | Running at a speed of 8.0 m/min for 40 min for first week; starting from second week exercise running at 10.0 ± 1.5 m/min 3 times per week for a 12-week period. Final month of exercise with running speed set at 20 ± 1.5 m/min | Treadmill exercise resulted in improved mitochondrial oxidative phosphorylation complex activity. Improvement were also registered fot glycolisys, pyruvate deidrogenase and carboxylase activity | Treadmill exercise may be beneficial for motor behavior thanks to reverisng deficits in mitochondrial function in a rodent model of HD |
| E.S. Ji et al. 2015 [50] | Mouse general health and behavioral assessment | Mice | n = 40 | 30 min of treadmill running once a day for 14 days; running speed set at 2 m/min for the first 5 min, then at 5 m/min for the next 5 min and at 8 m/min for the last 20 min of exercise | Treadmill running exercise rescued motor coordination and suppressed caspase-3 expression | Running exercise could be beneficial in improving quinolinic acid-induced loss of spatial learning ability and coordination in HD mouse model |
| Kim et al. 2015 [51] | Mouse general health and behavioral assessment | Mice | n = 40 | 30 min of treadmill running once a day for 14 days; running speed set at 2 m/min for the first 5 min, then at 5 m/min for the next 5 min and at 8 m/min for the last 20 min of exercise | Treadmill running exercise enhanced the production of neurotrophic factors in the brain and ameliorated memory and learnig ability | Treadmill exercise influences positively the cell proliferation in the hippocampal dentate gyrus by ameliorating the BDNF expression in HD rats; hence, treadmill exercise has beneficial effects HD symptoms |
| Wood et al. 2011 [52] | Mouse general health and behavioral assessment | Mice | n = 128 | 11 days of training in Lashley III maze, then rotarod training for 1 day; lastly, 14 days of training in Lashley III maze again | There were no significant improvement in mice performance after training | Physical exercise on the rotarod did not significantly improve motor coordination of R6/2 mice, but it did not induced deleterious effects |
| Renoir et al. 2012 [53] | Mouse general health and behavioral assessment | Mice | n = 140 | 4 weeks of voluntary wheel running exercise | Wheel running exercise and chronic setraline treatment prevent depressive like behaviours by correcting the 5-HT1A autoreceptor dysfunction | Wheel-running exercise improved cognition and prevented depressive-like behaviours in R6/1 HD mice |
| Stefanko et al. 2017 [54] | Mouse general health and behavioral assessment | Mice | n = 320 | Running at a speed of 8.0 m/min for 40 min for first week; starting from second week exercise running at 10.0 ± 1.5 m/min 3 times per week for 6 months. Final month of exercise with running speed set at 20 ± 1.5 m/min | CAG140 KI mouse did not show significant worsening in performace at the rotarod test and forced swimmig test compared to wild type animals | A long term training program of running exercise is effective in delaying the onset of depression like behaviors in CAG140 KI mouse model of HD when started before the onset of motor symtoms |
| Harrison et al. 2013 [55] | Mouse general health and behavioral assessment | Mice | n = 67 | Running wheel exercise 14 h per day, for five days for 22 weeks. Behavioural testing every for weeks | Wheel running produced some benefit on stride length and reduction of striatal neuronal cell loss | Chronic wheel running exercise enhance cognitive funtion, reduce striatal cell loss in in the R6/1 HD mouse indicating that exercise may be benficial in HD |
| Corrochano et al. 2018 [56] | Mouse general health and behavioral assessment | Mice | n/a | Forced endurance training protocol consiting in 30 min of rotarod set at 15 rpm, 5 day/week. Mice had also the oppurtunity to pratice voluntary running exercise in their cages | Endurance training was detrimental for HD mice, inducing the activation of AMPK in skeletal muscles | Physical activity that causes an high energy demands should be proposed to HD patients with caution |
| Authors | Participants Characteristics | Intervention Programs | Measured Outcome |
|---|---|---|---|
| Zinzi et al. (2007) [36] | n = 40 (M = 17; F = 23) age = 52.0 (3.3) CG = n/a | Respiratory exercise, speech therapy, physical therapy, occupational therapy, cognitive rehabilitation exercise | Balance, gait, depression, cognitive status, activities of day living |
| Thompson et al. (2013) [39] | n = 20 (M = n/a; F = n/a) age CG = 53.8 (2.9) age IG = 52.2 (2.9) | Aerobic exercise, resistance exercise, home-based occupational therapy | Motor function, cognition, body composition, postural stability, quality of life |
| Piira et al. (2013) [40] | n = 37 (M = 18; F = 19) age = 52,4 (13.1) CG = n/a | Physiotherapy, occupational and speech therapy, gym/swimming exercises, group discussions | Motor function, quality of life, cognitive function, depression/anxiety |
| Busse et al. (2013) [41] | n = 31 (M = 16; F = 15) age CG = 47.4 (9.5) age IG = 53.3 (12.5) | Aerobic training, resistance exercise | Motor function, quality of life |
| Khalil et al. (2013) [42] | n= 25 (M = n/a; F = n/a) age CG = 51.3 (16.9) age IG = 54.2 (9.9) | Resistance exercise, balance exercise. | Gait, balance, quality of life |
| Cruickshawk et al. (2015) [44] | n= 15 (M = 8; F = 7) age = 52.5 (6.6) CG = n/a | Home-based aerobic and resistance exercises, occupational therapy | Grey matter volume, verbal learning, memory |
| Quinn et al. (2016) [45] | n= 32 (M = 16; F = 16) age CG = 51.0 (17.0) age IG = 53.0 (11.0) | Aerobic training, resistance exercise | Motor function, fitness, cognition |
| Frese et al. (2017) [46] | n= 24 (M = 24; F = 0) age CG = 49.1 (6.8) age IG = 54.8 (7.1) | Aerobic and endurance training, high-intensity interval training | Motor function, dementia, cardiovascular performance |
| Mueller et al. (2017) [47] | n= 24 (M = 24; F = 0) age CG = 49.7 (6,8) age IG = 53.2 (8.8) | Aerobic and endurance training, high-intensity interval training | Mitochondrial function |
| Bartlett et al. (2020) [48] | n= 29 (M = 10; F= 19) age CG = 50.55 (9.49) age IG = 40.89 (11.73) | Aerobic exercise, resistance exercise, dual-task, bilingual exercise, cognitive training | Grey matter volume, BDNF concentration |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trovato, B.; Magrì, B.; Castorina, A.; Maugeri, G.; D’Agata, V.; Musumeci, G. Effects of Exercise on Skeletal Muscle Pathophysiology in Huntington’s Disease. J. Funct. Morphol. Kinesiol. 2022, 7, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7020040
Trovato B, Magrì B, Castorina A, Maugeri G, D’Agata V, Musumeci G. Effects of Exercise on Skeletal Muscle Pathophysiology in Huntington’s Disease. Journal of Functional Morphology and Kinesiology. 2022; 7(2):40. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7020040
Chicago/Turabian StyleTrovato, Bruno, Benedetta Magrì, Alessandro Castorina, Grazia Maugeri, Velia D’Agata, and Giuseppe Musumeci. 2022. "Effects of Exercise on Skeletal Muscle Pathophysiology in Huntington’s Disease" Journal of Functional Morphology and Kinesiology 7, no. 2: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/jfmk7020040